
Abstract
BACKGROUND:
Laboratory– related musculoskeletal disorders (LMSDs) are injuries resulting from working in the laboratory. Biomedical scientists (BMSs) play an important role in any health care system. However, they are at high risk of exposure to the LMSDs.
OBJECTIVE:
This study aimed to estimate the prevalence and the associated risk factors of LMSDs among this group of healthcare professionals.
METHODS:
We conducted a cross-sectional survey using the Nordic Musculoskeletal Questionnaire to estimate the prevalence of the LMSDs among the BMSs. BMSs with occupational or non-occupational accidents that affected their musculoskeletal system were excluded from the study. A Chi-square test was performed to measure the significant association between different risk factors (age, gender, weight, height, nationality, specialty, educational level, nature of the job, and the number of experience years) and the prevalence of the LMSDs among the BMSs.
RESULTS:
The study included 83 BMSs. Females represented 63.9% and 36.1% were in the age group of 35– 44. The overall prevalence of the LMSDs was 77.1%. The most prevalent LMSDs were neck, shoulders, and lower back with 50.6%, 49.4%, and 43.4%, respectively. A total of 65.57% of BMSs had irregular symptoms of LMSDs.
CONCLUSION:
The study found that the prevalence of LMSDs among the BMSs was high. Good practice and training in ergonomics may minimize the prevalence of LMSDs among the BMSs.
Introduction
Musculoskeletal disorders (MSDs), known as cumulative trauma disorders or repetitive stress injuries, are injuries to muscles, nerves, tendons, ligaments, joints, cartilage, and spinal discs [1]. Whereas the work-related musculoskeletal disorders (WMSDs) are conditions in which the work environment and performance of work contribute significantly to the condition, and/or the condition is made worse or persists longer due to work conditions [2]. To the best of our knowledge, we are the first to introduce the term laboratory-related musculoskeletal disorders (LMSDs), which can be defined simply as injuries resulting from working in thelaboratory.
Biomedical scientists (BMSs) play an important role in any health care institution. They work in medical laboratories, where specimens are prepared and processed for the detection, diagnosis, and treatment of various diseases. BMSs are professionals that identify pathogenic microorganisms in microbiology, measure chemicals in biochemistry, match blood samples in hematology, help to diagnose cancer samples in histopathology, recognize antigen molecules in immunology, detect gene variants in genetics, and others. However, in a medical laboratory, they are exposed to repetitive activities such as microscopy, microtomy, pipetting, and mostly work in standing positions. With time, repetitive motion can affect muscles, joints, tendons, and nerves [3]. The long-term and severe LMSDs can highly affect the productivity of the work and shortness the work duration, therefore this will eventually lead to occupational disability and cause a major health challenge for individuals and healthcare systems around the world [4]. About 33% of all sickness absence of health care professionals result from MSDs [5]. MSDs are one of the common health problems among all health professionals [6]. In addition, about 30% of people worldwide have at least MSDs [7].
Few studies are available on the ergonomic hazard which can lead to the LMSDs [8]. Ergonomic is simply the balance between the work requirement and the capacity of the worker [9]. In addition, MSDs studies on certain professionals such as dentists, nurses, and surgeons are well covered, however, data on the prevalence of the LMSDs among the BMSs is scarce. Hence, this study aimed to evaluate the prevalence of LMSDs among the BMSs and assess the risk factors associated with the BMSs.
Material and methods
Study design
This is a cross-sectional observational study that was conducted in 2020. The study is ethically approved. Preceding the study, a detailed procedure of the study was explained, and a voluntary consent form was also signed by each participant before the study. BMSs with occupational or non-occupational accidents that affected their musculoskeletal systems were excluded from the study.
Sample size
Currently, there is no available information on the proportion of MSDs among the BMSs. Hence, a pilot study was conducted among 20 participants who fulfilled the research criteria. Those who participated in the pilot study were excluded from the study. The sample size was calculated as 97. After sampling, the number was increased to 15% to avoid non-response or inappropriately filled questions and that number was randomly selected from the overall population. The Cronbach’s alpha reliability of the questionnaire was 0.675.
Data collection
The survey included two main sections. The first section was used to obtain characteristics such as age, gender, weight, height, nationality, specialty, educational level, nature of the job, and the number of experience years. The second section was from a previously validated Nordic Musculoskeletal Questionnaire [10]. This section was used to assess the prevalence of MSDs among the participants. The first two questions were about the health status of the participants and whether they had any occupational or non-occupational accidents that affected their musculoskeletal systems. Therefore, those who answered yes to these two questions were excluded because they did not fulfill the research criteria. The participants were asked in this section if they experienced any pain in different nine anatomical regions of the body, specifically in the neck, shoulder, upper back, elbows, lower back, wrists/hands, hips/thighs, knees, and feet/ankles in the last year preceding the survey and in the last seven days before the study. Further, the participants were asked in this section if they visited a physiotherapist or were prevented from doing work due to any pain in the same nine regions mentioned above. There was a diagram to show these body sites for clarification to the participants. The section also includes questions about the intensity, frequency, and duration of the pain related to any musculoskeletal injuries.
