
Abstract
BACKGROUND:
Research has shown that the decrease in the inner diameter of vessels caused by hyperlipidemia lowers the capacity for blood oxygen delivery to the cochlea. This leads to impaired cochlear metabolism and causes hearing problems.
OBJECTIVE:
The effects of dyslipidemia on noise-induced hearing loss in workers were examined.
METHODS:
This descriptive cross-sectional study was performed on 692 male employees in a petrochemical industry in the southwest of Iran exposed to 85 dB noise. Clinical audiometry and blood sample tests were used to evaluate the hearing and prevalence indices of dyslipidemia (cholesterol, triglyceride, HDL and LDL). The data were analyzed using SPSS software version 25 (p = 0.05).
RESULTS:
The results showed that the prevalence of dyslipidemia was 24.5% with abnormal relative triglyceride frequency of 49.5%, HDL of 28%, LDL of 33%, and total blood cholesterol level of 37.8%. There was no significant relationship between NIHL and dyslipidemia (p > 0.09). However, the major NIHL drops at different frequencies were in the individuals with dyslipidemia. The parameters age and dyslipidemia increased NIHL odds ratio (95% C.I.) by 1.130 (1.160–1.100) and 1.618 (2.418–1.082) respectively.
CONCLUSION:
The rate of hearing loss in individuals with dyslipidemia increases at different frequencies and it leads to an increase of the OR of NIHL in individuals with dyslipidemia. We can control dyslipidemia and its effective factors. The NIHL is more common in people exposed to noise.
Introduction
Studies have shown that noise pollution in workplaces is one of the most important and hazardous factors affecting people’s hearing health [1–3]. According to the National Institute of Occupational Safety and Health (NIOSH), noise is a hazardous frequency for the hearing system [4]. Almost 5% of the world population suffers from noise-induced hearing loss (NIHL) in industrial, military, and recreational activities [5]. The NIHL is considered as the most common occupational disease in the United States and around the world [6]. A study in the United States showed that HL-induced hearing loss is a pervasive and costly condition, with significant economic and social impacts compared to common illnesses that affect workers’ health. In addition, it has received less attention compared to common cardiovascular disease [6–8]. The important impacts of the HL problem include a decrease in productivity, a decrease in the quality of life and hearing health, and an increase in stress [9–11]. Workers in noisy industries are at high risk of hearing loss (HL). Approximately, 30 million workers are exposed to the hazards of noise on daily basis [12]. Human ears are unable to withstand prolonged and repeated exposure to high levels of sound intensity. Thus, continuous exposure to noise that exceeds the permissible level cause damages to the inner ear and especially to the outer hair cells that are more sensitive [13, 14]. Research has shown that NIHL is one of the factors affecting hair cell damage [14–16]. Noises of 40–60 dB causes complete destruction of the outer hair cells and the inner hair cells, which leads to haring loss in the cochlea [14, 15]. The NIHL initially indicates damage to the cochlear sensory-nerve structures, affecting not only the sensory hair cells but also auditory nerve cells [14, 17]. In addition to noise, other factors such as age, gender, family history of ear diseases, race, and metabolic disorders such as hypertriglyceridemia and diabetes affect the development of hearing disorders [18, 19]. Examination of the constituent structures of cochlear tissue indicates that lipid composition, fluidity, and membrane stiffness of the outer hair cells are important for electromotive function and cochlear reinforcement. Thus, any dyslipidemia disorder may affect the function of the outer hair cells [20, 21]. Dyslipidemia involves a range of lipid and lipoprotein abnormalities, which include abnormal decreases and elevations in the level of the ear’s lipoproteins. Dyslipidemia lipid metabolism is a common problem [22]. It has been reported that high levels of the indices of dyslipidemia, including cholesterol and triglycerides, can be one of the major risk factors for the development of occupational hearing loss. A decrease in the inner diameter of the hyperlipidemic vascular bed reduces the supply of blood oxygen to the cochlea and causes chronic hypoxia due to decreased oxygen content in the inner ear. This leads to impaired cochlear metabolism and consequently impaired hearing in the cochlea. This is due to a decrease in oxygen supply to the inner ear [23]. Studies have shown that hyperlipidemic disorders such as dyslipidemia can cause hearing impairment mechanisms, which may be due to microcirculatory disorders in the inner ear [2, 25]. Dyslipidemia is a known cause of coronary artery disease and atherosclerosis, and it is the leading cause of myocardial infarction, stroke, and death in the United States. However, the role of dyslipidemia in hearing loss remains unclear [26–28]. Brownell et al. Showed that the outer hair follicles of guinea pig cochlea can absorb water-soluble cholesterol, which causes cell stiffness and thus interferes with inner ear function [29]. Given the financial and health costs caused by hearing loss that affect the economic and social status of individuals and paucity of studies on the effects of dyslipidemia on noise-induced hearing loss, this study is aimed at investigating the effects of dyslipidemia and noise-induced hearing loss.
