
Abstract
BACKGROUND:
Integrated approaches are valued in several occupational health strategic programmatic orientations. A better understanding of the use of integrative prevention in coordinating measures is needed to develop its use in workplaces.
OBJECTIVE:
Identify workplace integrative prevention approaches and definitions of prevention (primary, secondary and tertiary) in the literature.
METHODS:
A scoping review was conducted following Arksey and O’Malley (2005). The literature search was carried out in three databases without date restrictions. In order to be retained, the articles needed to address at least two levels of prevention using an integrative approach in a workplace setting. A qualitative analysis was conducted.
RESULTS:
The review yielded 16 published articles between 1995 and 2017. The articles addressed mental health, musculoskeletal disorder prevention and comprehensive approaches. Integrative prevention approaches are diverse and are not always named as such. Prevention definitions are not homogenous.
CONCLUSIONS:
This review identified some of the integrative prevention characteristics aimed at coordinated action for prevention in the workplace and to clarify measures taken at different levels of prevention. Further studies are needed to elaborate on the implementation of integrative prevention in the workplace.
Keywords
Introduction
Primary, secondary and tertiary prevention levels [1] are often compartmentalized in workplaces. However, several studies show that coordination between prevention levels could be a useful practice in workplaces [2–4]. Coordinated prevention activities would allow for the development of more efficient strategies to reduce the incidence and severity of workplace injuries and disability [2, 3].
Following a literature review of primary and secondary prevention of disability from occupational low back pain, [5, 6] a strategy that considers multidimensional aspects and encompasses several health determinants is necessary in order to understand the factors influencing disability. Interventions that combine several disciplines and take into consideration individual, organizational, and contextual factors should be developed to improve worker health [7], as [8, 9] have shown in the field of rehabilitation.
Concerns regarding the articulation of activities related to different prevention levels emerged during work activity analysis interventions in companies and were formalized by the ERIPRIT team 1 including clinical staff and ergonomists. As such, empirical studies carried out in workplaces where there is no coordination between the prevention levels demonstrate the inconsistencies that can occur between preventative measures and disability management practices. For example, the workstation rotation system put in place for prevention in companies is compromised by the temporary assigning practices used for workers returning to work. Temporary assignment is a practice by which workers with injuries are assigned tasks while waiting for them to be able to return to their original position in order to allow them to return to work earlier. Consigning “light” tasks to a temporary assignment occurs at the expense of workers who would ordinarily fulfill these tasks on a rotation with more difficult work [10]. In another study, returning workers were found to be assigned work that was detached from production and created especially for them during their temporary assignment period; these positions were undervalued and not suitable for their re-training [11]. In addition, disability management may be hampered by claims discrediting the link between work and injury. The roles and mandates of these departments can reinforce the separation between the human resources department and the occupational health and safety department [12]. Occasionally, these two departments even develop job analysis frameworks independently, without coordination. In clinics, occupational therapists are confronted with people who have been re-injured since their return to work because the working conditions have not changed [13]. Further, laws governing prevention and compensation are often separated.
It is important to remember that workplaces are heterogeneous, complex and dynamic. Prevention practices and occupational injury management are anchored in the organizational context of the workplace, which is itself influenced by economic, political and social contexts [14]. Coordinated action between prevention levels in workplaces is a challenge, and no consensus exists surrounding the concept of integrative prevention, prevention level definitions or the activities related to each level.
No exhaustive review has shone light on different understandings of integrative prevention or even on the different levels of prevention. The objective of this literature review is to identify different integrative prevention approaches, which implies also identifying the prevention level (primary, secondary and tertiary) definitions in use and measures taken. The results of this review should help us clarify the concept of integrative prevention and improve coordination of prevention activities in workplaces.
Methods
Given the interdisciplinary nature of integrative prevention, a scoping review methodology was used [15, 16]. This method allows for the clarification of definitions and the drawing of boundaries around a research field that is composed of heterogenous and complex studies [16]. Scoping reviews are also suitable for evaluating the contribution of the literature to the field of study [17].
Step 1: Identifying the research question
Interdisciplinary exchanges between ÉRIPRIT researchers uncovered several research questions, of which two were retained for the present study: What integrative approaches are addressing the coordination of several prevention levels for mental and physical illnesses in the workplace? What definitions and measures are associated with the different prevention levels (primary, secondary and tertiary)?
