
Abstract
BACKGROUND:
Self-employment (SE) is a growing precarious and non-standard work arrangement internationally. Economically advanced countries that favor digital labor markets may be promoting the growth of a demographic of self-employed (SE’d) workers who are exposed to particular occupational diseases, sickness, and injury. However, little is known about how SE’d workers are supported when they are unable to work due to illness, injury, and disability.
OBJECTIVE:
Our objective was to critically review peer-reviewed literature focusing on advanced economies to understand how SE’d workers navigate, experience, or manage their injuries and illness when unable to work.
METHODS:
Using a critical interpretive lens, a systematic search was conducted of five databases. The search yielded 18 relevant articles, which were critically examined and synthesized.
RESULTS:
Five major themes emerged from the review: (i) conceptualizing SE; (ii) double-edged sword; (iii) dynamics of illness, injury, and disability; (iv) formal and informal health management support systems; and (v) occupational health services and rehabilitation.
CONCLUSION:
We find a lack of research distinguishing the work and health needs of different kinds of SE’d workers, taking into consideration class, gender, sector, and gig workers. Many articles noted poor social security system supports. Drawing on a social justice lens, we argue that SE’d workers make significant contributions to economies and are deserving of support from social security systems when ill or injured.
Introduction
Globally, self-employment (SE) has emerged as a key non-standard, precarious, and contingent work relationship [1, 2]. In the current digital age, SE appears in configurations and contours that differ from the labor market of 50 years ago and is part of a ‘paradigm shift’ from manufacturing/managerial capitalism to entrepreneurial capitalism [3, 4]. In Canada, for example, 2.9 million people were self-employed (SE’d) in 2018 and this is more than double those SE’d in 1976 [5]. Overall, SE’d workers account for 15%of employment in Canada [5]. Similarly, 10%of the Australian workforce is SE’d [6], and SE’d workers now comprise 15%of the workforce in Europe [7]. This SE trend is accelerating due to the rising ‘gig’ economy and the undermining of the former employment structures that provided secure, lifetime jobs with predictable advancement and stable pay [8–10].
In research literature, SE’d workers have been depicted as a special group of homogenous people [11, 12] who possess good health, enjoy the freedom of being their own boss and having flexible working hours, do not rely on the state (e.g., social security protection), and enjoy greater job satisfaction, quality of life, and opportunity to gain work-life balance than employees [7, 13]. They have a reputation for taking on a high level of personal risk to grow their businesses and also of creating employment opportunities for others [7, 15]. However, these depictions do not reflect the recent reality of SE [7, 16]. A murky, or dark side of the labor market, exists where a significant number of SE’d workers, both in high and low-income economies, are compelled to undertake this type of work due to unemployment, scarcity of alternatives, and other financial hardships [1, 17]. The diversity of SE’d workers is described by the Law Commission of Ontario (2012) who note that: “the experiences and vulnerabilities of this group range from billionaire entrepreneurs to taxi drivers working 90 hours a week simply to pay their bills and includes many people who are gaining income from SE activity alongside their main job” [1 p75]. Therefore, SE does not always mean self-sufficiency. Rather, some SE’d workers can be considered precariously employed as they earn low incomes and are at risk of poverty and social exclusion [1].
Mounting international evidence stresses that the changing nature of work is having profound adverse effects on workers’ safety, health, and wellbeing [4, 18–20]. For example, SE’d workers are at higher risk for certain diseases such as musculoskeletal disorders, joint pain, sleep disorders, and digestive complaints, compared to salaried workers [14, 22]. These risks stems from their job nature, for example, SE’d people encounter a higher level of job demands and workloads, self-exploition and absence of social protections, such as lack of health insurance, elevated anxiety about financial matters [14].
As well, SE’d workers are largely excluded from workers’ compensation coverage across jurisdictions [4, 23–25]. SE’d workers are often not eligible for sick pay, paid annual leave, or an old-age pension [25]. Without these safety nets, lower-income SE’d workers may unable to ensure their housing costs, medical expenses, food, and future security (e.g., retirement pension). They may encounter particular stressors due to work, or when out of work, as compared with employees in standard employment. In addition to income-based poverty, SE’d workers face particular challenges when they are unable to work due to illness or injury/disabilities, whether on a short- or long-term basis [4]. Surprisingly, very few attempts have been made to systematically investigate how these new forms of employment, including other forms of precarious employment, impact occupational injury and diseases.
Economically advanced countries that favor digital labor markets may be promoting the growth of a demographic of SE’d workers who are exposed to particular occupational diseases, sickness, and injury. Therefore, these jurisdictions may be considering the expansion of supports for sick and injured SE’d people and related changes in relation to labor laws, workers’ compensation policies, and social welfare policies. Despite the growth of SE in advanced economies, little is known how, and to what extent, social security systems support SE’d workers when they are away from work due to sickness and injury. Our overarching objective in this critical review was to understand how SE’d workers navigate, experience, or manage their injuries and illness when unable to work for health or impairment reasons.
