
Abstract
BACKGROUND:
Complex behaviors, such as physical activity (PA), may be related to different levels of influence.
OBJECTIVE:
To analyze the role of social support, mood and alcohol consumption as psychosocial predictors on the engagement in PA among Brazilian workers.
METHODS:
This is a quantitative, cross-sectional analytical study. A sample of 395 participants answered a sociodemographic questionnaire, the Alcohol Use Disorder Identification Test (AUDIT), the Baecke Habitual Physical Activity Questionnaire, the Social Support Scale for Physical Activities (SSSPA) and the Brunel Mood Scale (BRUMS).
RESULTS:
Analysis via Pearson’s Correlation Test indicated a negative correlation between PA and depression and fatigue, and a positive correlation between PA and alcohol consumption, vigor and the four variables of social support (support of family members for walking; support of friends for walking; support of family members for moderate and vigorous physical activity; support of friends for moderate and vigorous physical activity). A positive relationship between PA and low-risk alcohol consumption was also identified. A hierarchical multiple regression analysis showed that family support for walking, friends support for moderate and vigorous physical activity, vigor and alcohol consumption are predictors of PA. Hayes’ moderation analysis indicated that social support has a moderating effect on the relationship between alcohol use and PA.
CONCLUSION:
Different factors may be involved in engaging in PA. A broader approach that addresses the singularities of individuals, especially in actions for different patterns of alcohol consumption, is recommended.
Introduction
Physical activity (PA) is an important aspect for maintaining the individual’s physical and mental health [1–5], however the majority of the population does not engage in such activity at levels recommended by health agencies [1–5]. Therefore, economically active individuals constitute a priority subgroup for research on this topic, in view of the impact that unhealthy lifestyles and behaviors have on health, work capacity and on levels of absenteeism [6, 7].
The adoption of healthy lifestyle is a complex process that involves countless factors in peoples’ lives. In this context, the socioecological model describes that a behavior has different levels of influence such as intrapersonal, interpersonal and environmental factors [8]. Recent literature that investigated factors associated to PA among workers has focused mainly on intrapersonal factors such as sociodemographic characteristics, tobacco usage, work satisfaction, anxiety, burnout, stress, and self-efficacy [9–17].
In addition, some aspects of interpersonal level, such as the institution’s incentive and the support received by colleagues and family members, have been configured as strategic elements for engagement in PA [14–17]. However, these studies were carried out in developed countries and done with specific groups of workers. Thus, addressing psychosocial predictors among low and middle-income countries is important in planning tailored interventions.
In the present study, we choose to explore intrapersonal and interpersonal correlates of PA, which are characterized as variables of interest to workers’ health and which can be managed by health interventions. In this sense, we proposed to consider mood, a variable associated with psychological well-being and mental health protection [18]; the usage of alcohol, because it is a factor that, when excessively, can lead to health complications and work performance [19]; and social support as it is widely studied and pointed out as a protective factor for various aspects of health [20]. We hypothesized that workers who consumed less alcohol and showed more perception of social support and positive mood would engage in more PA.
Thus, the aim was to analyze the role of social support, mood and alcohol consumption as psychosocial predictors on the engagement in PA among Brazilian workers. It is expected that the investigation of these elements will provide subsidies for the planning of actions and organizational guidelines for the improvement of PA levels, as well as for the promotion of health and well-being among workers in low and middle-income countries.
Methods
Study design and setting
This was a quantitative, cross-sectional study conducted on the campus of a public university in the interior of the state of São Paulo, Brazil.
Participants, sampling, and procedures
The study population was composed of technical-administrative staff members from different professional categories and sectors, distributed in: a) academic community support (nutrition and food, cultural and sports activities); b) maintenance of structures; c) laboratory support; d) secretary and administrative activities.
The technical-administrative staff members perform fundamental and strategic tasks for the functioning of the institution, although it is not directly related to teaching practices. Considering that these workers have their own regulations with differences on work processes and career plan when compared to the professor’s category, we have chosen to focus only on these workers.
During the development of the study, the campus had 2,075 workers allocated in 10 units, organized in teaching and research or campus management units. The sampling plan adopted was Stratified Random Sampling with proportional allocation by strata, and each one of them was formed by the campus units. For the sample calculation, a 10% relative error and a 5% significance level were adopted. Thus, a minimum sample size of 324 participants was identified.
