
Abstract
BACKGROUND:
Distinctive features of low back pain-developers (LBPDs) as pre-clinical low back pain (LBP) population have been evidenced in three areas of alignment, muscle activation, and movement patterns. To clarify whether the reported altered functional movement patterns in chronic LBP patients result from or result in LBP disorders, LBPDs’ functional movement patterns should be investigated.
OBJECTIVES:
This study aimed to compare female LBPDs’ functional movement patterns with non-pain developers’ (NPDs).
METHODS:
Sixty female LBPDs and NPDs were recruited based on the research requirements. The Functional Movement Screen (FMS) was used to investigate movement quality. Data were compared between groups via Mann-Whitney U tests and correlation analyses examined association between pain intensity and onset during prolonged standing and the FMS score. Receiver Operating Characteristic Curves and Chi Squares were conducted to find the best cutoff points. An alpha level of p≤0.05 was used to establish statistical significance.
RESULTS:
LBPDs scored significantly lower, or rather worse than NPDs in the FMS composite score (12.06±1.33 vs. 16.43±1.59, U = 3, P < 0.001). Moreover, the optimal cutoff scores of≤14 on the FMS, 2 on the push-up, and 1 on the deep squat discriminated between female LBPDs and NPDs. The FMS composite score was correlated negatively with LBP intensity (r (60) = –0.724, p < 0.001) and positively with LBP onset (r (60) = 0.277, p = 0.032) during prolonged standing. Finally, the results indicated that female LBPDs presented with at least one bilateral asymmetry on the FMS had 10 times (95% CI, 2.941–34.008) and with at least two bilateral asymmetries on the FMS had 15.5 times (95% CI, 3.814–63.359) higher odds of developing LBP during prolonged standing than NPDs.
CONCLUSIONS:
Female LBPDs, who are at higher risk for developing LBP in the future, have significantly lower quality of functional movement patterns compared to NPDs. Moreover, the FMS appears to show promise for predicting individuals who are at risk for LBP development during prolonged standing.
Introduction
Low back pain (LBP) is a serious health problem with great social and economic costs [1]. The best approach to manage this problem is to prevent it from ever happening. The high prevalence of reported susceptibility to LBP development [2, 3], particularly in females [2, 5], further highlights the need for the comprehensive research into LBP prevention in this population.
In order to plan for LBP prevention, many studies have focused on low back pain developers (LBPDs) who are pre-clinical LBP population [6]. They are previously asymptomatic healthy people reporting pain during prolonged standing [7]. Nelson-Wong and Callaghan have reported that LBPDs had significantly higher rates of clinical LBP during the 3-year-follow-up period and a 3-fold increase in the likelihood of experiencing an episode of clinical LBP over the first 24 months compared to the non-pain developers (NPDs) [6].
The distinctive characteristics of LBPDs and the predictors of LBP development during prolonged standing can mainly be classified into 3 categories of alignment [8, 9], muscle activation [2, 11], and movement patterns [9, 12]. Changes in all three areas have been evidenced amongst these individuals compared to NPDs including early fatigue of hip abductors [7], gluteus medius co-activation during prolonged standing and even prior to pain development [5, 13–16], less range of motion in hip abduction [14], and altered muscle activation of gluteus maximus [10]. It is also necessary to investigate LBPDs’ quality of functional movement patterns as they are widely used in the activities of daily living and sports and can lead to pain and pathology if they are impaired.
On the other hand, Ko et al. [17] reported that patients with chronic LBP presented with impaired functional movement patterns and scored significantly lower on the Functional Movement Screen (FMS) composite score compared to their healthy counterparts. An important question is whether the reported altered functional movement patterns in the patients with chronic LBP result from or result in LBP disorders. If the presence of such altered functional movement patterns predisposes individuals to LBP disorders, LBPDs as pre-clinical LBP population [6] are expected to present with these alterations to their functional movement patterns.
