
Abstract
BACKGROUND:
Two patients received ocular injuries from rusted metallic projectiles at their industrial workplaces. Said injuries resulted in the loss of their eyes by evisceration surgeries to prevent fatal infections.
CASE DESCRIPTION:
The first case, a man in his twenties, received a stock conformer immediately after surgery and started prosthetic therapy within 2 months. The second case, a man in his forties, started prosthetic therapy after 10 years. Definitive custom ocular prostheses were fabricated and relined according to conventional protocol.
RESULTS:
On issue of the prosthesis, there was adequate retention, aesthetics and stability to extra-ocular movements and treatment was considered successful for both cases. However, follow-ups showed noticeable prosthetic eye movements for case 1 which, to some extent mimicked the physiologic movement of its fellow natural eye. Case 1 adjusted to his prosthesis better while case 2 was still adjusting with little to no physiologic movement.
CONCLUSION:
Prosthetic rehabilitation should be started as early as possible to obtain optimum rehabilitative results.
Introduction
Occupational ocular injuries are preventable however, despite all the safety and protection protocols in place, 31%of all accounted occupational injuries affect the eyes [1]. Occupational hazards to the eye range from foreign projectiles scratching the cornea to complete destruction of the globe. Chemicals and burn also play a role in the hazard [1–3].
When the eye is unsalvageable, complete surgical removal by evisceration surgery is performed to prevent fatal infections, gas gangrene, orbital cellulitis and a chance of cavernous sinus thrombosis [4, 5]. It is advised to start ocular prosthesis rehabilitation immediately after surgical removal to obtain the best possible aesthetic results, to avoid contracture of soft tissue, reduced socket size and depth, eyelid constriction, eyelid incompetence, and decreased residual muscle movement [6]. However, the patient’s emotional distress and financial restraint make the process quite challenging. Often, trauma counselling is given first priority to tackle emotional distress and patients delay seeking prosthetic treatment [7]. Thruston et al. mentioned five stages that the patient can go through after an eye loss with different time intervals between each stage. According to that, the patient is ready for rehabilitation step only at stage four [7]. By then, the soft tissue of the socket has undergone grade 4 (severe) contraction as classified by Tawfik et al., making the rehabilitation trickier [8]. This manuscript describes the rehabilitation process of two patients who faced identical workplace injuries. While one patient started prosthetic treatment immediately following evisceration, the other waited 10 years before starting treatment.
The basic steps of ocular prosthesis rehabilitation
The procedure of fabrication of custom-made eye prosthesis comprises different clinical and laboratory steps, and multiple visits and compliance from the patient [6]. The following steps are generic and describe the eye prosthesis fabrication for both patients. Impression of the eye taken: By injecting polyvinyl siloxane impression material into the eye socket until the adequate volume was obtained. The impression material was allowed to set while the eye is kept stationary, with vision directed to a fixed point and impression material was extracted from the lower palpebral region using a special tray and coordinated muscle trimming. Conformer fabrication: Clear acrylic conformers were fabricated using transparent heat-cure acrylic. The procedures followed conventional laboratory flasking methods and protocol for curing. Conformer modification using wax: clear conformer was inserted into the patients’ sockets and checked for fullness, retention, stability and aesthetic outcomes. When needed the conformer was modified with either addition using modelling wax or trimming the excess from acrylic. Conformer issue: conformer with modifications was re-processed in the laboratory and issued to the patient for a specific amount of time for habituation. Marking the iris and the center of the pupil: On subsequent follow-up, Pinpoint positioning of the iris was done using a transparent graph grid template and the contralateral eye’s iris. DSLR camera images were taken as a record for the color of the iris and coloring of the sclera. The final demarcated conformer and photograph were then processed in the laboratory. Definitive custom ocular prosthesis: The sclera was fabricated using white cold-cure acrylic and iris coloring was done according to the photograph of the healthy eye using poly-dimethylsiloxane silicone colors. This was later sealed by a thin layer of transparent acrylic. Issue and review: The patients were evaluated first on weekly basis for 4 weeks, followed by monthly intervals for 6 months and then asked to attend the clinic yearly for five years. The patient was educated on how to maintain prosthesis and soft tissue hygiene during that period.
The first case
A Malay male in his early twenties was referred to the clinic for rehabilitation of an ocular defect of the left eye. The patient had an evisceration surgery 2 months prior due to occupational trauma by rusted screw. On the day following successful evisceration surgery, a plastic prefabricated conformer was placed in the eye socket. On examination, the ophthalmic socket mucosa was healthy, socket volume was adequate, lacrimal secretions were normal but he had upper eyelid ptosis (Fig. 1A). The treatment plan involved fabrication of a custom-made ocular prosthesis with modifications to correct the upper eyelid ptosis. A conformer was made and modified until a satisfactory eye opening was achieved. (Fig. 1B). The conformer was issued and iris was marked after 2 weeks (Fig. 1C), the center of the pupil was demarcated. (Fig. 1D) The definitive custom ocular prosthesis was fabricated (Fig. 1E) and inserted into the patient to check for retention, stability and aesthetic outcome. (Fig. 1F). The patient was educated on proper usage and was placed under follow-up.

