
Abstract
BACKGROUND:
Residual capacity evaluation via neuropsychological testing can facilitate the development of a rehabilitation plan in patients following a traumatic brain injury (TBI).
OBJECTIVE:
This study aimed to confirm the tasks that patients must perform well for early return to work (RTW) following TBI using the Wechsler Adult Intelligence Scale III (WAIS-III).
METHODS:
In total, 40 male and 13 female patients who suffered from neurobehavioral disabilities following TBI were recruited and classified into two groups: the successfully returned to work group (SRTW-G; n = 22) and the unsuccessfully returned to work group (USRTW-G; n = 31). The outcomes assessed by WAIS-III and the time to RTW were compared between the SRTW-G and USRTW-G groups. Multiple logistic regression, multiple regression analysis, and Cox regression were employed to assess differences between the groups.
RESULTS:
The Comprehension and Letter-Number Sequencing subtests of the WAIS-III were significantly correlated with early RTW more than the other subtests.
CONCLUSIONS:
We found that, as reflected in the two subtests, patients with TBI must be able to perform well in the following tasks for early RTW: Retention of information for short time periods, information processing, and social judgment based on the knowledge of the patient’s experience.
Introduction
Advances in emergency medicine have resulted in improved survival rates of patients with serious head injuries [1]. Neurobehavioral disability is an unfortunate outcome of traumatic brain injury (TBI), which can result in impaired social interaction. Greenspan et al. reported that 63%of patients with TBI are of working age (15–64 years) and Bell et al. also reported that the most common age group was 46–55 years based on 305 patients with TBI [2, 3].
Therefore, vocational rehabilitation is an important issue for these patients [4–11]. Studies revealed that the rate of successful return to work (RTW) in patients with TBI is 0%–84%, based on various follow-up periods and severity reports [12]. For patients with TBI, vocational rehabilitation is necessary for a successful RTW [13]. However, the factors that determine the success of RTW are difficult to identify from medical interviews and the patient’s appearance. Thus, an appropriate assessment is an important first step in facilitating the development of vocational rehabilitation programs to help patients with TBI achieve an early RTW [14]. A common approach is the evaluation of a TBI patient’s residual capacity via neuropsychological tests [15], such as the Wechsler Adult Intelligence Scale (WAIS) test to assess general intelligence [15–20]. Previous studies have considered the association between intelligence quotient (IQ) and RTW in TBI [21–24]. Cattelani et al. and Ip et al. reported that the WAIS-R IQ was associated with RTW and was useful for the estimation of RTW [21, 23]. Green et al. reported that the Similarities subtest of the WAIS-III was useful for estimating RTW [24]. Some studies have reported an early RTW following vocational rehabilitation in TBI patients [25, 26]. However, no study has focused on the association between a specific WAIS subtest and early RTW or compared the subtests of this measure.
Therefore, this study aimed to examine the outcomes of WAIS-III for each subtest and compare the time required to RTW between the successfully returned to work group (SRTW-G) and the unsuccessfully returned to work group (USRTW-G). Furthermore, we aimed to confirm our hypothesis that WAIS-III subtests can predict an early RTW in patients with TBI.
Materials and methods
Subjects
We recruited the patients retrospectively. We also opened the information letter about the study with an opt-out option by the research ethics board site at Hokkaido University Hospital.
For patients who suffered neurological problems following TBI, we used the hospital’s data management system to confirm each patient’s clinical records and personal information, including age, sex, medical history, physical examination, neurological test results, and cerebral contusion findings on magnetic resonance imaging.
A total of 122 patients with TBI who were attempting to RTW were recruited from the Department of Rehabilitation Medicine of the Hokkaido University hospital.
The study’s inclusion criteria were as follows: (1) A clear record during the 3-year follow-up period, (2) able to complete WAIS-III testing at the first medical examination for TBI, (3) aged between 18 and 65 years, and (4) clear cerebral contusion findings on magnetic resonance imaging.
The study’s exclusion criteria were as follows: (1) The presence of a disease primarily or frequently affecting the central nervous system, including de-mentia, Parkinson’s disease, multiple sclerosis, and stroke; (2) some physical difficulty in RTW, such as severe paralysis, amputation, and so forth; and (3) refusal to participate in the study.
Among the recruited patients, 53 were eventually selected. All patient data were kept anonymous.
The follow-up period was determined based on a previous study that reported that the rate of RTW increased at a 3-year follow-up in patients with TBI [27].
Neurological tests
The validity and reliability of WAIS-III have been reported previously [28, 29], and it is a frequently used neurological test in daily medical examinations. We recorded WAIS-III scores for each subtest and used these scores in the statistical analyses to identify the intelligence factors for RTW.
We checked each patient’s medical record and confirmed the patient’s initial WAIS-III scores. Some patients underwent a second WAIS-III at a later time. It is necessary to follow the change in WAIS-III scores (either a decrease or increase) in TBI patients in order to include the effect of rehabilitation. However, in this study, we primarily focused on the abilities required for an early RTW following TBI.
Analysis
Logistic regression was calculated between RTW and the subtest scores of the WAIS-III at a 5%significance level. To identify the level of importance of each subtest, multiple regression analysis was conducted for each subtest to evaluate the performance intelligence quotient (PIQ) and verbal intelligence quotient (VIQ) between groups at a 5%significance level. Finally, Cox regression was calculated to determine the intelligence factor for early RTW at a 5%significance level. RTW was set as the event, and the time elapsed from the first medical interview to RTW was set as the duration of the event. Statistical analyses were conducted using the statistical software package JMP 8 (SAS Institute, Cary, NC, USA).
Ethics
This study was conducted in accordance with the Declaration of Helsinki and was reviewed and approved by the institutional review board of Hok-kaido University (016-0142).
Results
The SRTW-G consisted of 22 subjects (20 men and 2 women, mean age = 41.0±10.7 years), whereas the USRTW-G consisted of 31 subjects (20 men and 11 women, mean age = 42.3±11.3 years). The USRTW-G experienced neurobehavioral disability following TBI and attempted to RTW (Fig. 1). Both groups received the same general medical care comprising usual rehabilitation and medication based on individual symptoms and problems.
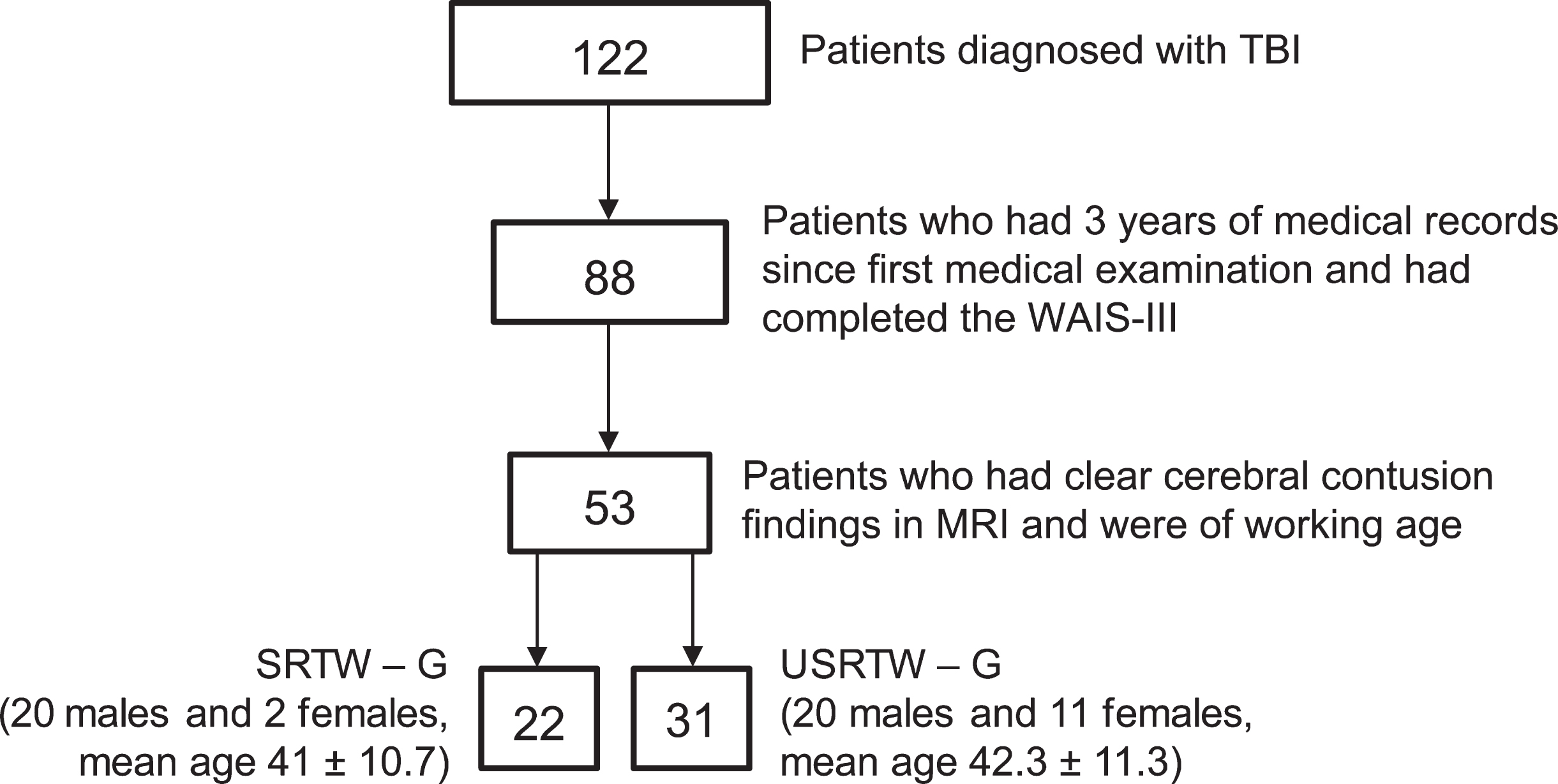
Flow of patients in the study.
