
Abstract
BACKGROUND:
The occurrence of subacromial pain syndrome (SPS) is associated with the frequent handling and lifting of heavy loads and excessive repetitive work. Thus, assembly workers have a high prevalence of SPS.
OBJECTIVE:
The purpose of this study was to investigate differences in shoulder ROM, muscle strength, asymmetry ratio, function, productivity, and depression between workers with and without SPS.
METHODS:
Sixty-seven male workers (35 workers with SPS and 32 workers without SPS) participated in this study. Shoulder internal rotation (SIR), shoulder external rotation (SER), shoulder abduction (SAB), shoulder horizontal adduction ROM and SIR, SER, elbow flexion (EF), scapular depression and adduction, scapular protraction strength were measured. The asymmetry ratio was calculated using the asymmetry ratio formula; shoulder functions were measured using the shoulder pain and disability index (SPADI), disabilities of the arm, shoulder, and hand (DASH), and visual analogue scale (VAS); and Endicott work productivity scale (EWPS).
RESULTS:
The SPADI (p = 0.001), DASH (p = 0.001), and VAS (p = 0.001) values of workers with SPS were higher than those of workers without SPS. Also, workers with SPS had lower SIR (p = 0.001) and SAB (p = 0.002) ROM compared to workers without SPS. In addition, workers with SPS exhibited lower SIR (p = 0.012) strength than workers without SPS. Workers with SPS had higher asymmetry ratio in SIR (p = 0.015), SER (p = 0.005), and EF (p = 0.008) strength than workers without SPS.
CONCLUSIONS:
The SIR, SAB ROM, SIR strength, and the asymmetry ratio of SIR, SER, EF strengths could provide an important baseline comparison for the workers with SPS.
Keywords
Introduction
Subacromial pain syndrome (SPS), most commonly referred to as ‘shoulder impingement syndrome’ is common not only among athletes performing overhead movements such as throwing or swimming but also among workers who perform constant arm movements [1–3]. Especially intensive work using shoulder joints can be a risk factor for SPS in workers [1, 4]. Repeated strain on the shoulder joint and working with hands above the acromion height can lead to mechanical compression of the rotator cuff, subacromial bursa, and biceps tendon, leading to shoulder disease such as tendinitis, bursitis, and rotator cuff tear [1]. SPS considered to be a part of the process involved in the degeneration of the rotator cuff [5]. Therefore, early identification of the physical factors that could mediate SPS is important [6]. Several factors contribute to the onset of SPS, including abnormal acromial morphology, incorrect kinematic patterns associated with altered rotator cuff or scapular muscle function, and capsular abnormalities (including posterior capsular tightness and capsular laxity) [2, 8].
Studies have suggested that SPS patients exhibit decreased range of motion (ROM) of the shoulder complex [2, 9]. Warner et al. found that patients with SPS exhibited significantly reduced shoulder internal rotation (SIR) and shoulder horizontal adduction (SHA) angle compared to those with shoulder instability. Similarly, Tyler et al. found that patients with SPS in the dominant arm exhibited reduced SIR ROM compared to normal subjects, and patients with SPS in the non-dominant arm exhibited reduced SIR and shoulder external rotation (SER) ROM. In addition, patients with SPS showed increased posterior capsule tightness. Tightness of the posterior capsule can contribute to abnormal arthrokinematics or the inability of the humeral head to roll anteriorly and slide posteriorly in the glenoid, resulting in a decreased SIR ROM [2].
The shoulder complex, composed of four joints (glenohumeral, acromioclavicular, sternoclavicular, and scapulothoracic), relies on muscles to provide dynamic stability during its wide ROM [10]. Dynamic stability refers to the synergistic action of the muscles surrounding the shoulder complex to stabilize the humeral head on the glenoid fossa [10]. Proper balance among the muscles surrounding the shoulder complex for dynamic stability is essential for shoulder mobility [11, 12]. For example, normal shoulder elevation appears as a major force couple interaction between the serratus anterior and trapezius muscles, which rotates the scapula upward [10]. However, the lack of ROM or strength in specific muscles must be compensated for by another shoulder muscle, which leads to shoulder dysfunction [13]. These muscle imbalances lead to changes in joint kinematics and, eventually, SPS [13]. In a text about assessment and treatment of muscle imbalance, the Janda approach suggested that weakness of shoulder muscles, such as the serratus anterior, infraspinatus, lower and middle trapezius, as well as tightness of the pectorals and upper trapezius muscles, cause SPS [11]. Other studies have reported that weakness of the rotator cuff muscles affects the onset of SPS [14].
