
Abstract
BACKGROUND:
Perinatal loss affects many parents in the workforce. Yet, current knowledge about their workplace experience while facing this difficult event is sparse.
OBJECTIVES:
The goal of this study was to review and synthesize the extent of scientific literature on the specific experiences of workers coping with perinatal loss and the resulting bereavement.
METHODS:
A scoping review was carried out using eight different databases. A total of 15 references, all using a qualitative methodology, were identified.
RESULTS:
Most of the references focused on the experience of mothers and on late perinatal loss (from the 20th week of pregnancy). All references highlighted the taboo and the non-recognition of perinatal grief and bereavement in both organizational practices and interpersonal relationships with colleagues and immediate supervisors. They also emphasized the difficulties associated with returning to work after the loss and the significant changes in the meaning attributed to work.
CONCLUSIONS:
While the studies included in this review clearly indicate that perinatal loss can affect working life, larger, quantitative studies are needed to quantify this phenomenon and its impact on employees and their organizations.
Introduction
Perinatal loss refers to the death of a child occurring during pregnancy, childbirth, or the first 28 days of life [1]. Each year, nearly one in five pregnancies end in miscarriage (fetal death during the first 20 weeks of pregnancy), stillbirth (death after the 20th week of pregnancy or after reaching 500 g), or neonatal death (infant death during the first month of life) [2]. These figures may be even higher since early miscarriages are often not reported or tracked. Perinatal loss is a difficult event for parents, and many studies have reported its negative effects on their mental health [3–5]. Studies have also indicated that in some cases, symptoms of depression, anxiety, and grief may persist for more than a year after the death [6, 7].
Most parents facing perinatal loss are in the workforce and must return to work with few or no days off. Indeed, in some countries (e.g., Canada, United Kingdom), a fixed number of weeks of maternity leave are available if the death occurs after the 20th week of pregnancy, while no leave is usually provided for fathers or parents experiencing a miscarriage. However, given the duration and intensity of this type of bereavement, many of them return to work duties while still experiencing a significant level of psychological distress, which further impacts their well-being and functioning at work [8]. Despite the frequency and importance of perinatal loss, very few studies have documented its impact on parents’ workplace experiences. To date, studies on workplace bereavement have focused on other forms of loss, such as the loss of a loved one. Those studies all point in the same direction: grief is considered taboo in organizations and, more often than not, employees deal with it in silence [9–11]. This trend may be explained by the fact that grief-related reactions (e.g., sadness, anger, exhaustion) do not conform to expected reactions in the workplace [9, 12]. Grieving employees therefore seek to rein in their emotions as much as possible when at work [9]. This can be a difficult task, since, as the family to work spillover effect stipulates, the barrier between personal and professional life is not impermeable, and experiences and emotions related to the home domain transfer to the work domain [13, 14]. Thus, bereaved employees must expend great effort in concealing their emotions throughout the workday. This unrecognized and unexpressed grief in the workplace can have negative effects on employees (e.g., psychological distress, difficulty concentrating at work), their work teams (e.g., isolation from colleagues), and their organizations (e.g., productivity problems, workplace accidents) [15–17].
Like other types of bereavement, perinatal bereavement can also be difficult to deal with in the workplace. However, it involves several specific issues that are still poorly understood and under-recognized in society [18]. First, the fact that parents have had little or no contact with the child sometimes leads people to believe that it is not a genuine loss or that it is easier to deal with. However, the absence of shared memories with the child may make grieving even more difficult [19]. In addition, this type of loss is characterized by its sudden, unexpected aspect, diverging from the usual course of a pregnancy [20]. Parents may find themselves in a situation of dual grieving where they are grieving not only for their child, but also for their family plans and expectations [21]. Some authors have suggested that perinatal grief is a disenfranchised grief, which makes it even more difficult for parents to live with [10, 22]. Recent data indicate that, compared to medical, family, and social settings, the workplace is one of the environments where perinatal bereavement is least recognized [23].