All SRTW-G patients worked full time before their injury. Among the USRTW-G patients, five had worked part time and the rest of the patients full time. In terms of educational level, among the SRTW-G patients, none had 0–9 years of education (junior high school graduate), 1 had 10–12 years of education (high school dropout), and 21 had more than 12 years of education (high school graduate). Among the USRTE-G patients, none had 0–9 years of education, two had 10–12 years of education, and 27 had more than 12 years of education (and the educational level of 2 patients was unclear). Almost all patients had greater than a high school graduate educational level.
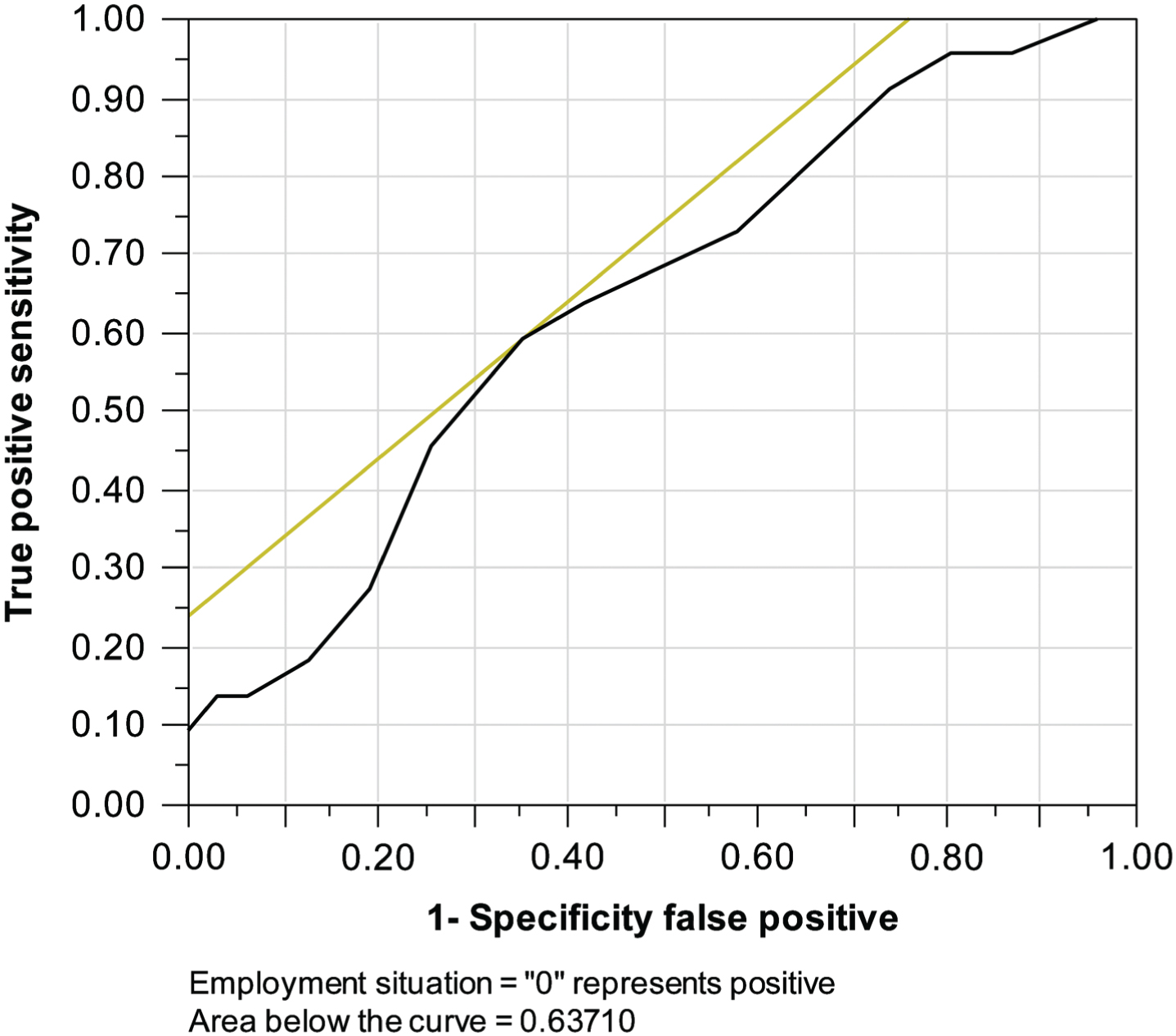
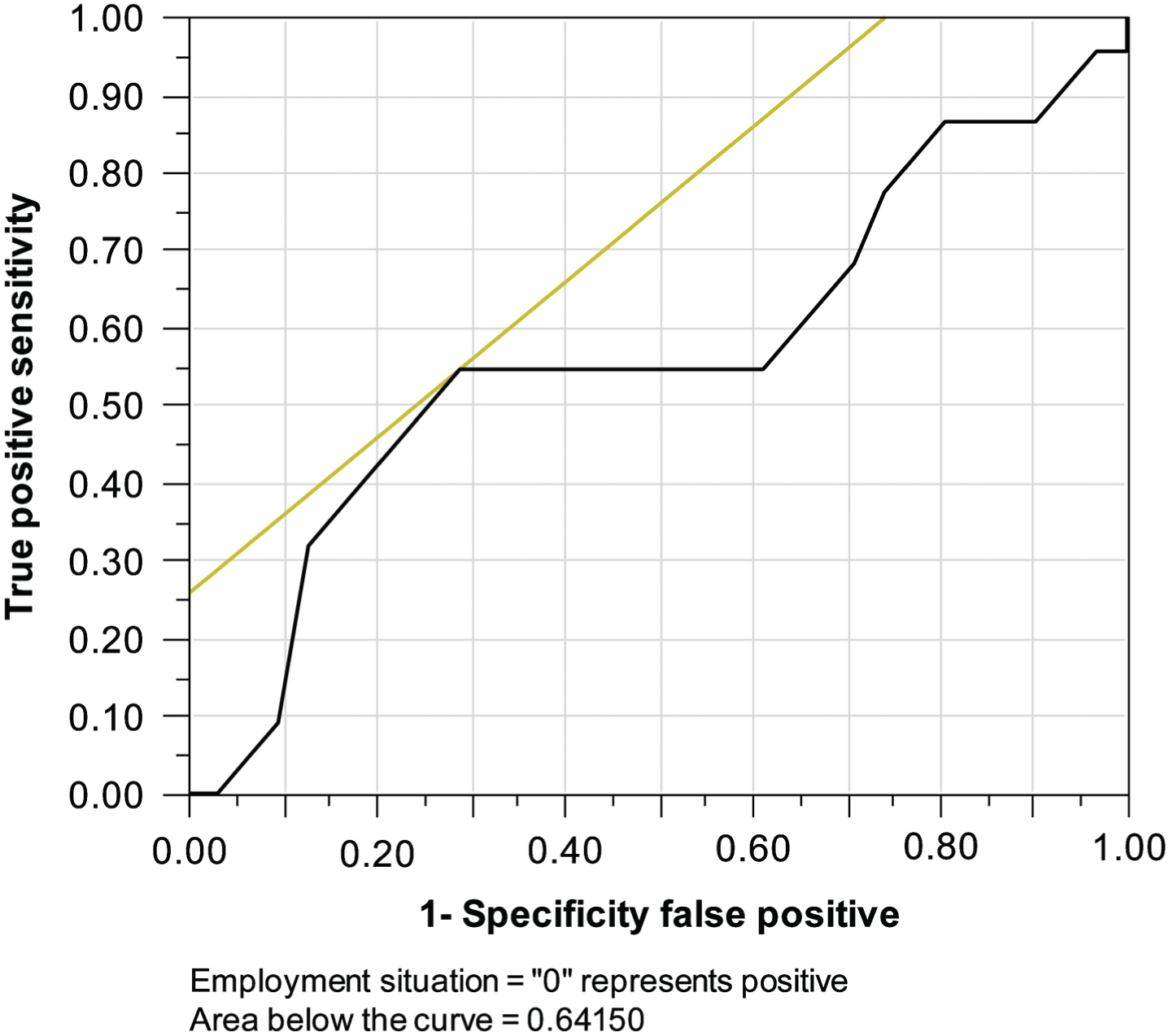
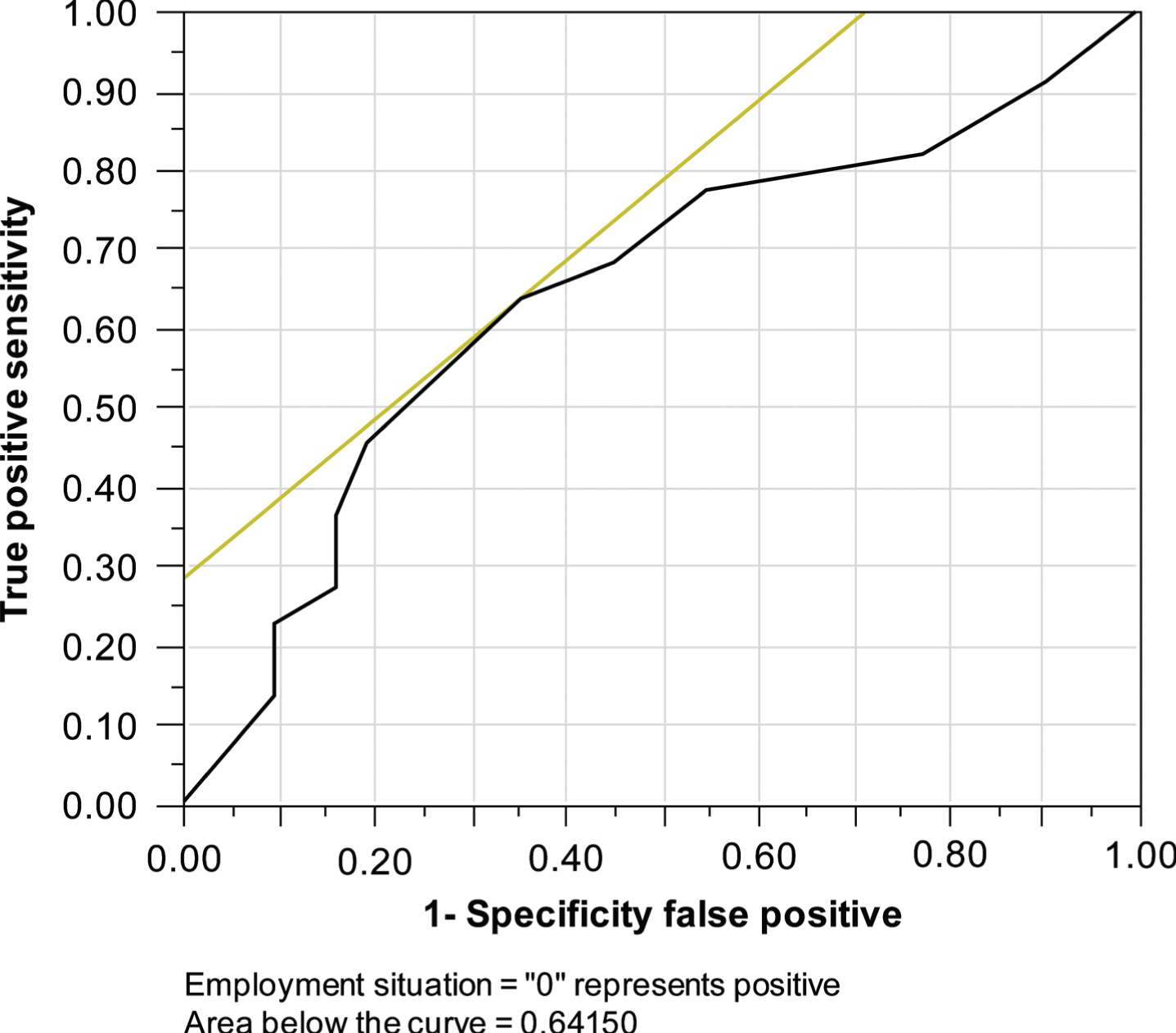
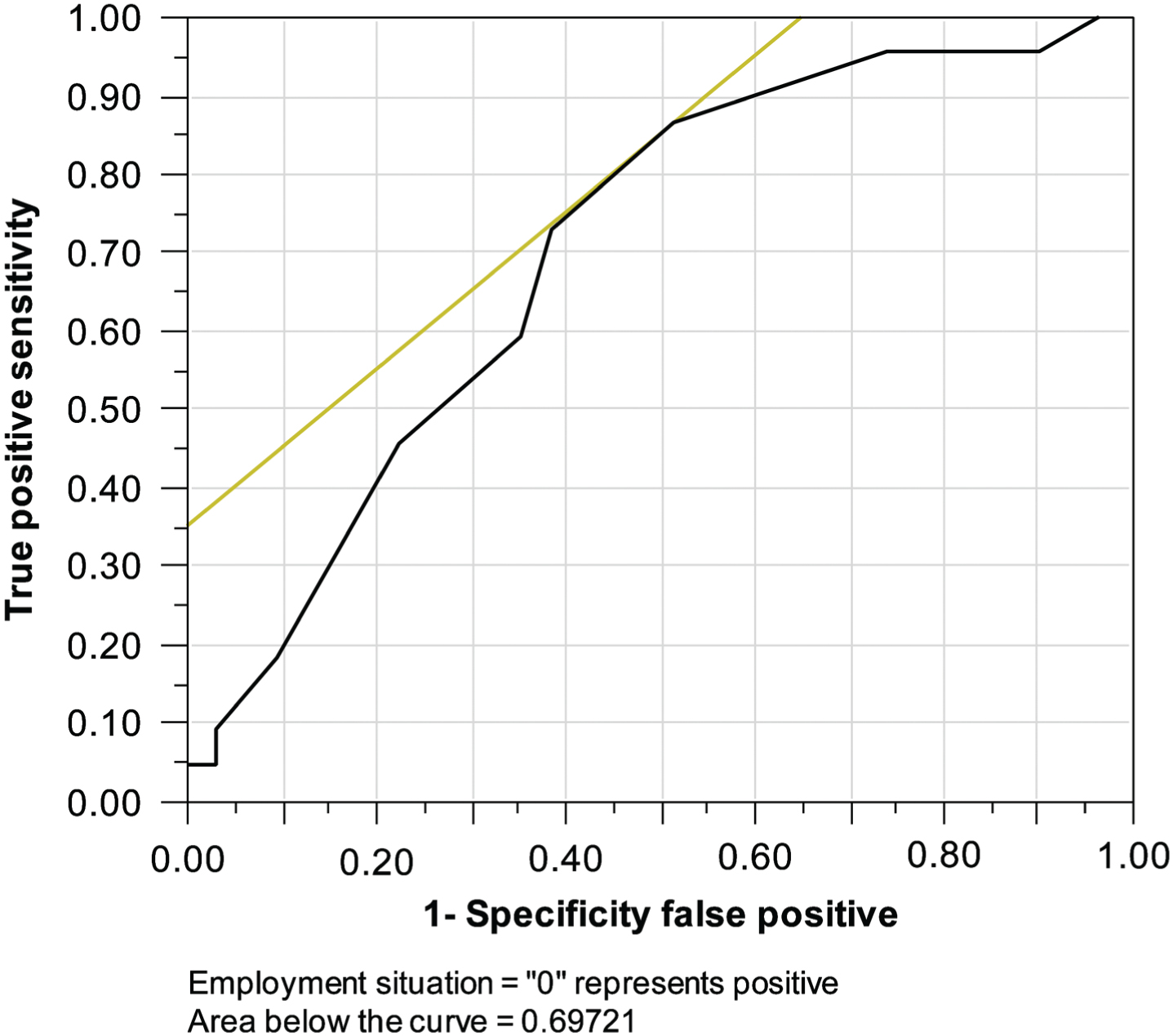
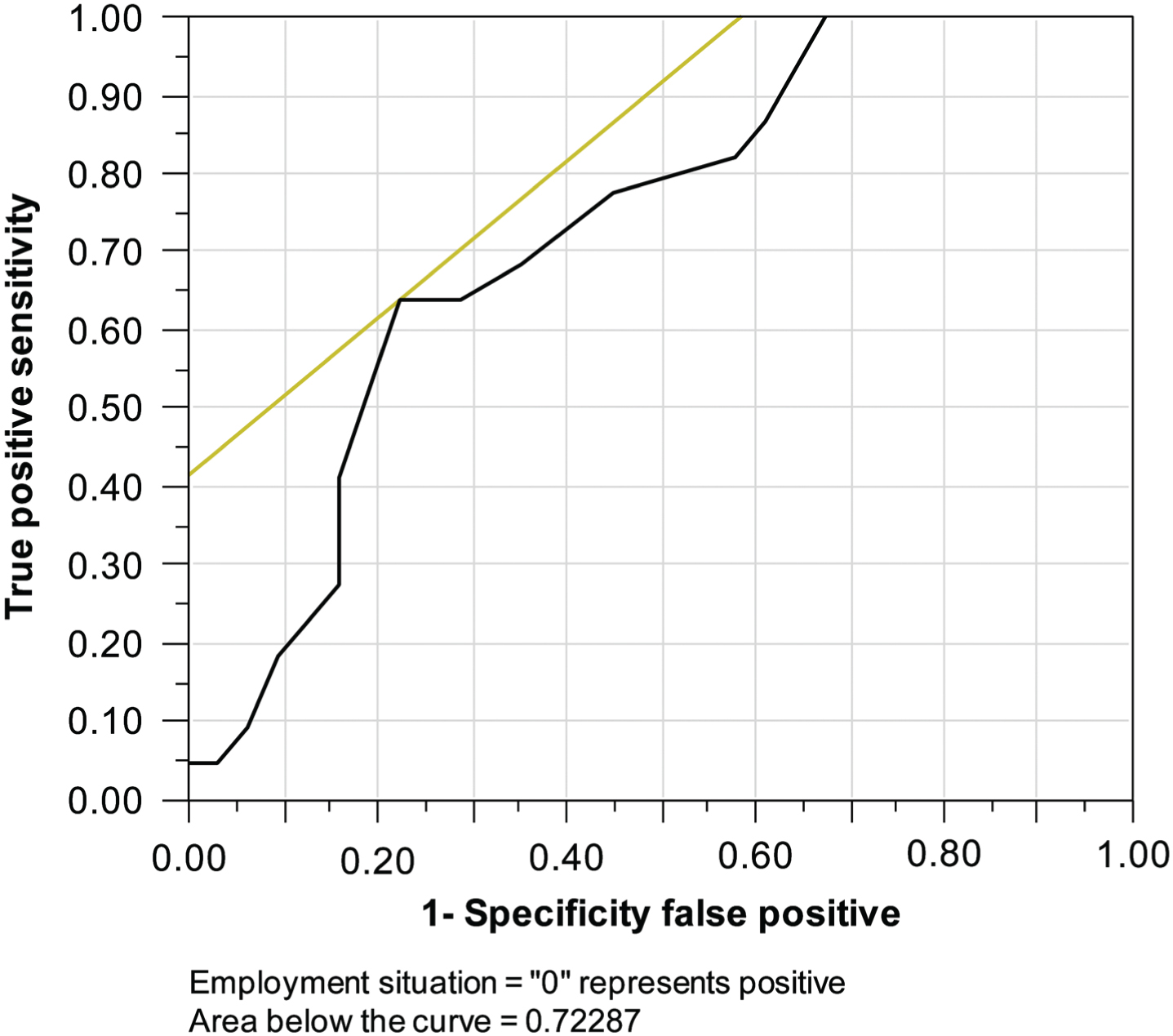
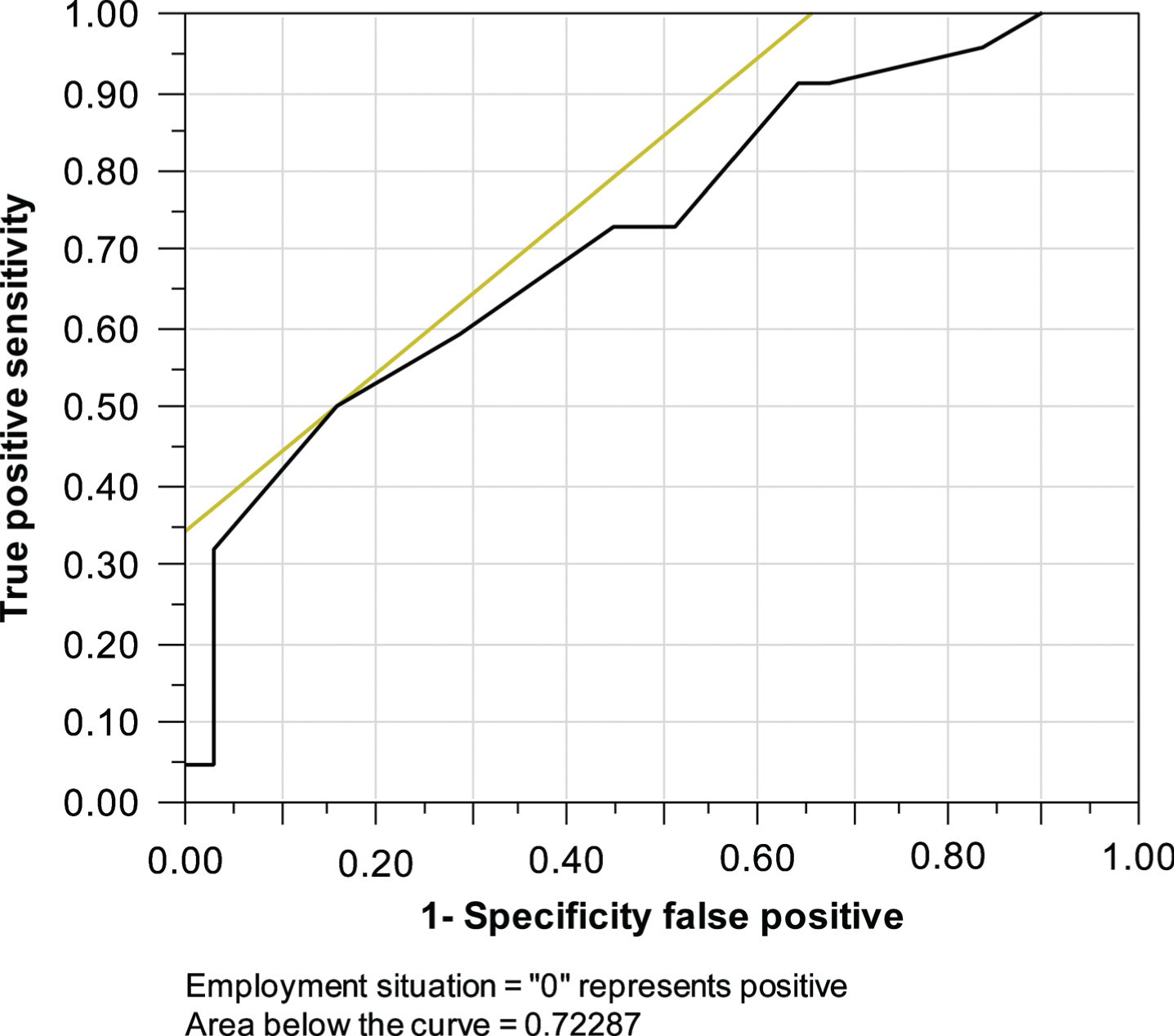
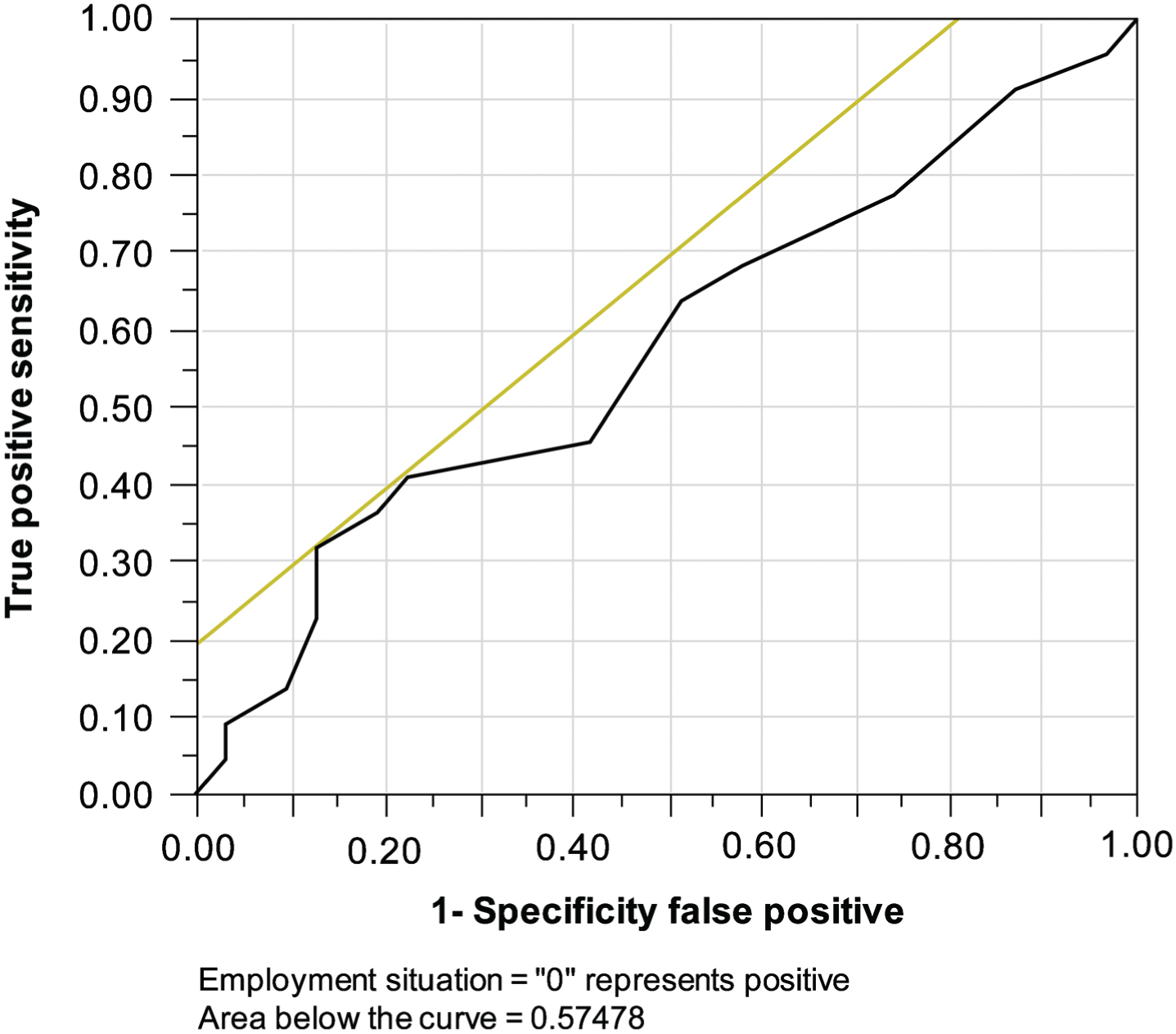
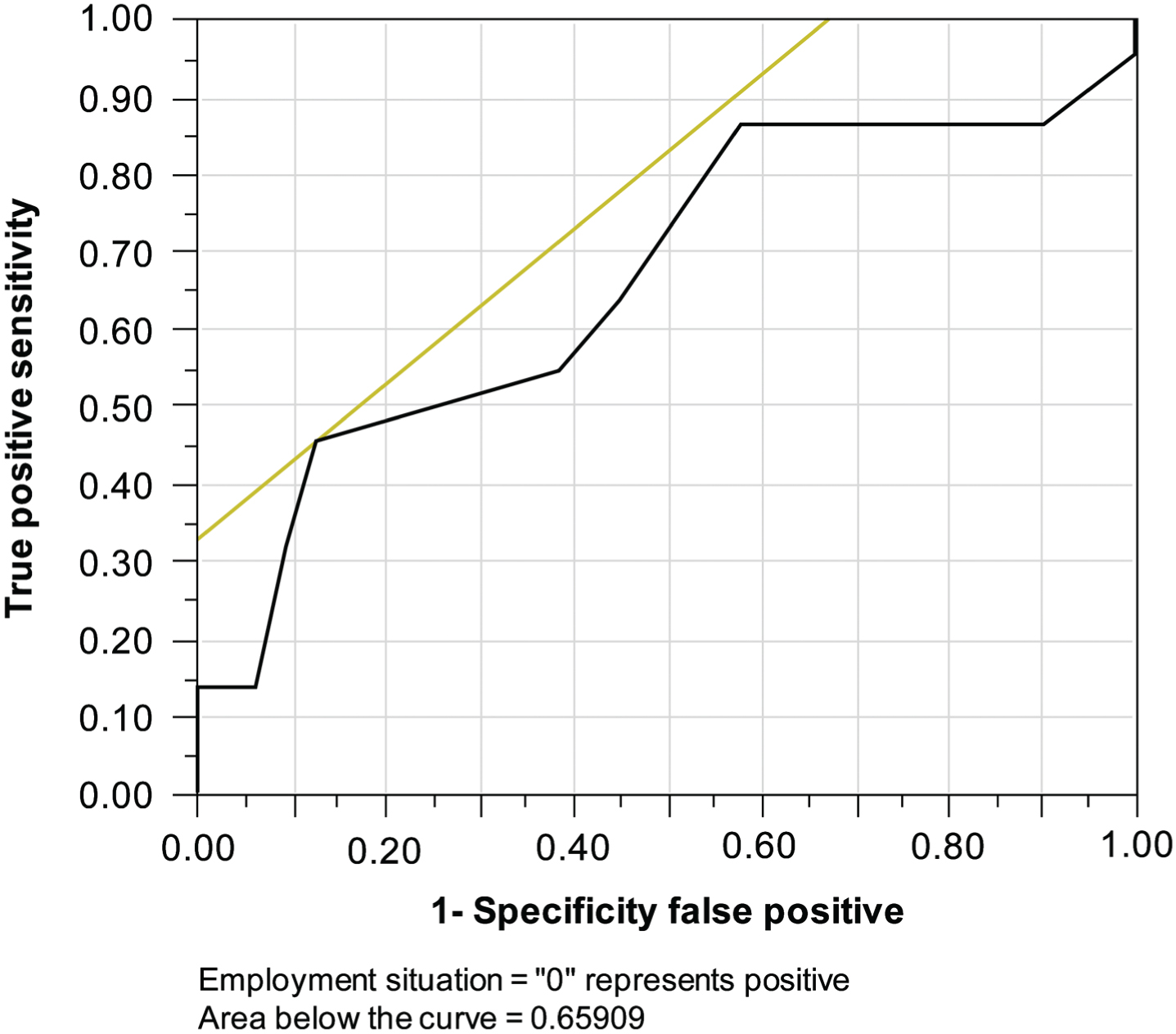
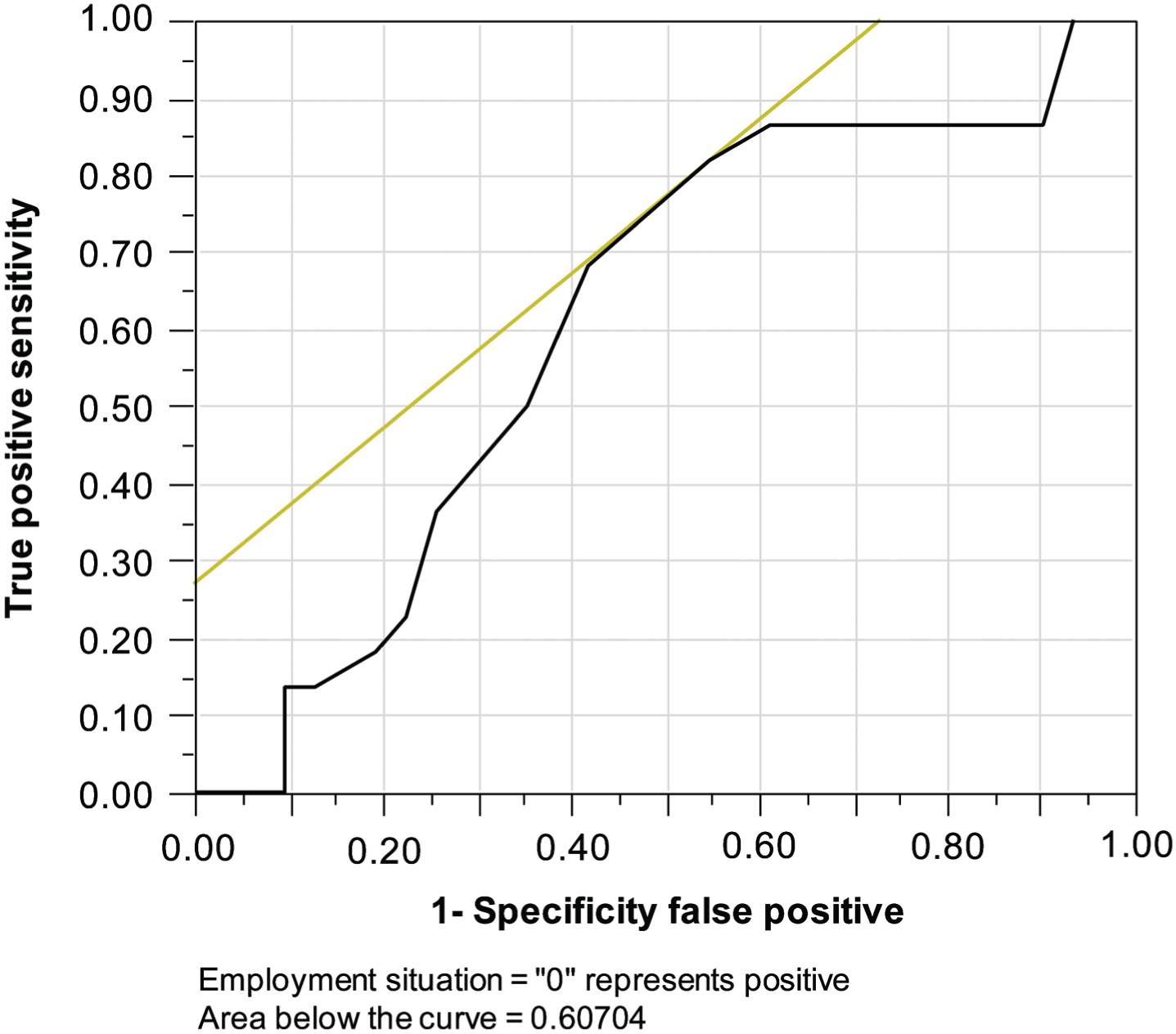
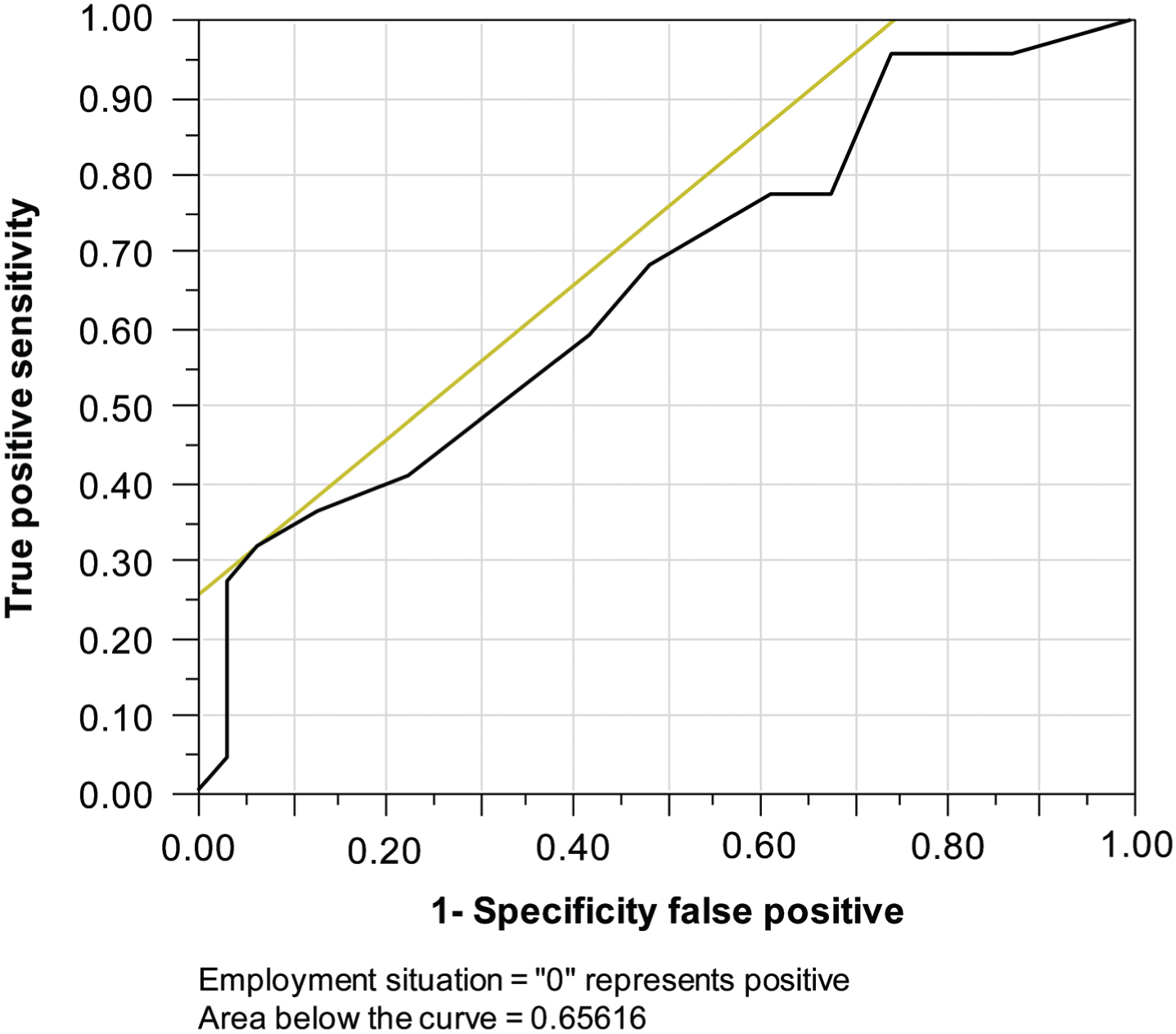
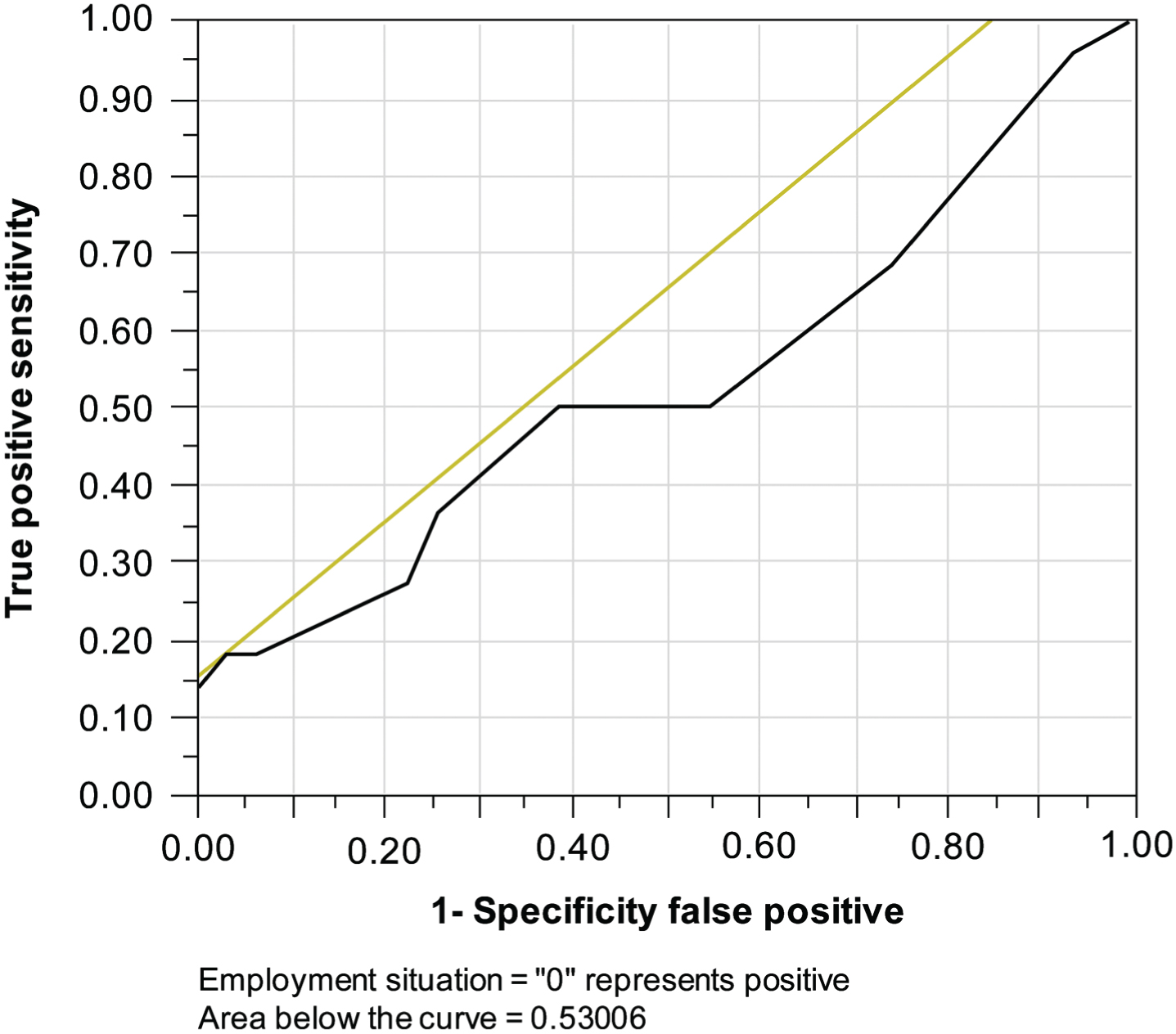
