
Abstract
BACKGROUND:
Constant use of hand-held vibratory tools may cause health issues, including hand dysfunction, among farmers. Thus, exposure to these vibratory instruments may cause hand-arm vibration syndrome (HAVS).
OBJECTIVE:
The study aimed to measure the prevalence of HAVS and evaluate neurological and vascular symptoms among farmers.
METHODS:
This cross-sectional study included 20 villages in Pakistan and used a three-part questionnaire to collect data from farmers exposed to vibration while farming. The study included demographics, the Health Surveillance Questionnaire, and the Stockholm Workshop Classification Scale. SPSS version 22 was used for the data entry and statistical analysis.
RESULTS:
433 (43%) participants had musculoskeletal discomfort and 568 (57%) had hand vibration. Raynaud phenomenon was evident in 430 (43%) participants, whereas carpal tunnel syndrome was found in 218 (22%). Tingling was reported by 255 participants (26%), and numbness was reported by 543 (54%). According to the grading of neurological symptoms, 461 (46%) participants were exposed to vibration but did not experience any symptoms, placing them in stage 0. 185 (18.5%) participants with HAVS with infrequent episodes affecting just the tips of one or more fingers were categorized in stage 01 based on grading of vascular symptoms.
CONCLUSION:
HAVS are common among harvesting farmers, with the most noticeable vibrations occurring in the shoulder region. Similarly, most farmers had no vascular symptoms, and most were exposed to vibration but had no neurological symptoms.
Introduction
Workplace exposure to vibration from hand-held power tools or vibrating work surfaces can cause a condition known as hand-arm vibration syndrome (HAVS) [1]. Farming is a career that requires a lot of work, so farmers are more likely to get musculoskeletal injuries, upper limb dysfunction, cumulative trauma disorders, and more. Individuals exposed to HAV run the risk of acquiring a variety of neurological, vascular, and musculoskeletal symptoms commonly referred to as HAVS [2]. According to hygiene and medical research, from 2.5 percent to 82.8 percent of workers using vibrating devices have HAVS. Experiencing and reacting to hand-transmitted vibrations has been linked to vibrating white finger incidence [3].
Hand-transmitted vibration has multiple signs and symptoms involving neurological and vascular disorders, including numbness, tingling, discomfort, pains, and stiffness [4]. Integration of these sign and symptoms triggered by hand-communicated vibration is known as HAVS. In fact, parameters presenting all these symptoms due to hand-transmitted vibrations are not fully known. Thus, it is said that HAVS can affect different people in multiple ways, for those who are affected but not diagnosed and for those who are affected and diagnosed [5].
Strong dynamic and static joint loading and repetitive hand-arm motions cause upper extremity vibration injuries. Low frequency percussion causes joint cartilage damage by repeated shocks from the tool and additional articular loads [6] and wrist vibrations cause hand bone cysts and osteoporosis, according to previous studies [7]. The neuropathological effects of direct energy transfer from vibration to muscle cell were observed in muscles and tendons [8]. Low frequency vibrations affecting the upper arm can cause shoulder, acromioclavicular, and elbow osteoarthrosis [6]. Long-term vibration exposure weakens hand, wrist, and forearm muscles, resulting in shaky grip [9]. It causes tendinitis and osteoarthrosis of the wrist, elbow, shoulder, and the acromioclavicular joint [10]. Injuries to the triangular fibrocartilage complex (TFCC) are linked to hand-arm vibration in farmers [11]. Carpal tunnel syndrome is common among farmers using hand-arm vibration system due to structural damage and edema formation, reducing sensory nerve conduction in hand and wrist [12]. Repetitive movements and high intensity vibrations in the wrist can damage the myelin layer of nerves and cause signs of perineural fibrosis [13]. The musculoskeletal injuries using hand-arm vibration system result in weakness of intrinsic muscles of hand, loss of muscle control and loss of manipulative dexterity [6]. The classic vibration white finger is rare. HAVS symptoms include finger blanching, tingling and numbness, pain in the hands, loss of manual dexterity, and hand muscle weakness [13]. These changes include vessel wall hypertrophy and endothelium cell damage. Changes in digital tuft mechanoreceptors (Pacinian corpuscles) and myelinated digital fibres have been described [14].
