
Abstract
BACKGROUND:
Musicians’ health is an essential field of healthcare that is specifically tailored to the needs of musicians, which encompasses multiple facets of health.
OBJECTIVE:
The research seeks to determine the prevalence of physical injuries in music students and musicians, and to identify possible causes.
METHODS:
A previously unvalidated 42-item survey was distributed to music students, non-music students, and professional musicians. The questions addressed demographics, physical health, mental health, medication use, and interest in musicians’ health. The study was conducted from Fall semester 2017 to Winter semester 2019 at McGill University, with analysis completed in August 2019.
RESULTS:
A total of 585 complete responses were obtained. Music students (35%) had higher prevalence of physical injuries than non-music students (18%), and professional musicians had the highest prevalence (56%). Multiple factors dictate the prevalence of physical injuries among musicians, including gender, age, program of enrollment, and instrument of choice. Of note, daily duration of practice was not one of these factors.
CONCLUSIONS:
Several factors were identified through this cross-sectional analysis to be associated with musicians’ physical injuries. These findings can serve as a foundation through which physicians and post-secondary institutions may implement changes to better enhance the physical health of musicians. It also cast doubts on previous assumptions associated with physical injury of musicians.
Introduction
Musicians’ health and well-being encompasses their physical and psychological health, including but not limited to musicians’ injuries, their use of prescription medications, performance anxiety, depression, etc. The limited literature available is restricted by narrow scope, poor experimental design, or outdated data [1–3]. Due to the nature of a musician’s training, it is common for many to sustain physical injuries [4–6]. In prior literature, these injuries are referred to as playing-related musculoskeletal disorders (PRMDs) [7], a term which we will use synonymously with physical injuries which impact playing. Previous research demonstrates the importance of screening music students early in their education [8], and to make appropriate changes to their long term-training [9, 10].
Though practice methods such as the Alexander Technique [11, 12] have been utilized with varying success [13], we seek to understand the exact factors [14], modifiable or unmodifiable, which predispose musicians to PRMDs. Previous studies have found that further investigations should be longitudinal and should include the physical injuries of populations beyond professional, or classically trained post-secondary institution-based musicians [15]. By understanding these risk factors, physicians and educators can identify musicians who are predisposed to PRMDs and work with them on preventing and managing injuries. Only by understanding the severity and shortcomings in the current state of health among musicians can we truly begin to make changes and provide musicians with an environment which fosters open discussions on health with the hopes of advancing the culture of musicians’ health. The first step in working towards this is to gather information on musicians’ physical health and injury rates in order to understand how to better support musicians throughout all levels of their career.
Methods
Participants
(a) Music students –undergraduate students registered in the music program at the undergraduate institution; this is our primary population of interest. The participants in this category are further broken down into subcategories for further analysis based on their age, duration of practice, subspecialty program of enrollment, and year of study at the institution.
(b) Non-music students –undergraduate students registered in a program other than music at the undergraduate institution. This was selected as our control population to allow for excluding biases such as age, or the stressors of being an undergraduate student. We further subdivided this cohort into non-music students who play an instrument and non-music students who do not play an instrument to determine whether it is the act of playing an instrument, or the study of an instrument in an undergraduate academic setting that has an impact on physical injuries.
(c) Professional musicians –any musicians associated with an academic or professional music organization, or performers who had graduated with a degree in music. This population of participants is our secondary population of survey.
Procedure
Following ethics review board approval from McGill University [16], a 42-item voluntary survey was made available online and on paper to students recruited in classes, and to community-based professional musicians online. Since the survey was carried out in a bilingual province, it was made available in both English and French. At each time point, participants were reminded not to duplicate survey entries. There were no compensations or benefits, and implied consent was obtained through voluntary participation. The survey obtained information regarding demographics, physical and mental health, medication use, and musicians’ health initiatives. We approach PRMDs as one aspect of many in a multidisciplinary approach, as previously suggested in an orchestral-based analysis [17].
The physical health section included questions on the current and past PRMDs, specifically, whether the participant sought help from a healthcare professional, whether the injuries originated from instrument practicing, and the anatomical location of injuries. These questions were designed as an adaptation of the Nordic Musculoskeletal Questionnaire (NMQ) [18], but with 3 major improvements –(a) defining the injuries as PRMDs, in line with other publications in this field, (b) introducing more regions/categories of injury to take into account the nuanced injuries of musicians, (c) addressing the acute vs chronic components of injury, as prior studies have demonstrated the association between past injuries with present ones [3].