Methods
This descriptive-analytical cross-sectional study was performed on 692 male workers of a petrochemical company in the southwest of Iran exposed to average sound pressure level above the recommended standard (85 dB) in 2019. Inclusion criteria were age younger than 55 years, no experience of illness or ear surgery, not taking autotoxic drugs, using of personal protective equipments (ear muff and earplug) and exposure to loud noise for at least one year. Information from a self-reported questionnaire was used to assess the inclusion criteria. Some of the questionnaires were randomly selected to verify the information of the participants in the study, and the inserted information was compared to the workers’ health records. Workplace sound pressure level was measured using a TES 1358 sound meter (made in Taiwan) based on ISO 9612 : 2009® guidelines [30]. After recording demographic data, the subjects received clinical examinations and hearing assessments using clinical audiometry. In order to determine the rate of hearing loss due to noise, it is necessary to first remove the effect of age. The age-related hearing loss [31] was obtained as follows:
Where N is the age of the individuals and K is obtained using the device tuning frequency from Table 1. Blood samples were taken after 12–14 hours fasting to measure the paraclinical variables. According to the definitions of dyslipidemia, the candidates who met the following criteria were considered as dyslipidemia cases. The criteria included elevated triglyceride levels > 150 mg /dl, high-density lipoprotein levels less than 40 mg /dl in men and less than 50 mg /dl in women, elevated low-density lipoprotein (LDL-C) levels greater than 100 mg /dl, and total cholesterol greater than 200 mg/dl [21, 22]. Enzymatic methods were used to measure the levels of cholesterol, triglyceride, and high-density lipoprotein (by Cho-GPO-PAP, PAP and phosphotungstate, respectively). In addition, low-density lipoprotein was determined using the Fridewld formula [32].
Demographic characteristics and biomarkers of the subjects
BMI=Body mass index; Total Chol = Total Cholesterol; LDL = low-density lipoprotein; HDL = high-density lipoprotein; TG = Triglyceride.
Statistical analysis was performed using SPSS version 25. Independent t-test and logistic regression were used to correlate some of the indices and Chi-square and Kramer tests were used to detect the correlation between the components. Kolmogorov-Smirnov test was used to check normal distribution of variables and Valid percentages were used for Miss cases. Data were analyzed at the significant level 0.05.