Although the relative weakness or tightness of certain muscles among these scapulo-thoracic and scapulo-humeral muscles may cause SPS, other studies have reported conflicting results. According to Erol et al., the strength of SIR did not differ significantly between people with and without SPS. Likewise, no significant difference was found in terms of in SER strength between the people with and without SPS [15]. Only a deficit in relative SIR muscle strength on the involved side compared to that on the normal side was found to be a significant difference between those with and without SPS [15]. Bak and Magnusson reported no significant difference in the SER strength of elite swimmers with and without SPS.
Shoulder impingement syndrome, the classic meaning of SPS, has been known to cause pain due to the compression of the rotator cuff and related structures with the acromion and coracoacromial ligament [17, 18]. Recently, different classification of shoulder impingement syndrome such as coracoid impingement and internal impingement have been introduced as causes of rotator cuff injury [19, 20]. If the SPS that causes the rotator cuff tendons to impinge in the coracoacromial arch is called ‘outlet impingement’, the intra-articular impingement where the rotator cuff tendons press with the labrum in the posterior-superior glenoid during shoulder abduction and external rotation such as throwing motion is called ‘internal impingement’ [21]. Although many studies have compared physical factors such as shoulder ROM and muscle strength in patients with and without SPS, previous studies did not classify or subdivide SPS according to the characteristics of the subjects, so there may have been conflicts in describing the physical differences of subjects with SPS. Therefore, this study aimed to identify any differences in shoulder ROM, muscle strength, asymmetry ratio, function, pain, productivity, and severity of depression between workers with and without SPS. We hypothesized that workers with SPS would have reduced shoulder joint ROM and muscle strength compared with normal workers due to shoulder muscle imbalance. Also, the asymmetry ratio between the involved and uninvolved sides of workers with SPS would be greater than those of workers without SPS. In addition, shoulder function, psychological factors, and work performance would be reduced.
Methods
Subjects and design
This was a cross-sectional study conducted at automobile assembly line owned by the Mando Company in Wonju City, Kangwon-do in Korea, and the workers on the assembly line were all male. We conducted pilot study in preparation for this research. Based on a pilot study, the required sample size (n = 62) was calculated using G*Power 3.1 software (G*Power Software Inc., Kiel, Germany) with an effect size of 0.73 standard deviation (SD) with an α level of 0.05 and a power of 0.80. A flowchart of the study is provided in Fig. 1. Sixty-seven assembly line male workers (35 workers with SPS and 32 workers without SPS) participated in this study (Table 1). All subjects were explained the risks and benefits associated with this study, and they signed an informed consent form. Workers with SPS were included if they had a pain located on the anterolateral side of the shoulder for at least 3 months; and a positive sign in one or more orthopaedic tests [22]. The orthopaedic tests used in this study were the Neer and Hawkins tests, procedures to induce symptoms associated with subacromial pain syndrome [22, 23]. The exclusion criteria were history of dislocation; traumatic injuries of the shoulder, elbow, or hand; history of shoulder, elbow, or hand surgery. This study was approved by the Yonsei University Mirae Institutional Review Board (approval number: 1041849-201710-BM-112-02).
