
Abstract
BACKGROUND:
Individuals fluent in sign language (signers) born to non-signing, non-deaf parents (non-natives) may have a greater injury risk than signers born to signing, deaf parents (natives). A comprehensive analysis of movement while signing in natives and non-natives has not been completed and could provide insight into the greater injury prevalence of non-natives.
OBJECTIVE:
The objective of this study was to determine differences in upper extremity biomechanics between non-natives and natives.
METHODS:
Strength, ‘micro’ rests, muscle activation, ballistic signing, joint angle, and work envelope were captured across groups.
RESULTS:
Non-natives had fewer rests (p = 0.002) and greater activation (p = 0.008) in non-dominant upper trapezius. For ballistic signing, natives had greater anterior-posterior jerk (p = 0.033) and for joint angle, natives demonstrated greater wrist flexion-extension range of motion (p = 0.040). Natives also demonstrated greater maximum medial-lateral (p = 0.015), and greater minimum medial-lateral (p = 0.019) and superior-inferior (p = 0.027) positions.
CONCLUSIONS:
We observed that natives presented with more rests and less activation, but greater ballistic tendencies, joint angle, and envelope compared to non-natives. Additional work should explore potential links between these outcomes and injury risk in signers.
Introduction
Over 30%of sign language interpreters are physically injured on the job with 57%of injuries from repetitive motion [1]. Demand for interpreters is anticipated to grow 20%by 2029 [2], suggesting higher numbers will suffer from musculoskeletal pain. Preserving the health and reducing injury in those who use their upper extremities (UEs) to communicate is not only paramount for the wellbeing and livelihood of interpreters, but also for deaf and non-deaf individuals fluent in sign language (signers). Signers who have at least one signing, deaf parent are considered natives [3] and are an overlooked demographic [4]. Most signers are born to non-signing, non-deaf parents and are considered non-natives. Musculoskeletal pain from signing is more common from non-natives than natives. Sixty-seven percent of non-natives report UE pain with 46%experiencing pain for six months to one year and 17%from one to five years compared to 0%of natives [5]. The reasons underpinning this risk disparity are unclear.
Little work has examined the specific contribution of UE biomechanics to the high percent of musculoskeletal pain in signers [6–9]. Feuerstein and Fitzgerald [10] performed a study that informed a text on cumulative trauma disorders [11]. In that work, they identified several factors unique to the biomechanics of signers (Table 1). Further quantification using more current instrumentation is needed to generalize these findings to the signing population.
Biomechanical considerations unique to signers [10]
Biomechanical considerations unique to signers [10]
Previous literature assessing the biomechanics of signers is sparse with inconsistent methods and participant groupings. Ratings of frequency and scale [10], biaxial unilateral/bilateral electrogoniometers [13–16], an electromagnetic motion capture system [17], and electromyography (EMG) [13, 18] have all been used to measure a variety of biomechanical parameters in signers. Some work has shown no difference between early- and late-signing interpreters [14, 16], while other work demonstrated that novice interpreters had increased ‘micro’ breaks and reduced velocity compared to experienced interpreters [17], and interpreters had greater percent pause when conversing compared to deaf students [15]. Prior research has helped to reach a foundational basis for these biomechanical considerations; however, it lacks standardization and has yet to reach a consensus, limiting practical application.
The goal of this work was to examine UE biomechanics in natives and non-natives while signing. Specifically, we sought to quantify strength, ‘micro’ rests, muscle tension, ballistic signing, joint angle, and work envelope. It was hypothesized that non-natives will have reduced strength, fewer rests, and greater tension, ballistic tendencies, non-neutral joint position and envelope, indicating less favorable biomechanics, compared to natives.
This study was approved by the Institutional Review Board at Arizona State University (STUDY00003832). All participants voluntarily provided written informed consent to participate.
Participants
Fifteen self-reported non-natives and 10 self-reported natives were studied (Table 2). Sample size calculations were based on acceleration, the identified primary risk factor associated with cumulative trauma disorder [19]. Power analysis (power = 0.80; α= 0.05) using GPower 3.1.9.2 software (Dusseldorf, Germany) from Qin et al. [20] provided group differences in left wrist flexion-extension acceleration. A large (0.8) effect size would achieve significance with an estimated 22 total participants, therefore 25 were recruited.