Thus, studies are needed to better understand the specific experiences of workers coping with perinatal loss and the resulting bereavement. Although some studies have been conducted in this area [10, 24–28], it is still a new and under-explored research topic, and the scope of existing scientific literature is not well-known. This article therefore aims to fill this gap by undertaking a scoping review of the literature to review and synthesize the literature on the work experience of parents coping with perinatal loss.
Method
A scoping review was carried out following Arksey and O’Malley’s methodological framework [29]. This framework includes five stages: 1) identifying the research question; 2) identifying relevant studies; 3) selecting the studies; 4) charting the data, and; 5) collating, summarizing, and reporting the results. The review also complied with PRISMA Extension for Scoping Reviews (PRISMA-ScR) guidelines [30].
Stage 1: Identifying the research question
This study aimed to answer the following research question: What is the scope of existing scientific literature on the work experience of parents coping with perinatal loss? The main goal was to explore and synthesize the current literature on the subject in order to identify relevant research leads.
Stage 2: Identifying relevant studies
In order to answer the research question, a literature review was conducted from August to October 2018 in the following eight databases: MEDLINE, CINAHL, SocINDEX, Academic Search, PsycARTICLE, Scopus, Pubmed, and ProQuest. The ProQuest database, which lists theses and dissertations, allowed for searching the supplementary grey literature. The following keywords, identified and approved by all the authors of this article, were used for each of these databases: miscarriage, perinatal death, stillbirth, perinatal mortality, spontaneous abortion, perinatal loss, infant mortality, infant death, perinatal bereavement, perinatal grief, fetal death, pregnancy loss, neonatal death, work, employ*, career, job, occupation, and organization. Boolean operators were used to combine keywords. Database thesauri were consulted to augment the selected keywords.
To complete the search strategy, the reference lists of all selected articles were carefully reviewed to identify other relevant publications. Finally, the authors of key articles were contacted by email to find out if they had published any other articles on the subject that might not have been identified by our search.
Stage 3: Selecting the studies
The search covered the period from 1980 to 2019. This period is intended to be limited while taking into account the fact that research on perinatal loss flourished in the 1980s when there were significant advances, particularly with regard to the psychological repercussions of perinatal loss [31, 32]. The inclusion criteria were as follows: 1) studies using a qualitative or quantitative design; 2) written in English or French; 3) addressing both perinatal loss and the experience at work of fathers and/or mothers.
As shown in Fig. 1, a total of 2991 references were identified. After eliminating duplicates, 2511 references were retained. A first screening of these references was performed by a team member (DL) based on a review of the titles and abstracts. A total of 2474 references were excluded as they either did not deal with perinatal loss and the workplace (n = 2432) or were written in a language other than French or English (n = 42). Subsequently, two independent judges (DL and SZ) read the summaries of the remaining 37 references. As a result of this process, 19 were excluded because they did not directly address the experiences of workers following perinatal loss. Finally, the full text of the remaining 18 publications was read by two independent judges (SZ and SM). At this stage, three articles were excluded since they did not specifically deal with perinatal loss in the workplace (n = 2) or did not present any research results (theoretical article, n = 1). In the end, the results of this scoping review were based on 15 different publications.