The eligibility criteria were being a technical-administrative worker on the university campus. Those who were not at the unit during the data collection period and those who were outsourced employees were excluded. Considering estimate numbers of missing and refusals, based on previous study carried in this setting [21], 527 eligible workers were invited; of those, 395 accepted and constituted the final sample, according to Fig. 1.
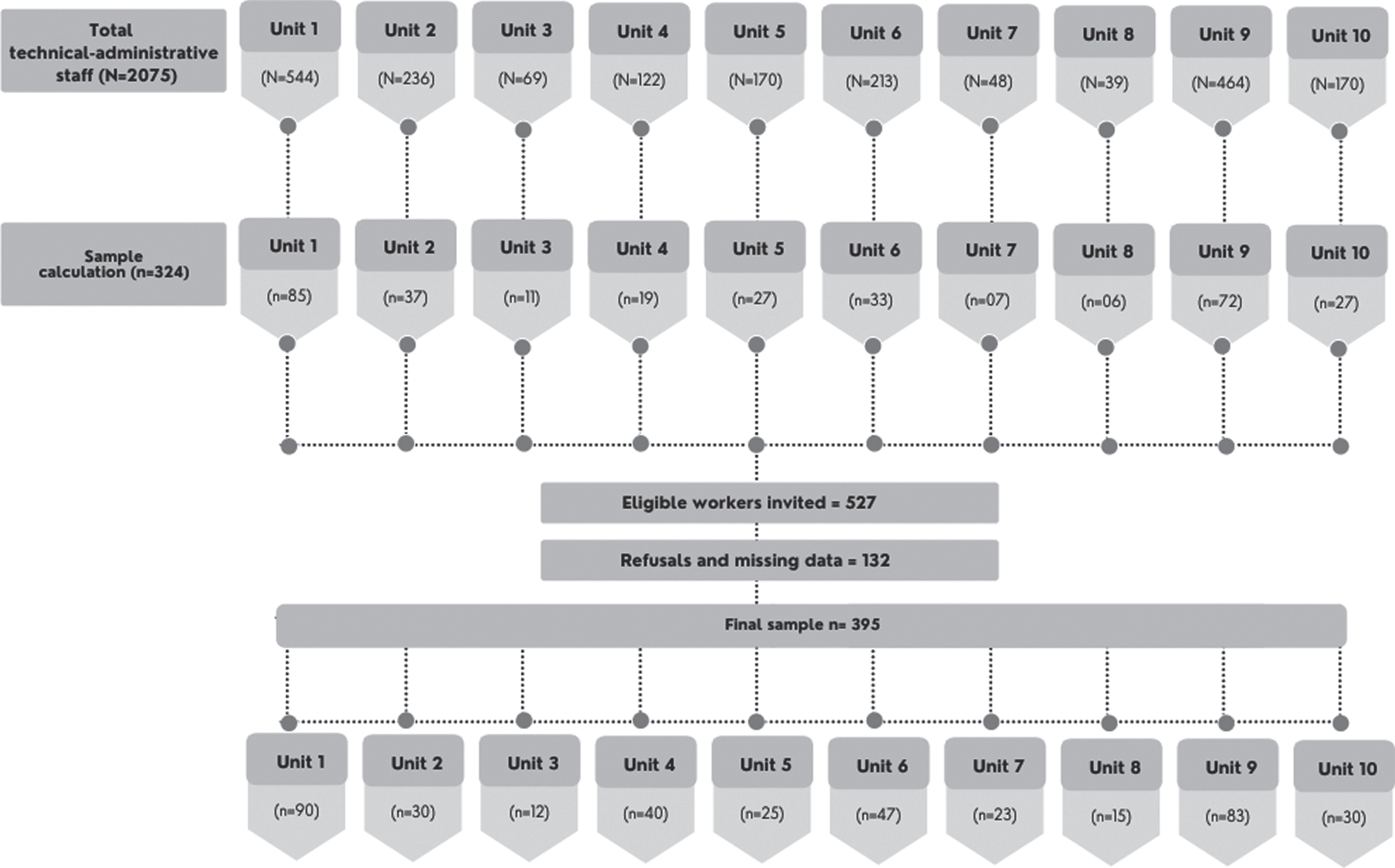
Flowchart of the steps for sample constitution. Brazil, 2018 (n = 395).
Initially, the main researcher, after authorization from the workers’ leaders, made visits to different units to invite the workers to participate in the research. In this approach, a brief presentation of the research was made, including objectives, procedures and ethical aspects.