Measures
The variables of comparison determined in the demographics section were based on pilot study data and previous variables associated with the physical health of musicians [5, 19]. The adapted NMQ questions included in the physical health section of the survey were not previously validated, but prior studies on adaptations of the NMQ have shown comparable validity [20–22].
Our sample size for our primary population of interest, music students, was set to be over 60%of the total number of students enrolled in the music faculty. Due to the ethics board requirements set by the University, we were unable to determine the reasons and the exact number of participants who chose not to complete the survey.
Analysis
All survey entries were verified twice by researchers and processed using a pre-specified protocol (Fig. 1). Non-music students who play an instrument served as the control. Fisher’s exact test was used to analyze all nominal data (Fisher’s exact test was used because some categories had fewer than 5 participants due to the criteria of the categories). One-way ANOVA tests were used to analyze all ordinal data, and the Tukey HSD test was performed for all post hoc comparisons. Not all participants answered all the questions; those jeopardizing the accuracy of the survey were excluded based on protocol (< 1%). As well, questions answered with the option “Prefer not answer”, or those left blank, were excluded from the analysis of the given question. The significance level was set at 0.05 and the statistical analysis was performed using GraphPad Prism, version 8.0.2.
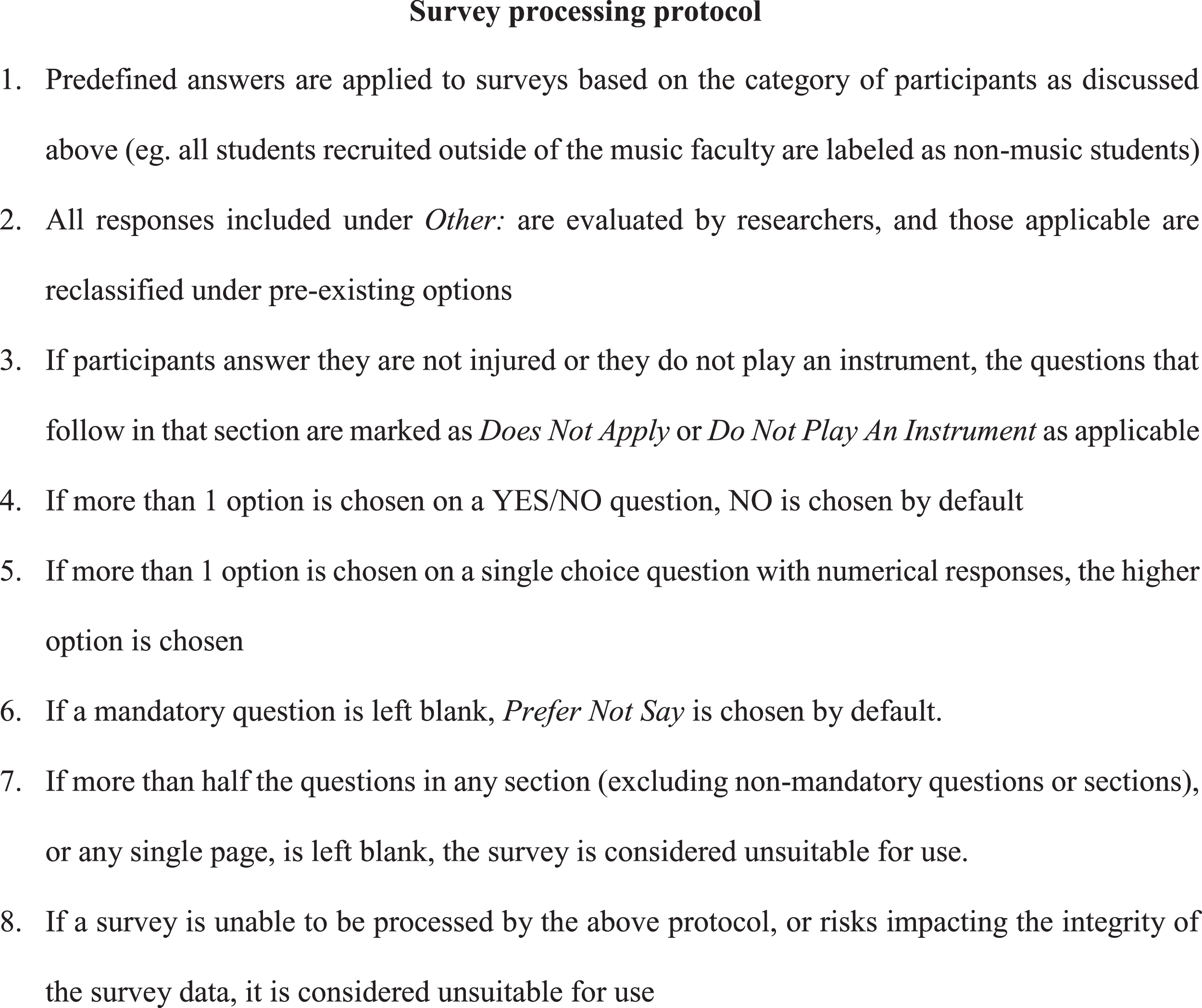
Protocol used to analyze usability and completion of the survey, as well as when individual questions were left empty.