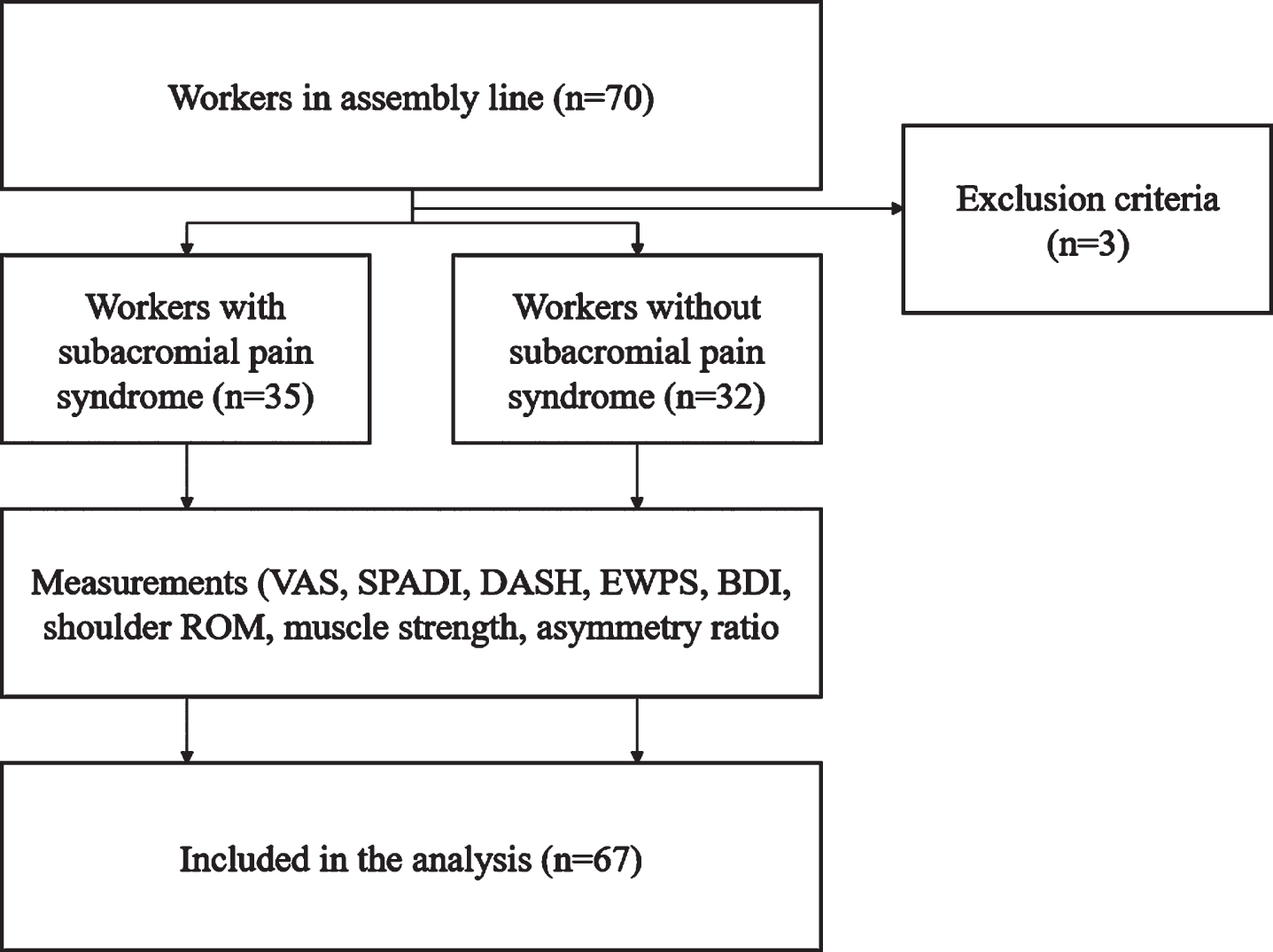
Flowchart of study.
Subject characteristics (mean±SD)
All subjects completed the shoulder pain and disability index (SPADI), disabilities of the arm, shoulder, and hand (DASH), visual analogue scale (VAS), Endicott work productivity scale (EWPS), and Beck depression index (BDI). The SPADI is a self-reported questionnaires that measures pain and disability in the shoulder and used to assess the degree to which shoulder pain impacts functional activities. In this study, SPADI that was translated into Korean was used to evaluate the symptoms and severity of SPS [24]. DASH is a self-reported questionnaire for diagnosing orthopedic disorders of the hands and upper limbs disorders, and it was developed by American Orthopedic Society and Institute for Work & Health as a tool for determining the subjective state of the upper limbs. DASH that was translated into Korean was used to evaluate the subjective state of the upper limbs of SPS [25]. VAS is a reliable and valid assessment tool that has been used to assess pain levels. VAS was used to measure the severity and perception of shoulder pain caused by SPS. The self-reported EWPS questionnaire consists of 25 items, and it was used to measure behaviors and subjective feelings or attitudes that can reduce productivity and effectiveness in work activities [26, 27]. EWPS was used to evaluate whether the health status of workers with SPS affects their work performance. BDI is a 21-question multiple-choice self-report inventory, and it is among the most widely used psychometric tests for measuring depression severity. Korean-BDI version I was used to measure the severity of depression among workers.
Experimental procedure
Before data collection, the subjects were familiarized with the testing protocol, provided instructions, and asked to practice the shoulder ROM and strength measurements to ensure proper motion. All subjects were measured ROM including SIR, SER, SHA, SAB, and the maximal isometric muscle strength including SIR, SER, scapular depression and adduction (SDA), elbow flexion (EF), scapular protraction (SP). Each measurement was repeated three times. When measuring strength, subjects maintained each trial for 5 s and 1 min resting period was given between repetitions. 5 min of resting period was given between strength measurements to prevent muscle fatigue. The shoulder ROM and strength were measured using the Smart KEMA motion and strength sensors (Smart KEMA system, KOREATECH Co., Ltd., Seoul, Korea). While the examiner performed the measurements, another examiner recorded the data of the sensor transmitted to the tablet in real time. All shoulder ROM measurement data were expressed in degrees and the shoulder muscle strength measurement data were expressed in kilograms. The real-time value of strength for was recorded over 5 s, and the Smart KEMA software computed the average of the data for the middle 3 s for data analysis. The average strength was recorded with software and was normalized to the subject’s weight (Nm/kg). The asymmetry ratio was calculated as (uninvolved – involved side)/(uninvolved+involved side) * 100) for the SPS group and (dominant – non dominant side)/(dominant+non dominant) * 100) for the control group.