Step 2: Identifying relevant studies
The research was carried out in three databases, Scopus/Medline, PubMed and Google Scholar, without date restrictions but until 2017, in French and English (Fig. 1). These databases were chosen in accordance with the desired disciplines and Google Scholar’s ability to redirect to articles that were cited in a specified article. Five word-groupings were used: workplace (e.g. occupational, job), primary prevention (e.g. incidence, protective), secondary prevention (e.g. absenteeism, prevalence, remain at work), tertiary prevention (e.g. disability prevention, sickness absence, rehabilitation) and integrative intervention (e.g. participatory approach, coordination). The snowball technique was employed using the bibliography generated by the search and the options “cited by” and “search similar citations” in Google Scholar in order to identify further articles.
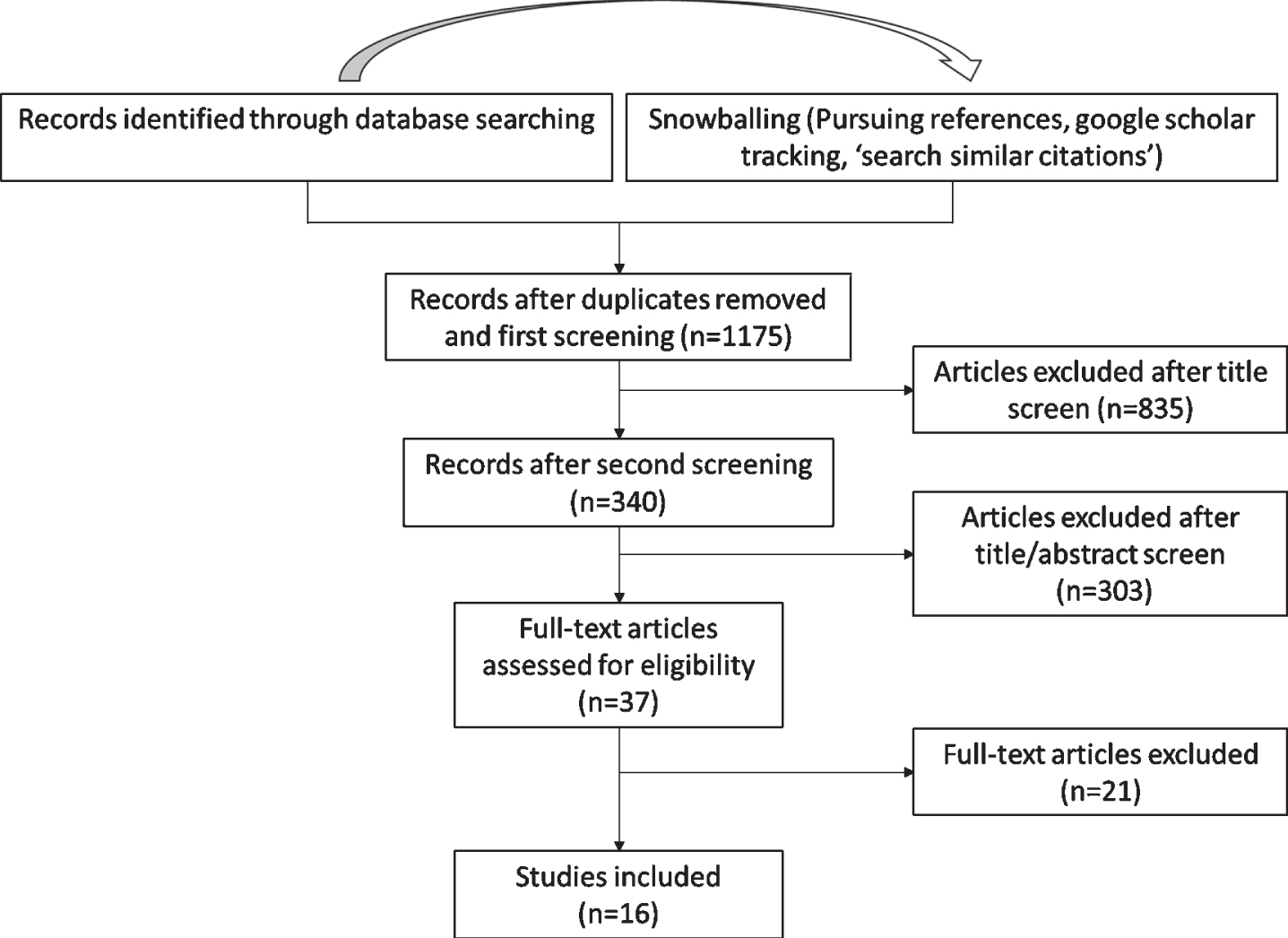
Study flowchart for the scoping review process.