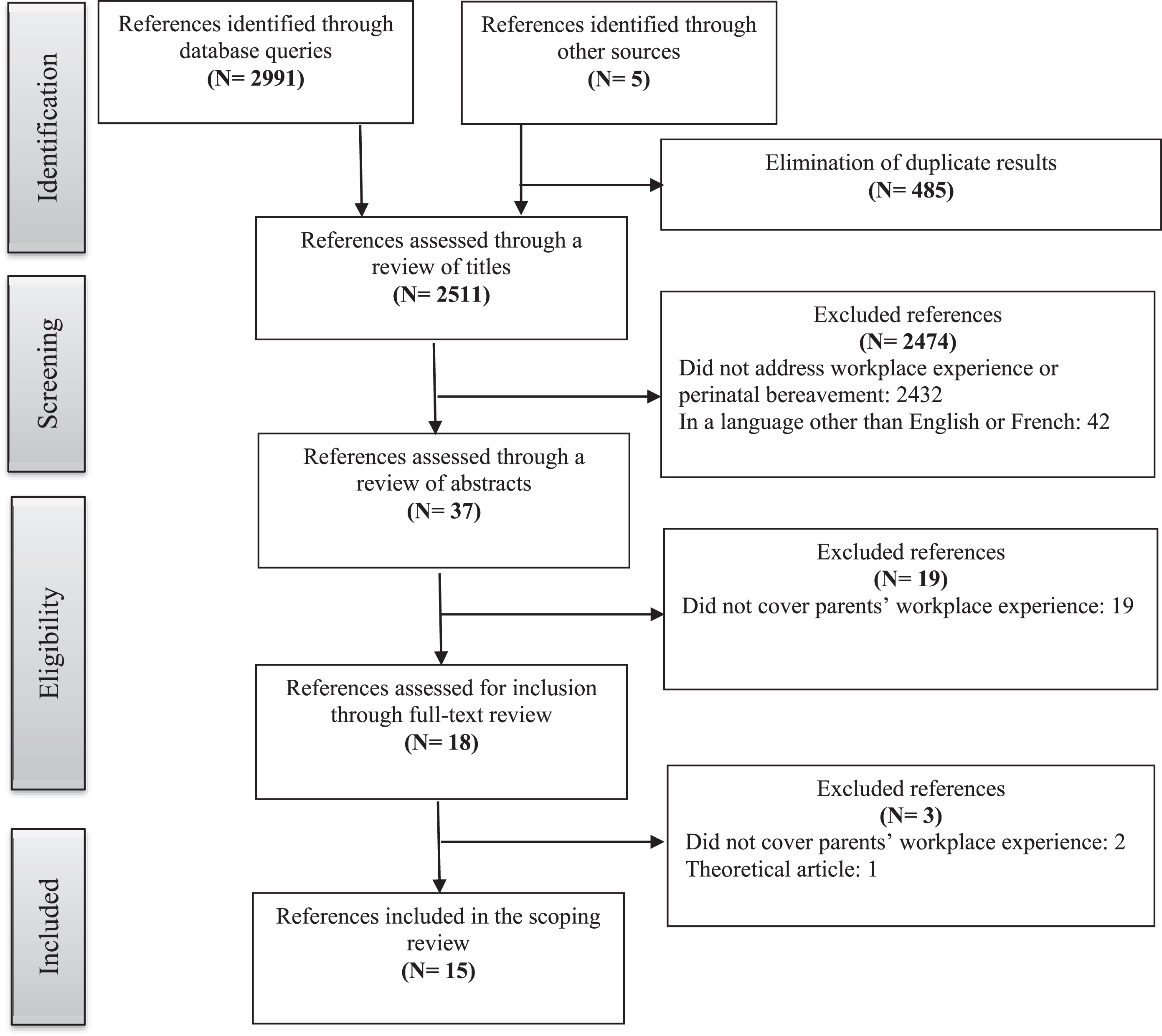
Flow diagram of articles identified and excluded according to PRISMA guidelines.
The relevant information from the references included in the review was compiled in an Excel table consisting of the following data: author(s), discipline, country where the study was conducted, year of publication, study objectives, methodology, population (gender of participants, job type, type of perinatal loss), main results, future research leads, and centrality of the topic. The table was completed in duplicate by two independent judges (SM and SZ).
Stage 5: Collating, summarizing, and reporting the results
The various characteristics of the selected publications were first synthesized in order to build an overall picture of the types of studies focusing on the experience of perinatal bereavement in the workplace. Subsequently, the main results of these publications were submitted to thematic analysis as described by Braun and Clarke [33]. Data on the experience of perinatal bereavement in the workplace were then carefully read to identify codes. These codes were grouped into different thematic categories, and data from each thematic category were collected. Finally, the data were systematically reviewed to ensure that each thematic category was assigned a title and clear definition that matched the coded data. It should be noted that the thematic analysis carried out in this scoping review was based on a framework that focuses on the subjective perspective of the persons concerned, namely the meaning they give to this experience, as well as on how the social context contributes to the structuring of this subjectivity. This is what Braun and Clarke [33] termed a contextualist framework.