Moreover, in a prospective study of 37 Division I female collegiate rowers, Clay et al. [18] reported that participants with a composite score of≤14 were significantly more liable to experience LBP during the season. The question still remains whether an optimal FMS cutoff score can be identified to predict LBP development during prolonged standing, thereby discriminate between insufficiently active female LBPDs and NPDs. Therefore, this study primarily aimed to compare functional movement patterns between female LBPDs and NPDs and, if possible, to identify an optimal FMS cutoff score to discriminate between the two. It was also hypothized that lower FMS scores would be associated with pain onset and intensity (maximum pain) during the PSP, in sense that LBPDs with worse functional movement patterns would experience an earlier pain onset with higher intensity during the PSP.
Secondarily, 5 out of 7 the FMS tests compare movement quality between sides, thereby providing an opportunity to identify movement asymmetry. In a number of prospective studies, researchers have reported that athletes with an asymmetry on any individual sub-test of the FMS were at greater risk of a musculoskeletal injury than others [OR range from 1.8 to 2.73] [19–21]. Therefore, we aimed to investigate whether an asymmetry on the FMS sub-tests could be associated with greater odds of developing LBP during prolonged standing. We also hypothized that more asymmetries on the FMS sub-tests would be associated with higher pain intensity during the PSP.
Methods
Ethics approval for research involving human subjects was obtained from the Institutional Research Ethics Committee at the University of Tehran (approval code IR.UT.SPORT.REC.1397.023). Sixty female volunteers were recruited from the university population. Inclusion criteria were: 1) no lifetime history of an episode of LBP leading to health intervention (e.g., medical, physical therapy) or three or more successive days of missed work or school [12, 22]; 2) no history of musculoskeletal disorders, dizziness, and balance disorders over the last 12 months prior to participation in the study [17]; and 3) no history of previous hip surgery [22]. Exclusion criteria included: 1) employment in a job involving prolonged (>1 hour) standing in the same place over the last 12 months [12, 22] and 2) a report of LBP symptoms at the very beginning of the PSP [12].
Informed consent was obtained and the rights of participants were protected throughout the study. Participants’ height and mass were measured. Then, in order to examine the homogeneity of the LBPD and NPD groups, each participant completed a questionnaire of Personal Information and Baecke questionnaire of habitual activity [23] evaluating habitual physical activity over the previous 12 months. It is scored from 5 to 15 with a cutoff point of 13 to distinguish between individuals who are physically active (scored over 13) and those who are not (scored below 13).
Following a 10-minute warm-up consisting of jogging at a self-selected pace on a treadmill [24], participants were divided into the LBPD and NPD groups based on their score on the Active Hip Abduction (AHAbd) test [22]. The AHAbd reliably [22] assesses an individual’s ability to maintain trunk and pelvis alignment while moving the lower extremity in an unstable position and can discriminate between those with and without LBP with high specificity [22]. The test was performed in side-lying position with lower limbs fully extended and aligned with the trunk and head throughout the movement. The pelvis was in perpendicular to the bed. The participants were specifically instructed not to let the pelvis tip backwards or forwards. The AHAbd is scored from 0 to 3 with higher scores reflecting a higher susceptibility to LBP development during prolonged standing. Both sides are tested and the score from the worse of the 2 sides is assumed as the final grade. The participants were assigned to the LBPD group if they were scored 2 or 3 in this test. They were blinded to group assignment.
Following group allocation, the FMS was performed to compare functional movement patterns between the two groups. It is reliable [25], valid [26], widely and conveniently applicable, and non-invasive. It consists of deep squat, hurdle step, in-line lunge, shoulder mobility, active straight-leg raise, trunk stability push-up, and rotatory stability. Each trial is scored from 0 to 3 with and the FMS composite score ranges from 0 to 21 with higher scores reflecting better functional movements [27]. Shoulder mobility, trunk stability push-up and rotary stability sub-tests include an accompanying test to evaluate the presence of pain (clearing test). Shoulder clearing test, spinal extension clearing test, and spinal flexion clearing test are performed at the end of shoulder mobility, trunk stability push-up, and rotatory stability, respectively. If pain was produced in a clearing test, the score would be zero for the related test. The FMS movements were videotaped in both sagittal and frontal planes. The videos were examined carefully by a single, certified FMS examiner using Kinovea video-analysis software version 0.8.15 for data analyses. The examiner’s intra-rater reliability was established by randomly selecting 20 participants’ videos. These videos were scored twice (spaced 2 weeks apart). Percent agreement between days was 100%.