Participant demographics (n = 25)
Participant demographics (n = 25)
Notes: At least one RID certification was required from all non-deaf participants. Acceptable certifications included: Comprehensive Skills Certificate, Certificate of Transliteration, Certificate of Interpreting, National Interpreter Certification, Educational Certificate: K-12 with≥level four on the Educational Interpreter Performance Assessment, or a Specialist Certificate: Legal or Performing Arts.
All participants were healthy, deaf or non-deaf adults aged ≥18 years. Sign language fluency of non-deaf participants was measured using Registry of Interpreters for the Deaf (RID) standards [21]. Primary use of sign language for communication since birth, or during primary or secondary education equated to fluency for deaf participants. While formal RID certification for deaf participants was not required, one participant was a Certified Deaf Interpreter and two others were preparing to become certified. Exclusion criteria included those enrolled in interpreter preparatory programs, with pacemakers, who were pregnant, and/or diagnosed with a neuromuscular disorder.
Isometric joint moment was used to assess strength and measured with a Humac Norm isokinetic dynamometer (CSMI, Stoughton, MA, USA). Measurements were taken in standard postures: supine for shoulder internal-external rotation, sitting for shoulder abduction-adduction and flexion-extension, and sitting for wrist flexion-extension and radial-ulnar deviation [22]. A hydraulic hand dynamometer (Jamar, Hatfield, PA, USA) was used to measure grip strength. Three five second trials were performed bilaterally for each test; one minute of rest was given between trials and two minutes of rest were given between tests to offset fatigue [23].
Participants converted three trials of a seven-minute video source showing a deaf community leader sharing her experience during a historical protest movement into their own sign language. The video had closed captioning and audio overlay to ensure accessibility for all participants. At least five minutes of rest were given between trials. A 16-channel, wireless Noraxon DTS system (Noraxon, Scottsdale, AZ, USA) was used to measure surface EMG. Measures were acquired bilaterally from upper/middle trapezius, anterior/middle deltoid, and wrist flexion-extension and radial-ulnar deviation muscle groups at 1000 Hz. Prior to data collection, maximal voluntary contractions (MVC) were acquired from each muscle using postures that elicit maximal activity [24].
An eight Kestrel camera motion capture system (Motion Analysis, Santa Rosa, CA, USA) tracked the three-dimensional (3D) location (x: medial-lateral; y: anterior-posterior; z: superior-inferior) of 9 mm reflective surface markers on UE segments while signing. Prior to testing, a static recording was obtained for marker definition. A total of 23 markers were placed bilaterally on the second/fifth metacarpophalangeal (MCP) joints, radial/ulnar styloids, medial/lateral epicondyles, posterolateral acromions, sternoclavicular joints, seventh cervical vertebra spinous process, xiphoid process, anterior midpoint of the forearms/proximal UEs, and an offset marker on the left posterior shoulder [25]. Participant involvement was complete at the end of a single five-hour testing session.
Data processing
Strength was quantified by identifying the maximum joint moment maintained for ≥0.5 seconds during each trial with a custom MATLAB (MathWorks, Natick, MA, USA) script [22]. Hand strength was identified as the maximum grip strength value across the three trials.
Since an induced training effect was intended, surface EMG data from the first minute of the third trial were analyzed. Raw EMG signals were band-pass filtered from 10–490 Hz with a fourth order Butterworth filter, rectified, and enveloped using a second order low-pass Butterworth filter with 6 Hz cutoff frequency via a custom MATLAB program. Signals were normalized by each muscle’s corresponding MVC. ‘Micro’ rests were defined as a temporal delay ≥0.257 seconds between sequential signs with activation < 18%MVC [13, 26] and signified as the total percentage of time in rest (%rest). Mean muscle activation represented muscle tension (%MVC).