Tables 1–4 present the results of the logistic regression, which demonstrate an association between RTW and WAIS-III scores. Patients in the SRTW-G had significantly higher scores on the WAIS-III than those in the USRTW-G for the following sub-test metrics: full intelligence quotient (FIQ); VIQ; factor structure of Working Memory (WM) Index; Processing Speed (PS) Index; and Letter-Number Sequencing, Comprehension, Digit Span, Symbol Search, and Block Design subtests. The scores of these tests, with significant differences between groups, indicated that abilities measured by these tests were associated with RTW. The receiver-operat-ing characteristic curves for the logistic regression results are presented in Figs 2–15.
Results of the logistic regression for the VIQ, PIQ, and FIQ: association between RTW and the WAIS-III
*p < 0.05.
Results of the logistic regression with regard to factor structure: the association between RTW and the WAIS-III
*p < 0.05.
Logistic regression results of the VIQ: the association between RTW and the WAIS-III
*p < 0.05.
Logistic regression results of the PIQ: the association between RTW and the WAIS-III
*p < 0.05.
Vocabulary receiver-operating characteristic curve of the logistic regression results.
Similarities receiver-operating characteristic curve of the logistic regression results.
Arithmetic receiver-operating characteristic curve of the logistic regression results.
Digit Span receiver-operating characteristic curve of the logistic regression results.

Information receiver-operating characteristic curve of the logistic regression results.
Comprehension receiver-operating characteristic curve of the logistic regression results.
Letter-Number Sequencing receiver-operating characteristic curve of the logistic regression results.

Picture Completion receiver-operating characteristic curve of the logistic regression results.
Digit Symbol Coding receiver-operating characteristic curve of the logistic regression results.
Block Design receiver-operating characteristic curve of the logistic regression results.

Matrix Reasoning receiver-operating characteristic curve of the logistic regression results.
Picture Arrangement receiver-operating characteristic curve of the logistic regression results.