Results
The results showed that out of 692 petrochemical workers, 24.5% (n = 168) had dyslipidemia, 49.5% (n = 340) had relative abnormalities of triglycerides, 28% (n = 195) had high-density lipoprotein, 33% (n = 227) had low-density lipoprotein, and 37% (n = 260) had total cholesterol level. The study of noise-induced hearing loss in the subjects showed that 148 (21.7%) of them had hearing loss while 78.3% (n = 544) had no hearing loss. Moreover, 9.8% (n = 21) had noise-induced hearing loss in the both ears, 38.6% (n = 83) had noise-induced hearing loss in the right ear, and 51.6% (n = 111) had noise-induced hearing loss in the left ear. Diagrams 1 and 2 compare hearing loss in left and right ears and compares hearing thresholds in the two groups with and without dyslipidemia at different frequencies. The comparison of hearing loss at different frequencies between those with and without dyslipidemia showed that the severity of hearing loss in people with dyslipidemia was higher than those without dyslipidemia. The results of the analysis of noise induced hearing loss at different frequencies showed that the highest hearing loss in the subjects as well as those with and without dyslipidemia was related to the frequency of 4000 Hz in the left and right ears (Table 3). Hearing loss in the left ear is higher than that of the right ear; and the results also showed that the highest hearing loss occurs at 4000Hz. Table 1 lists the demographic characteristics and blood biomarkers of the study subjects, with the mean age and weight of the participants equal to 42.98±7 7.73 and 83.60±14.04 respectively. Moreover, BMI classification showed that 24.6% of the subjects had normal BMI and 47.8% and 27.6% were overweight and obese respectively. Table 2 lists the relationship between NIHL on blood biomarkers and demographic characteristics of the subjects. Statistical analysis showed that there was a significant difference between mean age and low-density lipoprotein in those with and without NIHL (p < 0.05). The NIHL odds ratio (OR) increases with age. The results of OR analysis (C.I. = 95%) of NIHL with regard to demographic and blood biomarkers are presented in Table 4. Each of the age and dyslipidemia parameters increased OR of NIHL by 1.618 (1.60–1.100) and by 1.618 (2.418–1.082) respectively.