General demographics
A total of 585 surveys were collected throughout the data collection period. This included 403 (69%) entries from music students, 132 (23%) entries from our control group non-music students, as well as 50 (9%) professional musicians working in the community. Over the span of the Fall 2017 semester to the Winter 2019 semester, there were 599 students enrolled in the music faculty [23, 24], of which our sample represented 67%(Table 1).
Breakdown of demographics
Breakdown of demographics
*Number in parentheses representing the percentage of the participants who meet the given criteria within that participant category.
General comparison
Comparing the overall prevalence of PRMDs, music students were found to have a significantly higher prevalence compared to the non-music students who play an instrument control. Moreover, professional musicians had a significantly higher prevalence compared to both music students and non-music students who play an instrument control (Table 2).
Prevalence of PRMDs between participant categories
Prevalence of PRMDs between participant categories
The number of PRMD locations reported by the participants were also found to be significantly different (F(2,564) = 16.03, p < 0.001). Post hoc comparisons indicated that the mean number of PRMDs of music students (M = 0.75, SD = 1.26) was significantly higher than that of non-music students who play an instrument (M = 0.25, SD = 0.63). The mean number of PRMDs of professional musicians (M = 1.28, SD = 1.55) was also significantly higher than that of non-music students who play an instrument. There was also a significant difference between the mean number of PRMDs when comparing professional musicians to music students.
The 3 target populations had no variance regarding whether injured participants consulted a healthcare professional. Nor, was there any difference whether the injury occurred as a result of practicing an instrument.
Comparing the effect of practicing on prevalence of PRMDs, participants who practiced less than 1 hour per day had a significantly higher prevalence of PRMDs in music students relative to the control group, but the same was not seen in professional musicians. However, professional musicians who practiced 1–2 hours per day had a significantly higher incidence of PRMDs when compared to both music students and the control group (Table 3).
Fisher analysis of PRMDs with increasing practice times per day within each participant category
Fisher analysis of PRMDs with increasing practice times per day within each participant category
Among music student participants (F(4,366) =0.56, p = 0.70) and professional musician participants (F(3,45) = 0.47, p = 0.70), no variations were observed between individuals of different daily practice durations. However, there was significant variance within non-music students who play an instrument (F(3,75) = 3.72, p = 0.02). Post hoc comparisons indicated that the mean number of PRMDs of non-music students who play an instrument who practiced 1–2 hours daily (M = 0.63, SD = 1.01) was significantly higher than those who practiced less than 1 hour daily (M = 0.10, SD = 0.31).
Next, the impact of the number of years a student has studied in a post-secondary institution on PRMDs was investigated. Music students in years 1 through 3 had a significantly elevated risk of developing PRMDs. However, students in Years 1 and 4 still had a significantly lower prevalence of PRMDs compared to professional musicians (Table 4). Within the music student population examined longitudinally, there was a significant peak in PRMDs among students studying in Year 2 compared to those studying in Year 1. This elevation remained throughout Year 3 before a significant decline was seen for students studying in Year 4 and 5 (Table 4).
Fisher analysis of PRMDs and year of study
Fisher analysis of PRMDs and year of study
Significant differences were identified between students in the different years of study (F(6,524) =4.92, p < 0.001). Post hoc comparisons indicated that the mean number of PRMDs of Year 1 music students (M = 0.64, SD = 1.21) was significantly lower than that of professional musicians (M = 1.24, SD = 1.59). The mean number of PRMDs of Year 2 music students (M = 1.00, SD = 1.44) was significantly higher than that of non-music students who play an instrument (M = 0.25, SD = 0.63). The mean number of PRMDs of Year 3 music students (M = 0.84, SD = 1.19) was also significantly higher than that of non-music students who play an instrument.
The role of age on PRMDs both longitudinally and between participant categories were examined. Participants within the 20–22 years-old range were found to have variation between participant categories, where music students and professional musicians were significantly more likely to have PRMDs. Longitudinally, no variation was observed among the music student and professional musician populations. In the non-music student population, participants in the 20–22-year-old age range had significantly lower prevalence of PRMDs compared to participants over the age of 23 (Table 5).