After the FMS performance, participants reclined and rested for 20 minutes, then performed the PSP in accordance with the instructions presented by Nelson-Wong et al. [22]. The PSP is a valid [28] and reliable [15] test to functionally induce LBP and discriminate between LBPDs and NPDs. Thus, the initial assignment of participants to either group based on the AHAbd test was approved and the induced LBP onset, and intensity were quantified. To perform the PSP, participants stood for 2 hours while performing simulated, light work tasks. Participants reported their LBP every 15 minutes throughout the 2 hours of standing using a 100 mm visual analogue scale (VAS) with end point anchors of “no pain” and “worst pain imaginable”. Participants reporting LBP of 10 mm or more on VAS were categorized as LBPDs [22].
Data were analyzed with descriptive and inferential statistics using IBM SPSS 21.0 (p≤0.05). Independent samples t-tests were used to identify group differences in age, BMI, and activity level as documented by Baecke questionnaire of habitual activity. The FMS composite score was calculated, and the Mann–Whitney U test was used to determine differences in the FMS composite and sub-test scores between the LBPDs and NPDs. Since the FMS, trunk stability push-up, and deep squat had significantly high effect sizes to induce rank differences between the LBPDs and NPDs, a series of Receiver-Operator Characteristic (ROC) curves were used to determine their optimal cut-point scores which was realized when sensitivity (true positives) was maximized and 1-specificity (false positives) was minimized, identifying the score with the highest positive likelihood ratio for these screening tests. Data were also analyzed using Chi-square statistics in order to determine significant associations between LBPD group and the FMS composite cut-point score, FMS sub-test cut-point scores, and asymmetries on individual sub-tests. Further, a series of Spearman Coefficient Correlations were conducted between the FMS composite score and LBP intensity and onset during the PSP. Finally, the relation of LBP intensity with the rates of bilateral asymmetries on the FMS and with LBP onset were also examined using Spearman coefficient correlations. Statistical significance was set at p < 0.05 and 95% confidence intervals were calculated throughout the analyses.
Results
Baseline characteristics of the participants within each group (LBPD and NPD) were statistically similar (Table 1). However, both composite and individual component FMS scores were significantly lower, or rather worse in female LBPDs than NPDs (Table 2).
Participants’ demographic characteristics
Participants’ demographic characteristics
Abbreviations: BMI = body mass index; LBPD = low back pain developer; NPD = non-pain developer.
Descriptive data and results of Mann-Whitney U tests of the composite and individual FMS score between LBPDs and NPDs
Abbreviations: FMS = Functional Movement Screening; LBPD = low back pain developer; NPD = non-pain developer; *= Statistically significant.
Due to relatively high effectiveness of the FMS composite score to induce rank differences in the LBPDs and NPDs (Table 2), the ROC curves and subsequent Chi-square tests were used to determine the optimal cutoff scores for FMS composite score, trunk stability push-up, and deep squat in order to discriminate between the LBPDs and NPDs. The areas under the ROC were 0.977, 0.887, and 0.882, respectively (Fig. 1). Based on Youden’s Index [29], the most appropriate FMS composite score, push-up score, and deep squat score to use for this population as a predictor of susceptibility to LBP were≤14 (J = 0.933), ≤2 (J = 0.632), and≤1 (J = 0.573), respectively. Table 3 summarizes sensitivity, specificity, positive likelihood ratio (sensitivity/1-specificity) and negative likelihood ratio (1-sensitivity/specificity) of these cutoff scores.