Four inclusion criteria used were: 1) the article describes, carries out, evaluates or discusses an integrative approach that implies the coordination of at least two prevention levels for physical or mental illnesses related to work (e.g. a return-to-work program and prevention activities in a company to prevent stress or musculoskeletal disorders (MSDs)); 2) the strategy described in the article is aimed at a workplace and its organizational structure; 3) the article is in French or English; and 4) full texts were available. Exclusion criteria: Articles presenting a health promotion approach (e.g. healthy lifestyles) aimed only at individuals were excluded in the first screening because, while worthwhile, these approaches do not target the workplace. Articles which addressed several levels of prevention but without discussing the coordination between them were also excluded since coordination of activities was the focus of the present research.
The article selection process unfolded over several steps (Fig. 1). First, through reading the title only. Second through reading the title and the abstract. Finally, by reading the entire article. At each step, at least two reviewers were responsible for excluding articles not responding to the inclusion criteria. All disagreements were resolved through consensus.
Step 4: Charting the data
While reading the articles, passages that addressed an integrative prevention approach and prevention levels were highlighted. The following variables were recorded: article details (authors, year of publication and study location), description of the article (aim of the study, overview of methods, problems addressed) and elements that would allow for the analysis of the integrative prevention approach presented, as well as its components. The primary, secondary, and tertiary prevention levels were extracted and analyzed according to several criteria: characteristics, targeted objective, and measures proposed by the author. The objectives and measures were also categorized according to their orientation (based on the type of workplace intervention or on the health status of individuals).
Step 5: Collating, summarizing and reporting the results
The qualitative analysis was conducted iteratively. Articles were categorized into three groups according to their target: MSD prevention, mental health prevention and comprehensive approaches to prevention. The integrative prevention approaches targeting coordinated prevention activities described in the articles are summarized in (Table 1). Several elements were documented: the integrative prevention approach, the elements subject to integration, and the primary, secondary and tertiary prevention definitions used. The analysis was carried out on excerpts of the texts: words (e.g. expressions used for ‘integrative prevention approach’), phrases (e.g. prevention level definition) or paragraphs (e.g. description of elements subject to integration). The data were categorized in tables to compare and elicit integrative prevention properties (Table 2) and primary, secondary and tertiary prevention definitions (Table 3). Repeated reading and detailed analysis by two authors clarified the integrative prevention and primary, secondary and tertiary prevention definition categorization.
Study details
Study details
*Articles addressing the same program, Prevention and Early Active Return to work Safely (PEARS). **: Articles addressing the same integrative prevention approach.
Description of approaches that coordinate at least two prevention levels
Classification of the primary, secondary and tertiary definitions proposed in nine articles
The scoping review yielded 1175 articles. 16 articles published between 1995 and 2017 were selected according to the established criteria (Fig. 1). Table 1 presents a description of each of these 16 articles addressing the coordination of at least two levels of prevention, whether it be primary, secondary or tertiary, using an integrative approach. The principal authors are from different countries: four from the United States [18–21], seven from Canada [22–28], four articles from Australia [29–32], and one article from France [33]. All articles are in English, except one which is in French [28]. The physical and/or mental health problems addressed in these articles are the following: musculoskeletal disorders [22–28, 33], mental health and occupational stress [19, 29–32], and occupational health more generally [18, 21]. Only five articles present an integrative prevention approach implemented in a workplace [22, 25–28], of which four address the same program. The 16 articles describe different integrative prevention approaches, as well as distinct elements being integrated.