Using vibratory tools for long periods of time might well have negative health consequences for harvesting farmers, resulting in anomalies in the function of the hand. The long-term use of these vibratory tools or exposure to these vibratory tools may result in HAVS [15]. Hand-held olive harvesters cause high levels of HAV due to hand contact with the handle. Long-term exposure to these stresses may cause HAVS, which affects upper-limb structures (musculoskeletal, nervous and vascular). The escalation of these issues in both developed and developing countries confirms the importance of ergonomics in agriculture [16]. Farmers with HAVS use significant force in the fields and perform activities such as lifting, digging, and shoveling due to the use of machinery such as tractors and harvesters. Using tractors and other machinery exposes farmers to complex and varied vibration conditions (ranging from 1– 9 Hz) with multi-axis translation and rotational vibration inputs to different parts of the body, causing disorders [11].
The duration of tool disclosure, the required gripping power, the structure or composition of the work surface on which the work is performed, the posture in which the work is performed, the season of the year in which the work is performed (summer or winter), and the individual susceptibility or liability are all determinants that may contribute to the development or progression of HAVS symptoms among farmers [17].
Patients with HAVS may exhibit the following symptoms: sensory abnormalities, tingling, and paresthesia; excessive use of instruments that produce vibration may impair hand functioning and increase the chance of developing tremors [18]. HAVS affects around 288,000 people in England. According to a survey conducted by the Medical Research Council in 1997 and 1998, close to 5 million people are asked to use vibratory tools in a given week, with both male and female ratios, but the majority being male, and the conclusion being that males are more prone to develop HAVS than females [19]. HAVS is more likely to develop in occupations that employ vibratory instruments, such as inflatable drills, crushers, and power wrenches [20]. There are following characteristic indications involving fingers vasospasm may produce by ice, sensory loss, paresthesia and tingling, and disturbed hand function [19]. The severity or extremity of HAVS can hinder the daily activities [21].
Su [22] performed a study in stifling kingdoms to examine the individualities of HAVS in a hot environment, comparing the results to the United Nation’s National Institute for Occupational Safety and Health structured analysis. The assessment only included measurements derived from a humid or subtropical climate. Vibration induced white finger was not seen in tropical kingdoms. Symptoms of nervousness were seen in most vibration-exposed labours. Finger coldness seems to be a substantial alternative to vascular illness in a tropical setting. HAVS has been shown to cause advanced vasospastic effects (shaking-induced white finger), finger sensorineural instabilities (digit numbness, obstructed material purpose), and musculoskeletal irregularities leading to muscle fatigue, deteriorating progressions over frames and junctions [23].
To improve occupational safety, ISO 5349 explains how to perform the task and covers the general requirements for measuring and evaluating human exposure to hand-transmitted vibrations. Furthermore, ISO 5349-2 provides practical guidance for implementing appropriate measurement and evaluation techniques in the workplace. Detailed specifications of the equipment to be used when performing measurements in accordance with ISO 5349 are contained in ISO 8041 [24].
Upper extremity HAVS is caused by neurologic, vascular, and osteoarticular issues in tremor-exposed workers. Peripheral sensorineural complaints are more common in training groups employing vibratory cookware. Composition utensils have been related to radiocarpal joint degeneration, elbow stiffness, and osteophytotic. For sensorineural instabilities and bone and joint issues, there is a lack of epidemiological evidence to suggest consistent disclosure-response connections. Vibration-induced white finger (VWF) is a numerical vasospastic symptom that occurs more often while using hand-held utensils [25].
Investigation of hand-arm vibration disorder symptoms in a relatively large population of pebble workers in Italy. The quantity response connection for shaking was also planned. The survey included 570 quarry drillers and stone carvers and 258 management level workers who only used handbooks. Every participant was surveyed for happiness and productivity. On the Stockholm workshop measures, VWF and sensory complaints were severe. VWF was found to be 30% prevalent in the whole cluster exposed to vibration. Raynaud’s phenomenon was seen in 3% of the panels. According to the experience data of this education, the predictable proportion of stone employees affected with VWF tends to extend unevenly in percentage (for a certain exposure period) or quantity to the four-sided origin of the period of exposure (for a continuing amount of shaking). The trembling disclosure aircraft now being debated in Europe looks to offer low-cost protection for workers against harmful hand-transmitted vibrations [26].
