
Abstract
BACKGROUND:
Validation studies have not been able to confirm the stage-specific understanding as operationalised in the readiness for return to work (RRTW) questionnaire.
OBJECTIVE:
To explore retrospectively how working female cancer survivors experienced the process of becoming ready to RTW during and beyond participation in an occupational rehabilitation intervention and thereby expand the understanding of the RRTW construct.
METHODS:
A qualitative research design was employed. Thirteen female cancer survivors were included for semi-structured interviews one to two years after they had completed active treatment and returned to work. The RRTW construct guided data generation and analysis. Content analysis was performed in four analytical steps that combined a concept-driven and a data-driven analytic strategy.
RESULTS:
Three themes were identified; “To have and then lose the safety net”, “Realise a changed life situation”, “Strive to balance work and everyday life”. In a time span of approximately one to two years (from receiving treatment, being enrolled in an intervention and to gradually returning to work); the identified themes were interdependent of each other as one theme gradually evolved to the next theme in the process of engaging in sustained work participation.
CONCLUSIONS:
The present study points towards continuous development of the RRTW construct and whether the addition of a preparedness dimension would improve validity.
Introduction
Return to work (RTW) after cancer treatment is reported as an ambiguous process related to a variety of social and psychology-, physical health-, structure-, and economy-related factors [1, 2]. Cancer survivors (CSs) often suffer from long-term side effects from treatment, and late effects may occur even months or years after treatment has ended [3, 4]. Consequently, the RTW processes are influenced negatively as is the readiness of the CS to embrace everyday life [5, 6]. Female survivors experience more adverse work outcomes than male survivors [7, 8]. Although the scientific literature demonstrates that female CSs mentally begin to prepare their RTW as soon as they have finished treatment [1, 6], the incentives of the CSs are often counteracted by vulnerability and uncertainty about their RTW [9]. CSs’ experiences of RTW difficulties are suggested to be best assisted by addressing work readiness [10].
The readiness for RTW construct
The process by which individuals become ready to engage in returning to work can be viewed as a progression through stages of change; from pre-contemplation (not intending RTW), contemplation (considering RTW), preparation (planning to RTW), and action (gradual RTW) to uncertain maintenance (staying at work) and proactive maintenance (staying at work in a sustainable manner) [11, 12]. These series of stages were conceptualised in the readiness for RTW (RRTW) questionnaire [12]. It has been proposed that the RRTW questionnaire could enable occupational rehabilitation professionals to detect rehabilitation needs and guide them in the provision of tailored interventions by matching the stage-specific needs of the individual worker to different types of intervention elements [10]. Recent studies [13–15] however, including a Danish validation study [16], found difficulties in confirming the stage-specific understanding as operationalised in the RRTW questionnaire [11].
Municipal RTW intervention
The Danish Sickness Benefit Act applies to everyone on sick leave and municipal social security offices are responsible for initiating and providing occupational rehabilitation to support sick-listed people, including cancer patients in their RTW process [17]. The maximum period a sick-listed employee can receive sickness benefit payments is 22 weeks. With some exceptions, sickness benefit may be prolonged. Occupational rehabilitation services during cancer treatment are not standard municipal procedure, and hospitals devote even less attention to patients’ everyday life including work [18]. Employers are responsible for paying wages to sick-listed employees in the initial 30 days of a sick leave. If the sick leave exceeds 30 days, the employer will get reimbursement from the state as from day 30 and until the employee returns to work, the employment contract ends voluntarily or involuntarily, or the maximum sickness benefit period (22 weeks) ends or cannot be prolonged. Hence, in a legal sense, employers’ financial responsibility for the RTW process applies only to the first 30 days of a sick leave where they have to bear the cost of the employee’s absence. RTW is a collaborative effort where municipal social workers (SW) in the social security offices support employees to RTW.
In a RTW intervention [19], municipal SWs used the RRTW questionnaire to identify stage-specific needs and guided them in the provision of the RTW support offered to CSs. In Fig. 1, a timeline of the intervention and its elements are shown together with the timing of this study. The RTW intervention took place parallel to cancer treatment given at the hospital and continued for a maximum of one year [19]. The SWs were specifically trained in Acceptance and Commitment Therapy [20], which enabled them to communicate in a way that committed the CSs to RTW goals. From a theoretical point of view, that would motivate and ultimately fuel the progression in RRTW [12].