For those workers who expressed interest, a printed letter of invitation was delivered containing the research design and the informing consent form. After confirmation of consent, an email address was requested to forward the data collection questionnaire. The email message consisted of a brief comment about the study and orientation for the participant to access the link questionnaire available on Google Forms platform. This message was individualized, issued by the main researcher and addressed to a single person.
It is important to highlight that, in some cases, when the participant mentioned having limited access to the internet, an opportune moment was agreed to carry out the collection through a printed form.
Measures
A sociodemographic questionnaire, the Alcohol Use Disorder Identification Test (AUDIT), the Baecke Habitual Physical Activity Questionnaire, the Social Support Scale for Physical Activities (SSSPA), and the Brunel Mood Scale (BRUMS) were used.
Alcohol
The AUDIT, developed by the World Health Organization (WHO), is a 10 item questionnaire that evaluates patterns of alcohol consumption, including frequency, quantity, dependence and consequences. It was translated and validated for the Brazilian population [22, 23]. A total score from zero (0) to 40 is obtained: 0–7 = abstinence or low-risk use; >8 = high-risk use or possible dependence [24].
Physical activity
The Baecke Habitual Physical Activity Questionnaire, developed in the Netherlands by Baecke, Burema, Frijters on 1982 and validated for the Brazilian population by Florindo and Latorre on 2004, is composed of 16 questions, assessing PA in the past 12 months, considering the following dimensions: occupational, locomotion, leisure and structured physical exercises [25, 26]. In the present study, only the total score was adopted, calculated as the sum of scores from different dimensions [26].
Social support
The Social Support Scale for Physical Activities (SSSPA) was developed in English by Sallis et al. (1982) and was validated for the Brazilian adult population by Reis, Reis and Hallal (2011). This scale consists of 12 questions and two dimensions: family and friends who provide support in relation to moderate and vigorous physical activities (MVPA) or walks during leisure time [27, 28]. In each item, respondents must report the frequency in which their supporters “did”, “invited”, or “encouraged” the practice of PA, during the past three months [27].
Each question has three answer options: never (0), sometimes (1) and always (2). The score is calculated from the sum of items in each set and indicates the intensity of support for walking or MVPA [27]. In the present study, the acronyms SFaW were adopted for the support of family members for walking, SFrW for the support of friends for walking, SFaMVPA for the support of family members for moderate and vigorous physical activity and SFrMVPA for the support of friends for moderate and vigorous physicalactivity.
Mood
The Brunel Mood Scale (BRUMS), validated for use in Brazil by Rohlfs et al. 2008 was adapted from “profile of mood states” which was developed in 1971 by Mcnair, Lorr & Droppleman. This scale is consists of 24 items, subdivided into six domains: 1) confusion, 2) depression, 3) fatigue, 4) anger, 5) tension, and 6) vigor [28–30]. The answer options range from zero to five and the score for each domain is obtained from the sum of the scores of each item. The higher the score, the greater the respective moodstate [29].
Analyses
Statistical analyses were performed using Statistical Package for Social Science for Windows®, version 20, for Windows. Correlation between PA scores, social support scores (SFaW, SFrW, SFaMVPA, SFrMVPA), scores for mood factors (confusion, depression, fatigue, anger, tension, vigor) and the AUDIT score were analyzed using Pearson’s Correlation Test.
A hierarchical multiple regression analysis was undertaken to identify the predictors of PA. The selection and order of introduction of the independent variables in such an analysis, for theoretical reasons, began with social support and, subsequently, mood, and alcohol consumption.
Hayes’ moderation analysis [31] was used to test the possible effect of social support on the relationship between PA and alcohol use. The macro PROCESS that was developed by this author and made available for free in SPSS was used. It is a computational tool that simplifies moderation analysis as well as mediation analysis. The data provided in the syntax allowed the construction of a graph of the moderation function, which helped to visualize this effect.
To perform the moderation analysis specifically, social support was categorized as “absent” when the participant did not mention supporters and “present” when any source of support was mentioned (family and/or friends). Thus, for different values (present or absent) of the variable “social support”, variations in the form, strength, or sign of the relationship between PA and alcohol use were expected.
Ethical considerations
This study was approved by the Research Ethics Committee of Ribeirão Preto College of Nursing, University of São Paulo (protocol no.: 2,129,977; date: 21 June 2017). The development of the research followed the Regulatory Guidelines and Norms for Research involving human beings, as established by the Resolution of the Brazilian National Health Council no. 466/2012. All workers provided written informed consent.