Integrative prevention approaches
Different approaches aiming at integration and traversing several prevention levels are presented in the articles using different terminology. Occasionally, the approach is not explicitly referred to as an integrative prevention approach. The following terms are used: “systems approaches,” “integrated intervention approach,” and “integrated approach” [30–32]. Other ways of describing integrative prevention approaches are used in some studies, whether it be “integrated framework of work disability” [18], “integrative workplace health management” [29], “integrated disability management” [20], “holistic management of MSD” [28] or “integration of clinical and preventive occupational health services” [21]. Only Roquelaure [33] refers to “integrated prevention” while putting emphasis on the coordination of stakeholders involved in prevention. Cole et al.’s [23] synthesis article, which is an in-depth conceptual reflection of workplace MSDs in the field of prevention, covers the concept of integrative prevention. According to the authors, different elements of prevention can be integrated: “biomechanical & psychosocial, multi component (engineering controls, administrative/production, employee involvement, management support, training, medical management), occupational health & safety systems; and of course, primary, secondary +/- tertiary prevention”.
The articles reviewed here put forward holistic workplace interventions and propose ways of implementing them.
Musculoskeletal disorder (MSD) prevention
Integrative prevention approaches targeting MSDs comprise several elements described in Table 2. Of the eight articles concerning MSDs [22–28, 33], four discuss the Prevention and early active return to work safely (PEARS) program implemented in hospitals [22, 25–27]. The evaluation of this program demonstrated benefits related to reduced costs associated with workplace disability [22, 25]. In this program, the team’s prevention activities are communicated to a program leader and used to guide rehabilitation and return-to-work activities [27]. A bipartite steering committee oversees the program. A physiotherapist is on site to help employees stay at work and improvements to workstations can be made. Ouellette et al. [27] have shown that workplace assessment is an important element of the program to decrease work disability. This program emphasizes the organizational culture of safety involving the cooperative participation of stakeholders including a supportive work climate and cooperation and trust between management and labor (unions) [22, 26].
According to Roquelaure [33], one of the difficulties in preventing MSDs resides in the fact that stakeholders (e.g., managers, trades unions, workers, prevention practitioners, physicians, insurers) who need to collaborate to carry out primary, secondary or tertiary prevention have different understandings of MSD etiology and different prevention intervention models. Sharing common knowledge and understanding of workers’ activities among stakeholders would improve intervention outcomes. Thus, Roquelaure [33] puts forward a systemic approach that accounts for the fact that stressors experienced by people during their work activity can have causes or determinants derived from different sources, whether they are the work tools used, work organization or company culture. Roquelaure [33] emphasizes the need to describe the work activity and its stressors and to seek out the experience of one or more worker in order to carry out effective prevention measures, whether they be at the primary, secondary or tertiary level. This is an approach developed primarily by French-speaking researchers focused on the analysis of work activity and the improvement of working conditions [34]. Tremblay-Boudreault et al. [28] implemented this approach combining a systemic vision of work situations with a detailed work activity analysis. In this example, workplace training was used as a means to share responsibility for MSDs by different company stakeholders, both in terms of prevention and return-to-work. Tremblay-Boudreault et al. [28] showed that training led to changes in company stakeholders’ perceptions of MSDs. For example, whereas risk analysis targeted work habits of the injured worker following an accident or an MSD, an improved understanding of working conditions among company stakeholders led to the implementation of solutions to factors related to the working environment more generally.
Mental health prevention
Of the 16 articles, five deal with mental health [19, 29–32]. The main characteristics of these articles are presented in Table 2. All of the authors promote a holistic approach in workplaces and prioritize the participation of all stakeholders. For example, Chu and Dwyer [29] propose a process that requires management support, evaluation, needs assessment and the development and implementation of an action plan, all while ensuring active participation of workers and other stakeholders. For their part, the approach used by LaMontagne et al. [30, 31] is inspired by the University of Michigan job stress model developed by Israël et al. [19]. This model suggests putting in place nine principles during mental health prevention interventions. Among the principles are: “a context specific intervention, a comprehensive approach to prevention intervention to address the complex set of factors in the stress model, collective action and broad-scale change, participants’ involvement and control, multidisciplinary teams, and others”. One of the nine principles concerns integrating the three prevention levels (primary, secondary and tertiary). In the University of Michigan job stress model developed by Israël et al. [19], Quick et al.’s [35] definitions are used to delineate the prevention levels. According to the authors, the three prevention levels are needed for a comprehensive mental health approach. In 2014, LaMontagne et al. [30] expand on the approach presented in their 2007 [31] article with three threads for intervention: reduce work related risk factors, develop positive aspects of work and worker capacities, and address mental health problems regardless of cause. Finally, Memish et al. [32] evaluate around 20 guides from different countries that give recommendations from an authoritative source for prevention and/or management of mental health problems in the workplace and specifically developed for use by employers. This study evaluates both the quality of the proposed mental health workplace guides as well as whether LaMontagne et al.’s [30] criteria are taken into account in the guides targeting employers. The following integrative prevention elements were established to evaluate the guides: recommendations for the individual, recommendations for the organization, minimize risk factors, promote positive factors, primary prevention, secondary intervention and tertiary intervention [32].