Measurement of range of motion
To measure SIR ROM, subjects were positioned supine on a table, with the shoulder to be tested positioned at 90° of glenohumeral abduction. The examiner held the subject’s forearm and turned the shoulder in the internal rotation direction until the end feel of the shoulder joint was felt [28, 29]. To measure SER ROM, subjects were positioned supine on a table with the shoulder to be tested positioned at 90° of glenohumeral abduction. Then, the examiner held the subject’s forearm and turned the shoulder in the external rotation direction until the end feel of the shoulder joint was felt [28]. SAB ROM measurement was performed in a sitting position. In the sitting position on the table, the subject’s palm was pointed along the forward direction. The examiner held the subject’s distal humerus and performed the abduction motion until the end feel of the shoulder joint was felt [30]. To measure SHA ROM, the shoulder to be measured was placed on the table with the subject lying down sideways to prevent abduction of the subject’s scapula during the movement. The frontal plane of the body was aligned to be perpendicular to the ground. Then, the shoulder was flexed by 90°, such that the subject’s palm faced the ceiling. The examiner held the distal part of the humerus and moved it in the horizontal adduction direction without EF, while the upper body or acromion was prevented from rotating in the front or rear direction [31]. SHA ROM was measured when the examiner felt the end feel of the shoulder joint (Fig. 2).
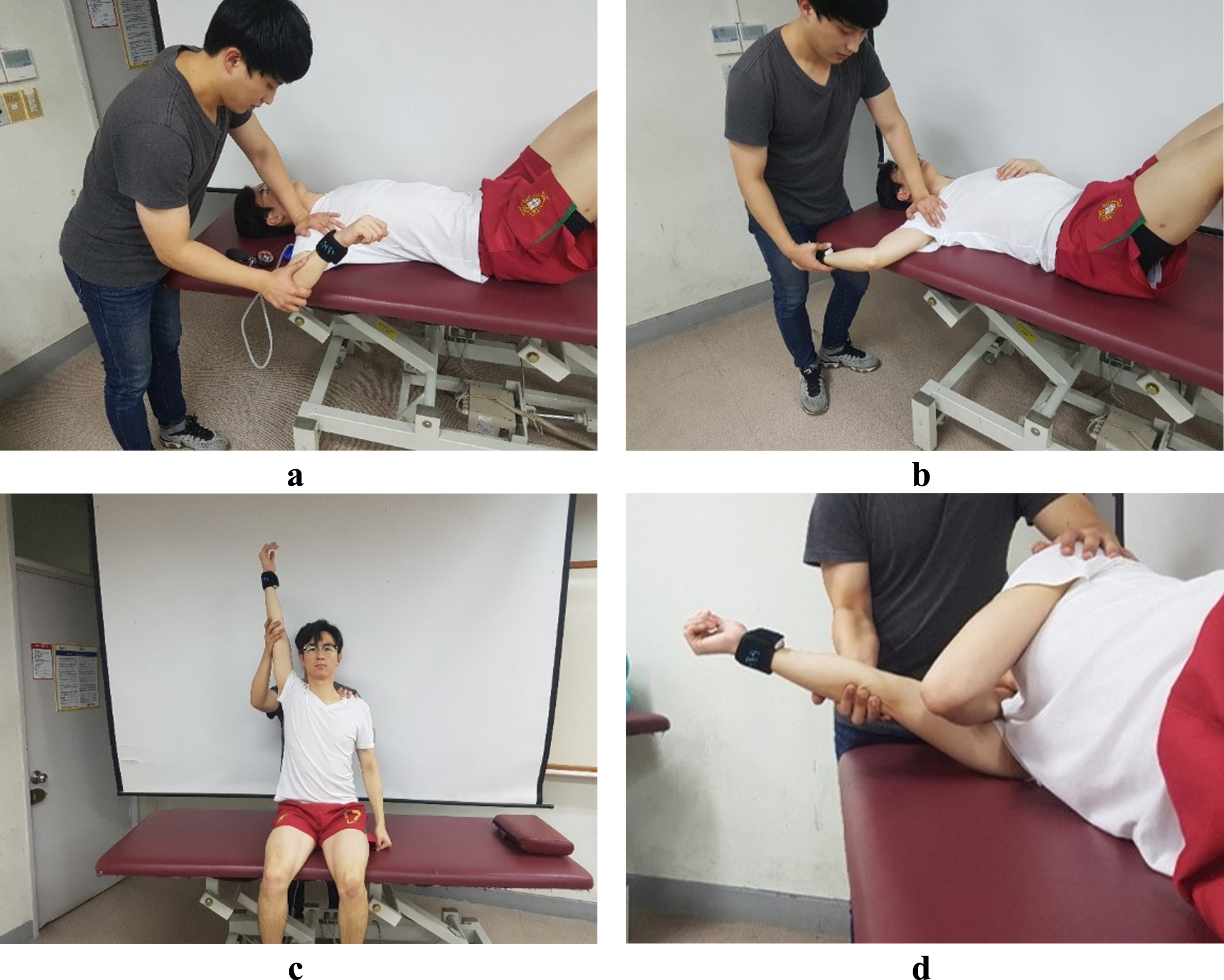
Measurement of shoulder ROM: a) shoulder internal rotation; b) shoulder external rotation; c) shoulder abduction; d) shoulder horizontal adduction.