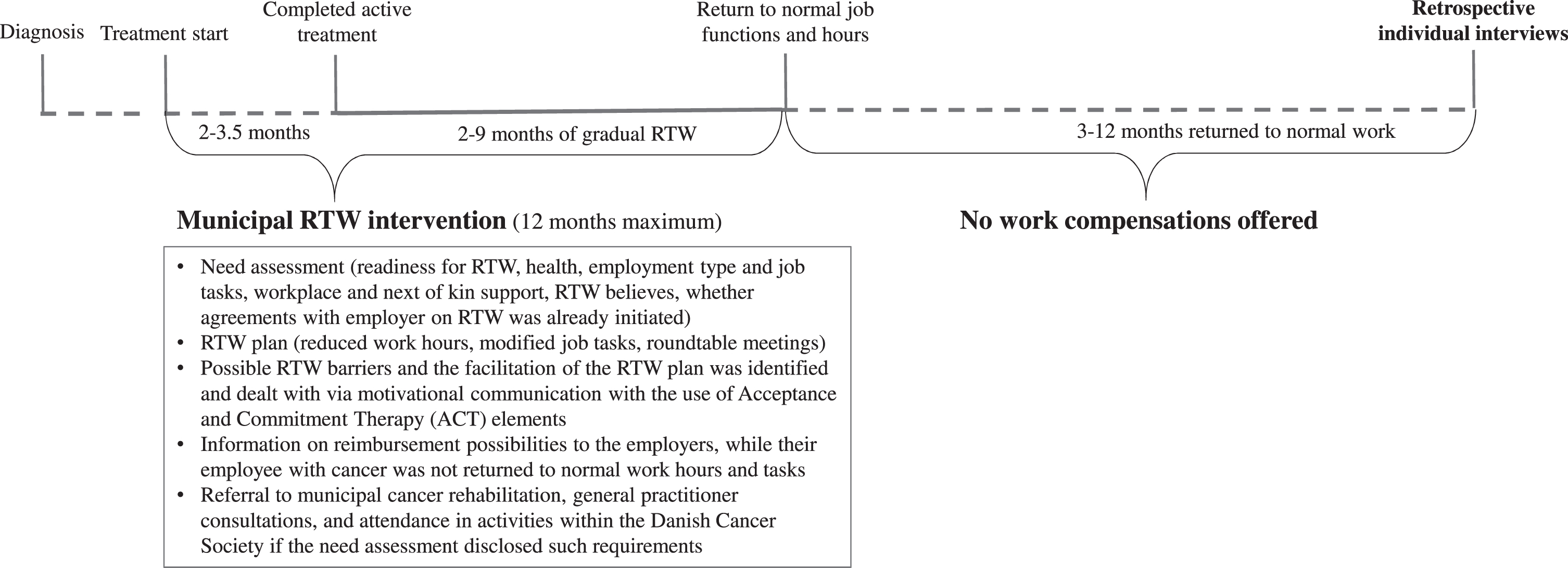
Timeline of the return to work (RTW) intervention and timing of the study.
As the current structure of the RRTW questionnaire appears not to be able to capture the RRTW construct as specific stages [13, 16]; further stage-specific understanding of the RRTW construct is needed. This understanding may in return provide ideas on how the structural validity of the RRTW questionnaire could be improved.
The purpose of this study was to explore retrospectively how working female CSs experienced the process of becoming ready to RTW during and beyond participation in a RTW intervention and thereby expand the understanding of the RRTW construct.
Semi-structured individual interviews of female CSs one to two years after they had completed active cancer treatment and had returned to work were performed (Fig. 1).
Sampling and recruitment of participants.
A purposive sample strategy was applied [21]. Inclusion criteria were female CSs, previously enrolled in the municipal RTW intervention study [19], who had returned to work for at least three months, i.e. working full-time or part-time at the former or at a new workplace, and with no additional prolonged sick leave after their return. Thirteen female CSs were included (Table 1). One participant had started her education one year after her initial RTW; as this education encompassed practical training on a regular basis, she was still considered to have met the inclusion criteria. Four female CSs were invited, but declined and three did not respond. ‘Information power’ regarding study purpose, sample specificity, theory use, quality of the dialogue, and the chosen analytic strategy guided the determination of sample size [22].
Characteristics of the study participants
Characteristics of the study participants
The RRTW construct [11, 12] provided a theoretical frame and guided data generation and analysis. The construct is based on the Stages of Change Model [23] and the Phase Model of Occupational Disability [12, 24]. According to these models, the worker is claimed to be influenced by three individual psychological dimensions when making conscious decisions about RRTW: decisional balance, self-efficacy, and change processes. This is operationalised in the RRTW questionnaire, which aims to capture a person’s progression through stages of behavioural change [11].