Results
Description of the retained publications
The scoping review identified 15 publications, including 11 scientific articles, three theses, and one book chapter. Table 1 presents the characteristics of these 15 publications. They represented studies that were conducted mainly in North America: four in the United States [10, 34] and nine in Canada [23–27, 35–38]. Two other studies were conducted in Great Britain [39, 40].
Characteristics of included publications
Characteristics of included publications
All of the selected publications were qualitative empirical studies using various data collection methods: semi-directed interviews [10, 40], focus groups [24–27], auto-ethnography [28, 37], and open-ended questionnaires [39]. Sample sizes were also relatively consistent across most studies. Apart from the study by Brierley-Jones et al. [39], which included 162 mothers, all the others included samples of less than 30 participants. It should also be noted that among the 15 publications selected, one single sample resulted in four articles [24–27] and another sample in two articles [10, 11].
In terms of the type of perinatal loss, most studies focused on late death, i.e., from the 20th week of gestation. The only two exceptions were the article by Porschitz and Siler [28] on miscarriages, or early death (within the first 12 weeks of gestation), and the book chapter by de Montigny et al. [35], which involved fathers whose spouses had a miscarriage and/or stillbirth. The majority of studies also focused more on the experiences of mothers. Only three studies were either interested exclusively on fathers’ experiences [34, 35] or included both fathers and mothers in their sample [40].
Finally, it should be noted that perinatal grief in the workplace was a central topic in seven publications [10, 24–28], and a peripheral one in the remaining eight [23, 34–40]. In the latter studies, perinatal loss was studied in a more global way, the sphere of work being one of several examined. In articles where the workplace was more central, the participants’ job types were more fully described and encompassed a wide range of sectors: education, health and social services, the financial sector, construction, and private companies.
The thematic analysis, detailed above, made it possible to describe the experiences of working parents at three levels: organizational, interpersonal, and individual. Each of these levels is described next.
Organizational level: Established practices
Organizational practices play an essential role in the experience of bereaved parents returning to work after a perinatal loss [11, 25]. These practices are primarily shaped by the requirements of labour laws. The articles that addressed this point were all based on studies conducted in Quebec, Canada. In this province, the Quebec Parental Insurance Plan (QPIP) stipulates that a mother may take her 18-week maternity leave if the baby dies at 20 weeks of pregnancy or more. Below the 20-week threshold, no leave is provided. Accordingly, the mothers interviewed in the study by Zeghiche et al. [23] reported that this practice was well recognized and had been applied in their workplace. However, for many, this prescribed time limit can sometimes seem rigid. As for fathers, they are not entitled to paternity or bereavement leave when the baby dies before birth. If they feel the need to take leave, they must take sick leave or leave without pay. Not surprisingly, the chapter by de Montigny et al. [35] indicates that many of them therefore return to work while they are still experiencing intense grief symptoms, which consequently affects their functioning at work.
In addition to this legislated practice, some studies also addressed other organizational practices that can be implemented based on collective agreements or employee needs. In this regard, the results of the article by Gagnon et al. [27] concluded that almost none of the 55 collective agreements analyzed provided for perinatal bereavement leave (paid or unpaid) beyond the maternity leave provided for by law. While almost all of the collective agreements analyzed (52/55) provided for very short bereavement leave (2 to 5 days) for parents upon the death of a child, only four provided mothers with three weeks in the event of pregnancy termination before 20 weeks’ gestation [27]. Moreover, stated practices did not always correspond to implemented practices. In the Jones’ study [40], several participants reported that they took days off on their own initiative, without it being offered by their organization. Similarly, of the nine mothers interviewed in the Gagnon and Beaudry study [24], more than half were not offered the extended leave option, despite stated practices. Some even indicated that their employer put pressure on them to return to work sooner, simply not respecting the leave provided for by law. For others, this option was not feasible because it entailed a loss of salary or loss of employment. In all, only two were able to take advantage of this leave, with their employer recognizing the importance of letting them take a period of rest. In addition, nearly half of the mothers found that the leave they were taking was not long enough [26].