HAVS is a group of neuromuscular and vascular symptoms caused by exposure to vibratory instruments. This condition is characterised by finger paresthesia, hand and wrist discomfort, cold intolerance, intrinsic muscle groups or weak point flexors, finger staining, open pores, and skin lacerations. HAVS is reversible in the early stages, but detection of symptoms is rare in later stages, and use of vibrating equipment in such circumstances is hazardous [27]. HAVS requires a lot of exposure. Vibration affects the human body in various ways that are difficult to quantify, including the body posture, the biodynamic properties of the individual and the environment [28].
The sensorineural and vascular components of HAVS tend to follow and develop independently of one another [27] and is a common condition in Canada. Workers need support and resources to investigate symptom management and nonviolent work disability reduction. HAVS sufferers face mental, emotional, and physical challenges [29]. In agriculture and in relevant fields, HAVS is primarily exposed by tractors, combine harvesters, and bulldozers, and by vibrating hand tools such as chainsaws, forage harvesters, and potato harvesters [30]. Farmers are the backbone of many nations’ economies. The lack of understanding and awareness among farmers about the increase in HAVS caused by the use of hand-held utensils that cause vibrations led to the research. As far as the authors are aware, no study examining the prevalence of HAVS among farmers is being conducted in Pakistan. Thus, the purpose of this study was to determine the prevalence of HAVS among harvesting farmers, to ascertain the frequency of HAVS-related factors, to determine the frequency of finger tingling and numbness, and to evaluate neurological and vascular symptoms using the Stockholm Workshop Scale (SWS).
Methods
Participant recruitment
Farmers from 20 randomly selected villages in the Faisalabad District, Pakistan were included in this study. A convenience sampling technique was used to select the sample of farmers from the selected villages, and the sample size was determined using online Epi Tools software [31]. Farmers aged 18 to 60 who have used vibrating tools for more than two years voluntarily participated in this study. Dairy farmers, farmers with Parkinson’s disease or muscular dystrophy, and farmers who had not used vibrating tools for more than two years were not included in this study. Every participant provided written consent before data collection. The study was approved by ethical review committee of Riphah International University.
Data collection
The data were collected using previously administered questionnaire the through face-to-face interviews. The questionnaire was divided into sections to collect the following information: socio-demographic and occupational information, a cold-induced white finger questionnaire, and the SWS for vascular and neurological symptoms. The principal investigator (PI) and two additional investigators, both of whom were physical therapists, travelled to the selected villages with the survey forms and conducted direct interviews with formers, recording their responses on the survey form during the workers’ lunch break. Farmers who were not present during the collection of responses were also excluded from the study. Each of the 914 participants completed the questionnaire on their work history, symptoms of cold-induced white fingers (CWF), numbness, discomfort, and reduced grip force.
Screening for cold-induced white fingers
White finger’s screening question was consisted of questions such as when it becomes chilly, one or more fingers turn white and lose their sensitivity. Do you have white fingers? (Y/N). After defining numbness, the first screening question questioned if the respondent had numbness in their hands or arms (Yes/No), and whether the numbness was limited to vibratory instruments (Yes/No). Blanching questions: Have you ever had white fingers? If no, move to tingling symptoms. If yes, how often does it occur (in the previous 2 years)? In reaction to the weather? Musculoskeletal questions: Do you have troubles with your hands/arms/wrists/elbows/shoulders? Pain? No/Yes, Stiffness? Swelling? Weakness? Numbness questions: Do your fingers go numb? In response to cold? With blanching? While working? At other time? If others times, what circumstances, and how long does it last?
Screening for HAVS
An international workshop held in Stockholm, Sweden in 1986 called “Symptomatology and Diagnostic Methods in HAVS” resulted in the development of the SWS [32]. White finger and neurological symptoms were classified using the SWS. White finger was diagnosed based on a history of cold-induced blanching of fingers or sections of fingers. There was no history of neurological symptoms such as numbness or loss of sensory perception or manual dexterity.