Data generation
From January to March 2018, 13 individual interviews were performed by the first author (n = 6) and the second author (n = 7). Each interview was between 60–90 minutes. The interview guide was structured in accordance with the six stages in the RRTW questionnaire [11, 12], and guided generation of interview questions together with themes identified in previous reviews on factors influencing the RTW process [7, 25–29]. The interview was initiated with questions related to: cause of cancer and treatment, functioning, physical and mental health, social support, municipal rehabilitation. Then questions related to the six stages of the RRTW construct were brought into play and supplemented with factors from the RTW literature deemed relevant based on the study purpose. These six stages and accompanying factors were: 1) Pre-contemplation and job function; 2) Contemplation and motivation; 3) Preparation for action; 4) Action and attitude; 5) Uncertain maintenance and work-related fears, job demands, workability, working environment, support from colleagues and employer and communication and support from the municipality; 6) Proactive maintenance. To enable participants to express their experiences of their RRTW process, open-ended and follow-up questions were asked [30]. The interviews took place in the participants’ homes, at their work places, or at a local setting according to individual preferences. All the interviews were audiotaped and transcribed verbatim. The first two interviews were discussed in the research team (all authors) in order to qualify the interview guide.
Data analysis
Schreier’s approach to content analysis was followed [31]. The first and second author carried out the analysis as a joint interactive coding process with ongoing discussions of the content and patterns as they arose from the analysis. Findings were discussed with the research team. The content analysis was performed in four analytical steps, combing a concept-driven and a data-driven analytic strategy [31].
Step 1: Concept-driven coding frame was composed (as shown in Fig. 2), by drawing on the study aim, the RRTW construct, and results from previous systematic reviews on the RTW process [7, 25–29]. The transcribed interviews were read and followed by a preliminary sorting into the concept-driven categories by use of the NviVo software programme.
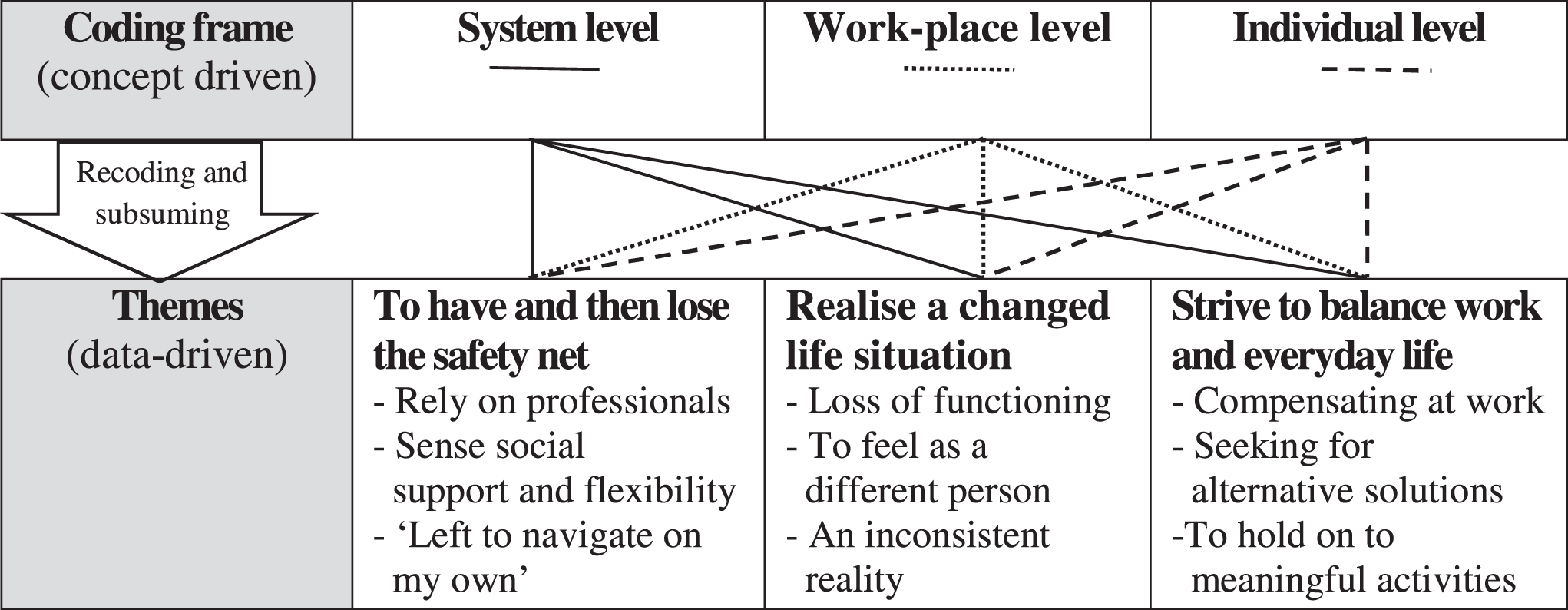
Concept-driven and data-driven analytic process and themes and subthemes identified.
