
Abstract
BACKGROUND:
Multiple sclerosis (MS) is a neurological chronic disease that causes a number of physical, cognitive and emotional symptoms. The identification of these factors will allow mitigating unemployment and improve quality of life of patients. The Buffalo Vocational Monitoring Survey (BVMS) is a tool to characterize Work-Challenged patients.
OBJECTIVE:
To describe and analyze BVMS data in people with multiple sclerosis (PwMS) from Argentina. To study the association with physical, cognitive and psychiatric morbidity in employed patients, comparing the performance of MS Work-Challenged and MS Work-Stable patients, with and without accommodations.
METHODS:
119 MS patients were administered the Argentina adaptation of the BVMS, and completed measures of physical disability, fatigue, depression, cognitive processing speed, memory and verbal fluency.
RESULTS:
65.54% of the patients were employed and 19.32% were unemployed, the remaining having roles of housewife, students and disability retirees. Within the employed subgroup, 60.26% were working as employees and 39.74% were self-employed. Cognitive and clinical variables differentiate patients with and without negative events and accommodations (p > 0.05).
CONCLUSIONS:
This Spanish version BVMS is considered a new tool to monitor employment difficulties in Spanish-speaking MS patients. MS Work-Challenged had a higher depression, fatigue and worse performance in cognitive variables.
Background
Multiple sclerosis (MS) is a neurological chronic disease that causes a number of physical, cognitive and emotional symptoms and mainly affects young adults aged 20–40 years [1]. These symptoms should be analyzed in a social and work context in which the patient is immersed. In this regard, one of the main concerns of this population is related to their ability to work [2, 3]. Working conditions and employment are basic determining factors of health and wellbeing [4]. In the past years, market globalization has been affecting working conditions in developing countries such as Argentina. It has also led to different types of non-standard employment, which are usually linked to patient’s precarious employment conditions, and the appearance of new labor risks [5, 6]. In accordance with the Argentine Ministry of Production and Labour [7], this year 12,112,500 registered workers have been reported, from which 1,955,000 are self-employed (individual tax payer and freelancer) and 490,000 work in private homes. In order to validate the term ‘self-employed’ in other countries, in this study we will consider it as the subject who performs his profession or runs a business as an entrepreneur or is an independent contractor [8]. In Argentina, the term ‘self-employed’ is subdivided by their income into individual tax payers and VAT payers, the latter have a higher income. Besides, the National Institute of Statistics and Census of Argentina registered a total of 4,950,000 salaried employees who are not registered, which means they are informal workers in accordance with the last report [9]. Therefore, taking into account that most of the individual tax payers have a low income, lack an employment contract, and a large number of employees are not registered, the society shows a high percentage of precarious employment. This is reflected in Jimenez’s words [10] when mentioning that there is too much informality, involuntary part-time jobs, over-employment, temporary work and job dissatisfaction within the public sector and medium- and large-sized companies in Argentina.
In recent years, it has been shown that that MS has a high impact on the work situation of patients, given that the disease affects young people of working age with economic obligations that involve their families [11]. Clinical aspects of the disease such as physical disability and fatigue [12], as well as psychological variables [13, 14] and cognitive aspects [15, 16] have been associated with job loss or deterioration of working conditions. Cognitive alterations, which are found in approximately 50% of patients [17, 18], were identified as one of the main symptoms predicting the employment situation [19]. In a recent review, one of the most consistent findings was the difference in the speed of information processing among patients who were unemployed or who had reduced their work hours and those who did not have changes in their work situation [20].
In addition to the job loss reports, other aspects that significantly affect patients, that is to say, work events considered negative, have been analyzed, for example, verbal reprimands or reduced responsibilities and the need to adapt the work field to perform the usual tasks [2, 21]. These adverse work events can be prevented or delayed by identifying the risk factors and possible strategies to deal with the situation in a better way [22]. Workplace accommodations can help people with MS deal with their illness and can be beneficial to improve performance. Examples include flexible work policies and practices, special equipment, ergonomic conditions and modifiable work schedules and tasks [23].