Data analysis
Statistical Package for the Social Sciences (SPSS) version 22 was used for the statistical analysis (IBM Corp., Armonk, NY, USA). Descriptive statistics include demographic data such as the mean and standard deviation and any VAS symptoms that may be present. Statistical significance will be set at P = 0.05.
Results
This study included 642 men and 358 females aged 18 or younger, 20– 23 years old, 24–29 years old, 30–39 years old, 40–55 years old, and >55 years old. The study included 41 participants in the underweight category, 376 in the normal category, 375 in the overweight category, and 208 in the obese category of the body mass index (BMI). Eight hundred twenty-nine participants are right-handed, 171 are left-handed, 542 are current smokers, 170 are ex-smokers, and 288 are non-smokers (Table 1). Our study found that 433 (43%) participants had musculoskeletal discomfort, 568 (57%) have hand vibration, and 329 (33%) had skin issues. Raynaud phenomenon was evident in 430 (43%) participants, whereas carpal tunnel syndrome was found in 218 (22%) (Table 2).
Demographic information of participants
Demographic information of participants
Frequency of HAVS-related factors among participants
Our study found that 430 participants had white fingers, 76 had white fingers in response to cold or wet conditions, 430 had blanching while working, 42 had white fingers at other times, 395 had white fingers for the first time when they were 1 to 10 years old, 35 had white fingers for the first time when they were 11 to 20 years old, and whiteness did not occur in 570 and happened every day in 430. Our study discovered that 255 participants suffered from tingling in their fingers, 157 responded to cold or wet conditions, 174 had tingling with blanching, 1 had tingling at other times, tingling lasted less than 20 minutes in 17 and more than 20 minutes in 254. Tingling was first noticed in 184 participants, more than or equal to 2 years in 9, and more than 5 years in 61. The results of our investigation revealed that 543 participants had numbness in their fingertips, whereas 457 did not. 80 participants respond to cold or wet conditions, 291 had numbness with blanching, 543 had numbness while working, 269 had numbness at other times, numbness first noticed, less than 2 years in 283, more than 2 years in 144, more than 5 years in 86, more than 10 years in 30, numbness lasted less than 20 minutes in 178 and more than 20 minutes in 365 (Tables 3 and 4).
Frequency in which participants suffered from whiteness of the fingers
According to the SWS, 461 (46.1 percent) participants are exposed to vibration but have no symptoms in the 0SN stage, 428 (42.8 percent) have intermittent numbness with or without tingling in the 1SN stage, 108 (10.8 percent) have intermittent or persistent numbness, reduced sensory perception in the 2SN stage, and 3 (3 percent) have intermittent or persistent numbness, reduced tactile discrimination, and/or reduced sensory perception in the 3SN stage (Table 4).
Frequency in which participants suffered from tingling and numbness of the fingers
According to the SWS, 570 (57.0 %) participants with no attacks are in stage 0, 185 (18.5%) with occasional attacks affecting only the tips of one or more fingers consuming mild grading are in stage 1, 153 (15.3%) with occasional attacks affecting distal and middle (rarely also proximal) phalanges of one or more fingers are in stage 2, and 73 (7.3%) with frequent attacks are in stage 3 (Fig. 1).