Gradual return to work was also identified as an element that can be helpful to ensure that employees can resume their professional activities without becoming exhausted, thereby supporting their professional reintegration process [26]. However, Gagnon and Beaudry’s study [26] with nine participants indicated that the possibility of a gradual return to work was approved in only three cases, was refused for two more, and was not feasible for another for financial reasons [26]. Yet, analysis of the collective agreements revealed that almost all contained a provision for gradual return to work after an absence for personal reasons [27]. As for the possibility of modified duties, only one participant was able to benefit from this option Similarly, only one participant was able to receive psychological support through the employee assistance program; for the others, either the option was not offered or their needs were assessed but ultimately there was no follow-through [26].
In short, the studies reviewed showed that there was sometimes a gap between stated practices and actual practices. Furthermore, even when there were certain organizational practices in place, they were often considered insufficient or inappropriate. At the same time, while organizational practices provide a framework for some aspects of a worker’s experience of perinatal bereavement, attention must also be paid to social interactions in the workplace that do not fall under the law or organizational policies but are part of norms that govern social relationships, in this case when death and bereavement intersect with work issues. The following theme provides insight into this area.
Interpersonal level: Support from colleagues and supervisor
After resuming their professional activities, parents who had experienced a perinatal loss had mixed experiences of social interaction with their colleagues or employer/supervisor. Thus, some parents felt genuinely supported by their supervisor, whether through listening, openness, or a willingness to adapt management practices to their specific needs [25]. Others reported that their supervisor had shown they recognized the importance of them taking time off to grieve [25, 26]. On the other hand, some mothers reported that their return to work had been particularly difficult because they had received insufficient social support from their supervisor [24]; they had to deal with indifference, as well as a lack of compassion. This was reflected in the fact that their supervisor focused on their productivity and performance, regardless of the suffering they were feeling, and refused their requests for gradual return to work, as explained above [23, 27].
Experiences with colleagues were equally mixed. For example, some mothers reported receiving support during their leave in the form of colleagues being present and assisting them with various daily tasks [23]. This support continued upon return to work, with some mothers reporting that they were well supported by their colleagues, who listened and empathized with them, including colleagues who were not very close to them, some of whom had had similar experiences [23, 40]. For her part, Forhan [37] recounted that several of her colleagues were interested in her experience and even asked her to turn it into a written testimony that could be used by others. Finally, Brierley-Jones et al. [39] found that some of the mothers they interviewed reported being treated by their colleagues with dignity, respect, and compassion.
This encouraging portrayal must be put into perspective by describing the instances where acknowledgement was lacking. Several mothers and fathers reported unease surrounding their interactions with their colleagues, who either avoided the subject or fled from them [23, 25]. Indeed, in addition to the lack of understanding from her colleagues, one mother reported sensing indifference, sometimes even from colleagues with whom she was close [25]. While some mothers reported insufficient support from colleagues, others reported awkward and hurtful comments, downplaying their distress [23, 40].
In fact, the issue of silence surrounding perinatal loss and bereavement in the workplace was the focus of several studies [11, 39]. According to Hazen [11], there are two dimensions to silence: silence imposed on bereaved parents (which she refers to as ‘silencing’) and silence that these parents internalize as a result in order to prevent this silencing. Thus, there is active silence and passive silence. Active silence is when colleagues (among others) act as if nothing has happened, as if it were a non-event [39]; in other words, as if the death had not occurred and the child had never existed. On this subject, Weaver-Hightower recounts: ‘It would take weeks before some of my colleagues even mentioned Matilda’s death, and many never have.’ [34, p. 484]. Similarly, Brierley-Jones et al. [39] explain that avoidance is a common reaction faced by the mothers interviewed in their study. They cite one of the mothers: ‘Work colleagues have been the hardest though as some have literally tried to avoid any conversation with me and have totally ignored what has happened’ [39, p.153].