The first minute of motion capture from the third trial was post-processed using Cortex software (Motion Analysis, Santa Rosa, CA, USA). Motion capture data were low-pass filtered at 5 Hz with a fourth-order Butterworth filter, then used to quantify ballistic signing and envelope. Absolute maximum resultant instantaneous linear acceleration of the dominant hand while signing ‘again’ (Fig. 1a) was the primary outcome for ballistic signing. Segment force (using anthropometry) [27] and jerk served as secondary outcomes. ‘Again’ was analyzed because the contact force between hands allowed for easy observation of ballistic tendencies. Work envelope was represented by the boundary of hand movement (Fig. 1c) and calculated by the absolute value of the maximum minus minimum linear motion of the relative difference between the dominant second MCP joint and ipsilateral acromion markers. Average position, 2D (medial-lateral by superior-inferior) area, and 3D volume were calculated as secondary outcomes for envelope. The C3D model builder module of the Motion Monitor software (Innovative Sports Training, Chicago, IL, USA) assessed wrist flexion-extension and radial-ulnar deviation for joint angle. Specifically, maximum, minimum, and average wrist position while signing ‘principal’ (Fig. 1b). ‘Principal’ allowed for easy observation of gross deviations from neutral wrist. Positive values indicated wrist flexion and ulnar deviation, and negative values indicated wrist extension and radial deviation. The maximum minus the minimum wrist position represented range of motion (ROM). Average wrist flexion-extension position and ROM served as the primary outcomes for joint angle. The maximum and minimum positions, and average wrist radial-ulnar deviation position and ROM were secondary outcomes.
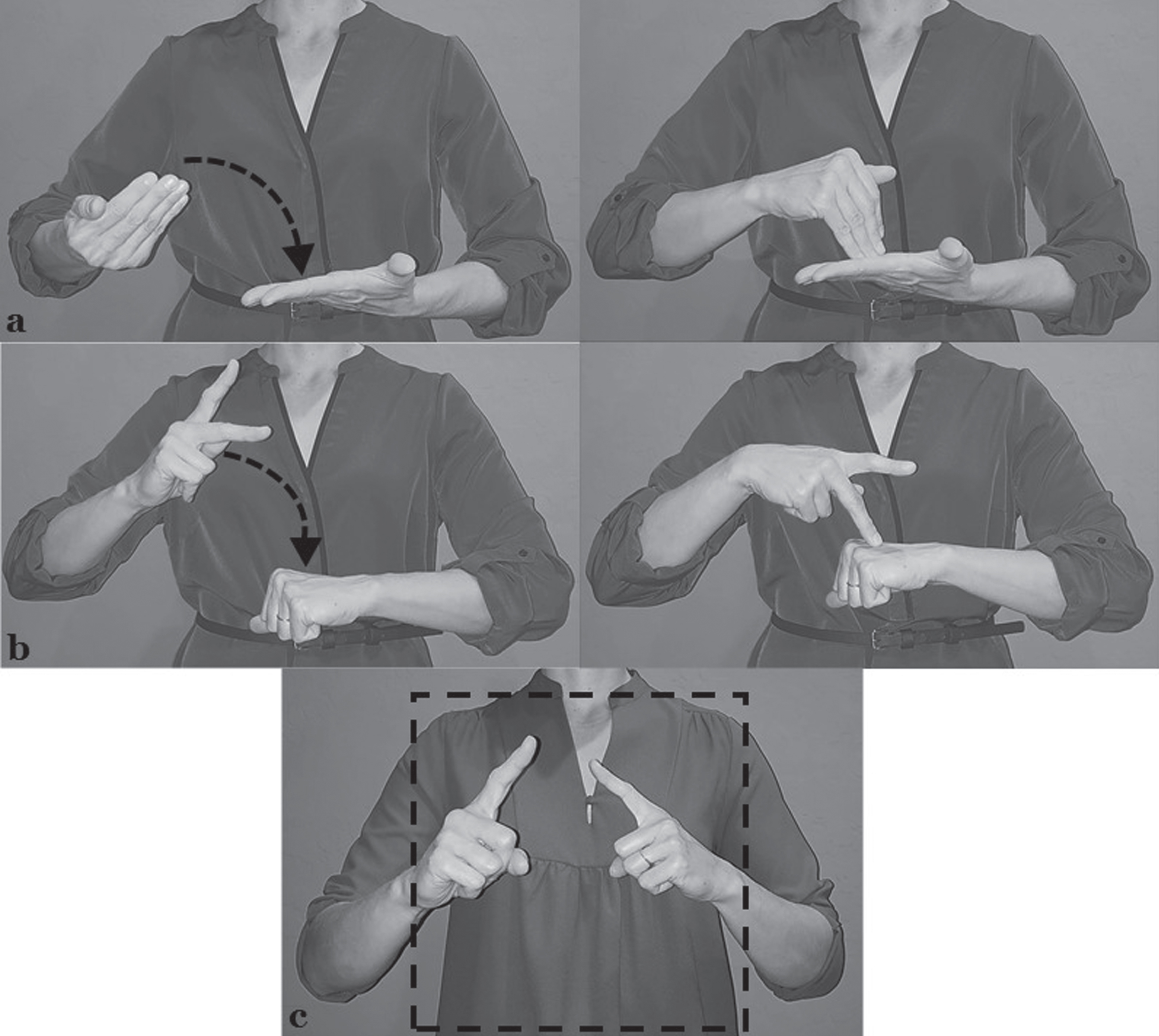
a) Sign for ‘again.’ b) Sign for ‘principal’. c) Visualization of work envelope.