Materials and methods
We conducted a critical interpretive review of peer-reviewed scientific literature [26]. Unlike a conventional systematic review, a critical interpretive review involves inductive interpretive synthesis that moves beyond aggregative summaries and enables reviews to build theory rooted in the empirical evidence under study [26]. This approach allowed us to appraise and critique a complex body of literature, irrespective of method, found by a systematic search. This method is particularly appropriate when there is a large body of diverse evidence on a subject [26, 27].
Searching the literature
Five databases were searched: Scopus, PsycINFO, CINAHL, PubMed, and ABI/INFO. The search was performed in January and February 2019. The choice of keywords and the search strategy were made in collaboration with a University of Waterloo librarian. Table 1 details the database search terms. To be included in this study, articles needed to focus on: 1) self-employment (either solo or with employees); 2) sickness, injury or disability; and 3) policy, insurance or other support systems relating to the inability to work or diminished capacity to work. As well, the articles had to focus on economically advanced economies as we sought comparable social security systems across the studies. Finally, articles had to be published in English in a peer-reviewed journal in 2001 or later.
Details the database search terms.
Details the database search terms.
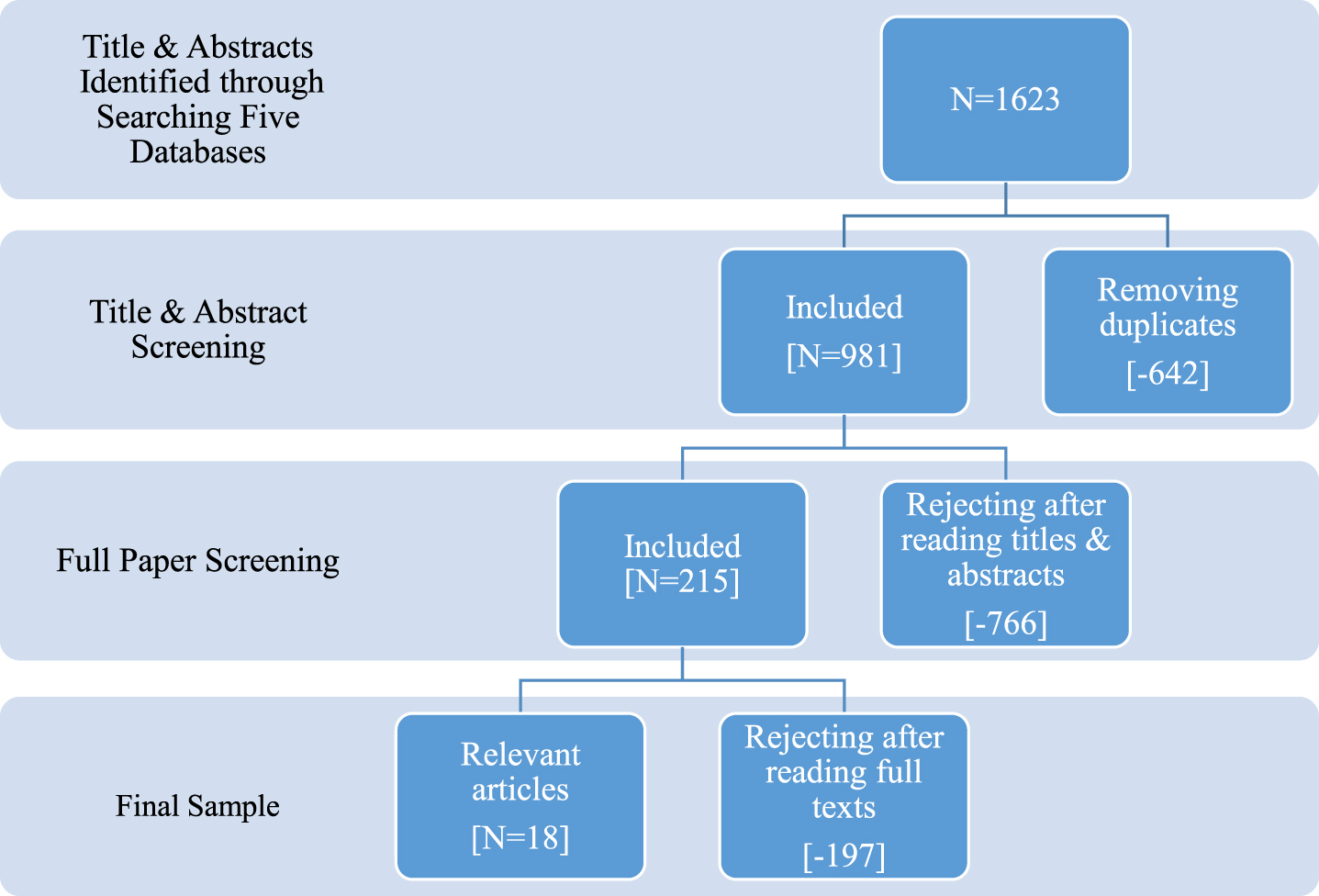
The database search yielded 1623 articles (See Fig. 1). After removing duplicates (642), 981 articles were screened by examining titles and abstracts. Inter-rater reliability among the three reviewers (the lead author and two colleagues) was established through a series of trials until 95%agreement was reached. A total of 766 articles were excluded after reading titles and abstracts and a further 197 articles after reading the full-texts. Thus, our final sample included 18 relevant articles.