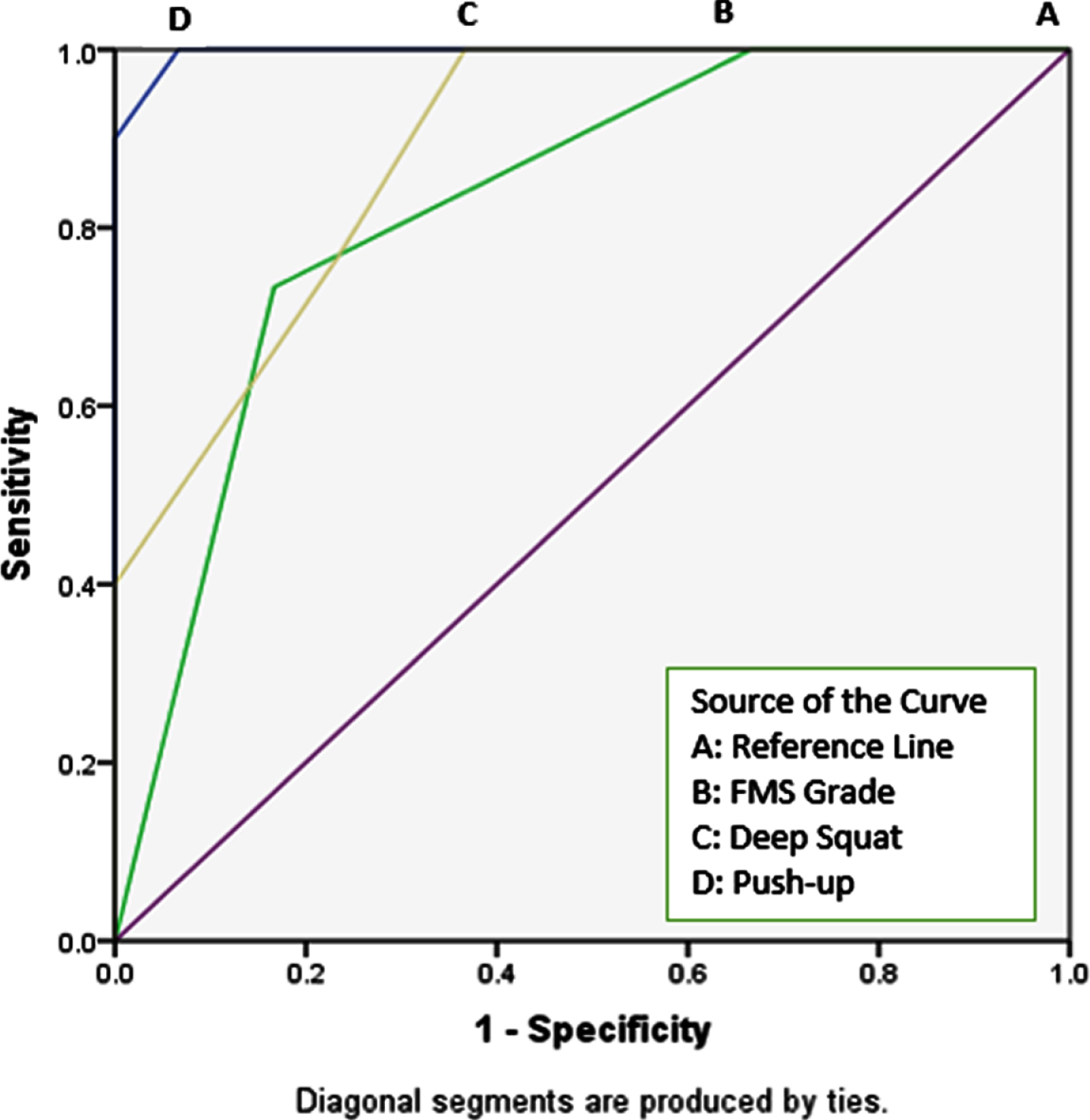
ROC plot for different cutoff thresholds of FMS total score, push-up and deep squat scores.
Diagnostic values (95% confidence intervals) for FMS composite, push-up, and deep squat scores for the susceptibility to LBP
Abbreviations: FMS = Functional Movement Screening; LBPD = low back pain developer; LR = likelihood ratio; NPD = non-pain developer.