The mean NIHL between the two groups with and without NIHL based on the frequencies under consideration
The mean NIHL between the two groups with and without NIHL based on the frequencies under consideration
*= p value for independent t-test.
Examination of the relationship of blood biomarkers and demographic characteristics with NIHL
*= p value for independent t-test; **= p value for chi-square test (χ2), BMI = Body mass index; Total Chol = Total Cholesterol; LDL = low-density lipoprotein; HDL = high-density lipoprotein; TG = Triglyceride.
Evaluation of the impact of demographic characteristics and indicators of dyslipidemia on NIHL OR
BMI = Body mass index; Total Chol = Total Cholesterol; LDL = low-density lipoprotein; HDL = high-density lipoprotein; TG = Triglyceride, a = Age > 29 considered as reference; the likelihood of dyslipidemia in other age ranges was compared with the reference age. This study was also conducted for BMI, considering obesity as a reference.
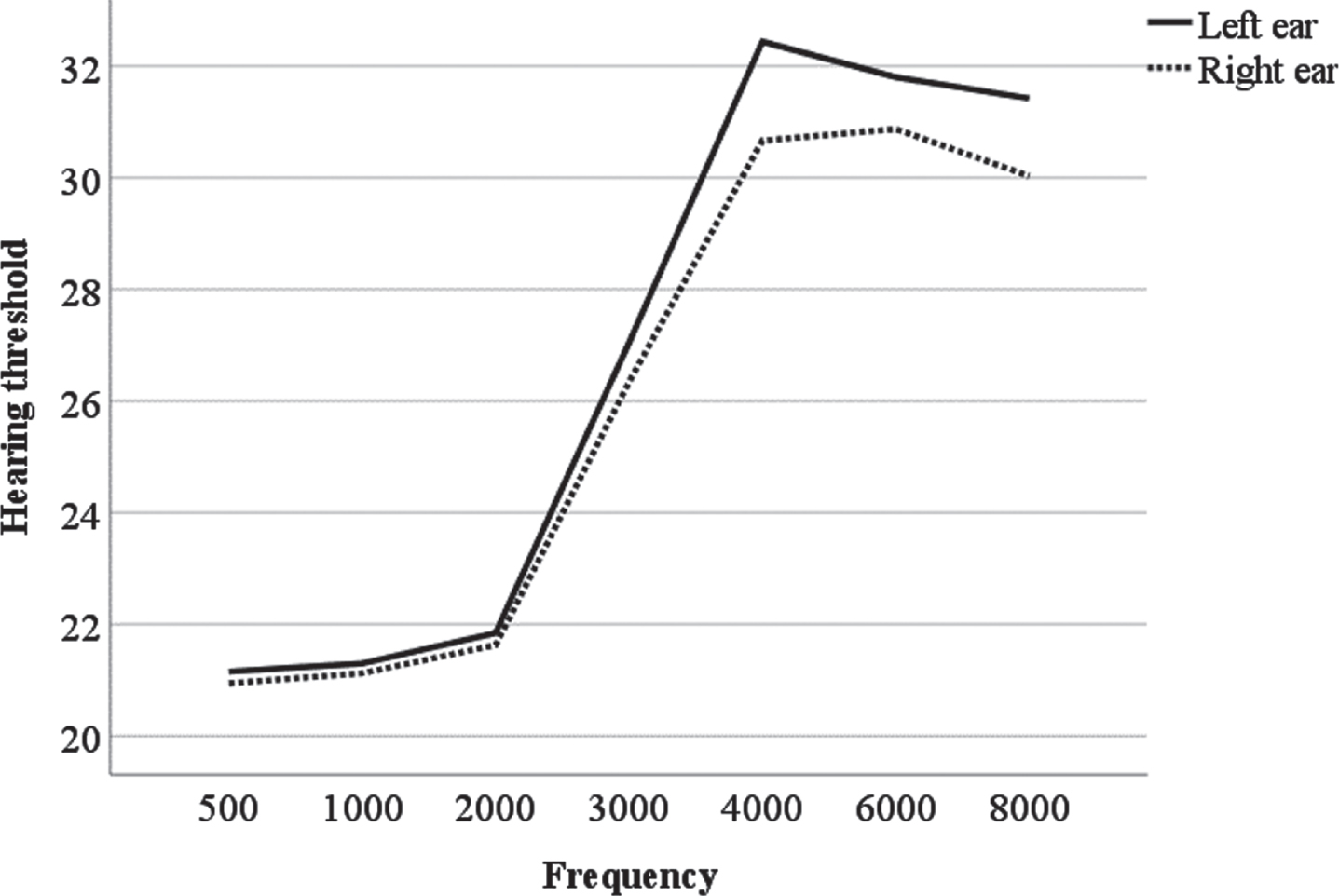
Average frequency of the left and right ears of the hearing threshold at different frequencies.
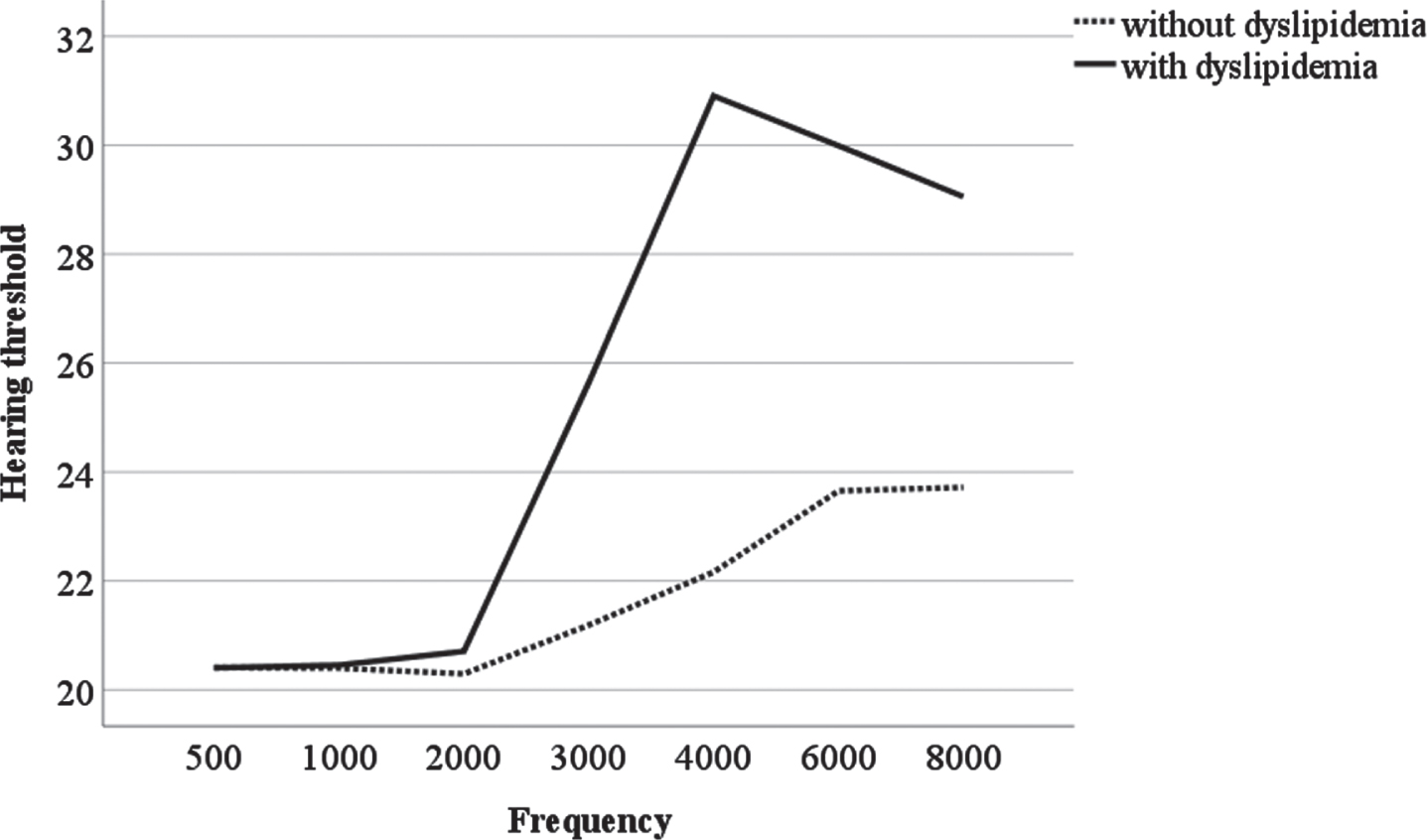
Hearing threshold diagrams in two groups of patients with and without dyslipidemia at different frequencies.
The results showed that the prevalence of dyslipidemia in the subjects was 24.5% (n = 168), which is lower than the results of studies in China (43.2% and 42.6%), Spain (31.3%), Thailand (88.9%) and Sri Lanka (77.4%) [29, 32–37]. The different results of studies are because of the fact that dyslipidemia phenotype is the result of several basic mechanisms and interaction between genetic, environmental, and behavioral factors. Measurement of dyslipidemia indices showed that TG was equal to 49.5%, Total Chol = 37%, HDL = 28.4%, and LDL = 33%. Of these indices, the lowest and highest percentage in individuals with abnormal condition are TG and HDL respectively. These results are consistent with the findings of the study by Abujbara et al. in Jordan and Bangladesh, while the results obtained for HDL are inconsistent. These studies showed that TG and LDL had the highest and lowest frequencies among the studied indices respectively [38, 39]. A study on noise-induced hearing loss in people exposed