Symbol Search receiver-operating characteristic curve of the logistic regression results.
Object Assembly receiver-operating characteristic curve of the logistic regression results.
Tables 5 6 present the importance of each subtest and RTW. The PIQ and VIQ were calculated for each group. Significant differences between groups were observed for only two subtests, and the remaining subtests revealed no significance. The Letter-Number Sequencing and Comprehension subtests demonstrated that the abilities associated with these tests were more important for RTW.
Multiple regression results of the VIQ
*p < 0.05.
Multiple regression results of the PIQ
*p < 0.05.
Table 7 presents the outcomes of the Cox regression indicating the association between early RTW and WAIS-III scores. The FIQ, VIQ, WM, PS, Letter-Number Sequencing, Comprehension, Digit Span, Symbol Search, and Block Design subtests were significantly associated with early RTW. In particular, the Letter-Number Sequencing and Comprehension exhibited the strongest association with early RTW.
Cox regression outcomes (odds ratio) between early RTW and WAIS-III subtest outcomes
*p < 0.05.
This study aimed to determine the abilities required for a successful early RTW in patients with TBI. The results revealed that the Letter-Number Sequencing and Comprehension subtests were associated with early RTW.
To evaluate the cognitive abilities following TBI, the examiners selected the WAIS from among a suitable battery of neurological tests. The WAIS is the most common test for assessing general intelligence. It was originally published in 1955, with a revised edition, the WAIS-R, published in 1981. The WAIS-III was published in 1997, whereas the WAIS-IV was published in 2008 [28, 30–32]. Furthermore, the Japanese edition of the WAIS-III was published in 2006 [33]. Accordingly, WAIS tests have been employed to evaluate patients with TBI [34, 35]. Previous reports have discussed that WAIS may or may not be used to predict RTW.
In a study that included 35 patients with severe TBI, Cattelani et al. demonstrated that the reemployment group (n = 19) exhibited significantly higher VIQ and PIQ scores than the non-reemployment group (n = 16) [21]. In a study including 45 patients, Ip et al. revealed that the PIQ score of the WAIS was the most significant RTW predictor in patients following TBI [23]. However, Jobnstone et al. reported contradictory results [22].
In this study, a higher FIQ and VIQ contributed to RTW, which is consistent with the results reported by Cattelani et al. However, no significant difference in the PIQ was observed between the two groups in our study. The PIQ is calculated from seven subtests, with time limitations in five of these subtests. However, the VIQ is calculated from seven subtests, with time limitations in only one of these subtests. Green et al. reported that the subtest without a time limitation is mainly used to determine the return to social activity in patients with TBI; furthermore, they reported that various activities with time limitations depend on the PS and can be compensated for to assign additional time [24].
The follow-up period of this study was 3 years, which we found to be sufficient for coordinating testing with working patients. We believe that this contributed to the lack of significant between-group differences in the employment status between the groups in this study, as shown on the PIQ.