A series of Chi-square tests of independence were calculated comparing the frequencies of at least 1 asymmetry on the FMS, at least 2 asymmetries on the FMS, the positive Trunk Extension Clearing Test, and positive AHAbd test in the LBPDs and NPDs. Compared to the NPDs, the LBPDs were more likely to have at least one asymmetry on the FMS (83.33% vs. 33.33%, X2 (1) = 15.429, p < 0.001), at least 2 asymmetries (63.33% vs. 10%, X2 (1) = 18.373, p < 0.001), positive Trunk Extension Clearing test (40% vs. 0%, X2 (1) = 15, p < 0.001), and positive AHAbd test (93% vs. 43.33%, X2 (1) = 17.33, p < 0.001). Finally, the results indicated that female LBPDs presented with at least one bilateral asymmetry on the FMS had 10 times (CI 95%, 2.941–34.008), with at least two bilateral asymmetries on the FMS had 15.545 times (CI 95%, 3.814–63.359), and with positive AHAbd test had 18.3 times (CI 95%, 3.674–91.22) higher odds of developing LBP during the PSP compared to NPDs.
A series of Spearman Rank-Order Correlations indicated that the composite FMS score was negatively correlated with LBP intensity (rs (60) = –0.724, p < 0.001) and positively correlated with LBP onset (rs (60) = 0.277, p = 0.032) during prolonged standing. In other words, lower FMS scores were associated with an earlier onset of pain with higher intensity. LBP intensity was correlated positively with the rates of bilateral asymmetries on the FMS (rs (60) = 0.513, p < 0.001) and negatively with LBP onset (rs (30) = –0.509, p = 0.004) during the PSP. Specifically, the participants presented with more bilateral asymmetries experienced an earlier LBP onset with higher intensity during the PSP.
This study indicated that LBPDs, who are at higher risk for developing LBP in the future, had significantly lower quality of functional movement patterns compared to NPDs. Therefore, altered functional movement patterns reported among chronic LBP patients [17] seem to occur prior to the onset of LBP. Importantly, our findings support the use of the FMS to discriminate between female LBPDs and NPDs.
One reason for the successful identification of the LBPDs using the FMS can be related to the characteristics of subtests. Considering the purpose for development of each FMS subtest and implications of low score in each [27], the common theme of stability keeps repeating; for example, one implication of low score in deep squat is “poor stabilization and control”, in hurdle step is “poor stability of stance leg”, in in-line lunge is inadequate “dynamic stability”, in active straight leg raise is insufficient “pelvic control”, in trunk stability push-up is “poor reflex stabilization of the core”, in rotary stabilization is “ poor reflex stabilization of the trunk and core”[27]. On the other hand, stability issues, or rather altered trunk and pelvis control have been reported in LBPDs [12, 22] and core stabilization exercises for trunk and hip control have been able to successfully change predisposing factors for inducing LBP which further verifies the existence of stability issues in LBPDs [11]. In other words, it implies that the FMS seem to have served its own purpose to identify poor stability within population whose impaired stability have already been reported [12, 22].
In order to further verify significant changes of functional movement patterns in female LBPDs, the relationships of composite FMS score with both the onset and the severity of LBP were also examined. The significant correlations of the onset and the intensity of pain with the FMS composite score (rs (60) = 0.277, p = 0.032; rs (60) = –0.724, p < 0.001, respectively) further confirmed the efficiency of the FMS to identify and characterize individuals prone to LBP development. As the FMS composite score reduced, pain emerged more intensely and within shorter amount of time.
Secondary findings of the research can help account for such significant correlations of the pain onset and the intensity with the FMS composite score. The significant relationship found between positive Trunk Extension Clearing test imposing a little more-than-normal load on lumbar area and susceptibility to LBP development (pain during the PSP) (X2 (1) = 15, p < 0.001) suggests there is pre-accumulated stress in the area. Further, the negative relationship between the onset and severity of LBP development during the PSP (rs (30) = –0.509, p < 0.001) further strengthens the notion. Stress accumulation in lumbar area can lead to tissue vulnerability in the sense that any kind of more-than-normal pressure and load such as prolonged standing [5, 30] can evidently cause pain and damage in the same way as Trunk Extension Clearing test can.