Step 2: Data-driven analysis was carried out based on the preliminary sorting of the data material, with attention to the meaning and relations appearing within the data material. Because of the complexity and differentiated circumstances of participants’ RTW process, the data-driven analysis indicated themes appearing across the concept-driven coding frame as illustrated in Fig. 2.
Step 3: The coding frame was revised according to the identified data-driven themes. The data material was recoded through a process of subsuming and creating new data-driven themes and underlying subthemes to capture the essence of the participants’ experiences of their RRTW process. Hand-mapping was used to strengthen the data-driven analysis and prevent losing sight of important segments.
Step 4: The writing-up process helped identify patterns and connections between the identified themes.
Based on the analysis, three themes were identified: “To have and then lose the safety net”, “Realise a changed life situation”, “Strive to balance work and everyday life”. The themes were interdependent of each other, as one theme gradually evolved to the next theme in the process of engaging in sustained work participation.
To have and then lose the safety net
This theme represents the participants’ experiences of the professional, social, and structural support provided during their RTW process and the way it affected their RRTW over time. The safety net consisted of support from the health care system during cancer treatment, support from SWs during the municipal RTW intervention, and support from employers and colleagues.
While undergoing treatment, the CSs relied on the health care professionals based on their expert medical knowledge. The participants explained the treatment period as “holding on to a running train”; all they had to do was to hang on to and follow the provided plan. Likewise, the participants relied on the support provided by the SWs from the intervention. It encompassed dealing with legislations, ensuring legal rights, mental support, and assisting the RTW plan.
“ . . . it was comfortable to talk with her . I was also worried about how long I could be sick-listed, and whether I was going to get fired and all that. She told me that I didn’t need to worry. Also, she took part in meetings and she was my supporter if I had problems with my employer. I always knew I had her on my side.” (ID 10)
The SW appeared to be a vital part of the experienced safety net of the participants. Based on the participants’ situation, the SWs either gently pushed them to initiate RTW or advised them to spend more time to get ready for RTW. Not all participants made use of the support at their disposal. However, the accessibility to SW support seemed to positively influence the participants’ RRTW.
To be aware of social support and flexibility from the workplace appeared an integral part of the safety net as well. Support from employer and colleagues while still sick-listed made the participants feel appreciated and valued. Work arrangements with reduced hours and responsibilities helped participants to adjust to their changed life situation. The Sickness Benefit Act helped to achieve the reduction in work hours by the provision of economic compensation to the workplace. The support seemed to strengthen the social attachment to the workplace and functioned as a motivational factor for the participants’ RRTW.
When treatment ended, the participants experienced that the support from the health care system, SWs, employer, and colleagues gradually diminished, which left the participants feeling on their own. The participants soon had to increase the amount of work hours and were expected to return to normal job functions, while still dealing with health-related problems.
“You feel left alone. The hospital has let go of you. And of course, they have to at some point, but it is also a very insecure situation. And then you are back to work, and suddenly you must manage your normal working hours, okay? This is just overwhelming.” (ID 3)
To lose the safety net appeared as a fundamental issue that negatively influenced the participants‘ RRTW. The participants explained that their unmet needs for support gradually made them realise their changed life situation.
Realise a changed life situation
Loss of physical, mental, cognitive, and/or social functioning was commonly reported among the participants and affected their workability, i.e. need for extensive planning, depending on colleagues, and avoiding stressful work tasks. The flexible work arrangements provided, as part of the gradual RTW, discontinued when normal work hours were resumed even though the challenges persisted. Additionally, physical and mental health problems were widely reported and left most participants with little energy for engaging in meaningful activities other than work, which had a negative effect on RRTW experiences.
The participants expressed that they had to deal with an inconsistent reality. Even though they had gone through a process of realising their changed life situation, work demands, structural conditions, and social life remained the same and the participants felt they still had to live up to pre-cancer expectations from their surroundings.