Data analysis
The data were analyzed using Statistical Package for Social Science (SPSS) version 25 software (SPSS Inc., Chicago, USA). Frequencies and percentages were used to represent the categorical data such as age, gender, and specialty. Continuous data were presented as a mean and standard deviation. A Chi-square test was performed to measure the significant association between different risk factors and the prevalence of the LMSDs among the BMSs. The P-value was considered significant if it was equal to or less than 0.05.
Results
A total of 114 BMSs participated in the study. However, 31 BMSs were excluded because they did not fulfil the research criteria. Therefore, a total of 83 BMSs were included in this study and 78.3% were Omani. The vast majority were females (63.9%) and 75.9% were married. The majority of the BMSs participants (36.1%) were in the age group of 35–44. The average of the total working years as BMSs was 11.52(±7.78) and the average of their total working years in SQU or SQUH was 9.89(±7.40). The hematology department distributed 28.9% of BMSs, followed by biochemistry with 22.9% and histopathology with 18.1%. Nearly half of the BMSs (48.8%) were juniors and 65.1% had a degree qualification.
Their average body mass index (BMI) was 25.3(±4.6). More than half of the participants (53.0%) did regular physical exercises. Almost all the participants are right-handed (94.0%). More than half (73.2%) of the participants worked while they were standing, and half of them (50.1%) worked while they were sitting. 