Results
The majority of participants were female (54.9%), between 26 and 70 years old (mean 44.4; sd = 9.7). Most were married or in a stable relationship (74.9%) and had children (67.1%). The monthly family income reported was diverse, with an average of $ US 2,253.01 (sd = 1,323.83) and approximately three-quarters of the sample had completed higher education (Table 1). Table 2 shows descriptive measures and correlation coefficients for the variables PA, social support, mood, and alcohol consumption.
Sociodemographic characteristics. Brazil, 2018 (n = 395)
Sociodemographic characteristics. Brazil, 2018 (n = 395)
Note: Brazilian minimum monthly wage at the time of data collection: US$ 261.36 (equivalent to R$ 954,00).
Correlation between PA and the variables of social support, mood and alcohol consumption. Brazil, 2018 (n = 395)
Note: *p < 0.05; **p < 0.01.
A negative correlation was identified between PA and the factors of depression and fatigue. In addition, PA was positively correlated with the four variables of social support, vigor, and alcohol consumption. In order to further explore the relationship between PA and alcohol consumption, a new correlation analysis was undertaken, considering ranges of alcohol consumption. This relationship was significant only among low-risk participants (p = 0.009; R = 0.141). Table 3 presents the model that best explained PA [F(8.386) = 19.231, p < 0.001;r2 = 0.285].
Explanatory variables of PA. Brazil, 2018 (n = 395)
According to the proposed model, family support for walking, friends’ support for MVPA, the vigor factor, and alcohol consumption were positive predictors of PA. Considering that the drinking habit was a predictor of greater engagement in PA, we sought to analyze the possible moderating effect of social support in this relationship (Table 4). As seen in Fig. 2, AUDIT scores increased expressively with PA scores among participants who had no social support. Among participants with social support, this increase was less pronounced.
Effect of moderation of social support on the relationship between PA and alcohol use among workers. Brazil, 2018 (n = 395)
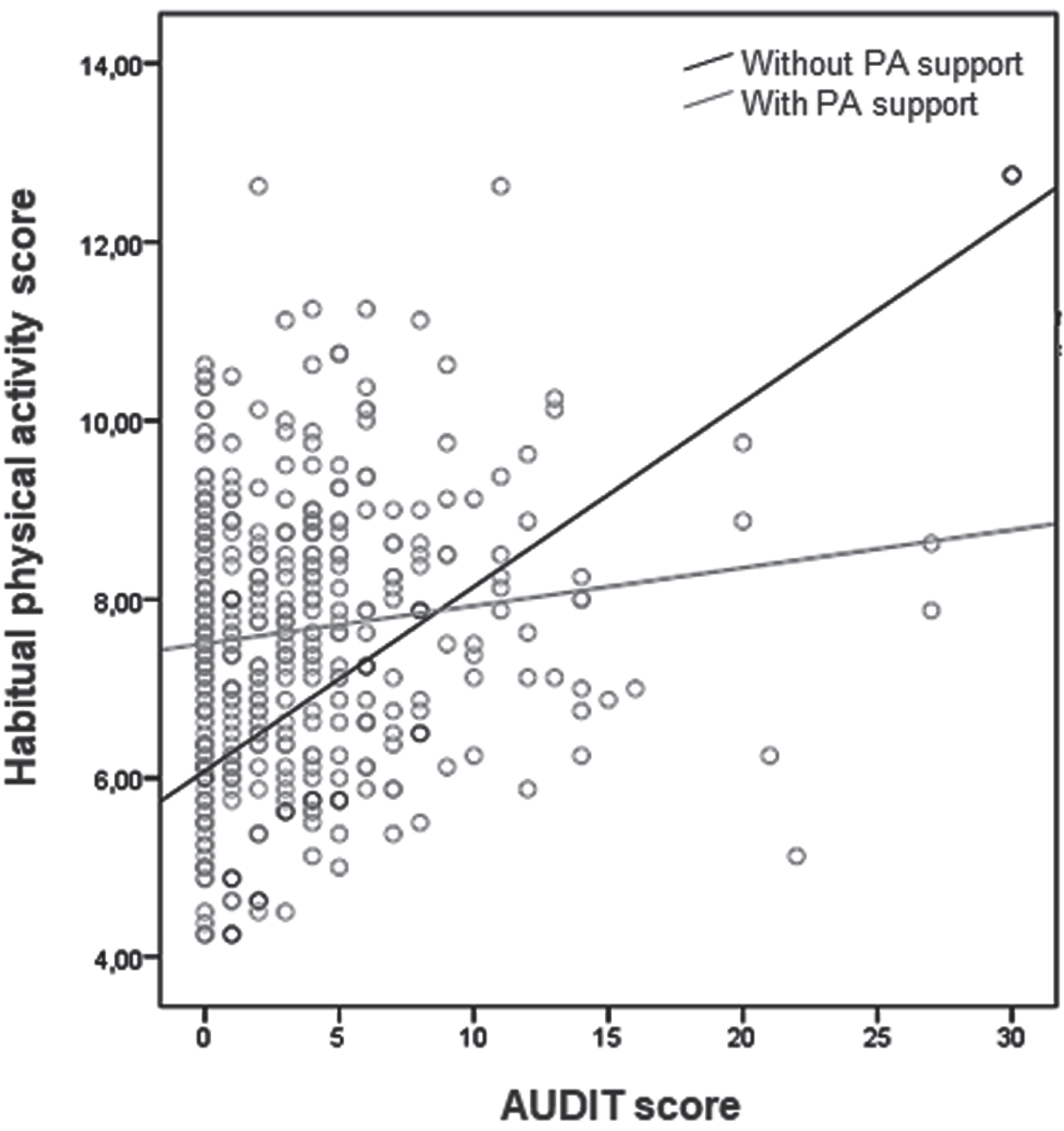
Social support as moderator of the relationship between PA and alcohol. [F(3.391) = 12.7578; p < 0.001; r2 = 0.0892]. Brazil, 2018 (n = 395).
In the present study, it was identified that social support (from family to walk and friends to MVPA) and positive mood (represented by the variable “vigor”) were factors related to greater engagement in PA. Alcohol consumption, among low-risk participants, was a predictor of PA, in contrast to the study’s hypothesis. However, social support had a moderating effect on the relationship between alcohol use and PA.
The socioeconomic profile of the participants was similar, in terms of sex, skin color, marital status and education, to previous study carried out with a public university technical-administrative staff [32]. However, when we compare to general Brazilian population, we find important gaps about skin color (45.2% white, 45.1% brown and 8.9% black skin color) and level education (only 13.5% have undergraduate degree) [33].
Considering these aspects and that the group investigated was composed exclusively by economically active individuals, we observe that they have a distinct profile if compared to the general Brazilian population and this condition can offer, to the study participants, more access to information and resources of adoption and engagement on health lifestyles like being more physically active.