to noise above 85 dB showed that 21.7% of them had hearing loss; while 78.3% had no hearing loss. In addition, the mean severing of hearing loss in the right and left ears and in general were 23.56±6.65, 24.19±7.17, and 29.03±13.71 respectively. Clearly the highest loss happens in the left ear and the lowest loss happens in the right ear. These findings are consistent with other studies. The lowest and highest percentages were in the right and left ears respectively; indicating a greater sensitivity of the left ear compared to the right ear. This is consistent with results from previous studies [31, 40]. There was no significant difference between dyslipidemia and non-NIHL subjects (p > 0.05). However, a comparison of hearing loss at different frequencies between those with and without dyslipidemia shows that the severity of hearing loss in people with dyslipidemia was higher than those without dyslipidemia. Concerning the effects of blood lipids on hearing loss, the results of the studies are inconsistent with Rosen et al.. Our findings suggested that cardiovascular risk factors such as total cholesterol may accelerate development of NIHL [41]. With regard to the storage of cholesterol in the outer hair cell wall, Other researchers have proposed a theory that increasing total cholesterol levels reduces the stiffness of the outer hair cells and ultimately causes hearing loss [22, 42]. Moreover, Gratton and Wright used the chinchillas model and showed that by inducing hypercholesterolemia, lipid accumulation occurs in stria vascularis and outer hair cells, which exacerbates the adverse effects of noise [43]. Various studies have shown that the highest hearing loss in subjects with and without dyslipidemia happened at 4000 Hz in the left and right ears, and the hearing loss in the left ear is higher than in the right ear. In addition, the results showed that the highest hearing loss occurs at high frequencies such as at 4000, 6000, and 8000 Hz. These results are consistent with the findings of the study by Cunningham et al. We found that the highest impact of 4000 Hz hearing loss was in individuals with high blood lipids [44]. One of the reasons for the increase in NIHL at high frequencies may be the synergistic effect of noise and cholesterol regimens [45].