Flowchart of the literature search.
The final sample of 18 articles was examined following Dixon-Woods and colleagues’ processes of quality assessment, data extraction, and data synthesis [26, 27]. They underline the importance of assessing the quality of the articles to be included in the review and analysis in terms of examining their overall relevance to facilitating understanding of the topic under study. Our critical approach added an additional step of evaluating the theoretical and substantial foci of articles for gaps and limitations in perspective.
Systematic data extraction focused on demographic information, research questions, study aims, year of publication, place of publication, methods, main results, important findings, sector of SE, work-induced injury/disability or congenital, and types of SE (full time or part-time). This approach resulted in a comprehensive overview of the final articles and facilitated analytical exchanges between the authors. A summary description of the studies can be found in Table 2.
Description of articles
Description of articles
Data were synthesized by recurring concepts, which ultimately contributed to themes. A process of constant comparison and negative case analysis guided the synthesis, which involved assembling issues and grouping topics under common concepts, and a reciprocal and iterative process to detect similar and analogous findings. For example, authors might use dissimilar words, but might be addressing a similar general concept (e.g., SE, independent contractor, contingent worker). The negative case analysis focused on studies that appeared to contradict each other. For instance, several studies reported that SE’d workers are generally healthier than wage workers [14, 29] because of flexibility, autonomy, and control over work. However, many articles stress that SE may bring physical and mental health hazards because of workload, self-exploitation, heavy physical jobs, and volatile income [7, 30–33] and isolation [34, 35]. In these cases, we attempted to reconcile these contradictions by noting contexts and methods. In this example, the negative case analysis directed attention to the nexus between SE and health in terms of relative benefits and demerits, which provided insight into how SE can have negative repercussions on health. Three phases of synthesis led to the final themes. First, an open-coding system was used to analyze the articles. This helped us to reflect on the overall patterns of our data, including identifying the repeated and common themes. In the second phase, open codes were re-reviewed and focused codes were generated. A focused code is a pattern or category that groups together two or more open codes [36]. Our focused codes then led to six major themes, together with sub-themes, focused on issues around SE, relative benefits and barriers, dynamics of illness, injury, and disability, formal and informal health management support systems, sick leave and health insurance, and occupational health services and rehabilitation. The lead author met and consulted with reviewers on a regular basis to discuss ongoing analyses of findings and to challenge preliminary interpretations, which facilitated thorough interpretations of the findings.
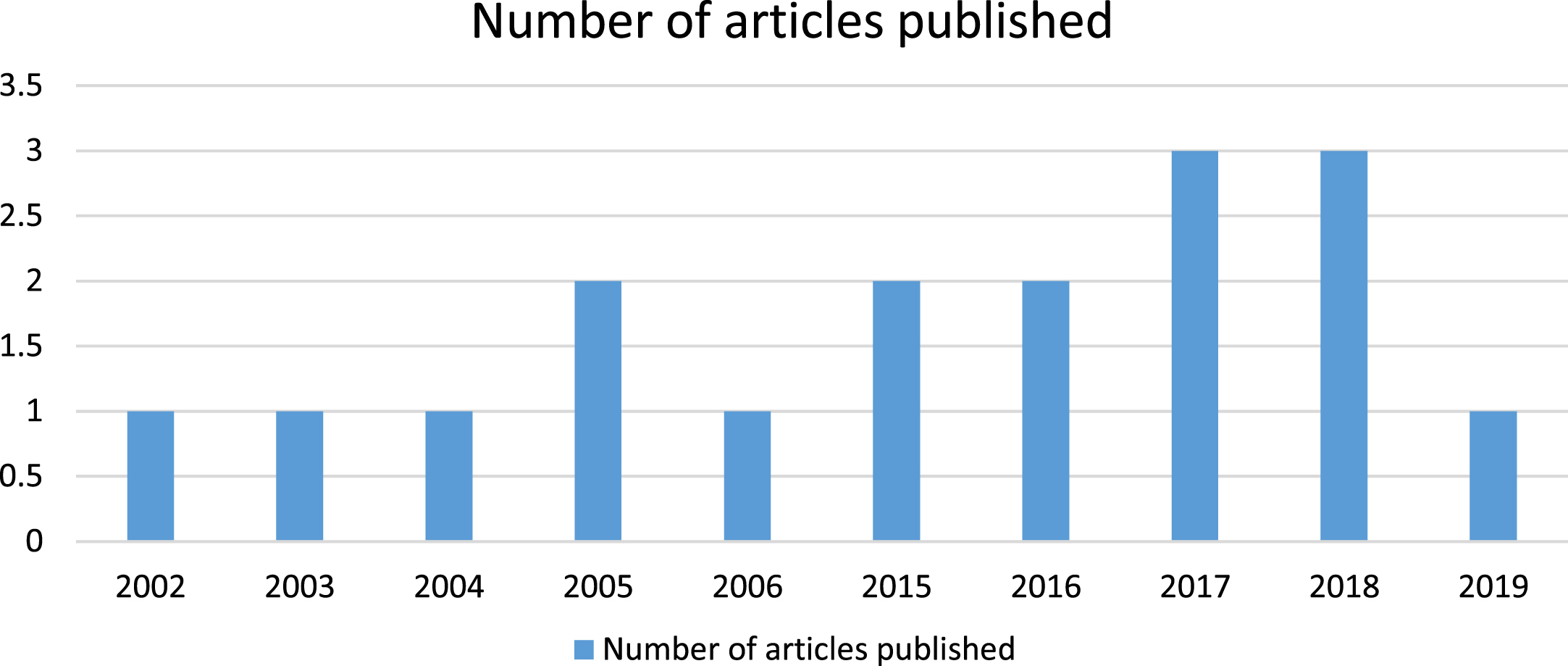
Of the final sample of 18, more than half of the articles [11] were published between 2015 and 2019, as presented in Fig. 2.