To measure the isometric strength of SIR, subjects were asked to maintain the shoulder in the neutral position and flex the elbow at 90° in a side-lying position with the test arm facing the table. Then, the wrist of the subject was moved toward the ceiling, and SIR was performed with the maximum force. To measure the maximal isometric strength of SER, subjects flexed their shoulder and elbow at 90° in a side-lying position with the test arm facing the ceiling. Then, the wrist of the subject was moved toward the ceiling, and SER was performed with the maximum force [32]. To measure the maximal isometric strength of EF, each subject was asked to sit in an upright position at the edge of a table. The examiner adjusted the length of the orthopedic belt to 90° of EF and the subjects performed EF against a strap [33]. The maximal isometric strength of the SDA muscle was measured by the subject in a prone position. The subject abducted the shoulder at 120°, fully extended the elbow joints, and rotated the shoulder externally as far as possible. The subject performed the motion by applying the maximum force with the wrist directed toward the ceiling [34]. The maximal isometric strength of SP was measured in the supine position. The subject flexed the shoulder joint at 90° and held the handle, which was set perpendicular to the ground. The subject performed SP with the maximum force toward the ceiling [33] (Fig. 3).
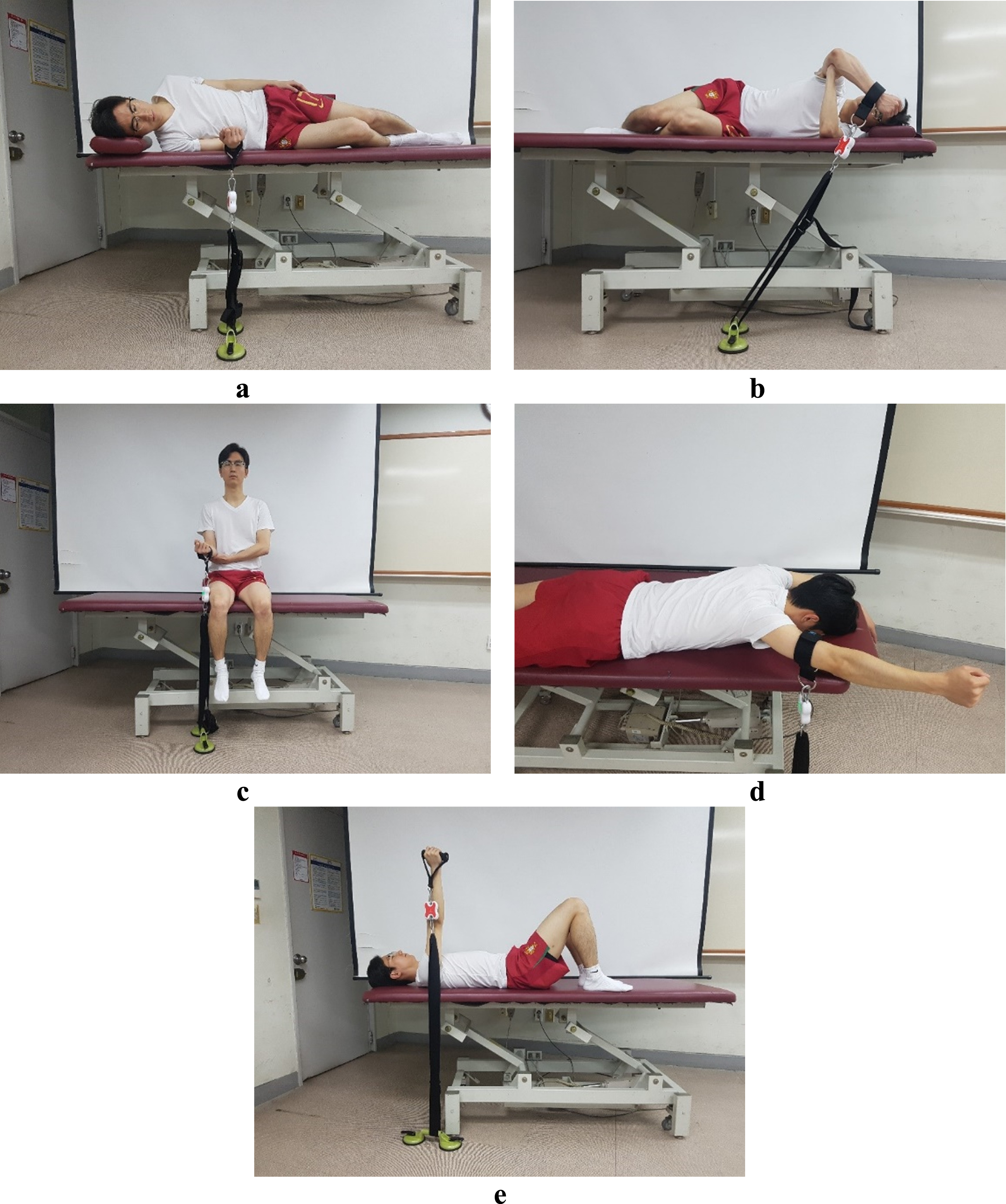
Measurement of shoulder muscle strength: a) shoulder internal rotation; b) shoulder external rotation; c) elbow flexion; d) scapular depression and adduction; e) scapular protraction.