Moreover, Axelsson et al. provided epidemiological evidences indicating that the risk of high-frequency hearing loss for people exposed to noise increases with elevated serum cholesterol levels [46]. Experimental evidences suggest that vascular injury may increase sensitivity to noise-induced hearing loss [47]. In fact, vascular injury can decrease peripheral blood flow. In addition, increased blood viscosity due to lipemia can reduce peripheral blood circulation, thereby reducing nutrients and oxygen to the cochlea and exacerbating metabolic fatigue [48]. Statistical analysis for individuals with and without NIHL showed that age was the only significant variable in development of NIHL (p < 0.001). In addition, given the OR for NIHL, age increases the OR of NIHL. The measured parameters increased with age and consequently the chances of hearing loss at work increases. The reason may be a decrease in the ability of auditory cells, which is consistent with the findings of Leensen et al. [49, 50]. The results showed that there was a significant difference between those with and without NIHL in terms of the mean hearing threshold in general and the average threshold Hearing at 4000 Hz frequency (p < 0.001). This is consistent with the findings of previous studies [44]. Although, the results in Davis et al.’s study showed no significant difference between the parameters of dyslipidemia measurement and NIHL [51]. Still, the results of this study showed that among the indices of dyslipidemia, only LDL with NIHL were significantly different in the both groups (p < 0.05), while there was no significant difference among total cholesterol, HDL, TG, and NIHL (p < 0.05). These results are inconsistent with the findings of the study by Suzuki et al., who investigated the association between high-density lipoprotein and NIHL [52]. Some researchers followed a theory of using diet therapy and anti-lipid therapies to treat tinnitus and NIHL and reported high frequency aerial tinnitus improvement after a 24-month follow-up [23]. The effect of blood biomarkers on NIHL odds ratio (CI = 95%) indicated that age and dyslipidemia were effective in increasing the odds of developing NIHL (p < 0.05). Whereas Doost et al. concluded that cholesterol and triglycerides increased the OR of NIHL to 1.02 (CI = 1.05–0.99) and 1.07 (cl = 1.10–1.04) respectively [18]. A study in the United States by Chang et al. concluded that triglyceride caused an increase in OR of NIHL (OR = 1.281 with C.I.=1.507–1.88) [53]. Moreover, the results of statistical analysis of the effect of blood biochemical factors on NIHL showed that there was no significant relationship between the biochemical parameters studied in this study and NIHL (p < 0.05), which is consistent with the results of the study of Gold et al. The comparison of mean biochemical indices in subjects with NIHL and those with occupational noise but normal hearing showed that the mean values of biochemical indices in the both groups were in normal range and the difference between these two groups was not significant [53].
This study was not without limitations. All participants were men so the results may not be generalized to the whole population. In addition, there are a few neglected details of work schedule such as exposure term to damaging sound levels and long working hours. The reason for this was inaccessibility of information about these factors. Future studies can cover these factors as well.
Conclusion
Given the increased rate of hearing loss at different frequencies in individuals with dyslipidemia and increased OR of NIHL with an increase of dyslipidemia, controlling dyslipidemia and its effective factors is a strategy for prevention of noise-induced hearing loss in people exposed to excessive noise.
Footnotes
Acknowledgments
The researchers are grateful for the contributions of the occupational medicine specialists, the health personnel, and the hardworking staff of the petrochemical complex.
Conflict of interest
None of the authors have any conflicts of interest to declare.
Funding
This research was supported by the Student Research Committee of Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran under project registration number 98s68.