Fisher analysis of PRMDs and age
Fisher analysis of PRMDs and age
No significant variance was found in the number of PRMDs within the music student participants (F(3,380) = 2.15, p = 0.09) or among the professional musician participants (F(3,45) = 2.14, p =0.44) across age. In contrast, significant variance was identified among the non-music students who play an instrument across age (F(3,92) = 3.28, p = 0.02). However, post hoc comparisons found no significant difference among the subgroups.
Upon investigating the impact of gender on prevalence of PRMDs, no significant variations were found within each category of participants. Comparing the participant categories within each gender, female music students and professional musicians had a significantly higher prevalence of PRMDs compared to the control. As well, in both male and female participants, professional musicians had the highest prevalence for PRMDs, and non-music students who play an instrument had the lowest (Table 6).
Fisher analysis of PRMDs and gender
Fisher analysis of PRMDs and gender
Variance was found in the number of PRMD locations within the genders and in the different categories of participants (F(8,519) = 3.57, p < 0.001). Post hoc comparisons indicated that the mean number of PRMDs in female professional musicians (M = 1.14, SD = 1.48), female music students (M = 0.84, SD = 1.32), and male professional musicians (M = 1.42, SD = 1.81), were significantly higher than that in female non-music students who play an instrument (M = 0.19, SD = 0.64). The mean number of PRMDs of male professional musicians was also significantly higher than that of male non-music students who play an instrument (M = 0.66, SD = 0.60).
Correlation between sub-specialty program of study and the prevalence of PRMDs were also investigated. Certain programs –namely, faculty program, music education, piano performance, orchestral performance, and jazz performance –were found to have a significantly elevated prevalence of PRMDs among their students. Alternatively, students in certain programs, such as music theory, early music voice performance, and organ/harpsichord performance, reported no PRMDs (Table 7). Significant differences were also observed in the number of PRMD locations between the various subspecialty programs of study (F(14,518) = 3.10, p < 0.001). Post hoc comparisons found the mean number of PRMDs within the students of the piano performance program (M = 1.12, SD = 1.53) and the jazz performance program (M = 1.15, SD = 1.56) were significantly higher than that of non-music students who play an instrument (M = 0.25, SD = 0.63).
Fisher analysis of PRMDs and program of study
Fisher analysis of PRMDs and program of study
The role of playing specific instruments correlating to the prevalence of PRMDs was analyzed. Music students who play instruments such as cello/double bass, piano, woodwinds, brass, percussion, and guitar were found to have a higher prevalence of PRMDs. Professional musicians who played piano and woodwinds were associated with increased prevalence of PRMDs, as well. No difference between professional musicians and music students who played the same instruments were observed (Table 8). The differences in the number of PRMD locations based on the participant’s choice of instrument were also compared. Significant variance was found between different instruments and different participant categories (F(24,507) = 2.01, p = 0.003). Post hoc comparisons, however, found no significant difference between the groups.
Fisher analysis of PRMDs and instrument played
Fisher analysis of PRMDs and instrument played
Physical injuries are detrimental to any musician’s career. There has been a trend to refer injured musicians to sports medicine specialists, due to the popular belief that the mechanisms of injury share a common cause [25]. Educators, who often have the most exposure with musicians and music students, should play an essential role in prevention and management [26]. Unfortunately, the institutional barriers that prevent musicians from accessing preventative medicine, or taking time off for injuries when they need, only accentuates this problem [27, 28].
This study found music students to not only have a higher prevalence of performance-related injuries, but also to have more locations of PRMDs compared to non-music students who play an instrument. It also found professional musicians to have a higher prevalence and more locations of PRMDs than those of music students. The results did not find age, practice durations, or consulting healthcare professionals to correlate with these findings. Furthermore, these findings address the specific lack of data regarding playing duration, different instrument groups, and longitudinal components as noted in a recent systematic review [2].
Surprisingly, we found no correlation within the music student population between practice duration and PRMDs, which had been indirectly suggested in previous studies [29–31]. With no prior standardized studies to serve as comparison [2], it is unclear why the observations differ. However, we believe that due to our larger sample size, our findings were less likely influenced by additional biases. It is possible that as musicians become injured, they opt to practice less, resulting in artificially elevated rates of PRMD prevalence. We also could not exclude the possibility that with shorter practice durations, music may have a therapeutic effect in non-music students. Nevertheless, we see a similar trend within the professional musician group where no correlation was found between practice duration and PRMDs. This leads us to believe that practice duration does not contribute towards PRMDs, but may in fact be limited by PRMDs themselves.