Passive silence is behaviour that parents internalize because of the active silence imposed on them in order to prevent awkward remarks or discomfort generated by the subject of perinatal loss. For example, Hazen [11] explains that many of the women interviewed learned to keep quiet, to swallow their words or emotions, or to reserve them for support groups, psychotherapists, or online platforms. Porschitz and Siler [28, p.566] echo this sentiment, stating that they both decided to hide their miscarriages from their colleagues and get back to work as if nothing had happened: ‘We both kept our miscarriage secret from our colleagues, without questioning that impulse. (. . .) we had (strongly) internalized the societal and workplaces silences about miscarriage.’ Finally, Brierley-Jones et al. [39] explain that these situations of misunderstanding and ignorance on the part of colleagues led mothers to try to minimize unease in social interactions that resulted from their situation, for example by using euphemisms to refer to their leave or by avoiding mentioning their babies’ names in conversations with their colleagues.
How can this silence be explained, and what consequences might it have? The two studies by Porschitz and Siler [28] and Brierley-Jones et al. [39] provide different but complementary perspectives on this subject. Brierley-Jones et al. [39] use Goffman’s theory [41] of stigmatization to explain that perinatal death, represents as it does a move away from the ‘normal’ or ‘expected’ scenario, is therefore perceived as having gone ‘off script’ or being an “unscripted” event. This situation often leads to confusion and disintegration of social interactions, which leads to social exclusion, of which silence is one manifestation. Porschitz and Siler [28] shed more specific light on the professional context by highlighting several reasons for this silence: 1) Miscarriage is considered an illegitimate bereavement, compared to other more normalized bereavements such as the death of a parent; 2) Women wish to avoid professional discrimination related to the reproductive function of women’s bodies, of which miscarriage is a manifestation; 3) The social norms governing professional interactions establish a clear separation between the intimate and private sphere (to which miscarriage belongs) and the public sphere; 4) Silence can be a strategy to protect against the awkward comments that this topic can generate if it is discussed.
However, this silence comes at a cost. While Brierley-Jones et al. [39] mention the guilt that results from concealing the existence of one’s baby so as not to have to face the discomfort that perinatal loss causes, Hazen [11] lists the psychosocial consequences: depression, fraying social relationships, shattered careers, missed professional opportunities. As she puts it very well: ‘Silences impact not only the individual grieving woman, but also work group relationships and the organization’s effective accomplishment of its mission’ [11, p. 245].
Thus, depending on whether social interactions are positive or negative, work can represent either an opportunity to share one’s experience of bereavement, to better understand the perinatal bereavement process, and to heal [24]; or a hostile space that isolates bereaved employees, exacerbates their suffering, and perpetuates the conspiracy of silence surrounding perinatal bereavement [11, 39].
Beyond social interactions, perinatal loss calls into question parents’ relationship to work, at first with respect to their motivations to return (or not) to their professional occupation, and then in the meaning they give to work in general, and to their occupation in particular. This often leads to a rethinking of priorities, which can sometimes lead to a career change. These issues are discussed in the next theme.
Individual level: Motivation and meaning of work
The motivation that drives someone who has lost a baby to return to work varies from one person to another. For some, the motivation is mainly financial, due to the loss of income that can result from extended unpaid leave; for others, there is social pressure, real or perceived, to return to work [26]. This pressure may manifest in different forms depending on whether it is aimed at women or men. Women may feel judged for being on leave when they do not have a baby to care for [24]; while men may feel compelled to be strong and take up work as a stepping stone to well-being [34]. The pressure may also come from contextual requirements, such as in the academic environment where a prolonged absence can be detrimental to obtaining a regular faculty position [34], or from the professional conscience of a person who wants to fulfill their work responsibilities [24]. For some parents, returning to work is seen as beneficial since it takes their mind off things [35, 38] and promotes a better life and sleep routine [38].
It is reasonable to assume that the reasons for returning to work will significantly affect the experience of a person returning to work. Thus, their experience will be different depending on whether they return to work because they want to resume their professional responsibilities or because they feel under pressure, guilty, judged, or potentially penalized, in financial terms or in terms of career advancement. This is consistent with the distinction made by Beaudry and Gagnon [24] between intrinsic and extrinsic motivation. If the motivation is solely extrinsic, returning to work may be premature and may therefore negatively affect the individual’s professional activity. Indeed, in cases of early return to work, the various psychological distress symptoms of bereaved parents can interfere with the tasks they must perform [10]. Conversely, when motivation is intrinsic, work can help alleviate symptoms of bereavement.