The combination of global reports of unemployed patients with MS [24–26] and the current working conditions in Argentina urged our team to study the employment status of patients with MS. In Argentina, no studies that analyze the labor quality of patients with MS have been reported. Such studies would be beneficial to suggest and supervise the incorporation of more appropriate behaviors and attitudes for the better functioning of the patients in their work environment.
Benedict et al. [2] have developed the Buffalo Vocational Monitoring Scale (BVMS) to characterize the patients’ work difficulties. It has been reported that this scale is useful to identify at-risk patients and study qualitative aspects of employment such as work events considered negative and the accommodations used, among other aspects [21, 28]. But considering the work situation and the quality of working conditions in Argentina such as informal work and/or temporary employment, among others, the BVMS has not only been validated in our setting, but it has also been adapted by incorporating mainly the self- employed. Due to this, the objectives of this work were to describe and analyze BVMS data in people with MS from Argentina and to study the relationship between negative events and job accommodations with the clinical and cognitive variables of the employed patients with MS.
Material and methods
Study design and participants
119 MS patients were recruited from two MS Clinics in Buenos Aires, Argentina. The participants were selected following the incidental strategy of non-probabilistic sampling. All participants who attended the neurological consultation and who met the inclusion and exclusion criteria were invited to participate. The local Ethics Committee and an independent institutional review board of Ramos Mejia Hospital and Neurosciences Institute of Buenos Aires –INEBA approved the study. All participants provided signed informed consent. A cross-sectional study of descriptive and analytical type was carried out.
Inclusion criteria for the MS group were a diagnosis of clinically defined MS [30], 18–60 years old, fluency in Spanish, and ability to provide informed consent for all procedures. Exclusion criteria were patients who were unemployed because of the current social situation in Argentina, such as closing factories or businesses, current or previous neurological disorder other than MS, history of psychotic disorder, current psychiatric disorder related to mood, personality, or behavior changes following the onset of MS (except for depression), a medical condition that might affect cognition, a history of developmental disorder, a history of substance or alcohol dependence, current substance abuse, motor or sensory disability that might interfere with test performance, and having experienced a relapse and/or corticosteroid pulse in the previous 4 weeks of assessment. Table 1 shows the demographic, clinical and cognitive data of the entire population of patients studied.
Demographic, clinical and cognitive data of the multiple sclerosis population
Demographic, clinical and cognitive data of the multiple sclerosis population
Notes: MS: Multiple Sclerosis; SD: Standard Deviation; EDSS: Expanded Disability Status Scale; BDI II: Beck Depression Inventory II; FSS: Fatigue Severity Scale; MSFC: Multiple Sclerosis Functional Composite; BICAMS: Brief International Cognitive Assessment for Multiple Sclerosis; SDMT: Symbol Digit Modalities Test; CVLT: California Verbal Learning Test; BVMT-R: Brief Visuospatial Memory Test Revised; BRB-MS: Brief Repeatable Battery for MS; PASAT: Paced Auditory Serial Addition Test; WLG: Word List Generation.
The BVMS was used to study employment status [2]. In order to adapt it to the Argentine population, a linguistic and conceptual adaptation was carried out according to the International Test Commission (ITC) [31], for which the following stages were considered: (1) Translation: it was carried out by two bilingual translators who translated the original instrument independently. It was carried out according to the double translation methodology, from English language to Argentine Spanish. (2) Conceptual equivalents: the versions obtained were evaluated by a jury made up of four judges. Each one of the members of the jury compared the suitability of the adaptation of each item independently. (3) Pilot testing: Finally, the BVMS was administered to a pilot sample of 15 subjects to examine the clarity of the items and the instructions of the survey. Based on the suggestions of the experts and the observations made by the participants of the pilot study, the final version of the BVMS was obtained.
The BVMS consists of four sections: demogra-phic questions, characteristics of the disease, descriptive information on employment, and negative work events and accommodations and two self-reported disability surveys: the Multiple Sclerosis Neuropsychological Questionnaire (MSNQ) [32] and the Patient Determined Disease Steps (PDDS) [33]. Regarding negative events, participants are asked to answer “yes” or “no” to questions related to poor performance or errors at work in the last three months: (i) verbal criticism for errors (from a supervisor or co-worker), (ii) reduced working hours, (iii) elimination of responsibilities, (iv) formal discipline, (v) need for additional support or training and (vi) need to work additional hours to complete their job tasks. Participants are also asked to select the accommodations they use at work to facilitate their performance from a list of 38 items; if they are using an accommodation that is not listed, they can add it.