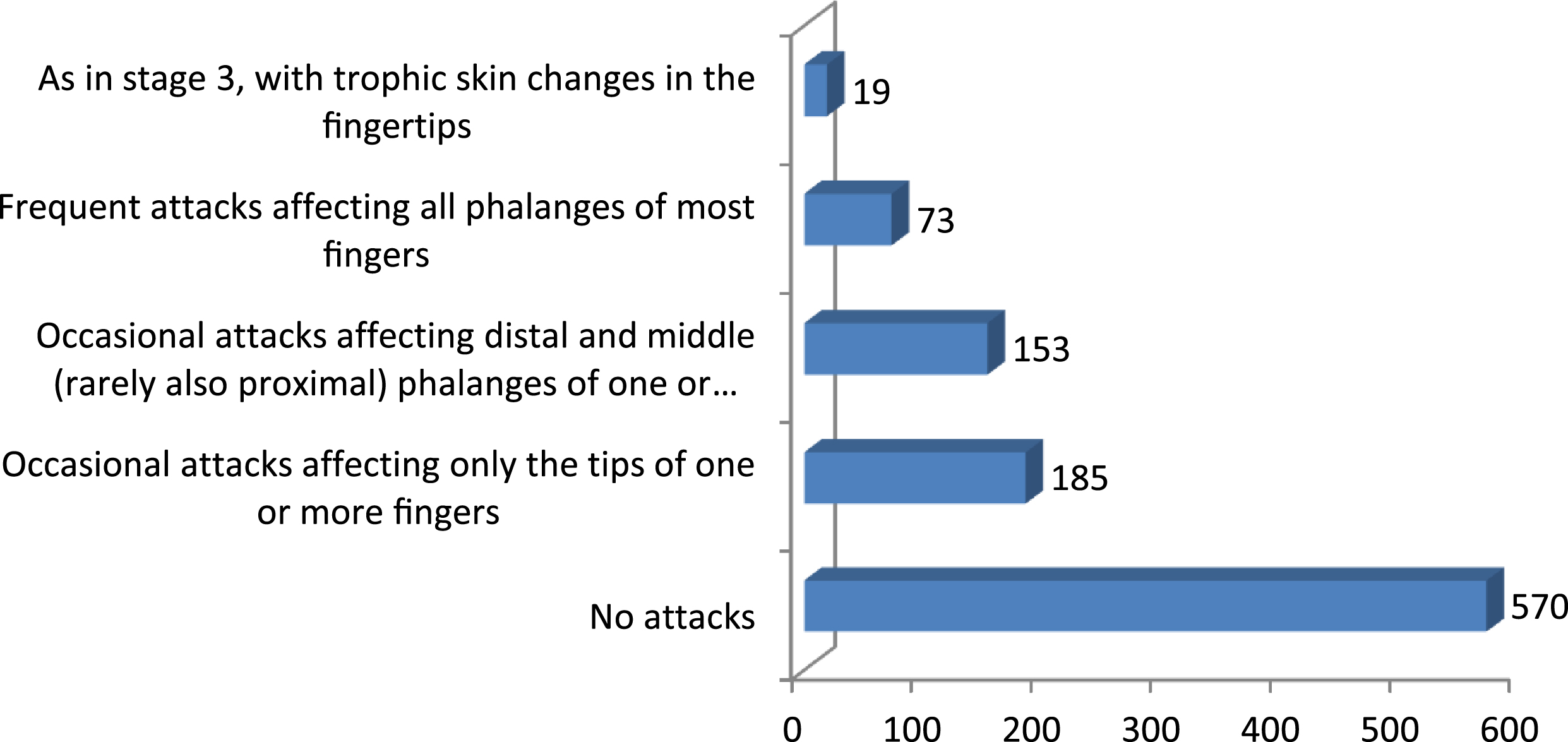
Grading of vascular symptoms according to the Stockholm Workshop Scale (SWS) and distribution in subgroups.
Use of hand-held power tools results in hand-arm vibration, which has been linked to numerous health problems, including painful and disabling conditions of the vascular system, nerves, and joints. The prevalence of HAVS was determined by surveying farmers in this study.
HAVS has been reported in sectors including, forestry, car assembly, construction, mining, foundry work and metal working crafts [33]. Research in the United Kingdom indicated that agricultural workers are exposed to HTV and hence susceptible to HAVS. The prevalence ratios of cold-induced finger blanching and sensorineural symptoms were observed to be 1.2–2.6 in these employees compared to unexposed employment [2]. This study revealed a lot about HAVS. This study found some regional and environmental variances. VWF, a kind of secondary Raynaud’s phenomenon, is the most established symptom for the diagnosis of HAVS [5, 34]. This is due to recurrent mechanical trauma causing endothelial damage and oxidative stress in the hand. The sympathetic nervous system is then activated, causing peripheral vasoconstriction [33]. However, these symptoms may be linked to weather and population dispersal. The temperature fluctuations in tropical climates may reduce these effects.