We observed music students within the age of 20–22-year-old to have a high prevalence of PRMDs. This age range corresponds well to being enrolled in Years 2 and 3 of study, in which we also observe a higher prevalence and number of PRMDs. Given that a similar trend was not observed within our other cohorts, we concluded here that age does not have a significant contribution towards playing-related injuries. We do, however, note a significant rise in PRMD prevalence between music students in their last year of study and professional musicians. No prior literature has investigated the longitudinal trend of PRMDs [2], making this a novel observation which requires additional exploration regarding the accumulation of injuries during the transition to becoming a music student, as well as the transition from being a music student to a professional musician.
This study observed participants of the female gender to have an increased likelihood of PRMDs. The literature in sports medicine found no differences in the incidence of injury between genders [32], though this had been previously observed by other researchers studying musicians [13, 19]. Here, we can simply postulate that there may be some contributing physiological [33], societal, or environment differences associated with the female gender, and that the types of musculoskeletal activity performed by a musician induces injury through mechanisms which are different from those in sports.
The study also found that the number of PRMDs and the prevalence associated with playing certain instruments did not correspond to the subspecialty program in which the music student participants are enrolled. While studies have investigated the role of playing certain instruments in developing PRMDs [34], our findings highlight the need to investigate further into psychological and environmental factors [35].
We do believe our physical health questions adapted from the NMQ demonstrates the need for a standardized and validated assessment tool to assess for physical injuries. The 3 major improvements we had made upon the questions addressed injuries that would otherwise not have been picked up by the NMQ, because it was never designed for the purpose of assessing for PRMDs [18]. It neglects or fails to elucidate injuries such as those to the ears or vocal cords. Furthermore, as highlighted in the lack of longitudinal assessment of physical injury of musicians [2], there is a need to investigate beyond the scope of 12 months constrained by the NMQ. Lastly, the inclusion criteria of the NMQ are inconsistent with the definition of PRMDs, a definition which is commonplace in literature regarding the physical health of musicians. Therefore, we believe our physical health survey questions based upon the NMQ framework is better suited for future studies of PRMDs of musicians and music students.
Limitations
Of note, our research was designed to understand the physical injury status of music students and to identify certain unmodifiable and modifiable factors that may be correlated. Though our findings do not elucidate the finer details of the mechanisms associated with these factors, they do highlight their contribution and the need for further investigation.
Conclusions
To our knowledge, this is the first study to investigate the health of music students and musicians in a comprehensive manner which encompasses multiple facets of health, as well as to try to identify unmodifiable and modifiable factors that may predispose musicians to physical injury. Moreover, we believe this to be the first study to investigate differences between professional musicians, post-secondary music students, and non-music students. It also fulfills a gap previously identified in literature [2] regarding the impact of practice duration on PRMDs and progressions longitudinally. While we may have identified risk factors which predispose a musician or music student to PRMDs, additional research is required to truly clarify the mechanisms behind how they result in injury. The findings also suggest that musicians’ PRMDs are perhaps unique and should be managed within the healthcare system differently from what is done in sports medicine, particularly regarding the impact of practicing on injury; it is essential not to generalize physical injuries as simply occupational hazards and suggest the avoidance of practicing and/or performing. We have also adapted the NMQ into a survey which we believe is more tailored for future research of PRMDs. Our findings on physical health are only one component of our research to understand musicians’ health as a whole, and it is likely that additional factors such as the presence of mental health issues and medication usage may be contributory as well. Most importantly, we hope the findings encourage educators and healthcare professionals alike to foster an environment for musicians and music students in which discussions of injuries are no longer discouraged, and where personalized treatments allow for long and successful careers [10, 37].
Footnotes
Acknowledgments
We thank the students at McGill University’s Schulich School of Music and all other participating musicians, collaborating professors (Dr. Jacqueline Leclair, Dr. Jerry Cain, Dr. Shawn Mativetsky, Dr. Helene Boucher, Maestro Alexis Hauser) for allowing us to survey their students, members of the Schulich Musicians’ Health committee (Alexia Hlynialuk, Madeline Weber, Alexa Dumont), other students (Renee Brechtel), and Orchestra Canada for their assistance in acquisition of data, Peter Hung for assistance in statistical analysis, and Claire Motyer for assistance in concept and design. Special thanks to Dr. Jacqueline Leclair and Dr. Ann Wechsler for supervising the project and proofreading the manuscript.
Author contributions
A.Y. Chang and H. Boone had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Concept and design: Chang, Boone; Acquisition, analysis, or interpretation of data: Chang, Boone; Drafting of the manuscript: Chang; Critical revision of the manuscript for important intellectual content: All authors; Statistical analysis: Chang; Supervision: Gold.
Conflict of interest
The authors have no conflict of interest to report.