Cognitive status was assessed using the Spanish adaptation of the Brief International Cognitive Assessment for MS (BICAMS) Battery [34, 35]. The procedure began with the Rao adaptation of the Symbol Digit Modalities Test (SDMT) [36], in which a series of nine abstract geometric symbols were displayed on a standard sheet of paper, each paired with a single digit in a key at the top of the page, followed by several rows of unpaired symbols. Over a period of 90 seconds, participants were asked to speak aloud the digit associated with each symbol as rapidly as possible. There was a single outcome measure: the number of correct answers obtained over the 90-second time span. The official BICAMS battery would next include the California Verbal Learning Test (CVLT) II [37], but for our purposes the Spanish version of the CVLT I [38] was used to provide a meaningfully equivalent assessment. This test began with the examiner reading a list of 16 words. Participants were asked to listen to the list and recall as many items as possible, in any order. Afterwards, the entire list was read again followed by a second attempt at recalling the words. This procedure was repeated three times for a total of five learning trials altogether. The outcome measure was the total number of recalled items over the five learning trials, thus yielding a range of scores from 0 to 80. Finally, the Brief Visuospatial Memory Test-Revised (BVMTR) [39] was administered. In this task, a page displaying six abstract designs was held in the patient’s view for ten seconds. The display was then removed from view and participants were asked to render the stimuli manually with a pencil on a sheet of paper. Each drawing received a score of 0–2 points, representing location and accuracy. Thus, each trial score ranges from 0 to 12. There were three learning trials, and the primary outcome measure was the total number of points earned over the three learning trials. Form 1 was used for the test procedure [39]. The The Rao Brief Repeatable Battery for MS (BRB-MS) was also administered, validated in prior research [17]. The 7/24 Spatial Recall Test [40] was employed to measure visual memory. The 7/24 also included a measure of total learning and delayed recall. The Paced Auditory Serial Addition Test [41] administered using the Rao adapted 2- (PASAT-2) and 3-second (PASAT-3) inter-stimulus interval [42] was applied. Finally, a word list generation task (WLG) [43] was administered.
Neurological disability was assessed with the Clinical-rated Expanded Disability Status Scale (EDSS) and the Multiple Sclerosis Functional Composite (MSFC) [44]. Patients complete the Timed 25-Foot Walk, the 9-Hole PegTest (9-HPT) MSFC, and the PASAT at a 3.0 interstimulus interval [45].
Depression was measured with the Beck Depression Inventory second edition (BDI-II) [46] adapted to Argentina by Brenlla & Rodriguez [47] and Fatigue Severity Scale (FSS) [48] was used to evaluate the degree of fatigue. Both are self-report surveys administered in Spanish.
Statistic analysis
The data were analyzed with the statistical package SPSS version 20.0. Descriptive analyses of all the included variables were carried out.
To analyze the differences in work, clinical and cognitive aspects between employed and unemployed patients, Independent samples t-Test were performed. Likewise, in order to compare the scores of patients in the clinical and cognitive scales between those who had negative work events or accommodations and those who did not, a Student’s T test was also performed. We considered the presence of one or more negative work events and up to three and / or three or more work accommodations to compare the groups. The use of accommodations according to their characteristics was also analyzed, grouping them into cognitive (e.g. memory aids) and physical (e.g. closer parking) types, considering the categories described by Frndak et al. [21].
To describe the results of employed patients, we classify the patients based on previous studies [21] incorporating the modifications of the Argentine adaptation. We use the concept “MS Work-Stable” (n = 59) to talk about employed patients (either as an employee or self-employed), with no disability benefits, and no negative work events; and “MS Work-Challenged” (n = 19) to talk about employed patients (either as an employee or self-employed) reporting at least one negative work event at the time of clinical assessment.