At the same time, it is not unusual for a major life event such as a perinatal loss to cause an upheaval in the frame of reference, priorities, and perceptions of bereaved parents, particularly with respect to work. Expectations tend to change after a perinatal death. Some bereaved parents stated they wanted to give some social purpose to their profession; others explained that the event had transformed their relationship with others [24]. In other cases, a disconnect develops between the meaning of their occupation and their needs or values after experiencing perinatal death. This gap can be resolved over time, with changes in priorities. This was the case for Forhan [37] and for some mothers in Djiba’s [36] study, whose relationship to work changed significantly; personal family life became a much higher priority.
Sometimes the gap does not disappear and can lead those affected to a radical change in professional direction. This was the case for some of the mothers interviewed in the Beaudry and Gagnon’s study [24] and in Hazen’s study [10], who opted for careers in the field of helping relations, as well as for some of the mothers interviewed in the Jones’ study [40], who undertook volunteer activities to help other parents experiencing perinatal death.
Thus, we see that perinatal loss can profoundly change the relationship to work, open a gap between personal and professional values, call into question a grieving parent’s priorities or their occupation itself, and ultimately even lead to a change in career or vocation.
Discussion
The purpose of this study was to examine the extent of the scientific literature on the work experience of parents coping with perinatal loss. The results show that very few studies have focused specifically on this subject. Indeed, only 15 publications were identified, and of these, more than half dealt with perinatal loss in a more peripheral way, addressing the workplace only very briefly. As stated by Bento: ‘It is as if the taboo that surrounds the issues of death and dying in organizations also keeps people from studying, writing and reading about it’ [12, p. 2]. Nevertheless, the parents interviewed as part of the studies reviewed expressed a deep unease regarding their work environment and stressed the importance of improving existing practices. Moreover, while work appeared to be helpful in some cases, in many others it contributed to worsening grieving symptoms. This is therefore an important issue and calls for further research to identify the risk and protective factors that can facilitate these parents’ work experience and functioning. Although the qualitative studies that have been conducted to date have opened the door to exploring this topic, longitudinal quantitative studies are now needed to properly document the effects of perinatal loss on workplace experience and to examine these associations over time.
This scoping review also highlighted some of the gaps in the study of perinatal loss in the workplace. First, it can be seen that most of the studies reviewed were concerned only with perinatal deaths occurring after the 20th week of pregnancy. However, miscarriage, defined as occurring before the 20th week of pregnancy, is a very frequent event that affects thousands of workers every year. As with other types of perinatal loss, it is associated with significant adverse effects on the mental health of parents that may persist over time [6, 42] and therefore necessarily affect the professional sphere [28]. In fact, the only two studies that included mothers and fathers who had experienced a miscarriage in their sample also highlighted important workplace issues, particularly the tendency of parents to conceal the event, to act as if nothing had happened, and to expend considerable effort to maintain normal functioning, while being physically and psychologically affected by loss [28, 35]. In the same vein, a recent qualitative study conducted among women who have experienced a miscarriage indicated that most of them returned to work before being physically and psychologically ready, which necessarily impacted their functioning at work [43]. Future studies would therefore benefit by further investigating the effects of this type of perinatal death on parents’ work-related functioning.
Another important shortcoming highlighted by this review concerns the limited consideration given to bereaved fathers. Indeed, the majority of the selected studies focused on the experiences of mothers and only three studies considered fathers among their participants, including one auto-ethnographical study [34]. Yet, several studies have indicated that, although fathers sometimes face different issues (e.g., limited work leave, pressure based on masculinity norms, different coping strategies), they are just as affected by perinatal loss as mothers [44, 45]. At the same time, their reactions are not necessarily identical to those of mothers and it is not possible to generalize the experiences of one parent to those of the other [46, 47]. Future studies would therefore benefit from considering both fathers’ and mothers’ specific work experiences during perinatal loss and subsequent bereavement.