Distribution of articles by year.
Half of the articles focused on the United States of America, while the remaining articles focused fairly evenly on the Netherlands, Australia, Canada, Germany, and France. Two articles focused jointly on European countries, as shown in Table 3. Thus, the issues of health (e.g., sickness and physical impairments) and health management among SE’d working populations appear to be under-researched in advanced economies. More than half (10/18) of the articles were based on quantitative analysis, and only four articles focused on qualitative data, while the rest of the articles were mixed method, commentary, discussion paper, and a policy paper, as shown in Table 4, which shows the substatuve foci of the sample articles.
Article published by country/geographical region
Study methods
Five themes and twenty-one subthemes emerged through an iterative process of data extraction and synthetization from 18 articles. The themes were (i) conceptualizing SE; (ii) double-edged sword; (iii) dynamics of illness, injury, and disability; (iv) formal and informal health management support systems; and, (v) occupational health services and rehabilitation. These are summarized in Table 5.
Summary of the themes and sub-themes
Summary of the themes and sub-themes
This section describes issues related to conceptualizing SE according to objective or structural conditions or according to purported subjective traits of SE’d people. Several articles described challenges regarding classifying or defining SE status [7, 37], including three articles [30, 38] that attempted to debunk this issue. Gevaert et al. [31] related two approaches –objective and subjective –to identifying SE. The objective approach defines SE from the legal, social, and contractual framework of a given country, including salient traits, such as the absence of regular wage relationship, independence in terms of a certain degree of economic and organizational autonomy, working with or without employees, and magnitude of economic activity. Rizzo [38] adopted a similar objective, or structural, approach to defining SE. However, two articles [7, 37] discussed how difficult it is to administratively identify SE’d people, with Quinlan’s article from Australia[37] elucidating how it has become common for employers to misclassify employees in order to avoid welfare and compensation coverage payments.
Substantive foci of papers
Substantive foci of papers
The second approach discussed by Gevaert [31] is subjective and focuses on individualistic traits of SE’d individuals. This is attached to the discourse of the “entrepreneurial self”, implying that SE’d are those people encompassing attributes associated with entrepreneurialism, including creativity, willingness to take risks, innovativeness, high intrinsic motivation, skillfulness, and the ability to recognize opportunities. Gevaert et al. [31] also discussed concerns about defining SE using lenses of the “entrepreneurial self” because of the risk of classifying people in neoliberal terms; a standard for which they ask, “to what extent even ‘real self-employed’ actually meet up to” [31]. The essence of Gevaert et al.’s [31] analysis is that there are pull factors that render people more willing to enter SE. Discourse underlying the “entrepreneurial self” approach relates to SE more broadly and advances the question of whether this explanation can be generalized to identify SE’d workers. Authors of several articles note that pull factors are often dismissed because some people opt for SE as an alternative to unemployment or as a good fit with a congenital disability. Thus, they may be forced to engage in SE against the backdrop of developing an identity in a society or integrating into mainstream society [28, 38–41].