Regarding to mood, vigor has also been identified as a predictor of PA in previous studies with other populations [34, 35], suggesting that this association occurs across various groups. Thus, the offer of programs and interventions that help people aware of the importance of involvement in PA is important across populations [34–42]. Such recommendations assume even greater emphasis on the work environment, since the adoption of healthy lifestyle habits tends to contribute substantially to the quality of the work and to professional valorization [36–43].
In relation to social support, the results of the present study showed that social support of family for walking, and friends for MVPA, were predictors of PA. Although the comparison with other studies is limited due to the methodological aspects used in the various studies, this finding is similar to a previous study carried out with Brazilian adults that used the same instrument to collect social support data [44]. This result suggests that incorporating different sources of social support in PA promotion strategies is promising. That is, a network approach with family and friends who are aware of the effects than roles as supporters of PA may contribute to positive results in the health of their peers.
In addition, these findings provide interesting triggers to discussions about intensity of PA and about some social support elements. The understanding of this condition, still incipient in the literature, can help develop new hypothesis and promote more effective interventions. In this sense, we recommended that future studies explore, in depth, the possible relationship between supporters and engagement on more or less intense activities.
In the context of the present study, for example, it is suggested that the fact of the university campus offers PA programs that, for the most part, are characterized by group activities which intensity could be moderate or vigorous, may have contributed to mobilize workers to invite, encourage or do these activities with friends. About the support for walking provided by family members, it is suggested that, as it is an activity carried out with different objectives (such as leisure or displacement), it may permeate factors such as family dynamics and structure, shared behavior or access to resources.
As for the use of alcohol as a predictor of PA among workers, a similar result was identified in previous surveys undertaken with other populations such as students and healthy adults [45–50]. Despite this, it is worth noting that in the present study, more specific analyzes pointed out that such a relationship occurred, mainly, among low-risk participants.
This result emphasizes the importance of considering different patterns of alcohol consumption both in research and interventions [45–47], as these patterns seem to represent a set of different health outcomes and the practice of PA. However, it is noteworthy that there are several controversial results regarding the direction of the relationship between these variables, including some evidence on the promising effect of PA for reducing alcohol consumption, especially in groups of those who are dependent on this substance [51–54].