General health prevention in the workplace
Many characteristics emerge from integrative prevention approaches that do not target a particular health problem (Table 2). Rieth et al.’s [20] early article describes “workplace integrated disability management” inspired by the concept of “Total health management developed by the Ohio based Fortune 500 company.” The objective of this article was to support occupational health nursing practices. The authors emphasized the importance of coordinated actions and gave the example of companies implementing a program that incorporated several elements of a process aiming to manage employee disabilities. The authors classified the actions needing to be coordinated according to primary, secondary and tertiary prevention levels, but the program aimed mostly “to coordinate a team effort to holistically manage employees.” The following activities are explained in detail: case management, disability resolution process, rehabilitation plan development and return to work programs/accommodations. On the other hand, few measures pertaining to the environment or work organization are given.
Amick et al. [18] measure the impact of organizational behaviors on work disability prevention and management. The authors use the American Counseling Association (1998)’s conceptual model, “Organizational influences on work disability” in which organizational policies and practices correlate with workplace disability incidence. There are two prevention levels in this model, which are not named explicitly as primary, secondary or tertiary, but which correspond to before injury behaviors and after injury responses. The articulation between disability prevention and management of interventions in this model exemplifies strategies to minimize the incidence and disability consequences of injuries and diseases arising in the workplace. However, this model is used to develop questionnaires based on indicators that measure organizational behavior as evaluated by employers and employees and is not focused on workplace interventions. Further, the dimensions are measured independently even though they coexist in the workplace, as the authors point out in their own discussion.
Rudolph et al. [21] target occupational physicians and appeal to the responsibility that they have to patients who are suffering from workplace related health problems. Their focus is to promote the linkage between prevention and treatment. They demonstrate the need to improve clinical occupational health preventive services. They describe several instances in which this linkage was beneficial, but they also identify numerous challenges and barriers to such integration. According to the authors, prevention in occupational health can be characterized as primary, secondary, or tertiary. Weeks et al.’s [36] definitions are used to differentiate the levels of prevention. According to Rudolph et al. [21], if primary prevention is not effective, secondary and tertiary prevention will be required. The authors highlight that cases of occupational illness or injury should serve as indicators for targeted primary prevention measures to be taken in the workplace. For this reason, the authors believe that prevention measures across different levels should be coordinated and that close working relationships between occupational health service providers and the workplace should exist.
The terms primary, secondary and tertiary prevention are used differently in the varied integrative prevention approaches presented here, whether they be in MSD prevention, for mental health prevention or in the case of occupational health more generally. It is worthwhile to examine authors’ definitions as well as the measures associated with the three prevention levels in these integrative prevention approaches.
Prevention level definitions in integrative prevention approaches
It is important to clarify the definition of each prevention level in order to identify which elements need to be coordinated in integrative prevention. Articles fall into two groups. We will first examine, in detail, the nine articles in which definitions are explicitly articulated. Then we will analyze the seven articles in which the prevention levels are not explicitly developed or in which the prevention levels are classed into only two categories.
Articles that explicitly define prevention levels
Of the 16 articles analyzed, nine give explicit definitions of prevention levels (Table 3). For each level, the approach’s characteristics, the objectives, as well as the suggested prevention measures were extracted from the article. The objectives and the prevention measures were defined according the whether they oriented around improved workplace conditions or individual health.