56.1% of the BMSs worked in pipetting, 39.0% in microscopy, and 15.9% in microtomy. A total of 60.2% BMSs were sometimes stressed at work, 50.0% were sometimes working overtime, and 79.0% did not have heavy work at home (Table 1).
Demographic data of biomedical scientists
Demographic data of biomedical scientists
BMI: Body mass index.
The overall prevalence of the LMSDs among the BMSs in the last 12 months in any part of the body was 77.1%. Neck complaints were the highest; 50.6% and 25.3% in the last 12 months and 7 days, respectively. Followed by shoulders complaint 49.4% and 16.9%, lower back complaint 43.4% and 15.7%, upper back compliant 34.9% and 14.5%, knees compliant 30.1% and 8.4%, ankle or feet 26.5% and 4.8%, wrists or hands 24.1 % and 4.8%, respectively. Elbows complaint was the lowest in both periods, 9.6% and 2.4% followed by thighs or hip complaints, 10.8%, and 3.6%, respectively (Fig. 1). A total of 65.57% of the BMSs had irregular symptoms of the LMSDs, 54.10% experienced moderate pain due to these symptoms, and 44.26% had symptoms that persisted from hours to days (Fig. 2).
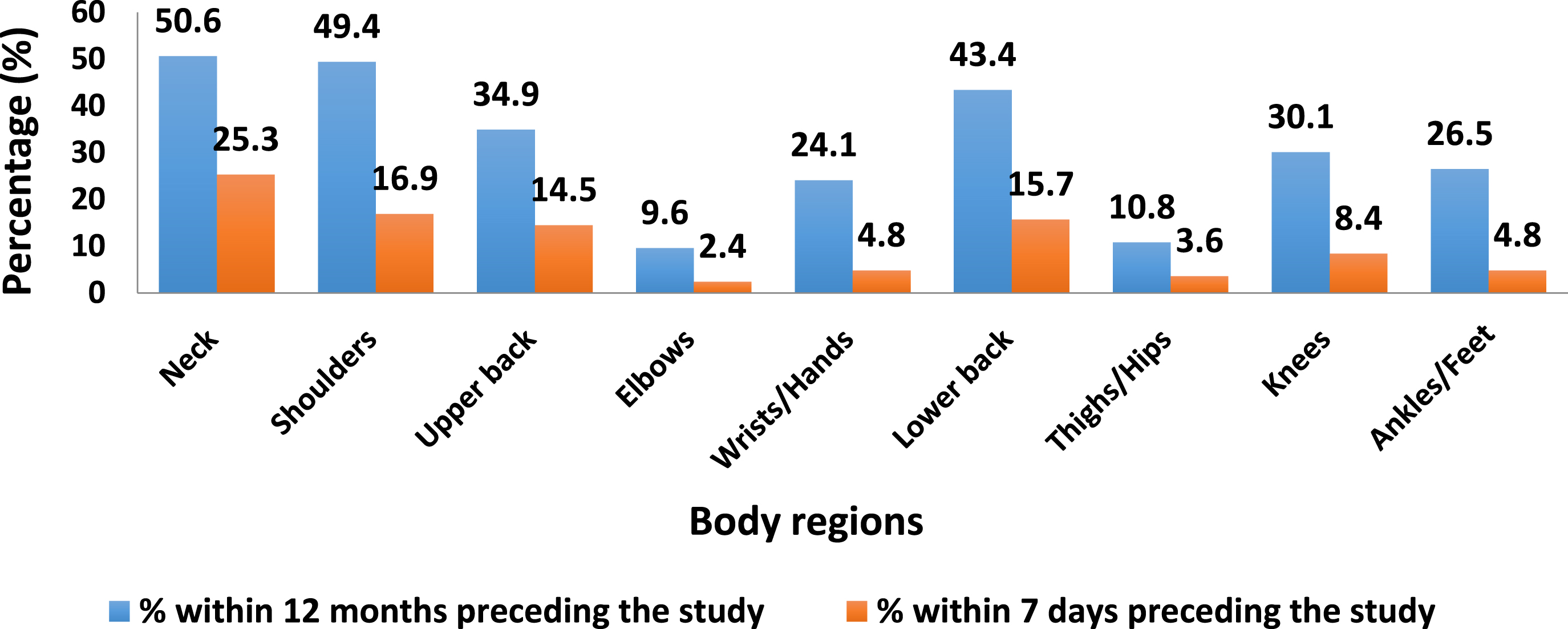
Comparison between the prevalence of the laboratory-related musculoskeletal disorders among the biomedical scientists in the last 7 days and 12 months preceding the study.
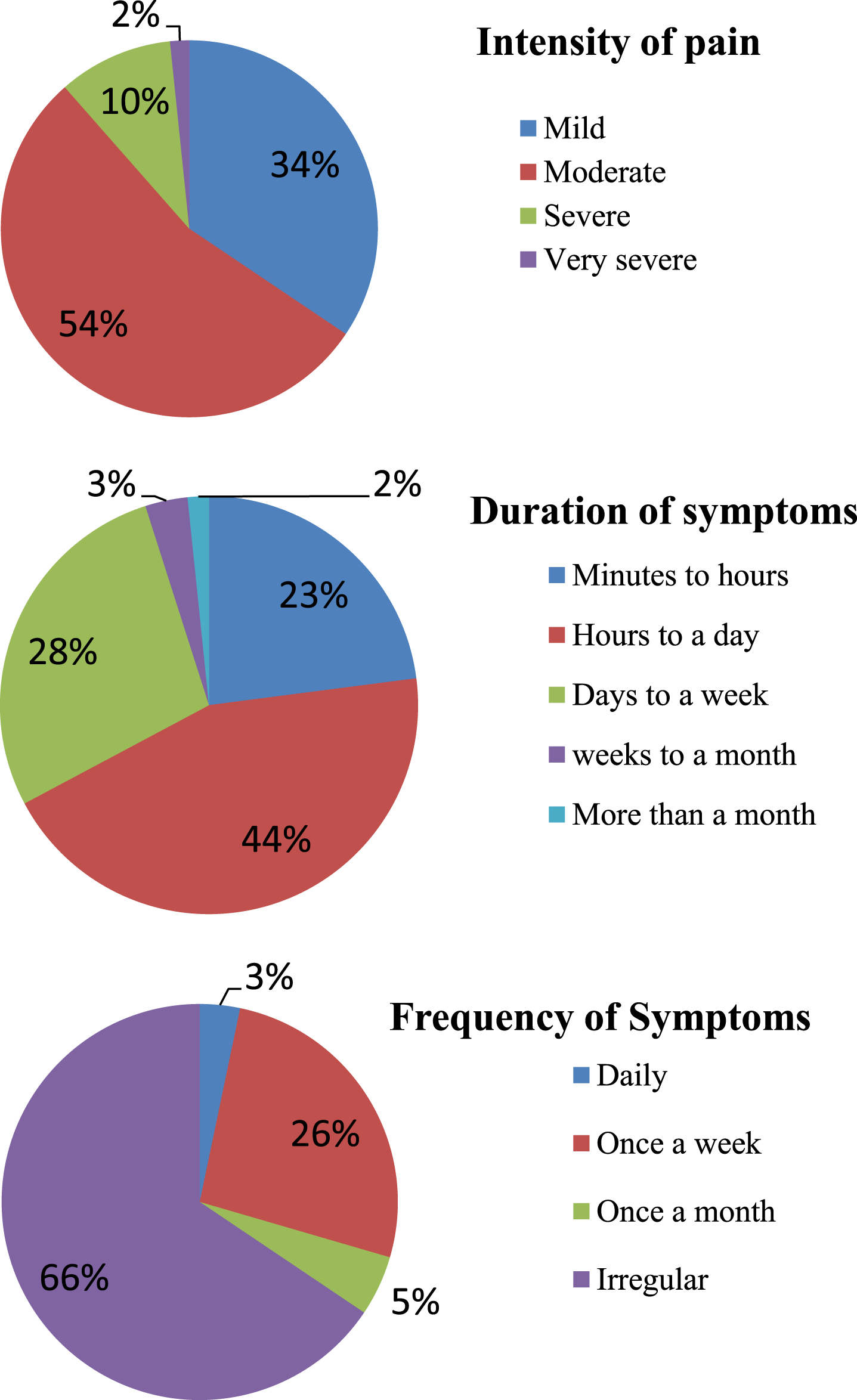
Pain and symptoms characteristics of the laboratory-related musculoskeletal disorders experienced by the biomedical scientists working within 12 months preceding the study.