“I think that most people can, especially during the treatment, understand that you feel bad. But how bad you actually feel, and how much it is affecting you in the long run, I don’t think anyone can imagine.” (ID 5)
These conflicting demands seemed to negatively influence and challenge the experienced readiness of the participants for a sustained work attachment. Thereby, the process after the RTW intervention and the gradual RTW, without the needed support from the safety net, was experienced as a striving to balance work and everyday life.
Strive to balance work and everyday life
The participants explained that their loss of functioning caused them to compensate at work and deprioritise their personal and social life. The participants carefully explained that they constantly tested what worked best for them in the current situation to find new meaning in their changed life situation. During gradual RTW, participants managed to engage in meaningful activities, besides work, which helped balance work and everyday life and positively affected their RRTW.
“I actually started riding. I have always wanted to ride and when our son was going to horse riding and had done so for several years, I was so fascinated by it –then my husband said isn’t it now you have to start . . . then I thought that if death have to have a reason then you may as well die happy.” (ID 1)
Nevertheless, when normal work hours and tasks were resumed most of the participants described that they used all their energy at work and felt exhausted when they got home. The lack of energy and fragility forced the participants to have a day-to-day approach, which may have affected their readiness for a sustained RTW. The progression in work activity meant that most participants tried to seek alternative solutions, which appeared as a common strategy in striving to balance work and everyday life. Most of them expressed a wish for part time jobs, but found it impracticable because of their financial situation.
“I think, if I only could –and this I have felt before and I have thought about this especially now with my heart condition –if I had the opportunity, I would like to have fewer work hours so I didn't have all these long days with night hours and weekend arrangements . . . I have thought of contacting my union to hear if they see any possibilities. Especially now when I have got heart problems, I feel a lot of pressure.” (ID10)
Lack of confidence in finding and managing a new job stopped most of the participants from pursuing other options.
The experienced changes and ongoing struggles seemed to be balanced through engagement in meaningful activities, thereby influencing their RRTW positively. However, the constant work pressure and unaltered demands from the workplace seemed to slowly tip the energy scale at the expense of their family and social life. This progression created a downwards spiral and affected the sustained RRTW of the participants.
Discussion
Sufficient support, expressed by participants as a safety net, acted as a catalyst in the progression through stages of behavioural change towards RTW. When this safety net of professional support diminished over time, it became clear that it was a struggle to balance private and work life. The participants exhausted themselves to meet work demands, which was at the expense of engagement in spare time activities. The unmet needs for support as time went by prevented the participants of feeling able to stay at work in a sustainable way.
To break the trend of increased risk of adverse work outcomes in CSs, new RTW strategies have been called for [32, 33]. It has been suggested that CSs’ RTW difficulties are best dealt with by addressing work readiness [12]. Access to validated instruments that enable identification of, in many cases complex, occupational rehabilitation needs are thus in demand.
However, the structural validity of the RRTW questionnaire has not been confirmed [13, 16]. The RRTW construct may, thus, consist of not yet discovered dimensions that are not part of the RRTW questionnaire in its current form. The participants explained that the support offered by the safety net, significantly influenced their RRTW. For instance, provision of reduced work hours and modified work tasks had compensated for their loss of functioning during their gradual RTW. The experienced loss in functioning corresponds to previous studies on CSs’ vulnerability regarding RTW following cancer treatment [1, 34]. Thus, the elements encompassed in the RTW intervention [19] seemed to address work disability needs and were perceived to be important by the participants with regard to their eventual RTW. However, when normal work hours and tasks were resumed, the accomplished work readiness was compromised, as the SW support stopped and yet another piece of the safety net was gone. From that point in time, the participants expressed a steady decline in their work readiness. Uncertainty dominated their thoughts as they were left to manage on their own with no access to support or alternative solutions. That seems to be a general experience, also among CSs not involved in a RTW intervention [35, 36]. The findings of this study indicate that along with early professional support, there is a need for continuous health and work-related support in the years following treatment to enable those affected by cancer to maintain employment.
Along with gradually facing a changed life situation with decreased functioning and work ability, the participants also realised that these changes were not sufficiently recognised among their private and professional relations. The work places were not prepared for a continued need of support in order to prevent the participants from relapsing into lower RRTW stages. This is a common issue [37, 38], as many employers do not realise that a significant proportion of CSs have impaired work ability when they RTW. Thus, the preparedness of the work place may be just as important as the readiness of the individual. This is in agreement with previous findings [12] in which the preparedness of the work place is suggested to be as prioritised as the work environment to facilitate the progression of the CSs’ levels of work functioning. Facilitating preparedness may display challenges as the work place arena has multiple demands to accommodate. In a previous study [39], both employers and co-workers were motivated to provide gradual RTW with fewer work hours and less demanding work tasks. However, if the increased workload and work accommodations went on for an extended period of time, the patience of co-workers and employers was stretched, and it became a burden to maintain a supportive work environment [39].