To optimize the analysis of the variables, a factor analysis was carried out, from which two factors emerged, the clinical factor and the cognitive factor. The clinical factor was made up of four indicators, physical disability through the EDSS, fatigue with the scale, FSS, the BDI II depression scale and manual dominance, measured by the 9-Hole Peg. It showed a Cronbach’s index of 0.57. While the cognitive factor is made up of seven indicators, speed of information, SDMT, attention measured through PASAT-2 and PASAT-3 seconds, verbal memory with the CVLT test and visual memory, the BVMT-R and 7/24 and verbal fluency, yielding a Cronbach’s index of 0.86. The seven cognitive indicators make the factorial analysis a one-dimensional structure, taking into account the criteria of Kaiser, Carmines, Hattie and Gorsuch [49–52], with a high Cronbach’s index.
Results
In the population described in this study, 65.54% (78) of the patients were employed, 19.32% (23) were unemployed, 4.20% (5) were disability retirees and 10.92% (13) belonged to the group of housewives and students. Out of 65.54% of the employed patients, 60.26% (47) were working as an employee and 39.74% were self-employed, of which 24.36% (19) were informal workers (e.g. cosmetologist, masseur, babysitter, clothing salesman by catalog) and 15.38% (12) were freelance professionals (e.g. lawyer, architect, computer technician, music teacher, psychologist).
When analyzing the demographic and clinical variables and the cognitive performance of the patients employed in comparison with the unemployed patients, significant differences were found in the cognitive functions. The performance of the employed patients was superior in the visual memory task BVMT-R (t = –2.63, p = 0.01), and in the SDMT information processing speed tests (t = –2.26, p = 0.04), PASAT 3 seconds (t = –2.24, p = 0.03), and PASAT 2 seconds (t = –2.50, p = 0.01). No statistically significant differences were found in the clinical aspects or in the demographic variables. The demographic, clinical and cognitive data of employed and unemployed patients are shown in Table 2.
Demographic, clinical and cognitive data. Comparison between employed and unemployed patients
Demographic, clinical and cognitive data. Comparison between employed and unemployed patients
Notes: MS: Multiple Sclerosis; EDSS: Expanded Disability Status Scale; BDI II: Beck Depression Inventory II; FSS: Fatigue Severity Scale; MSFC: Multiple Sclerosis Functional Composite; BICAMS: Brief International Cognitive Assessment for Multiple Sclerosis; SDMT: Symbol Digit Modalities Test; CVLT: California Verbal Learning Test; BVMT-R: Brief Visuospatial Memory Test Revised; BRB-MS: Brief Repeatable Battery for MS; PASAT: Paced Auditory Serial Addition Test SD: Standard Deviation, *p < 0.05.
On the other hand, when studying more specific aspects of the employment situation regarding employed patients who work as an employee, it revealed that 19.14% of the patients reported at least one negative event. Out of all these patients, 14.89% reported they have had a decrease in their working hours, 10.64% had to request to work additional hours to complete their tasks, 8.51% received verbal criticism, 6.38% were obliged to train, 6.38% disciplinary measures and 4.26% reported reduced responsibilities. When analyzing the differences between patients who had a negative event in their work (MS Work-Challenged) and those who did not (MS Work-Stable), it was found that there are significant differences in the depression symptoms (t = –3.47, p < 0.01), fatigue (t = –2.14, p = 0.04), in the clinical factor (t = –3.25, p = < 0.01) and in the cognitive factor (t = 2.66, p = 0.01). In this way, MS Work-Challenged had a higher presence of signs of depression and fatigue and a higher severity score in the clinical factor and a significantly worse performance in the tasks that make up the cognitive factor. Fig. 1 shows the results obtained in MS Work-Stable vs MS Work-Challenged.