The WAIS-III has a new value, factor structure, which provides additional details regarding cognitive ability [28]. In 1987, Kyllonen reported that WM and PS are important factors for learning [35]. Furthermore, the WAIS-III includes the Letter-Number Sequencing for WM and Symbol Search for PS [33]. Previous reports revealed that these factor structures are useful for diagnosing learning disabilities, attention-deficit hyperactivity disorder, or other cognitive impairment. WM is the development concept of short-term memory and the concept assumes the memory’s ability for PS.
Whereas WM evaluates the ability of a patient to keep and process short-term information, PS evaluates the patient’s ability to process visual information in daily tasks and work [33]. In this study, the WM and PS scores were significantly higher in the SRTW-G than in the USRTW-G and were found to be associated with early RTW. These results support the idea that learning is a necessary ability for early RTW.
Prior studies have reported a significant difference in the outcomes of the Similarities subtest between an employment group and a nonemployment group of TBI patients. In their study of 63 patients with mild to severe TBI, Green et al. identified optimal neuropsychological tests and timing strategies. The results revealed that the VIQ calculated from the Similarities subtest was useful for predicting a later return to productivity [24]. In the current study, multiple regression analysis revealed that Comprehension and Letter-Number Sequencing were useful predictors of RTW. However, the Similarities subtest was not significantly associated with RTW.
Comprehension is a required oral test used to evaluate a patient’s comprehension of social norms and his/her ability to resolve challenges of daily life [33]. It also evaluates a patient’s inherent ability to verbalize practical knowledge, learn from past experiences, and understand institutional social norms [36]. Comprehension is associated with the concept of crystallized intelligence, social judgment, language comprehension, language conceptualization, and common sense. Crystallized intelligence is measured using comprehension tests when based on previously noted fluid intelligence. Acquired skills and knowledge based on past experience are important for learning, particularly in school education [37].
The comprehension test has the characteristic that the increase in point is in accordance with the age and overall life experience.
Thus, our study results could have been affected by the accumulation of reasoning from past experience, which can increase the baseline ability of an older population with a high mean age.
The Comprehension test is an adequate fixed test, which is similar to the subtest of Information and Vocabulary; however, it has been reported to have low sensitivity in TBI patients who do not have expressive language disorder [15]. In this study, the Comprehension test exhibited high specificity for RTW and easily detected an unsuccessful RTW.
Generally, the Comprehension test is highly correlated with the VIQ, and it is influenced by the patient’s education and life experience. Walker et al. reported the rate of RTW for each occupation category in 1341 patients with TBI. They demonstrated that successful RTW was associated with a less complex professional/managing work environment and a higher patient educational level [38]. The ability to perform commonsense decision-making from experience appears to be a required ability for RTW in patients with TBI. Consequently, we can confirm the patient’s residual ability using the Comprehension test.
The Letter-Number Sequencing subtest requires the patient to recall numbers in ascending order and letters in Japanese syllabary order with verbal directions. The Letter-Number Sequencing is a newly added subtest of the WAIS-III that evaluates WM and attention. It has been reported to reflect WM, fluid intelligence, short-term mastery and search, and expertise of Japanese syllabary and numerical characters [33, 37]. WM has been reported to detect the ability to repair the psychic phase of memory when performing complex tasks, such as logical consideration, comprehension, and learning. Baddeley reported the first model regarding WM [39].
In concrete terms, work tasks require the ability to use WM. If WM is inhibited, patients can learn to write notes or enter reminders on their mobile devices. In some cases, voice-recorded memos might be required to avoid multitasking at work. The ability to adjust to a new environment is reflected in the concept of fluid intelligence, as it demonstrates the ability to resolve new issues.
The scores of the Block Design and Symbol Search subtests of the PIQ were significantly higher scores in the SRTW-G than in the USRTW-G. However, multiple regression analysis did not reveal any significant difference. The Block Design subtest requires a patient to recreate a sample pattern using blocks. This test evaluates the patient’s visual perception from the whole design to each part and is configured based on the factor structure of perceptual organization [15]. In the current study, the results of the Block Design were divided into low- and high-point groups (Fig. 4). The following trend was observed: in patients with TBI, the Block Design subtest enabled easy differentiation of the score. Multiple regression analyses revealed no statistically significant differences compared with other subtests. Thus, we found that the Block Design test is a nonlinguistic intelligence test that may contribute to the prediction of early RTW in TBI, although the effect is limited.
The Symbol Search subtest involves the identification of as many stimulus symbols (two types of symbols) as possible from the symbol group (five types of symbols) within a limited time. Symbol Search evaluates the patient’s visual processing speed, planning, and perceptual organization [37] and is configured to the factor structure of PS [15]. Similar to the results of the Block Design, although the outcome was limited, we believe that inhibited visual PS following TBI may have an effect on a patient’s employment.
As mentioned earlier, Green et al. reported that the Similarities subtest was associated with RTW in patients with TBI [24]. However, in our study, no differences in the outcomes of the Similarities subtest were observed between the SRTW-G and USRTW-G. The Similarities subtest has been reported to be the parameter associated with abstractive consideration and verbal ability. However, this subtest has only partial sensitivity with varied brain injury and, similar to the Vocabulary subtest, does not correlate with general intelligence [15]. The Similarities scores found in this study might have been affected by this partial sensitivity, as we did not restrict subject recruitment based on the brain injury location.
Our findings support the hypothesis that the subtests of the WAIS-III can reflect a TBI patient’s ability to RTW early and that follow-up evaluations of ability are important for early RTW in these patients. The ability to resolve a new problem, short-term memory, and maintenance of information processing are reflected by the Letter-Number Sequencing subtest. The ability to perform social judgment based on common sense is reflected by the Comprehension subtest.
Grauwmeijer et al reported that in patients with moderate or severe TBI, the rate of RTW between 3 months and 1 year following injury was higher than that of RTW between 1 and 3 years after injury [27]. Thus, we should consider that RTW can be difficult over time.
Whitnall et al. examined the factors inhibiting RTW in patients with TBI over a 5- to 7-year follow-up period. In the first year, the inhibiting factors were age, education, rehabilitation period, and productivity before injury. In the second year, age and productivity before injury were inhibiting factors. In the third year, age and functional independence measures were determined to be inhibiting factors. In the fourth year, age, especially age > 40 years, was an inhibiting factor [40]. Thus, regardless of the patient’s recovery over time, age might be a limiting factor for a successful early RTW. In our study, the average patient age was 41.7±11.0 years, which is higher than that reported in previous studies (Cattellani et al.: 24.5 and 22.8 years for the SRTW-G and USRTW-G, respectively; Green et al.: 39.98±14.91 years). This could be attributed to the fact that 25%of Japan’s population is older than 65 years [21, 41]. One study reported the importance of medical rehabilitation and community-based support to promote positive outcomes over the life span in patients with TBI [42]. Furthermore, due to the aging population, we may have to help older patients RTW. Consequently, future studies on RTW in TBI patients should be conducted in older individuals.
Study limitations
This was a retrospective study that evaluated the ability for early RTW in TBI patients. Our findings can help patients return to their usual social lives. However, this study had some limitations with regard to the prediction of RTW based on IQ using the WAIS-III. Because IQ reflects the patient’s current abilities and weaknesses, we can use it to create a rehabilitation plan and set personalized goals. However, several factors, such as the patient’s life and work, must be considered. The statistical analyses of this study included education, productivity be-fore injury, acute condition, rehabilitation period and details, family economic situation, psychological well-being, and regular follow-up of neuropsychological testing. To promote RTW following TBI, greater individual assessment is required [43–46]. Future studies are required to analyze these data accordingly. Furthermore, the reassessment of follow-up procedures is required to provide continuous support and evaluate changes in ability over time in patients with TBI.
Conclusion
This study confirmed that the Comprehension and Letter-Number Sequencing subtests of the WAIS-III reflect the ability for early RTW in patients with TBI. Solving a new problem, using short-term memory, processing information, and performing social judgment based on common sense from past experiences are important abilities for vocational rehabilitation following TBI. The outcomes of this study could enable the formulation of rehabilitation plans and political goal setting for patients attempting early RTW.
Conflict of interest
The authors declare no conflicts of interest.