All data were tested for normal distribution by using the Kolmogorov–Smirnov normality test and assumptions for parametric testing were verified (homogeneity of variance assumptions). MANOVA analysis was conducted to compare the functional outcome measure scores on the SPADI, DASH, VAS, EWPS, and BDI, as well as shoulder ROM, muscle strength, and asymmetry ratio between both groups. MANOVA was conducted with subsequent multiple pairwise comparison tests using Bonferroni adjustment of a 0.05-alpha level to control for type I error. All analyses were conducted using SPSS 25.0 (SPSS Inc., Chicago, IL, USA).
Results
Shoulder function, pain, productivity, and depression
Regarding shoulder function, the workers with SPS perceived higher levels of disability through SPADI (p = 0.001) and DASH (p = 0.001) scores than the workers without SPS. The average SPADI score of workers with SPS was 47.78, higher than that of workers without SPS of 28.08. The average DASH score of workers with SPS was 32.24, which was higher than that of workers without SPS, 18.59. The workers with SPS perceived higher levels of pain through VAS (p = 0.001) than the workers without SPS. The average VAS score of workers with SPS was 54.43, which was higher than that of workers without SPS of 28.69. However, there was no difference in productivity through EWPS (p = 0.456) and severity of depression through BDI (p = 0.307) between workers with and without SPS (Table 2).
Comparison of SPADI, DASH, VAS, EWPS, and BDI scores between the two groups
Comparison of SPADI, DASH, VAS, EWPS, and BDI scores between the two groups
SPADI: Shoulder pain and disability index. DASH: Disability of arm, shoulder, and hand. EWPS: Endicott work productivity scale. BDI: Beck depression inventory. *The mean difference is significant at the 0.05 level.
Workers with SPS had more reduced SIR (p = 0.001) and SAB (p = 0.002) ROM than workers without SPS. The SIR ROM of workers with SPS was 43.25°, which was lower than 57.10° of workers without SPS, and the SAB ROM was 146.38°, which was lower than 162.58° of workers without SPS. However, there was no difference in SER (p = 0.378) and SHA (p = 0.452) ROM (Table 3).
Comparison of shoulder ROM between the two groups
Comparison of shoulder ROM between the two groups
SIR: Shoulder internal rotation. SER: Shoulder external rotation. SAB: Shoulder abduction. SHA: Shoulder horizontal adduction. *The mean difference is significant at the 0.05 level.
Workers with SPS had lower maximal isometric strength of SIR (p = 0.012) than workers without SPS. The SIR muscle strength of workers with SPS was 1.53 Nm/kg, which was lower than that of workers without SPS of 1.88 Nm/kg. but there was no difference in SER (p = 0.067), EF (p = 0.315), SDA (p = 0.121), SP (p = 0.375) strengths (Table 4).
Comparison of shoulder muscle strength between the two groups
SIR: Shoulder internal rotation. SER: Shoulder external rotation. EF: Elbow flexion. SDA: Scapular depression and adduction. SP: Shoulder protraction. *The mean difference is significant at the 0.05 level.
In the asymmetry ratio, the workers with SPS showed higher SIR (p = 0.015), SER (p = 0.005), and EF (p = 0.008) asymmetry ratios than the workers without SPS. The asymmetry ratios of SIR, SER, and EF muscle among workers with SPS were 10.17 %, 9.05%, and 6.8%, respectively, which were higher than -0.62%, 0.93%, and 1.36% of workers without SPS. However, there was no difference in the asymmetry ratios of SDA (p = 0.377) and SP (p = 0.333) (Table 5).