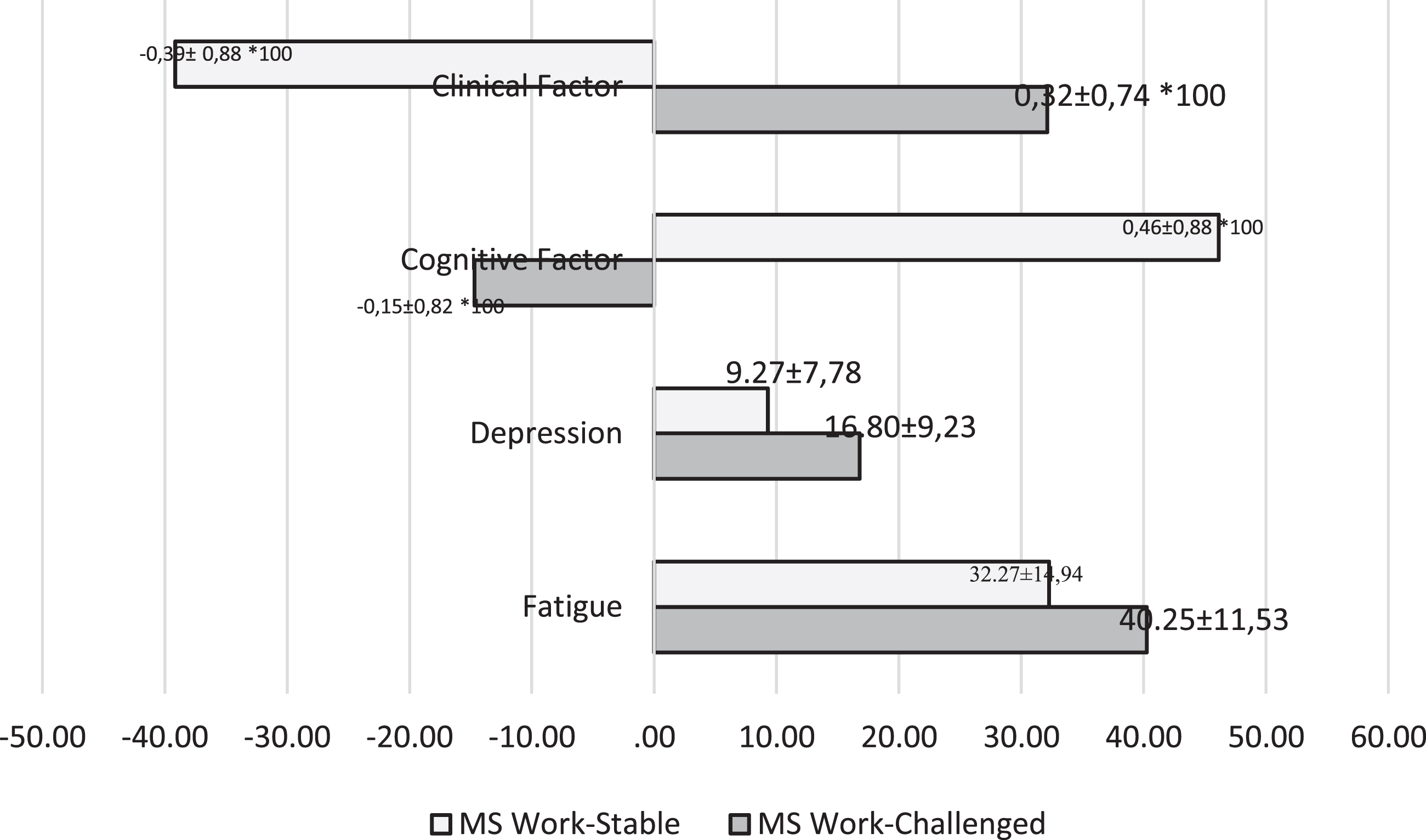
Performance in the clinical and cognitive variables: Comparison of patients of MS Work-Stable and MS Work-Challenged. Notes: Only significant results are shown. The value of the variables clinical factor and cognitive factor was multiplied by 100 in order to be better demonstrated graphically.