In this sense, different explanatory models on the relationship between alcohol consumption and PA are identified in the literature. The biological perspective is based on the premise that both alcohol use and PA act as rewarding stimuli that activate the brain’s mesocorticolimbic pathways [55, 56]. Another point to consider is how exercising and alcohol could be acting in the responses to stress and, consequently, in the hypothalamic-pituitary-adrenal axis, so people simultaneously adopt these behaviors, aiming to prolong such effects [55, 56].
About the motivations for concomitant involvement in paradoxical behaviors (healthy and unhealthy), a review conducted by Leisure et al. (2015) [55] compiled two perspectives. In the first one, PA precedes alcohol consumption (such as celebrate important achievements with the consumption of alcoholic beverages) and it seems to be a widely publicized condition, especially among university athletes [46, 55]. The second perspective refers that the use of alcohol is the factor preceding the PA. On these situations, for example, to body image [46, 57] and feelings of guilt [55], can contribute to better understanding of the relationship between these variables.
These different motivations described by the literature, in light of the results obtained here, raise questions on the complexity of the studied phenomenon, and on the different psychosocial factors involved in the expression of health-related behaviors. It should be added that the positive relationship between PA and alcohol, contrary to the hypothesis of the present study, prompted the investigation of other factors that could be involved in this problem. Although little explored in the literature, two studies were identified that investigated potential moderators for this relationship. It is worth mentioning that these studies focused on intrapersonal variables such as age and sex [50] and impulsivity [48].
The relationship between vigor, PA, and alcohol use, in a survey conducted with a large sample of Americans, was stronger in young adults than in older adults. In addition, sex moderated the relationship between medium-intensity PA and alcohol use; that is, among men, the intensity of this relationship was greater than among women [50]. Results the effect of impulsivity, tested in a sample of American university students, showed that high levels of impulsivity moderated the positive correlation between PA and alcohol consumption [48].
In general, the moderating effect of social support has been investigated in different physical, emotional, and social health outcomes, and has shown promising results [58–61]. The finding that social support had the potential to mitigate the effect of PA on alcohol use was one of the most relevant results of this study. These findings are expected to draw the attention of researchers, and health professionals who may integrate association strategies into these practices with recommendations to expand and strengthen social support networks, and include people from the individual’s social environment in motivational approaches to health promotion.
Additionally, it is worth mentioning that low-risk participants are not exempt from a possible escalation of consumption, therefore the proposals for intervention and prevention should consider this possibility. Despite this prospect, it is understood that, approaches different from those used for high-risk drinkers will likely be necessary. In addition, actions in the context of PA and, preferably, carried out by people who also practice such activities e.g., at parks, gyms, or sports courts.
The main limitation of the present study was that the adopted PA questionnaire was a subjective measure of data measurement, as there are more accurate ways of evaluating this variable, such as the use of technological equipment. Despite this, this method of data collection has been widely used due to its feasibility in relation to costs and ease of application, justifying its use in this research. Furthermore, the study was cross-sectional in design, so we can only claim correlations, and notcausality.
Future research could include an intervention to enhance the most impactful form or forms of social support, with pre- and post-intervention measures related to physical activities, and whether these had an impact on other variables, such as depression, or risky, harmful or dependent alcohol use.
Conclusion
It was identified that social support from friends and family, vigor, and alcohol consumption were predictors of PA in the studied group. Contrary to the hypothesis of the present study, a positive relationship between PA and alcohol consumption was also identified among workers who consumed alcohol in a pattern considered as low risk. In addition, it was found that social support had a moderating effect on this relationship, a factor to be explored in approaches aimed at adopting healthy habits.
In short, the findings of the present study reinforce the idea that elements at different levels of influence may be directly or indirectly involved in the engagement of individuals in the phenomenon of PA. Thus, it is understood that the complexity of active behavior requires, on the part of health professionals, a broader approach in order to contemplate the individual in a holistic manner, respectful of his or her preferences, and limitations. In addition, the importance of developing specific actions and proposals for each alcohol consumption pattern is highlighted, considering the psychological and socio-environmental characteristics of workers.
Ethical approval
The study was approved by the Research Ethics Committee of Ribeirão Preto College of Nursing, University of São Paulo (protocol no.: 2,129,977, date: 21 June 2017).
Informed consent
All participants provided written informed consent.
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Funding
The work was supported in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) (grant number 001). The sponsor had no role in the study design.