Comparison of asymmetry ratios of shoulder muscle strengths between the two groups
SIR: Shoulder internal rotation. SER: Shoulder external rotation. EF: Elbow flexion. SDA: Scapular depression and adduction. SP: Shoulder protraction. *The mean difference is significant at the 0.05 level.
In this study, we investigated the difference in shoulder ROM, muscle strength, asymmetry ratio, shoulder function, psychological factors, and productivity between workers with and without SPS. According to our results, as our hypotheses, workers with SPS had high pain and decreased shoulder function, but there were no differences in psychological factors and productivity. Also, it was observed that the shoulder ROM of workers with SPS decreased in the SIR and SAB motions, but there was no difference in the rest of the motions. In addition, there was no difference in muscle strength in the rest of the muscles except for SIR. The asymmetry ratios in SIR, SER, and EF strength were greater in workers with SPS.
SPADI, DASH, VAS scales were significantly higher in workers with SPS than in workers without SPS. The workers with SPS found it more difficult to perform upper limb movements in their daily lives due to pain than the workers without SPS. However, the EWPS and BDI scores of the workers in the two groups did not differ significantly. EWPS is a productivity questionnaire that tests physical, psychological, and sociological factors, such as attendance, quality of work, performance capacity, as well personal factors, such as social, mental, physical, and emotional states [27]. Therefore, we can consider that there were no differences in work attitudes or individual psychological and emotional states that could affect productivity during work between workers with and without SPS.
SPS is commonly associated with limited ROM [6, 36]. According to Endo et al., SPS caused a significant reduction in SAB ROM. Our study also showed that the average SAB in the frontal plane for workers with SPS was 148°, which is significantly lower than the average SAB angle of 170° for workers without SPS. Joung et al. found that SPS patients exhibited decreased SHA ROM due to shortening of the posterior deltoid muscle and tightness of posterior capsule. Also, Tyler et al. reported that patients with SPS in their dominant arm or non-dominant arm exhibited posterior capsule tightness and reduced SIR ROM compared to normal subjects. These findings suggested that SPS patients lose SIR ROM in their involved arm because of posterior capsule tightness [2]. Similarly, in this study, workers with SPS exhibited significantly reduced SIR ROM compared to workers without SPS. However, the present study did not find a significant difference in SHA ROM between the workers with and without SPS. Tyler et al. fixed the scapula of the arm to be measured directly with the examiner’s hand and then measured SHA ROM to examine posterior capsule tightness. However, since we measured SHA ROM with the arm to be measured on the table and passively fixing the scapular to the table, there may not have been any difference between the workers with and without SPS [31]. Furthermore, the SER ROM of the dominant arm of SPS patients did not decrease, but the SER ROM of the non-dominant arm of SPS patients decreased [2]. This decrease to reduced demand on the non-dominant arm to perform day-to-day activities [2]. Our study also showed no significant difference between the workers with and without SPS because most of the workers in the SPS group had impingement in their arms on the dominant side.
Muscle weakness is considered common clinical feature in SPS [9, 38]. Leroux et al. found that the SIR strength of the involved arm of SPS patients in the sitting position with 45° abduction and 30° flexion was reduced by 48–53% compared to the dominant arm of the subjects in the control group. In addition, several studies have suggested that SER muscle weakness may contribute to SPS [40, 41]. However, according to Erol et al., there was no difference in SER muscle strength between subjects with and without SPS. Also, according to Leroux et al., the degree of decrease in the SIR strength of SPS patients was relatively higher than the degree of decrease in SER strength. However, in this study, there was a significant difference in SIR strength between the two groups, but not a significant difference in SER strength. Cools et al. found that overhead athletes with SPS had a significant difference in the strength of SP muscle on the injured side compared with the dominant side of a healthy group. Also, Cools et al. found significantly lower SDA muscle (lower trapezius) activity when overhead athletes with SPS performed isokinetic abduction at 120°/s. Unlike athletes, who mainly perform overhead activities such as throwing or wielding a tennis racket, workers often place their arms under the shoulder level and perform motions for assembly. Therefore, in this study, there would be no difference in the strengths of the SP and SDA muscle, which play the major roles in scapular posterior tilt and upward rotation when raising arms, between the workers with and without SPS. Also, muscle strength varies widely based on physical characteristics, including body weight, height, shape of bone or joint, and psychological characteristics, including cognition, emotion, and motivation [44].