A) Left eye ocular defect of case 1, B) Conformer modification using wax (lateral view) C) Marking the iris using graph grid template D) The conformer after marking the iris using marker (Frontal view). E) The definitive custom ocular prosthesis for case 1 F) Issue of the ocular prosthesis for case 1. (frontal view).
A Malay male in his mid-forties was referred for ocular prosthesis fabrication in the same clinic with a right eye defect. The patient had undergone evisceration surgery 10 years previously due to an occupational accident with a rusted metal object. On examination, similar to case 1, the ophthalmic socket and mucosal tissues were healthy, albeit with a slight reduction in volume over the years. The patient had normal lacrimal secretions and upper eyelid ptosis (Fig. 2A) Impressions were taken and conformer was fabricated (Fig. 2B). The level of eye openings was marked, and necessary adjustments were made to compensate for inadequate sulcus fullness. This was followed by demarcating of the iris (Fig. 2C, D, E) and subsequent construction of the definitive ocular prosthesis. (Fig. 2F) The prosthesis was issued, and the patient was kept under follow-up.

A) right ocular defect in frontal view and lateral views of case 2 B) Conformer fabrication for case 2 (lateral view and tissue surface view) C) Conformer modification using wax (frontal view). D) The reshaped conformer according to the contracted socket E) the modified conformer in the eye socket. F) The definitive custom ocular prosthesis for case 2 G) issue of ocular prosthesis for case 2.
While both treatments were considered aesthetically successful, the early treatment allowed case 1’s socket bed to adjust with the prosthesis better and allowed for some amount of physiologic eye movement after the first month of use with similarly improved movement retained throughout the subsequent weekly and monthly follow-up visits. (Fig. 3) This movement was not, however, seen in case 2 who waited 10 years before seeking treatment. It is important to mention that long term (yearly) observation of case 2 was not possible as they stopped attending the clinic after a few months but demonstrated no satisfactory improvement in movement during the available period of monitoring.
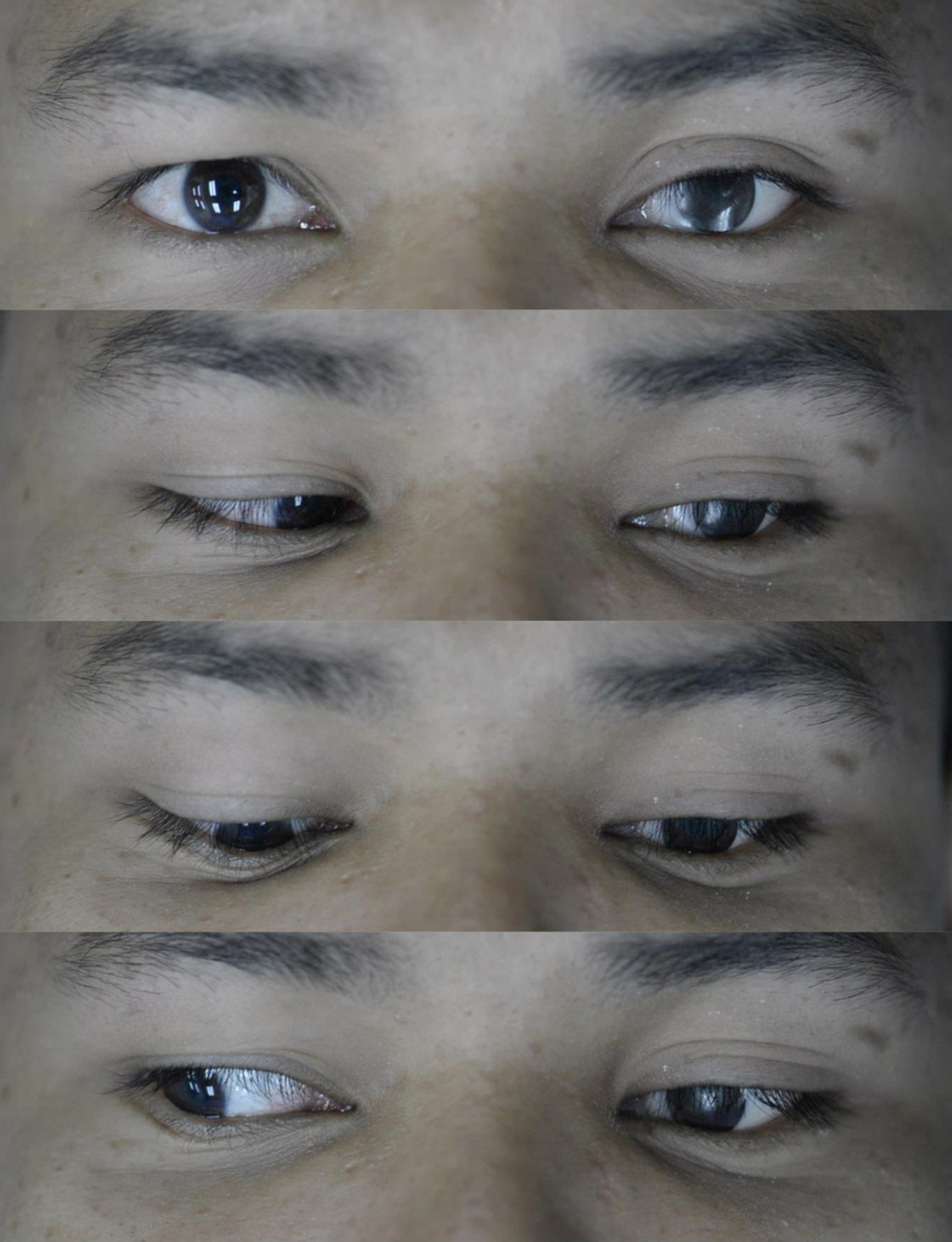
The result of prosthesis and mobility within the patient’s socket for case 1.
Early replacement of ocular globe by conformers have been shown to ease cosmetic rehabilitation and improve quality of life [9]. The concept of “glass eyes” has been replaced by acrylic conformers and prostheses due to its undistorted support, easy modification and biocompatibility amongst many other factors [10]. An acrylic ocular prosthesis can be stock or custom made (definitive). The use of stock ocular prosthesis is a cost-effective method of preserving socket size and depth immediately after surgery while custom oculars are tailored to individual patients. Custom ocular prostheses provide better aesthetic outcomes, allow for better socket adaptation and some degree of mobility [11].