Regarding work accommodations, 53.84% (42) reported they have made three or more of them. It was evidenced that the most frequently used accommo-dations include flexible working hours, the use of external aids for memory, access to the refrigerator and use of air conditioning. When studying the differences between those patients who made accommodations in their work and those who did not, we found that the years of progress (t = 3.08, p < 0.01), the SDMT (t = –2.02, p = 0.04), BVMTR (t = –2.37, p = 0.02), and the cognitive factor (t = –2.18, p =0.032) are the variables that significantly differentiate them. The patients with accommodations had a better score in the speed tests of information processing, in visual memory and in the cognitive factor, as well as having fewer years of disease progress. In a sub-analysis, accommodations were grouped into cognitive-type accommodations and physical-type accommodations. Regarding the former, when analyzing the differences among those patients who used some adaptation of cognitive type and those who did not, it was found that there are significant differences with better performance in SDMT (t = –2.45, p = 0.02), in visual memory both in the BVMTR test (t = –2.23, p = 0.03) and in the 7/24 visuospatial test (t = –2.04, p = 0.04) and in the cognitive factor (t = –2.26, p = 0.03). While no significant differences were found among the variables considered when analyzing the use of physical accommodations. These results are shown in Fig. 2.
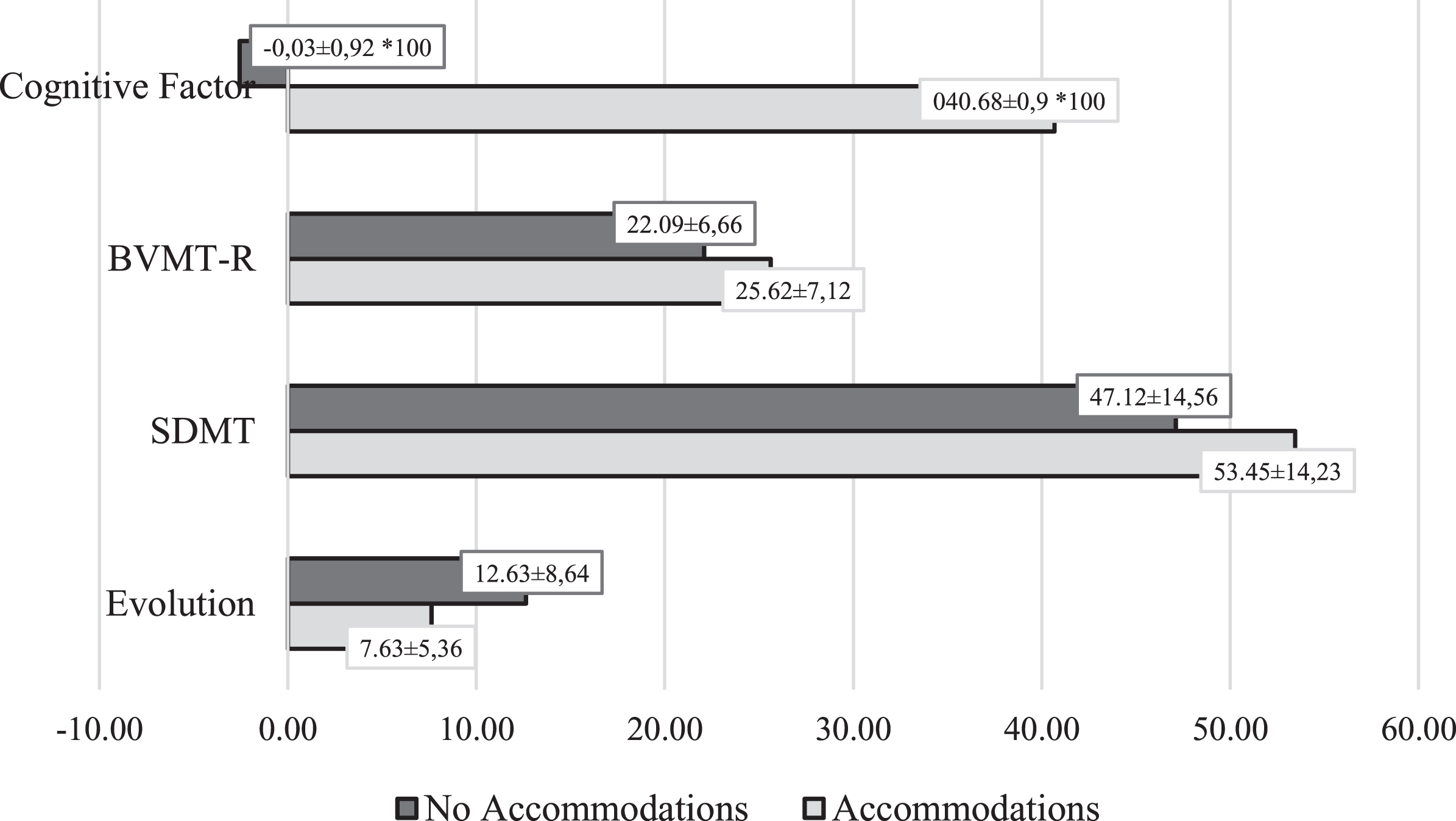
Performance in the clinical and cognitive variables: Comparison of patients with and without accommodations. Notes: Only significant results are shown. The value of the variable cognitive factor was multiplied by 100 in order to be better demonstrated graphically. SDMT: Symbol Digit Modalities Test; CVLT; BVMT-R: Brief Visuospatial Memory Test Revised.