In the last 12 months, 19.3% BMSs, followed by 14.5%, 13.3%, and 13.3%, were prevented from doing work at home or away from home due to the lower back, neck, shoulder, and upper back complaints, respectively. Among the BMSs who visited a doctor or physiotherapist regarding their complaints in the last year, 13.3% were due to lower back complaints, 8.4% due to neck complaints, and 7.2% due to elbows complaints (Table 2).
Biomedical scientists who were prevented from doing work and visited a doctor regarding their complaints within 12 months
There was no significant association between age and marital status and the LMSDs among the BMSs. However, there was a significant association between the neck and upper back complaints in the female gender (Table 3). In addition, no significant association was found between nationality, designation, and degree of qualification with the LMSDs among the participants. None of the complaints were significantly associated with the dominant hand, BMI, and regular physical exercises (Table 4). Heavy work at home was significantly associated with a lower back complaint. There was no significant association between working overtime and stress at work with the LMSDs in this study (Table 5). Regarding the nature of the job, shoulder complaint was significantly associated with microscopy and pipetting. Lower back complaints show a significant association with pipetting (Table 6).
Prevalence and association of the laboratory-related musculoskeletal disorders with age, gender, and marital status of the biomedical scientists within 12 months
Prevalence and association of the laboratory-related musculoskeletal disorders with dominant hand, body mass index, and physical exercises of the biomedical scientists within 12 months
BMI: Body mass index.
Prevalence and association of the laboratory-related musculoskeletal disorders with the working overtime, heavy work at home, and stressed at work among the BMSs within 12 months
Prevalence and association of the laboratory-related musculoskeletal disorders with the nature of the job of biomedical scientists within 12 months
NA: Not applicable.
In the present study, the overall prevalence of LMSDs among BMSs was 77.1%. This finding is higher than similar two studies, one was in Iran, which reported 72.4% MSDs among medical laboratory workers [11]. The other one was in India which found that the overall prevalence of MSDs among medical laboratory technicians was 73.3% [8]. In addition, our finding is higher than those who work in three specialized healthcare centers (Cardiovascular Laboratory, Nuclear Radiology, and General Radiography) in Malaysia, where the overall prevalence of MSD in all three departments was 70.6% [12]. However, our finding is lower than a recent study in Saudi Arabia which reported 82% MSDs among medical laboratory workers [13]. The most prevalent LMSDs among the BMSs were neck followed by shoulders and lower back with 50.6%, 49.4%, and 43.4%, respectively. This finding is in line with another study conducted in Metropolitan Washington, which found that neck complaint (61.5%) was the most prevalent symptom. However, their study also found that the wrists/hands (56.4%) symptoms were also high among their participants. This could be because their study only involved cytotechnologists who deal more with microscopes, and frequently use their hands/wrists to adjust the microscope knob [14]. Similar findings also reported that the neck (55–60%), followed by upper back (53%), and lower back (57%) were the most prevalent MSDs among the cytotechnologist [15]. In addition, similar findings were reported among the laboratory technicians which found that the neck was the most prevalent MSD [3, 17]. Another two studies, which used pathologists as target professionals, found that the neck was the most prevalent MSD [18, 19]. A recent study in Turkey showed that the neck (73.4%), followed by the shoulder (56.3%) and elbow (14.6%) were the highest musculoskeletal complaints that occurred in the healthcare workers during the COVID-19 pandemic in the last 12 months [20].