Separate Mann-Whitney U tests evaluated differences between groups for strength, rest, and activation. Outcomes were examined for dominant and non-dominant sides. A custom MATLAB code was used to perform a false discovery rate correction and control for type I errors across the multiple comparisons [28].
Upon achieving normality assumption, analysis of covariance (ANCOVA) via a univariate general linear model was used to separately analyze the outcomes across groups representing ballistic signing, joint angle, and envelope, while adjusting for the covariates of gender, age, hearing status, and handedness. Chi-square tests evaluated differences in the covariates (Table 2). Using the output from ANCOVA, secondary analyses of hearing status and handedness were also performed. All statistical analyses were performed using SPSS (IBM, Armonk, NY, USA), with significance defined as p < 0.05.
Results
Strength, rest, and activation were measured between groups. There were no significant differences in shoulder and wrist strength (p≥0.220). Natives had more ‘micro’ rests (p = 0.016; Fig. 2a) and less muscle activation (p = 0.016; Fig. 2b) for non-dominant upper trapezius. The variability of muscle activation was greatly impacted by one participant who presented with non-physiological values that could not be corrected for by filtering; therefore, rest and activation are presented without this outlier.
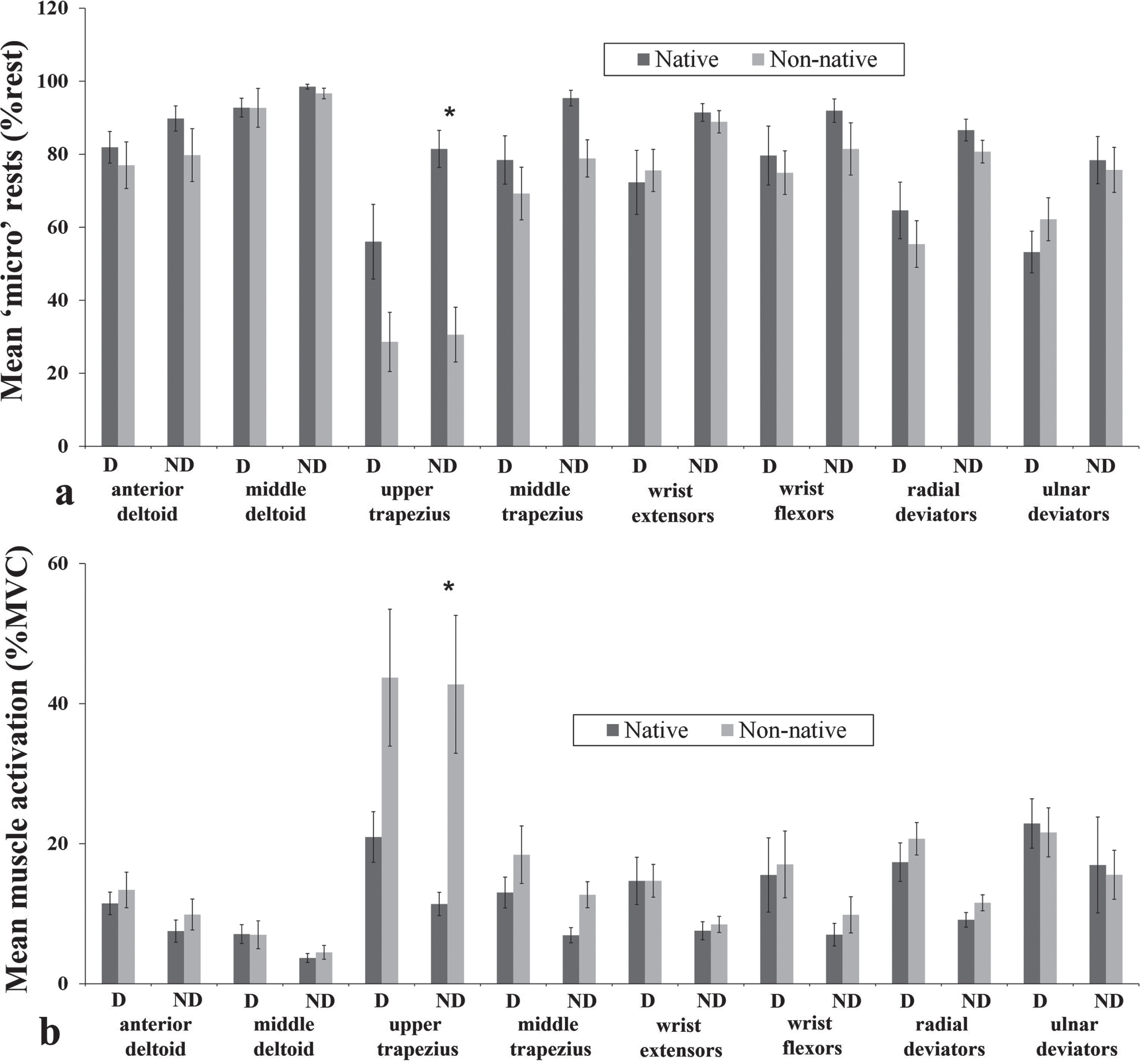
Mean (±SE) dominant (D) and non-dominant (ND) shoulder and wrist a) ‘micro’ rests and b) muscle activation for natives and non-natives over the first minute of the trial.