The employment status study of MS patients has become relevant worldwide because of the impact it has on the quality of life. The clinical and cognitive variables have an impact on employment, but not only in the presence or lack of employment, but also on employment types and quality. The obtained findings indicate that 65.54% of patients were employed, while 19.32% were unemployed, 4.20% were disability retirees and 10.92% belonged to the group of housewives and students. In this study, the main cause of unemployment of these patients is their disease, and this finding is lower than that obtained in other countries. This variation depends not only on the clinical variables of the disease, but also on methodological aspects. Regarding the variables of the disease, its stage and its clinical presentation can be mentioned; Krokavcova et al. [24] reported 56.5% unemployment, and 31% of the sample were progressive forms of the disease, while in this study only 9.24% were progressive forms [24]. In relation to the degree of physical disability, Strober et al. found that in a sample of 101 patients 46.53% were unemployed, but the subjects of such sample had greater physical disability, measured by the EDSS, compared to this study [25]. On the other hand, in relation to the methodological aspect, the difficulty lies in the operationalization of the unemployment construct in the bibliography. For example, some authors include retirees and students in this category, while others exclude them [14, 53].
Another vicissitude arises when considering emp-loyment in some investigations as full-time or part-time paid job, which excludes patients with occasional jobs, or jobs that they develop independently, as well as housewives, students and volunteers. In this sense, Dorstyn et al. [14] explain in their review that most researchers do not use a reliable definition of unemployment and that according to the International Labour Organization (ILO) the employment concept should be operationalized to paid jobs, both full-time, part-time or casual basis [14, 54]. Adhering to this criterion, Honan et al. [55] separated the sample of 111 patients, similarly to this study, into salaried and non-salaried employees and found that 56% were employed, both full-time and part-time, in accordance with what was reported in our population. Another behavior considered is that of Benedict et al. [2] who exclude non-salaried workers and that of Frndak et al. [21] who exclude self- employees.
Regarding the self- employed patients, 24.40% were informal workers and 15.4% were freelance professionals. Currently, as mentioned in the background, in the Argentine population the presence of informal jobs and unregistered workers is evident, showing a precarious employment condition, given the lack of contracts and a lack of labor rights, such as health security, coinciding specifically with our population of self-employed informal workers. This point is fundamental since there is a need to cover the necessary medicines in this disease. In fact, according to Fernández Massi [56], both the trade and construction sectors in Argentina are characterized by not having the recognition of labor rights, unstable labor contracts and longer working hours than those defined by law and low salaries. While, in the social services sector, including education and health, there is a similar scenario, with the particularity that, according to the author, there is specific forms of unstable and poor working conditions such as internships. In conclusion, given the presence of self-employed, characteristic of Argentina, and a large number of housewives, students and retirees, the comparison with other publications with different realities regarding employment becomes cumbersome/difficult, but the reported findings reflect that the adaptation of the BVMT Scale has been beneficial to capture the entire spectrum of employees in our country, both employees and self-employed.