Grading of neurological symptoms according to the Stockholm Workshop Scale (SWS) and distribution in subgroups
Grading of neurological symptoms according to the Stockholm Workshop Scale (SWS) and distribution in subgroups
Persistent episodic finger blanching, cold sensitivity, and VWF are some of the symptoms indicating a vascular component. VWF is a kind of secondary Raynaud’s phenomenon and is the most well-established sign for the diagnosis of HAVS [34, 35]. Despite the fact that the damage is minor, it happens as a result of local endothelium damage produced by recurrent mechanical trauma in the hand. As a result of the stimulation of the sympathetic nervous system, peripheral vasoconstriction occurs [36]. On the other hand, these symptoms may be linked to changes in atmospheric conditions as well as the geographic dispersion of the populace. Because of temperature fluctuations, these symptoms may be less noticeable in tropical locations.
Pain and weakness in the upper extremities causes diminished grip strength [36]. This causes discomfort and impairment of upper extremity function since the hand is the most distant component of the body. To determine the incidence of HAVS symptoms, including grip strength, among farmers who utilize equipment in addition to manual work, and to determine the link of TFCC damage with HAVS due to degeneration, repeated stress, and overuse.
Our investigation found that blanching is 43% and numbness is 54%. The farmers are chosen to analyses HAVS since no study on HAVS has been identified. A 2003 research by Barregard among Swedish auto mechanics quantified the prevalence of HAVS. Participants completed an 806-questionnaire on vascular and neurological problems. Cold-induced white finger was found in 24% and prolonged numbness in 24% of the participants [37]. Our research suggests that those who use vibratory instruments are more prone to HAVS. Heaver found that many workers suffer from HAVS after using excessively vibrating command utensils [19].
Using a cross-sectional study, we found that farmers who use hand-held vibratory utensils excessively are more likely to acquire vasospastic condition, such as VWF, than those who do not. Longitudinal cross-sectional epidemiology studies conducted by Bovenzi show that occupational exposure to vibration transmitted by hand from an abundance of different types and sizes of kitchen implements is associated with an increased incidence of numerical vasoconstriction disorders (VVF) [25]. In a study by Aeillo et al., the use of portable shakers carried a risk of hand-transmitted vibration exposure. Operators are exposed to hand-arm vibration due to the use of portable shakers. The circulatory system, nervous system, and locomotor apparatus of the upper limbs can be adversely affected by prolonged, daily use of such equipment. HAVS exposure results in a constellation of vascular, neurological, and musculoskeletal symptoms. Vascular and neurological disorders may occur simultaneously or independently in workers who have been exposed [38]. Hand tractor drivers have a high risk of HAVS, according to Bagye et al. A hand tractor is rolled by two to three workers for one day. The exposure threshold for an operator’s arm and hand is 6 m/s2. The study found that 59.3 percent of respondents were exposed to vibrations greater than 4 m/s2, while 40% were not. HAVS was diagnosed in 56.26 percent of respondents, while 43.75 percent of respondents were negative [39].
According to our study on farmers who use vibratory utensils, 43% of those surveyed had HAVS. In comparison to W Lin’s survey of the whole population of China, our sample size was just 20 villages, resulting in a significant disparity in the percentage of results. As of 2005, W Lin researched the prevalence of this illness in China, and it was found that 2.5 percent to 82.8 percent of workers who used vibrating devices were affected by it [3]. Our findings show that the male-to-female ratio of HAVS cases is higher than the female-to-male ratio. Raynaud’s phenomenon is frequent among the general population, according to a study conducted by Palmer. HAVS is responsible for a large number of deaths, disproportionately among males, underscoring the threat it poses to the general public’s health [40].
HAVS occurs regularly among harvesting farmers. The shoulder region was the site of the most noticeable vibration in the body region that was revealed in current study. The majority of the farmers in this study reported numbness rather than tingling. In addition, on the SWS, most farmers reported no vascular symptoms, and the majority of farmers were exposed to vibration but did not experience any neurological symptoms.
Preventive measures can be taken by workers in order to reduce the prevalence and risk of HAVS, including ergonomic tools, the contact surface with the hand, antivibration padding, gloves, and damping techniques, as well as job rotation, selecting appropriate tools and by scheduling break periods at their place of employment.
This study was not without limitations. It was not investigated in this current study whether HAVS was associated with the various types of tools used by farmers in their daily work. Furthermore, only one district in Pakistan was represented among the participants.
Conflict of interest
The authors declare no conflict of interest.
Funding
Not applicable.