With respect to the themes addressed by the publications we reviewed, it is not surprising to note that, consistent with the current literature on workplace bereavement, one of the main issues that emerged was the taboo and unrecognized nature of perinatal loss. Indeed, the results indicated that, on the organizational side, practices to support employees experiencing perinatal loss were often non-existent, insufficient, or inadequate. While various agreements on working conditions typically provide for bereavement leave, which varies according to the worker’s proximity to the deceased, there is no specific leave for perinatal loss. In addition, while support measures were present (e.g., employee assistance program), they were not always available to employees experiencing perinatal death. Thus, while different practices exist to support employees when they experience personal difficulties, there is almost nothing specific in the case of perinatal loss. This reflects the marginal consideration given to this type of personal hardship.
As for colleagues and immediate supervisors, the support received was rather mixed: while in some cases colleagues and supervisors showed empathy and openness, in many cases parents encountered indifference, discomfort, or a lack of compassion. However, the support of others is not only valuable, it is necessary to resolve grief [48, 49]. Ignoring or failing to acknowledge grief in the workplace makes it even more difficult and can push many parents to keep silent about the event. This effort of emotional control is exhausting and can have a negative impact on parents’ mental health. Indeed, according to the theory of emotional labour, the divergences between emotions that are actually felt and the emotions that can be expressed at work may be linked to greater psychological distress [50], low self-esteem, cynicism, or depression [51].
Finally, the results of this scoping review highlighted the extent to which personal life events can influence professional life events. Indeed, for some parents experiencing perinatal loss, work became more significant and could act as an outlet to help in their bereavement. For others, personal life took up more space, and work became a lower priority or was shifted to a profession enabling them to help people with similar difficulties. Thus, the barrier between the personal and professional spheres is not as impermeable as one might think, and changes in one sphere can also lead to significant changes in the other.
In summary, although few studies have been conducted on perinatal bereavement in the workplace, the studies reviewed here already indicate various recommendations for practice. First, at the societal and organizational level, policies to better support parents coping with perinatal loss are needed. Indeed, absence of parental paid leave and financial concerns and are among the most likely causes of a premature return to work following a perinatal loss [43]. Also, given the idiosyncratic experience of perinatal bereavement and its non-linear trajectory, these measures should be flexible so that they can adapt to meet individual needs. To this end, Gagnon et al. [27] recommend a flexible work schedule to allow concerned employees to leave the workplace if they are overcome by feelings of grief. They also recommend introducing specific perinatal bereavement leave, which would be distinct from maternity leave granted in the event of perinatal death after 20 weeks of pregnancy, in order to better recognize the importance of this event for both parents and to meet their specific needs. While the support of colleagues and immediate supervisors also appears to be a crucial element, they often feel helpless in such situations. Therefore, Gagnon et al. [27] suggest that bereavement training be offered to colleagues and supervisors to better equip them to deal with these types of situations. Hazen [11] proposes including simple managerial techniques in these training sessions, such as active listening, which can be useful in the context of grief in general and perinatal grief in particular. According to her, it is employers’ responsibility to provide support to grieving employees and to work with them to minimize any negative effects on their work.
Conclusion
This scoping review was intended as a first attempt to bring together the existing literature on the workplace experience of parents coping with perinatal loss. The results obtained can be used to guide future research initiatives in this area. However, some limitations are worth mentioning. First, only English or French language publications were considered, thus eliminating other potentially relevant publications that might have been written in other languages. Furthermore, the studies reviewed were mainly from North America, which limits the generalizability of the results. In addition, several articles were based on data from the same sample or focused on the author’s personal experience (auto-ethnography). Finally, given the limited number of studies on the subject, the keywords used were rather broad (e.g. work, workplace) and yielded a large number of non-eligible references. Nonetheless, this allowed for in-depth research and ensured that certain relevant publications were not overlooked.
In conclusion, perinatal loss is a major life event that has significant effects on different spheres of life, including work. However, this topic is rarely addressed, whether in the workplace or in the research community. More research is therefore needed to break the taboos around perinatal bereavement in the workplace, to better understand the experiences of working parents, and to ensure that work can become an environment that can help them to cope with their grief rather than hinder them.
Footnotes
Acknowledgments
This research was funded by a grant from the Paternity, Family and Society team, funded by the Fonds de Recherche du Québec - Société et Culture (FRQSC)
Conflict of interest
None to report.