Regarding the events considered negative in this study, 24.3% of patients report at least one negative event; this percentage is similar to that reported by Van der Hiele et al. [22] and Frndak et al. [27], although the latter used a threshold of two or more negative work events. Other authors reported higher percentages. Kordovsky et al. [28] found 30% of patients who reported negative events; however, in this study more patients with progressive forms were included, which could justify the difference. On the other hand, if we refer to the types of negative events reported, we find that, as in the previous literature [2, 21], the most frequent negative events have been the reduction in working hours, the need to work additional hours and the verbal criticism.
When analyzing the relationships between negative events and clinical and cognitive variables, it was found that both the clinical variables, such as depression, fatigue and the clinical factor, and the cognitive factor, discriminated between MS Work-Challenged for patients who presented negative events, and MS Work-Stable for those who do not. MS Work-Challenged had greater clinical and cognitive difficulties. These results are in agreement with that reported by Benedict et al. [57] who in one of the sub-analyses classify patients similarly to us, and find significant differences between Work-Challenged and Work-Stable patients in cognitive tasks such as PASAT and BICAMS tests and in clinical aspects such as walking. Although in our study no differences were found in the cognitive variables separately, they were found in the factor that groups them, which indicates that probably if the number of subjects in the groups were higher, this difference would appear. Regarding clinical variables, as in the research conducted by Van der Hiele [58], in this study no differences were found between walking times or mobility of upper limbs of patients as found by other authors [27, 57], although the latter, as mentioned above, included a greater number of patients with progressive forms, which would have greater impairment in their mobility. A significant difference was found in self-reports of depression and fatigue; patients with negative work events were more fatigued and with more episodes of depression, which is concordant with that reported by the pioneering study by Benedict et al. [2] and with other publications that analyze this relationship [28, 57].
In relation to the accommodations used by patients in the workplace, flexible working hours, cognitive aids such as the use of external aids for memory, and physical changes such as access to the refrigerator and the use of air conditioning stand out. Regarding the possibility of having flexible working hours, previous studies have reported similar findings [2, 28]. Furthermore, these results are also found in studies that administer another instrument for assessing accommodations [23, 59]. Frndak et al. [21] emphasize that patients use more physical than cognitive accommodations, but their sample included more patients with physical disabilities.
When assessing the use of accommodations re-garding the cognitive performance of patients, this research found significant associations between them. They were associated with better performance in the speed of information processing, visual memory and cognitive factor. In this sense, Frndak et al. [27] reported, in a sub analysis, that patients with worse cognitive performance were the ones who used fewer accommodations. In contrast to these findings, Benedict and colleagues [2] reported that patients with worse performance in an information processing speed test had more accommodations and also found an association with motor tests, although the sample included a much smaller number of patients than this study. Other authors found no differences in the use of accommodations among patients with cognitive difficulties [22].
All gathered patient’s demographic, cognitive or clinical data will allow healthcare professionals to identify those patients predisposed to experience alterations in employment conditions, and also to recognize the resources required to keep their employment or get it back, for those who have lost it. We estimate that these findings are fundamental in a society where precarious employment is gradually increasing. Likewise, the results reported in this study reveal that the Argentine adaptation of the BVMS Scale is beneficial for investigating the entire spectrum of the country’s employment status and negative events, which, when considered in time, can reduce the job loss risk. Moreover, given that the results obtained regarding associations with clinical and cognitive variables are similar to those reported in the population where the scale has been developed, it is considered reliable to be used in the Argentine population.
One of the limitations of this study was the impossibility to enroll a larger amount of patients with progressive clinical forms as well as the difficulty of comparing the results with countries with socioeconomic characteristics similar to Argentina.
Footnotes
Acknowledgments
We thank Marinangeli Aldana, Merino María de los Angeles, Pita Cecilia, Saladino María Laura and Silva Berenice for collaboration in the administration of neuropsychological and clinical tests and scales.
Conflict of interest
None to report.
Funding
The contents of this manuscript were developed with support through the Scientific Programming 2018-2019 of Science and Technology of the University of Buenos Aires –UBACyT –(Grant Number: 20020170200264BA). [Programación Científica 2018-2019 de Ciencia y Técnica de la Universidad de Buenos Aires –UBACyT.]