In discussions of why individuals enter into SE, a controversial issue emerged in some articles [7, 42] with respect to the relative benefits and barriers of entry to this form of work. On the one hand, people chose SE because of the benefits. Articles on the views of SE’d workers [7, 42] described varied reasons for choosing SE: it provides flexibility (e.g., work-life balance, caring for children and household chores that often fall on the shoulders of women) [28, 42], reduces discrimination (e.g., income inequality), increases independence or control over job (e.g., decision making) [34], and provides an identity of being own boss [28]; provides a sense of identity (e.g., people with disability) in a broader context [34]; and, it offers freedom and autonomy in terms of type of job, pace and schedule [7]. People with congenital (present from birth) disabilities welcomed SE as it helped them to integrate into mainstream society with a social identity [34, 44], which is why the number of persons with disabilities is higher in SE compared to the general population [41]. However, a number of articles [7, 42] underlined barriers to SE, such as job demands, self-exploitation, selection effect, cost of health insurance, and sick leave related complexity. In all, as proposed by one article, SE appears to be a “a double edged sword” [14]. On one hand, SE appears to be valued for the freedom and flexibility from certain aspects of traditional employment. For example, the ability to set one’s own hours and workload and the autonomy and identify affiliated with being one’s own boss, are potential pulls. Conversely, elements of insecurity are created by entering SE, such as potentially variable work and lack of insurances. This opposite side of the sword may cause circumstances that impact health and potentially negate any real or perceived health benefits derived from SE.
Dynamics of illness, injury, and disability
The articles included debates around whether SE’d workers are healthier than wage earners [7, 42]. One article discussed the view that SE’d workers are healthy because of the flexibility in work, [28] including their ability to take care of their health by buying private insurance [29]. However, other articles [7, 30–33], drew attention to physical and mental health hazards due to workload (e.g., farmers), drudgery (e.g., long working hours), heavy physical jobs, isolation due to working alone, reputational threat, customer and contractor betrayal, volatile income, financial worries, and less access to, or no occupational health services.
Interestingly, a few articles [32, 45] underlined the nexus of SE’d farm work and aging, which is intertwined with the health and wellness of SE’d farmers. Authors expressed their concern about how ‘aging’ undermine farmers’ health, as it is connected to a variety of diseases, such as musculoskeletal disorders. In Australia [33], Beattie et al. raised a concern that farmers are forced to work before complete recovery from hospital and rehabilitation because of their workload and lack of help [33]. One article provided statistics demonstrating how Australian farmers are more vulnerable than salaried workers, where farm injuries account for 17%of all worker fatalities [7]. Another study of SE’d people in the Netherlands underlined musculoskeletal disorders as a common cause of sickness absence in the farming sector [45].
A study [30] conducted in France found that SE’d workers in the foodservice industry were at higher risk of physical and mental health hazards than regular employees. The prevalence of a diseases such as sleep disorders, joint pain, musculoskeletal disorders, cardiovascular disease, digestive complaints, audiogram, and urinary abnormality was significantly associated with SE [30]. A study [7] of European data on SE and salaried workers’ cancer survival, provides further context in that, irrespective of cancer diagnosis, mortality rate was higher among solo SE’d people than salaried workers.
Mental health and illness of SE’d people were addressed in two articles, with SE’d people described as more vulnerable to mental disorders and illness than medium and large entrepreneurs and salaried workers [31]. Gevaert, De Moortel [31] identified some work traits of SE’d people, including being creative, risk taking, innovative, motivated, skilful, and able to recognize opportunities. They stressed that the absence of these charactertistics are responsible for poor mental health [31]. An article by Sharp et al. compared SE’d cancer survivors with salaried cancer survivors and found that salaried workers received social, emotional, and instrumental supports from managers and co-workers, which positively impacted post-cancer recovery and health management, including mental health. However, these services and supports are often unavailable for SE’d workers because they work alone [7].
Health management support systems
Several articles shed light on formal and informal support systems available for SE’d people across economically developed countries [18, 46], focusing on overarching themes of sick leave, health insurance, rehabilitation/vocational rehabilitation, family supports, and other social networks. The articles delineated various state-level support systems for SE’d such as government policies and services (e.g. health insurance, sick leave, income replacement or compensation in the USA, the Netherlands, Australia, and Canada) [29, 46] as well as support from non- government organizations and non-partisan groups (e.g., the Canadian Taskforce for Women’s Business Growth) [42], private agencies (e.g., health insurance providers in USA, Canada, Australia) [32, 46], and local organizations (e.g., local chamber of commerce in Canada) [42].
In relation to informal support systems for SE’d individuals, Hilbrecht describes varieties in Canada, [42] including instrumental support connected to practical assistance in terms of concrete skills or resources (e.g., receiving babysitting from a neighbor due to sudden need to meet a client); emotional supports, such as empathy or reassurance, especially during unstable or unexpected economic conditions; informational supports (e.g., offering valuable suggestions); and social networks (e.g., disabled workers association, business groups) [42]. Articles from the US also delineated how SE’d people with disability benefit through supports from similar informal groups and social networks [28, 41].