3.2.1.1.Primary prevention: Primary prevention is more developed in articles dealing with mental health [19, 30–32]. For these authors, primary prevention is proactive, work-oriented and focused on the workers before they feel symptoms. Objectives are principally oriented to the workplace. They aim to eliminate or reduce risk factors or job stressors [19, 33]. Articles concerned with mental health offer precise measures to implement in the workplace. For example, activities to reduce job demands are: increase time or other resource allocations to complete specific tasks, redesign the physical work environment to reduce musculoskeletal load and noise, and provide breaks from client-based work [31]. Some of the measures are less proactive, for example those that propose to modify the work environment [30] or to reduce job demands [19], both of which imply that exposure to certain risks is already present and that the prevention measures are a reaction to a problem.
Articles on MSD prevention identify the same primary prevention characteristics and objectives as the articles on mental health, but go into less detail on the workplace measures to implement [23, 33].
Health-focused goals are covered as much in mental health prevention articles as in MSD prevention or general occupational health articles [20, 30–33]. Using a more general workplace health prevention perspective, Rieth et al. [20] propose prevention programs for injuries whether they are related to work or not. Rudoph et al. [21] suggest identifying workers with health conditions which place the worker or co-workers at substantial risk in a particular work environment.
3.2.1.2.Secondary prevention: Compared to primary prevention, secondary prevention is more oriented to the worker than the workplace [30, 32]. This is a phase in which people begin to have health impacts [19, 32]. In several of the articles, spanning all three categories of health impact, intervening in injury progression is given as a goal, e.g. to stop or slow progression of disease or to reduce the risk of work disability [21, 33].
Several workplace measures are evoked specifically for MSD prevention, such as, stay at work programs, active surveillance for early detection or enhanced reporting systems for those with early symptoms [23]. Mental health articles [19, 32] place more emphasis on measures targeting modification to the workplace or workers’ ability to deal with stressors, whereas MSD prevention articles more often discuss symptom surveillance programs [23].
3.2.1.3.Tertiary prevention: Tertiary prevention is the prevention level that is defined most similarly across articles. Cole et al. [23] contend that tertiary prevention is a misnomer because it is in fact a treatment phase. It is reactionary and concerns affected workers who are returning to work [19, 30–33]. MSDs and more general approaches to workplace health prevention emphasize measures supporting return and stay at work, and rehabilitation programs [20, 33]. While citing the above-mentioned elements in the definitions given, mental health prevention articles also put forward examples of actions to take to safeguard affected worker’s health [19, 30–32].
Articles that depart from the three prevention levels
Seven studies depart from the three-tiered prevention level schema used by other articles. Of these seven articles, five only use two levels, explicitly or not. Two do not use the nomenclature of primary, secondary and tertiary prevention or depart from it to prioritize a more holistic approach.
Five studies only refer to two prevention levels [18, 25–27]. Four of these articles are related to the PEARS program, which is an integrated workplace-based program in disability prevention that coordinates primary prevention activities with onsite early intervention activities (prompt follow-up of injured workers) [25]. Maiwald et al.’s [26] article evaluating one aspect of the PEARS program presents primary prevention as having the following goal: to prevent work disability from occurring prior to reporting sick (including a work assessment). Secondary and tertiary prevention are combined into one level with the goal of reducing time-loss and supporting return-to-work after a sickness absence [26]. Moreover, Cole et al. [23] give definitions for three prevention levels but use the nomenclature ‘secondary +/- tertiary’ when discussing authors who use only two levels. Amick et al.’s [18] article uses a conceptual model that only provides two prevention levels “before injury behavior” and “after injury responses,” and they do not make use of the terms primary, secondary or tertiary prevention. Reference to disability management indicates that the terminology “after injury” refers to tertiary prevention rather than secondary.
Tremblay-Boudreault et al. [28] give definitions of the three prevention levels in the introduction but prefer to group all measures under the term “MSD prevention”, whether they are targeting preventing the manifestation of MSDs (primary prevention), maintaining workers who present with symptoms in their jobs (secondary prevention) or encouraging return-to-work by injured workers (tertiary prevention). The authors employ the term “return-to-work process” to designate the actions taken by the company to accommodate a worker who suffered an injury (tertiary prevention) [28]. Chu et Dwyer [29] also have a more general vision of prevention. The three levels are not explicitly named in the article; rather, concepts affiliated with the different prevention levels are presented, such as: prevent and manage physical and mental health problems, reduce risk factors and health and safety hazards, and improve health and rehabilitation [29].