For ballistic signing, no differences were found in the resultant (p = 0.200) nor along the three dimensions (p≥0.051) for maximum resultant instantaneous linear acceleration and in the resultant (p = 0.310) nor along the three dimensions (p≥0.168) for segment force. Natives demonstrated greater anterior-posterior jerk (p = 0.033) when signing ‘again.’ Secondary analyses demonstrated that non-deaf participants had greater anterior-posterior acceleration, anterior-posterior jerk and resultant jerk (p≤0.015) than deaf, and left-handed participants had greater anterior-posterior jerk than right-handed (p = 0.047).
When considering joint angle during ‘principal,’ natives had greater wrist flexion-extension ROM (p = 0.040; Fig. 3a). There were no differences in radial-ulnar deviation ROM (p = 0.070; Fig. 3a), or average wrist position (p≥0.526; Fig. 3b). Secondary analyses revealed deaf participants had greater wrist ROM and greater minimum wrist flexion-extension position (p≤0.023) than non-deaf.

a) Mean (±SE) wrist flexion-extension and radial-ulnar deviation range of motion and b) average wrist joint position for natives and non-natives while signing ‘principal.’
The dimensions captured for 2D work envelope were greater when compared to the 25 cm2 recommended norm (Table 3). Natives had a greater maximum medial-lateral, and greater minimum medial-lateral and superior-inferior positions (p≤0.027). Natives (35.80±1.36 cm) also had a slightly larger superior-inferior envelope than non-natives (30.84±2.09 cm; p = 0.051), although this difference did not reach statistical significance. Secondary analyses revealed right-handed participants had a greater superior-inferior envelope, and greater maximum medial-lateral and anterior-posterior positions (p≤0.024), and left-handed participants had a greater minimum medial-lateral position (p = 0.009). For 2D area, natives and non-natives were, respectively, 240%and 128%greater than the recommended 625 cm2 norm. There were no differences between groups in 2D area and 3D volume (p≥0.059).
Mean (±SE) relative work envelope for non-natives and natives
Notes: *p < 0.050.
The goal of this work was to quantify strength, rest, activation, ballistic signing, joint angle, and envelope in natives and non-natives while signing. It was hypothesized that non-natives would have less favorable biomechanics. The lack of difference in strength did not support this hypothesis, however, was consistent with past literature. Feuerstein and Fitzgerald [10] studied endurance of interpreters with and without pain and found no differences. Others [29] found assembly workers with lateral epicondylitis demonstrated greater muscle activity ratios suggesting that overuse injuries in industry and signers may be attributed to muscle activity imbalance rather than strength deficits. In support of this study’s hypothesis, non-natives had fewer rests and greater activation. Interpreters with pain had fewer rest breaks than interpreters without pain [10]. Comparisons can be made, respectively, between this study’s ‘micro’ rests for non-natives and natives with the rest frequency for interpreters with and without pain. Both non-natives in this work and interpreters with pain rested less. Contrary to our findings, novice interpreters had increased ‘micro’ breaks during a latter time increment when interpreting, which was attributed to fatigue [17, 30]. All novice interpreters were children of non-deaf parents, which is comparable to this study’s non-natives. Feuerstein and Fitzgerald [10] used a visual analog scale to measure muscle tension (zero = no tension; 10 = overt tension). Unfortunately, muscle tension was not included in their analysis because of poor interrater reliability; therefore, no comparable findings for this work are available.