Although both cases had identical workplace injuries from occupational hazard and had undergone identical surgical procedures, case 1 responded better and faster to the prosthetic treatment. Case 1 also acquired the skill to physiologically move the prosthetic eye in co-ordination. There are three possible explanations that could justify the prosthetic eye movement. The first is the waiting period; case 1 started treatment 2 months after surgery while case 2 came in for treatment after a decade. Another possible reason for acquired mobility and adaptation could be that the stock conformer was placed immediately following surgery. When there is no prosthesis within the socket, the soft tissues surrounding the eyes tend to shrink and collapse [6, 12]. Prolonged periods in that state tend to reduce aesthetic success in terms of eye opening and mobility.
Lastly, the age of the patient could be another factor that influences the adaptive nature of the soft tissue when trained. However, this is a topic of debate with multiple authors having different opinions and perspectives. Kahn and Shaw mentioned progressive aging as a process which results in bony structures undergoing a variety of morphological changes, and thereby agreed to aging as the cause of decreased adaptation [13]. The authors argued that with advancing age, they found an increase in bony orbital aperture with a subsequent soft tissue epidermal thinning and subsequent loss of collagen and elastin. This eventually lead to a loss in elasticity and eventually affected the amount to which the soft tissue can be trained [13]. On the contrary, Lowndes et al. found that the amount of muscle contracture (and subsequent adaptive nature) had no correlation with age, rather the site on the body where the muscles were in use [14]. Furthermore, Lowndes discussed how several other authors also agree with their perspective while also addressing that age dependent muscular atrophy and tissue degradation were eminent at the forth and fifth decade of life [14]. However, Sforza et al. noted that sex and race were equally important in affecting the overall aging process of the tissue. Furthermore, the age dependent degeneration was also found by multiple literatures to be largely co-dependent on the person’s existing craniofacial morphology [15].
Nevertheless, Juan et al. stressed that those patients with surgical loss of eyes undergo significantly progressive depression and anxiety and therefore prosthetic rehabilitation should be started alongside trauma counselling as early as possible to obtain overall satisfactory rehabilitative results [6, 16]. Successful rehabilitation can in turn improve the patient’s morale and add value to counselling and aid better outcomes [16].
Conclusion
Whether it concers the left or right eye, ocular prosthesis fabrication invariably follows the same procedural protocol. Good outcomes depend on immediate intervention, psychological counselling and early rehabilitation to avoid complications from late prosthetic intervention.
Footnotes
Acknowledgments
This study was funded by the Universiti Sains Malaysia Short term grant 304/PPSG/6315288.
Conflict of interest
The authors declare no conflict of interest.