Articles addressing formal support systems for SE’d individuals focused on Canada, Australia, and the USA and noted that support for SE’d individuals relative to salaried workers was poor, as few countries have social security systems designed to support SE’d workers [7, 46]. For example, Fossen and Konig [29] mentioned that health insurance systems have been designed primarily to protect paid employees in the USA. Although social security supports SE’d people exist in some jurisdictions, such as Canada, recent research shows that the SE’d people are not aware of these supports and they are under-used. For example, recently introduced Canadian federal government special benefits for SE’d workers, including maternity leave, parental leave, compassionate care leaves, sickness benefits, and benefits for SE’d parents of critically ill children, [42] were not known to SE’d workers [42]. Similarly, Barber III and Moffet [46] note that SE is affected by “job lock” systems, in which incentives or subsidies for health insurance do not guarantee that more wage earners will enter into SE because of barriers posed by other drivers, such as payroll taxes, capital investment, and capital gain [46].
Several articles focusing on USA, Germany, Australia, and the Netherlands, stress that SE’d people are less privileged than salaried workers, in terms of paid sick leave, sickness benefits, disability benefits, health insurance, and occupational health services [7, 46]. Two articles, from Australia and the Netherlands, where income supports are available to SE’d workers when injured or ill, demonstrated a causal relation between age and sick leave claims, demonstrating that aging is a crucial factor because sick leave claim rates increase with age, and older claimants seek more sick leave, predominately due to musculoskeletal disorders [32, 33]. Therefore, age is an important factor because SE’d are older than wage earners, found in at least in one American study [18]. A Dutch article found that in the Netherlands among SE’d workers, experiencing a first episode of work injury strongly predicted subsequent sick leave. Musculoskeletal disorders and mental illness cause most of the long-term sickness absence for SE’d in Denmark, and it differs in terms of the sector of SE. Therefore, some sectors of SE, such as farming and the food service industry, are more prone to expose risks in terms of health and illness for workers [32, 45].
Many articles presented a lack of health insurance as a strong deterrent to SE’d people taking sick leave [14, 42]. One article from Germany stressed that people avoid SE because of the higher cost of health insurance [29]. In the US, a study found that more people were interested in SE when a state provided subsidies for health insurance [46]. In terms of geographical setting, in the US, a study found that the number of SE’d people who do not have health insurance is higher in rural areas than the urban areas [40]. In practice, in most of the cases, SE’d workers have to depend on private insurance for health care and other compensations (e.g., income replacement). As these supports are costly and many cannot afford it, most SE’d people, especially those who are low earners, are not interested in adopting these supports [29, 37].
Occupational health services and rehabilitation
Several articles in this review argue that injured or disabled SE’d workers (e.g., in Germany, Australia, USA) have meager access to occupational health services and limited, or a complete lack of, vocational rehabilitation [14, 42]. The authors stress that SE’d workers require basic supports for rehabilitation and reintegration in labor markets following illness or injury, including education, degrees, training, and occupational health services [14, 42]. Several articles (e.g., in the USA and Europe) in our review stressed the significance of vocational rehabilitation counselors (VRC) for SE’d workers [28, 41]. However, their value was contested. Some authors argued that VRCs had a positive role in supporting SE, others found either ‘no’ or ‘negative’ impact of VRC for SE’d injured or disabled workers [39, 47]. Another tool for supporting SE’d workers is micro-credit. Arnold and Ipsen [39] showed how microcredit can be a successful means for rehabilitation for SE, who have disability, in American society. Through these interest free (or limited interest) loans, people with disablitites can create viable business in order to earn their livelihhod.
Discussion
The 18 articles included in this review covered diverse aspects of how self-employed are supported when they are unable to work due to illness, injury, and disability. In our view, one of the challenges of providing supports to SE’d people is derived from unclear definitions of who is SE’d. Three articles in our review attempted to demystify the conceptualization of SE [30, 38]. Key to this perspective is Gevaert et al.’s analysis that pull factors, such as flexibility, draw people to enter into SE [31]. We question if this explanation is broadly applicable to SE’d workers. It has become common to promote pull factors by highlighting that people opt for SE, both as an alternative to unemployment and a good fit for persons with a disability. This latter view downplays the context of underlying social and economic conditions [7, 31], and is inconsistent with an OECD cross-national study asserting that there is a causal relationship between unemployment and SE [3].
In the age of post-industrial labor markets, entrepreneurial capitalism [3], and fissured workplaces [4], SE as a category of work continuously “receives fresh blood and loses old blood through underground mobility” [3 p131], that is to say, SE is incessantly being reshaped in form and fashion, and it has become common for some wage-earning workers to also work as a SE in some sectors part-time. For example, conventional ideas of SE do not capture the working life of Uber drivers and Airbnb hosts, most of whom have another main job [48]. Conventional discourses defining SE have not acknowledged the heterogeneity of the new modes of SE work, despite several hybrid forms of SE [3, 16]. Weil [4] raised a very timely and crucial question, with respect to “fissured workplaces” about the restructuring of work arrangements in American society. This is now here clearer than between regular employees and those in alternative work arrangements, such as limited-term contracts, work with staffing agencies, and SE [4]. New forms of work, including freelancing, micro-farming, Uber driving, and Airbnb hosting, challenge the traditional understanding and conceptualization of SE. Despite this complexity, employment statistics, such as American household (e.g. Current Population Survey, Contingent Worker Supplement) and employer-based surveys (e.g. current employment statistics or Quarterly Census of Employment and Wages) do not sufficiently capture all relevant features of SE. As a result, existing estimations and definitions related to SE, for instance, in the USA, are insufficient and contradictory [4].