One factor for stress accumulation in this area may be due to the repetition of the reported asymmetric movement patterns in LBPDs’ lumbopelvic region which potentially results in accumulation of stress in one side of the spine [12]. In addition, LBPDs have shown higher levels of co-activation in their hip and trunk muscles at the beginning of the PSP [2, 12] which can impose higher load and force on the lumbar spine.
At present, there is still a doubt about the efficiency of the FMS composite score to predict injury [20, 21]. Accordingly, both the FMS composite and individual scores were examined in this study. The FMS composite score could efficiently identify female LBPDs (sensitivity of 100% and specificity of 93%). Indeed, the current study found composite FMS score of 14 to be an optimal cutoff point to identify females with a higher risk of developing LBP (a kind of injury) as many other prospective studies did to identify individuals with higher risk of injury [18, 32]. Furthermore, our data confirm previous reports that an FMS composite score of 14 could indicate a higher likelihood for subjective report of LBP [18]. This finding reinforces the utility of the FMS as a screening tool to identify LBPDs.
The current study also showed that female LBPDs with at least one bilateral asymmetry on the FMS had 10 times and with at least two bilateral asymmetries on the FMS had 15.545 times higher odds of developing significant LBP during prolonged standing. These results are consistent with the findings by Frost et al. [33] and Mokha et al. [20] indicating that the asymmetry in bilateral movements could well predict the occurrence of injury. Sorensen et al. [12] have also reported the existence of asymmetry in LBPDs’ movement patterns such as side-lying active hip abduction.
Asymmetric movement patterns have been reported to be associated with increased symptoms in LBP patients [34, 35]. Likewise, LBP intensity was significantly correlated with the rates of bilateral asymmetries on the FMS in LBPDs (rs (60) = 0.513, p < 0.001). This finding was consistent with the study conducted by Sorensen et al. [12] on 57 participants (28 females and 29 males) completing AHAbd test recorded with a motion capture system. The LBPDs’ lumbopelvic region significantly moved earlier during their left hip abduction and the amount of asymmetry was related to average symptom intensity induced during the PSP. Asymmetric movement of the lumbopelvic region which is repeated across activities can potentially lead to a greater accumulation of stress in the tissue on one side of the spine than the other [12] and thus to injury based on the Kinesiopathology Model [36].
Limitations
The present study may be open to criticism for not using high-tech 3D motion analysis, as the purpose of the study was to examine functional movement patterns using an accessible and inexpensive method available to all practitioners. Second, only females were included in the present study due to the higher rates of LBP and susceptibility to LBP development reported amongst females. Therefore, the results of our study may not be generalizable to males.
Future directions
Functional movement patterns differed significantly between Female LBPDs and NPDs and the FMS seemed to identify female LBPDs efficiently. Other researchers can investigate its replicability and the possibility of applying it to female and male LBPDs of different age ranges, sports, and levels of physical activities. Furthermore, the role of the FMS as a predictor of LBP incidence should be explored.
Conclusion
This study indicated that female LBPDs, who are at higher risk for developing LBP in the future, have significantly lower quality of functional movement patterns compared to NPDs. The FMS appears to show promise for predicting females who are at risk for LBP development during prolonged standing. In other words, practitioners can use the FMS as an efficient, non-invasive, and inexpensive tool for characterizing females prone to LBP development.
Footnotes
Acknowledgment
The authors would like to acknowledge their subjects for their contribution. This research project received no external financial assistance.
Author contributions
FK put forward the idea, carried out all tests, performed the statistical analyses, and drafted the manuscript; FS participated in the design of the study and statistical analyses, and helped to enhance the manuscript; RR conceived the study and participated in its coordination, and helped enhance the manuscript. AT critically revised and edited the paper.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding
The authors affirm that they have no financial affiliation [including research funding] or involvement with any commercial organization that has a direct financial interest in any matter included in this manuscript.