In contrast with our findings, a similar study was conducted in India, which included medical laboratory technicians from different departments such as pathology, microbiology haematology, histology, and biochemistry. They found that the lower back complaint (32.5%) was the most prevalent followed by knees (20.7%) [21]. Another similar study conducted in Ethiopia revealed that ankles/feet (21.7%) and knees (20.8%) were the most affected parts [3]. In addition, two similar studies in Sadia Arabia and Iran found that the lower back was the most prevalent MSDs among clinical laboratory workers [11, 13].
The finding of our study could be explained by the fact that the BMSs work with different procedures and deal mostly with specimens that require the use of microscopes. Therefore, they used to bend their neck for a long time. Further, they work with static or repetitive tasks without relaxing their arms. This may explain the reasons for their shoulders complaints. The high prevalence of lower back complaints could be due to nonadjustable chairs with unsupported back posture available in their workstations. Another factor that might be a reason for the lower back complaint is the job nature, in which the BMSs work for a long time while they were standing without back support. In the current study, the BMSs reported that their symptoms of the LMSDs occurred irregularly (Fig. 2). This finding is also consistent with another similar study [14].
Some risk factors such as increasing the age of the medical laboratory technicians and worsening the working conditions as well as standing and sitting for long hours were found to be associated with the development MSDs among the medical laboratory workers [3]. The current study found no statistically significant association with age, marital status, nationality, dominant hand, BMI, degree of qualifications, and working overtime. Similar findings were also reported [8]. Usually the BMSs work in multitasking jobs in which they move from one workstation to another. Therefore, they were able to avoid postural stress. Thus, this might explain the reasons for no significant association between age and MSDs [8].
The female gender showed a significant association with neck and upper back symptoms among the BMSs (Table 1). This finding agrees with another similar study [8]. In contrast, another study found that the female gender had no association with neck complaints [11]. In general, the prevalence of MSDs was found to be more common among women rather than men [22]. A study conducted in Amsterdam also found that female workers are at high risk to develop MSDs in the upper extremity [23]. There were several explanations for this gender difference. One of these explanations is the biological differences between females and males. For example, both genders can expose to the same physical work demands, however, they have different maximal physical work capacities. In addition, many workstations or tools are not taking into account the anthropometric differences between the two genders. Furthermore, it is suggested that the female reproductive system and, the use of oral contraceptives, during pregnancy, and childbirth can explain the high risk of MSDs among females. However, the precise mechanism is still not explored [23].
In the current study, pipetting showed a significant association with shoulders and lower back complaints. This is consistent with another study that found increasing pipette work was associated with an increase in shoulder complaints among the laboratory technicians [24]. The significant association between pipetting and lower back complaints can be explained by the fact that the BMSs did not use back supports while pipetting. Furthermore, our findings showed a significant association between microscopy and shoulder complaints. This may be due to the increased stress of the shoulder ligaments while using the microscope for a long time.
The present study found that there was a significant association between the LMSDs specifically the lower back complaints and the heavy work at home. This agreed with a similar study in which heavy work at home was also significant with the MSDs but with wrists/hands [11]. However, both studies found that there was no significant association between stress at work and the MSDs in the medical laboratories.
Limitations
Several limitations of our study are worth noting. First, due to the COVID-19 pandemic, we were not able to spread the questionnaire face to face to the BMSs. Therefore, we were incapable to provide more explanations about questions for the participants and encourage them to participate. Second, the study was restricted to the BMSs from a single hospital and university, even though this hospital serves as a tertiary referral hospital in Oman and the university is the national university of the Sultanate of Oman. Finally, the study did not distinguish if those LMSDs were partially or fully related to the instruments and machines used in different laboratories.
Conclusions
The current study provides evidence that the prevalence of LMSDs among the BMSs is considerably high. The most affected parts were the neck, followed by the shoulder and lower back. The study also found that the prevalence of the LMSD was associated with female gender, pipetting, microscopy, and heavy work at home. It is recommended that good practice and training of ergonomics in the medical laboratories may minimize the prevalence of LMSDs among the BMSs.
Ethics statement
The study was approved by the Medical Research Ethics Committee, College of Medicine and Health Sciences, Sultan Qaboos University, Oman (SQU-EC/095/2020). Preceding the study, a detailed procedure of the study was explained and a voluntary consent form was also signed by each participant before the study.
Conflict of interest
The authors report no potential competing interests.
Footnotes
Acknowledgments
The authors would like to thank all biomedical scientists at the College of Medicine and Health Sciences and Sultan Qaboos University Hospital who participated in this study.
Funding
Not applicable.