In this review, surprisingly, we found very few articles that exactly focused on our research question. Of the three components of our research question –SE status, issues around health and sickness, and state support systems, few explored all three components in depth. For example, Beattie et al. mainly discussed the experiences of Australian SE’d farmers after a serious farm injury [33], but barely addressed the experiences of how the injured farmers were supported during their sickness or when they were away from work. Similarly, Ashley et al. focused on people with congenital disabilities who are SE’d, and on available support systems to manage and grow their business, but not on work-induced injury or disabilities [41]. Yoon and Bernell placed more importance on the health issues (prevalence of health conditions) than health management issues (what happens when injured or ill) [18] and the Sharp’s article is a commentary, with an overall focus on the three components [7]. As such, there is a clear-cut knowledge gap in understanding the experiences of SE’d workers in relation to their health, illness, and work injury, and how they manage their illness and livelihood when they are unable to work.
It is unclear how the gig economy impacts occupational health and health-related services and social securities of SE’d workers. In our view, SE is inevitable in the age of flexible capital accumulation but needs proper supports to grow and be sustained [25]. However, globally several intermediate classes, such as temporary staffing agencies, are exempted from accountabilities in terms of providing legal and social security protections [49]. These gaps raise ethical and philosophical questions about working relations, in relation to neoliberal and capital market demands that provide value to consumers and investors, but fail workers. What is particularly interesting is that SE’d workers in complex supply chains are sometimes not aware of who funds their positions. Some employers intentionally set up workers as SE to evade or reduce tax liabilities or employers’ responsibilities –are called false (bogus) SE [50, 51]. Essentially, this neoliberal approach makes workers responsible for their own social protection.
Our review reveals that there is an ongoing debate around whether SE’d workers are healthier than wage earners. There is a hegemonic and popular discourse about positive experiences of SE’d people, with several articles promoting the view that SE’d workers are healthy because of the flexibility in SE’d work, [7, 42] and can, therefore, take care of their health (e.g., buying private health insurance and medical care) with their savings, enjoy better quality of life and health status, greater job satisfaction, and many more advantages compared to salaried workers [29]. In our view, however, these assertions are outdated. In practice, with diverse type of SE, including digital platform gigs, it is likely that many SE’d workers are earning low wages [52].
With few exceptions [53–55], we know very little from the existing literature on how contemporary SE’d people experience their work and health. As such, it is necessary to explore empirically how sector-specific SE’d people survive with low incomes, especially when injured or ill. Currently, statistical analyses do not accurately reflect the situation of SE’d people in economically advanced countries in the case of SE, and may not be applicable for other countries. It is noteworthy that most of the articles in our sample are based on quantitative analysis, national surveys and concentrated in the USA [18, 29]. Ultimately, what is at stake is a nuanced understanding of experiences of health, sickness and injury experiences of SE’d people. Research, based on quality or mixed-method approaches is needed, and more quantitative research is needed to explore the prevalence and role of SE. As well, because SE in the gig economy often involves workers doing multiple jobs (e.g., Uber drivers), possible negative health repercussion needs to be explored.
Class and SE is a topic that requires attention. For instance, in economically advanced welfare state countries, research studies often present SE’d farmers as healthy, but it is historically evident that SE’d farmers are rich through inter-generational inheritance, and thus have a certain amount of land and housing, and annual farm production and profit. Therefore, their health status must be framed according to their privileged position and the cannot be compared with other SE’d workers, such as those in the gig economy. Interestingly, some researchers expressed their concern about farmers because ‘aging’ is undermining their health status, and aging is connected to a variety of diseases [33]. Farmers are forced to work before complete recovery from hospital and rehabilitation because of workload and lack of help [33]. They are also vulnerable in terms of mental health, as they are socially isolated. While salaried workers are mentally supported by their coworkers, SE’d people work alone; thus, they are more vulnerable in terms of mental health and illness than salaried workers [7, 22]. A timely concern of consequence is that the next generation is not willing to continue with farming,[33] and this situation is aggravating the health of aging farmers.
A growing concern world-wide is that SE’d people working alone at home experience different physical and mental health hazards due to isolation; for example, 40%of SE’d people in the UK say they have felt lonely since becoming their own boss, which has profound impact related to depression, heart disease [35]. Ultimately, the work and health of SE’d workers is unclear and requires analysis taking into account the nature and sector of jobs and income level. Though many governments are encouraging SE, Gevaert et al. [31] acknowledged that the work-related mental well-being of SE’d people remains understudied and unexplored. In our view, mental and physical health issues of SE’d people need to be addressed in legislation and policies related to workers’ compensation and labor standards, and more research addressing this lacuna is needed. Although SE’d workers make significant contributions to economies [4], the discourse of providing social security system support them is surprisingly ignored globally despite their similar life needs in relation to wage earners in terms of foods, housing, and health care [25].