The main findings of this study were that the asymmetry ratios of EF, SER, and SIR are greater in the workers with SPS than those in the workers without SPS. The involved arm of the workers with SPS had upper extremity muscle strength deficits for EF, SER, and SIR motions compared to the uninvolved arm. The relative strength deficits of EF, SER, and SIR upper extremity strength of the involved arm may be due to the following reasons. The subscapularis is one of the muscles that rotates the head of the humerus internally, creating a SIR [45]. Richards et al. found that coracohumeral distance, one of the factors contributing to the development of SPS, was significantly reduced in patients requiring subscapularis repair surgery. In other words, a narrowed coracoid distance is one of the possible causes of subscapularis injury. Reddy et al. reported that subscapularis muscle activity was significantly decreased in 30°-60° of scaption in patients with SPS compared to those in the normal group. Therefore, decreased subscapularis muscle activity along with the possibility of a damaged subscapularis due to narrowed coracohumeral distance probably contributed to the decreased in the SIR strength of the involved arm with SPS and the high asymmetry ratio of SIR in the workers with SPS. Also, infraspinatus and teres minor fatigue among SER muscles can cause SPS by reducing the scapular posterior tilt movement during arm raising [35]. In addition, infraspinatus muscle activity was shown to be decreased between 30 and 90 degrees during scaption [47]. Although SER strength did not differ between the workers with and without SPS, due to fatigue or poor infraspinatus and teres minor muscle activity, the asymmetry ratio of SER muscle strength was significantly higher in the workers with SPS than that in the workers without SPS. Similarly, we found no difference in EF muscle strength between the workers with and without SPS, but the workers with SPS exhibited significantly higher asymmetry ratios of EF muscle strength than the workers without SPS. The long head of the biceps brachii is a depressor of the humeral head that prevents SPS when it functions properly during arm elevation [5]. When this muscle lacks strength or does not function properly, the humeral head is not depressed, which increases the likelihood of SPS development. Also, tendinitis of the long head of the biceps brachii is a common problem associated with SPS or rotator cuff tearing [48, 49]. In particular, Neer reported that most biceps tendinitis is caused by SPS. Thus, pain due to biceps tendinitis associated with SPS can be thought to contribute to muscle strength deficit on the involved side of the elbow flexor compared to the uninvolved side.
There were some limitations to this study. First, since all assembly line workers in this factory were male, this study was conducted only with male workers. For this reason, the results of this study cannot be generalized to all genders. Second, because it is aimed at adults who are currently engaged in vocational activities, it cannot be generalized to adolescents or the elderly. Third, because the study involved workers working in assembly lines, it is not possible to generalize these results to office workers who do not have a heavy load on their shoulder or to athletes who repeatedly perform certain motions.
Conclusion
Among workers who work on assembly lines that mainly perform repetitive motions and handle heavy loads, workers with SPS were found to have reduced shoulder function due to pain when performing daily activities. However, there was no decrease in productivity or changes in psychological factors such as depression. Also, workers with SPS had clear deficits in SIR, SAB shoulder ROM and SIR muscle strength. However, workers with and without SPS differed only in SIR strength, but in workers with SPS, the asymmetry ratios between the involved arm and the uninvolved arm were greater in SIR, SER, EF strength than those without SPS. Therefore, the asymmetry ratios of SIR, SER, EF muscle strength are good comparable factors for workers with and without SPS. The asymmetry ratios of shoulder muscle strengths could provide an important baseline comparison for the workers with SPS. In addition, these deficits support the need for exercises to restore the range of motion of specific shoulder movements and muscle strengths, especially to reduce the asymmetry ratio by strengthening relatively weakened muscles in workers with SPS.
Ethical approval
The present study was approved by the Institutional Review Board of Yonsei University, Seoul, South Korea (approval no. 1041849-201710-BM-112-02).
Conflict of interest
We wish to confirm that there are no known conflicts of interest associated with this publication and there has been no significant financial support for this work that could have influenced its outcome.
We confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. We further confirm that the order of authors listed in the manuscript has been approved by all of us.
We confirm that we have given due consideration to the protection of intellectual property associated with this work and that there are no impediments to publication, including the timing of publication, with respect to intellectual property. In so doing we confirm that we have followed the regulations of our institutions concerning intellectual property.
We further confirm that any aspect of the work covered in this manuscript that has involved either experimental animals or human patients has been conducted with the ethical approval of all relevant bodies and that such approvals are acknowledged within the manuscript.
We understand that the corresponding author is the sole contact for the editorial process (including Editorial Manager and direct communications with the office). He is responsible for communicating with the other authors about progress, submissions of revisions and final approval of proofs. We confirm that we have provided a current, correct email address which is accessible by the corresponding author, and which has been configured to accept emails from
Footnotes
Acknowledgments
Not applicable.
Funding
Not applicable.