For each of the prevention levels presented in the articles, associated measures can be directed at the source (eliminate the problem), between the source and the exposed person (adding a protection layer between the worker and the hazard source) or toward the exposed person (awareness raising or training on the hazards to which they are exposed). However, only measures taken at the source are explicitly addressed in primary prevention definitions, and these are comprised of eliminating or reducing the risk factors at the source for those authors who refer to them [28, 33]. Measures aimed at modifying the work environment, irrespective of prevention level, do not indicate whether this action is really located at the source (replacement of equipment or modification of a process) or between the source and the exposed person (addition of individual protection such as protective clothing or collective protection such as security guards).
Finally, the definitions offer as many measures targeting the workplace, whether they be at the source or between the person and the hazard, as they do measures aimed at individuals (exposed persons).
Discussion
The scoping review results identified different integrative prevention approaches aiming at the coordination of measures in primary, secondary and tertiary workplace prevention. These approaches targeted either MSDs, mental health or occupational health more generally. The mental health integrative prevention approaches presented in these articles are comprehensive, proactive and cover several components that capture the complexity of stress models. Articles addressing MSDs suggest integrative prevention approaches that are more anchored in tertiary prevention, assisting particularly in return-to-work.
Integrative prevention models coordinating workplace prevention measures are emergent. Concepts are often addressed implicitly in the articles, with varying definitions used by authors. Only two of the integrative prevention approaches were actually applied in a work environment and in both cases, it was in the context of MSD prevention.
Key elements of workplace integrative prevention
The approaches analyzed in this study demonstrate that there are a variety of ways of conceptualizing integrative prevention aimed at coordinating workplace measures. However, several common elements emerge and lead us to define integrative prevention as an approach that coordinates several workplace prevention levels (primary, secondary or tertiary) aimed at reducing or preventing MSDs, mental health issues or other injuries and disabilities, and that encourages a culture of health and wellbeing in all spheres of the company through involving each organizational level and different internal and external stakeholders in a participatory process.
All of the characteristics identified are described in Table 4. Using the above definition as a starting point, integrative prevention emerges as a relevant avenue that could respond to concerns raised by some empirical studies that inconsistencies between measures deployed at different prevention levels exist [10, 11]. However, a lack of information on how to coordinate measures at different prevention levels in workplaces remains. Nonetheless, several conditions can be fostered at workplaces to facilitate integrative prevention: adaptation to the particular context and using a participatory approach.
Characteristics of integrative prevention approaches that coordinate workplace prevention measures
Characteristics of integrative prevention approaches that coordinate workplace prevention measures
Implementation should be adapted to the particular context of the workplace rather than independent of it [19, 33]. This is consistent with what we know of workplaces: that they are heterogeneous, complex and dynamic environments influenced by the economic, political and social context in which prevention takes place [14]. Integrative prevention invites consideration of a company’s different structural strata using a systemic approach [33].
Using a participatory approach could be another method for successful implementation of integrative prevention [19, 33]. Developing the intervention with internal and external company stakeholders adapts it to the context. A work environment and prevention culture that encourages cooperation and trust between employer representatives (or managers) and workers (or their trade unions) is indispensable for coordinated prevention [22, 26]. Stakeholders need to share a common understanding of the working conditions in order to mobilize the necessary knowledge from each prevention level, particularly for the prevention of MSDs since their causes are multifactorial [33].
The results from this scoping review encourage the implementation of integrative prevention, but little in the way of concrete steps to take in the workplace are given. Work activity analysis, which is participatory and targets the organization, is recognized as an integrative prevention component [20, 29]. Work activity analysis can be used as a lever, beyond workstation adaptation and stakeholder participation, in the implementation of integrative prevention. Work activity analysis emerges as a promising method because it makes coordination between the primary, secondary and tertiary prevention measures carried out by the health and safety and human resource departments possible, as Tremblay-Boudreault et al. [28] showed in the case of a factory. Analysis of workers’ activity promotes the sharing of a common vision of actual working conditions (the impacts of the work environment on the activity, work activity stressors and the consequences on health and production), which facilitates stakeholder coordination [33].