Our review suggests that government and statuary supports to SE’d people in economically developed countries are limited (e.g., Canada, Australia, and France) compared to salaried workers, although some countries have statuary policy, such as health insurance, sick leave claim, to support SE’d workers (e.g., USA), as described in several articles in our sample [7, 30].
Our review also finds the existence of informal supports to help to grow an independent business [42]. However, as Beattie et al. stressed, without compelling government-sponsored social protection and support systems, there is no sustainable solution for the growing SE’d population [33]. In this context, we examine the situation of SE’d workers using a lens of social justice. Whether someone is working for wage or profit, under a contract, or providing gig services, their employment status should not be a determining factor or cornerstone to determine their eligibility for social protections, social insurance or tax legislations. All are workers with their only asset of human capital; thus, all workers who depend on the sale of their capacity to work and survive should be covered and protected by labor protections and social supports [20]. In this sense, there is a knowledge gap in understanding how SE’d workers are ensured social justice. In Australia, there is an assumption that SE’d are less likely to make compensation claims, compared to regular employees [37]. SE is one of the four categories of employment with the highest underreporting of compensation claims [23]. So, in Australia, similar to Canada, [42] SE’d workers are excluded from worker’s compensation claims, and even those covered do not lodge claims because of lack of knowledge of their entitlement [4].
The essence of the authors’ [19, 42] arguments draws attention to a recent debate in Canada about whether SE’d workers need government supports or whether these external supports should be approached in a sector-specific manner. In 2013, the Ontario workers’ compensation board imposed mandatory insurance on SE’d construction workers [56]. This decision prompted large protests from the SE’d independent contractors, who resisted the policy, which required them to pay six to seven times more than their ongoing personal insurance policies. They saw this as unfair and discriminatory to SE’d workers because the workers’ compensation insurance only covered work-related injury, while their private insurance covered all health conditions, regardless of the source of the injury or illness [56]. In our view, this debate calls for further study to understand the nuanced motives of SE’d workers behind acceptance or rejection of the government support and what kinds of programs would provide the kinds of support needed by SE’d people.
In our review, sick leave claim, aging, and musculoskeletal disorders are found to be intimately connected, because sick leave rates increase with age and older claimants seek more sick leave, predominately due to musculoskeletal disorders [32, 33]. In a similar vein, we argue that researchers should investigate how age along with gender, race, or ethnicity may influence SE’s health and return to work. Though several articles in our review addressed the role of health insurance and state subsidies or support systems, it remains unclear whether SE’d people who are subsidized by the government will take on the expense of health insurance [29, 33]. We suggest that state-sponsored and subsidized health insurance can play a pivotal role in growing SE. However, there are job lock effects counteracting this, as more incentives or subsidies on health insurance do not guarantee that more wage earners enter into SE due to other drivers, such as payroll taxes, capital investment, and capital gain, which underpin the barriers to entry to SE [46].
Conclusion
Results from this critical interpretive review of SE in economically advanced countries draw attention to controversies over conceptualizing SE status, why people choose SE, merits, and demerits of SE, and how SE’d people are supported by formal and informal health systems. A common issue was a lack of eligibility among SE’d workers for social protections, and almost no studies addressed how SE’d workers manage when they are unable to work due to sickness and injury. Through this synthesis, we have provided a clearer picture of SE labor conditions, elucidating how the discourses of SE’d workers’ health, sickness, and return to work are under-researched in academia and public policies. Under the circumstances, we believe that creating necessary support systems for sick and injured SE’d workers to support their return to work is of paramount importance and that future research should consider the broad diversity among SE’d workers and their contexts.
Footnotes
Acknowledgments
The authors wish to thank the University of Waterloo librarian, Jackie Stapleton, for her help with orienting and conducting article search processes. The authors also wish to thank their lab member, Meghan Crouch, for her support with testing interrater reliability. Finally, the authors acknowleldge the supports from the SSHRC/CIHR Healthy Productive Workforce Partnership Grant, Grant number: 895-2018-4009.
Authors’ contributions
Tauhid Hossain Khan (TK) and Ellen MacEachen (EM) conceived the original idea of the review.TK, with the help of a librarian, conducted the database search and the first selection of articles to be included in the review. EM approved the included articles, TK and EM discussed the final inclusion of articles in the review. Julia Goyal(JG) took part in testing interrater reliability. TK and Pamela Hopwood (PH) conducted screening the titles and abstracts of the articles to obtain a finale sample. In every stage of screening, TK and PH were supervised by EM. TK and PH extracted the data from the final sample of articles. TK synthesized and analyzed the data under the guidance of EM, and both TK and EM contributed significantly to the critical synthesis processes. TK drafted the manuscript and EM read and added to it. Finally, the first three authors read and approved the final version to be published.
Conflict of interest
None to report.