A few of the interviewed CS expressed a wish for not returning to work; but for economic reasons, this was not an option. In a French study [40], income was not considered an important factor in the RTW decision. Instead, issues related to 1) meaning of work had changed, 2) career plans were reconsidered or 3) the RTW process was expected to inflict problems; were found to affect the CS’s decision. Although it was concluded that such reasons should be accepted from CSs who wanted to deselect paid work despite sustained work ability [40], the generous Nordic welfare scheme is in opposition to this point of view. The right to health-related benefits, such as early retirement, presupposes that those whose work ability is not permanently reduced should resume work.
Methodological considerations
Data were generated retrospectively, which represented both strengths and limitations. The retrospective view enabled insights into the participants’ experiences as they had evolved over time. However, the retrospective design may have been influenced by potential recall pitfalls [41]. More interviews in a longitudinal study design over the RTW process could have strengthened the immediate experiences of the females at specific transitions, i.e. the initial work resumption on reduced work hours and work accommodations, the end of the intervention, and the transition to full-time work etc. Nevertheless, considering the recurrence and patterns occurring across participants’ experiences, the retrospective design did not appear restrictive. Applying a structured interview guide ensured focused data generation, which addressed the unconfirmed RRTW construct validity [13, 16]. This approach may limit attainment of participant-driven data and the ability to capture subjective experiences [30]. Therefore, to ensure the relevance of the questions asked, we conferred with an external female CS who represented the ‘lived experience’. As a result, questions about mental and physical late effects and cooperation with employer and employees during and beyond RTW were integrated.
A content analysis approach was pursued [31]. However, a linear link between the concept-driven and a data-driven analysis could not be drawn and further developed (Fig. 2). Thus, the concept-driven coding frame showed not to be directly applicable with regard to answering the study purpose and maintaining loyalty towards the data material. It may have limited the stringency of the analytic approach. Nevertheless, to assure the credibility and trustworthiness of data, the coding frame was revised to capture the essence of the CSs’ experiences (Fig. 2).
The majority of the participants were breast CSs, who represent a relative homogeneous group. Breast cancer is overrepresented in the research field of CSs [1, 34], which may cause limited attention to the challenges perceived by other CSs. Additionally, the sample represented a relatively and socio-economically strong group. Although, by considering the challenges experienced by the participants of this study, one may assume that CSs with low socio-economic status may face even bigger challenges than described in the present study [42].
Despite a homogeneous sample, we consider the results transferrable to similar settings because; late effects [25], decreased workability [9], and restrictive legislations [43] are commonly reported issues. Only female CSs were included in this study; parallels to males should be drawn cautiously, as gender differences have been identified [44].
The exploration of the process of becoming ready to RTW during and beyond participation in a RTW intervention, expanded our understanding of the RRTW construct. However, these new insights may not be directly transferrable to practice. Rather, new stage-specific understandings of the RRTW questionnaire were obtained, that point towards a refocus on the long-term sustained RTW challenges. Future research should explore preparedness of the workplaces at which long-term sick-listed employees are to return to.
Conclusion
The present study points towards continuous development of the RRTW construct and whether the addition of a preparedness dimension would improve validity. Further qualitative studies are needed in order to explore whether the preparedness concept is also present in other CSs, including men, and if so, to what extent preparedness is dependent on the type of workplace and work tasks the CSs return to.
Author contributions
KSP, ML and CMS conceived the study idea. All authors contributed in the design of the study. KSP and LSM performed independently interviews and analyses. All authors were engaged in the interpretation, discussion of results and drafting of the manuscript. All authors have read and approved the submitted manuscript.
Conflict of interest
The authors have no conflict of interest to report.
Ethical approval
All procedures followed were in accordance with the ethical standards of the responsible committees on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Approval for the use of questionnaire data was obtained from the Central Region Denmark (Danish Data Protection Agency j. no. 1.16-02-657-14). Oral and written information about the study aim was given to the participants and written consent was obtained before the interview from all individual participants included in the study.
Funding
The study was funded by the Danish Cancer Society [R-73-A4736], Central Denmark Region [1-31-72-6-13], and the Danish Health Foundation [2014B056].