Definitions for primary, secondary and tertiary prevention presented in the integrative prevention approaches varied, with those pertaining to tertiary prevention being the most homogeneous. Some authors propose only two prevention levels: before and after injury [18, 25–27]. We suggest retaining three levels of prevention. First, using three prevention levels better differentiates prevention measures at each step of the health continuum, notably in the case of MSDs (healthy worker, worker with discomfort/symptoms and incapacitated worker) [4]. Further, conserving the three levels is a way to ensure that primary prevention measures (proactive) are not sidelined and to properly distinguish them from secondary prevention measures.
Mental health prevention articles place more emphasis on the development of primary prevention measures than the other categories of articles. Primary prevention is promoted in the proactive models that integrate mental health prevention and promotion [19, 29–31]. The Model for occupational well-being, mental health promotion, and distress prevention [35] defines prevention as an integrated ensemble of measures taken at three levels of action. Quick et al. [35] criticize the fact that tertiary prevention is more widespread in practice than primary prevention and that measures taken at this level target the individual rather than problems stemming from the organization.
In our analysis of primary prevention definitions, several authors present actions more similar to those of secondary prevention, focused on monitoring and reducing existing stressors. The measures proposed presume that the workers are already exposed to stress and that the reduction of this stress was not considered while work situations were being designed. Several steps can be taken during workplace design to avoid the occurrence of work-related stresses, as NIOSH’s “Prevention through Design” illustrates. The goal of primary prevention should be to prevent the appearance of stresses (both physical and mental) in the workplace at the moment that workstations, organizational processes and production lines are conceived during expansion projects, implementation of new tools or new processes [37–39].
Thus, it is important to adopt the most proactive and operational definitions for workplaces, especially with regards to primary prevention. Vézina et al. [40] proposes the following definitions: Primary prevention: Measures taken during the design of new work situations aiming at the prevention of health problems or accidents. Secondary prevention: Worker population health status surveillance activities and screening of those at risk, leading to the implementation of programs or projects improving existing work situations. Tertiary prevention: Measures aimed at supporting worker’s return-to-work following a complete work disability (absence).
These definitions foster the operationalization of upstream prevention measures in order to act upon the work environment at all levels of workers’ health progression, and would be workable in the context of integrated strategies aimed at the coordination of prevention measures.
Strengths and limitations
In light of these preliminary results, some caution as to the established eligibility criteria set for the scoping review is warranted. First, the number of articles that met the selection criteria was limited. The scoping review was guided by the concept of “integrative prevention,” but it is possible that other approaches for coordinating prevention measures have been developed elsewhere.
Furthermore, most of the articles that were retained develop integrative prevention theory and provide reflection, but few describe how interventions were implemented in the workplace. Future research could better develop how interventions are carried out in the workplace. Analysis of the gray literature may be relevant to supplement these results.
More research is needed to determine which stakeholders to involve at each prevention level, to analyze how tasks are distributed among stakeholders at each level of prevention and to concretely explain coordination of these three levels of prevention in the workplace.
Conclusion
Several studies examining integrative prevention and the coordination of prevention measures were analyzed in this scoping review. Some articles indicate concrete measures to put in place in workplaces, but few were actually implemented and evaluated. Primary, secondary and tertiary prevention measures are described in the integrative prevention strategies, but little information is given on how to operationalize their coordination. This scoping review did lead to the clarification of concepts with an aim to developing integrative prevention approaches targeting the coordination of workplace prevention measures. Definitions for primary, secondary and tertiary prevention are proposed.
More work on the operationalization of interventions is needed before implantation in workplaces. More empirical studies would provide a better understanding of the barriers and facilitators for workplace implementation.
Footnotes
Acknowledgments
We would like to thank the organizations that financially supported this work: Fonds de recherche du Québec-santé (FRQS), Chaire de recherche de l’Université de Sherbrooke, CHU Sainte-Justine, Centre de recherche Interdisciplinaire sur le Bien-être, la Santé, la Société et l’Environnement (CINBIOSE), Centre de recherche sur les politiques en matière d’invalidité professionnelle (CRPIP), the Institute for work and health (IWH) and the Institut santé et société (ISS).
Conflict of interest
None to report.
ERIPRIT team is a French acronym (Équipe interdisciplinaire sur la prévention et la réduction des incapacités au travail) which refers to a Work disability research team led by University of Sherbrooke (Quebec, Canada). The group includes nine researchers in psychology, occupational therapy, human resources management, health economics and ergonomics. The mission is to foster the emergence of interdisciplinary projects focused on action and change in the field of work disability.