In opposition to this study’s hypothesis, natives had greater ballistic tendencies, joint angle, and envelope. Slower velocity of novice compared to experienced interpreters was also attributed to fatigue [17, 30]. Experienced interpreters trended toward greater velocity, which was consistent with this study’s findings. Feuerstein and Fitzgerald [10] found interpreters with pain had more rapid movements. Fewer ballistic tendencies in non-natives was contrary to the greater pace measured in interpreters with pain. Experienced interpreters increased their elbow ROM over time [17]. Natives in this study and experienced interpreters had increased ROM in comparison to non-natives and novice interpreters, respectively. When comparing wrist displacement between interpreters and deaf students conversing [15], deaf students demonstrated greater displacement. Natives in this work, experienced interpreters, and deaf students all demonstrated greater UE motion. This contrasted with the greater hand/wrist deviations in interpreters with pain [10]. The recommended envelope for signers was based on seated workspace specifications [31]. Data for the current study were gathered in standing; therefore, use of these values should help inform standing 2D and 3D envelope norms for signers. Contrary to our findings, interpreters with pain demonstrated greater excursions than interpreters without pain [10]. Greater envelope measurements in natives are inconsistent with the greater excursions of interpreters with pain. Greater jerk and ROM in natives may provide greater effectiveness when signing and therefore, be a counterintuitive response to ward against injury risk. There is some thought that a larger envelope is safer because it relies more on the larger shoulder/elbow muscles, rather than the smaller wrist/hand muscles. Indeed, we found greater dominant middle deltoid activation was associated with greater 2D area and 3D volume. Because pain is more common from non-natives than natives, the association of less favorable biomechanics with greater ballistic tendencies, joint angle, and envelope may need to be re-considered.
Secondary analyses of hearing status and handedness offered additional insight. The significance across deaf and non-deaf for ballistic signing and joint angle questions whether hearing status, rather than language acquisition, is better able to distinguish the biomechanics indicative of injury risk. The presenter in the video was right-handed and this may have factored into the increased jerk of this study’s left-handed participants. The greater minimum medial-lateral position for left-handed and greater maximum medial-lateral position for right-handed participants are clear, as someone who is left-handed is more apt to make greater movements on the left, while a right-handed individual makes greater movements on the right side of the body. Past evidence does not convey any significant findings when comparing handedness, so these findings, like muscle activation, are unsubstantiated in signers.
There were a few limitations to this study. The cross-sectional design limits our ability to detect causation. When comparing the calculated EMG results across the entire trial with the first minute, there were no differences; therefore, rest, activation, and envelope were quantified for the first minute. Ballistic signing and joint angle were assessed using a single representative sign. Future work may consider assessing all measurements across the same period. The current work was the first to calculate jerk in signers, although the linear calculations limit its comparability with the angular calculations of others. This study was powered to detect wrist acceleration as the primary outcome for ballistic signing, thus other analyses may be underpowered. These data can now power future studies exploring similar factors. Investigators used RID certification to ascertain language fluency for non-deaf participants, but no standard assessment determined fluency for deaf. In the future, use of the American Sign Language Proficiency Interview [32] should be considered with all participants.
Conclusion
This study provides a more complete description of UE biomechanics in natives and non-natives and will help inform the development of a composite measure of injury risk specific to signers [33]. The greater ballistic tendencies, joint angle, and work envelope exhibited by natives are in opposition to conventional thinking. More evidence is needed to be conclusive, hence this study motivates ongoing work to more fully explore potential links between the biomechanics unique to signers and injury.
Footnotes
Acknowledgments
The authors thank Thurmon E. Lockhart, PhD, CPE in the School of Biological and Health Systems Engineering and Pamela D. Swan, PhD, FACSM, FTOS in the College of Health Solutions at Arizona State University for their insights toward this work.
Conflict of interest
None to report.
Funding
The project described in this publication was supported by start-up funding (Vidt) from Arizona State University, an Academy of Physical Therapy Education Adopt-a-Doc Scholarship (Roman) from the American Physical Therapy Association, and the University of Rochester CTSA award number TL1 TR002000 (Roman) from the National Center for Advancing Translational Sciences of the National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.