
Abstract
BACKGROUND:
A prerequisite for interpreting electromyography (EMG) data is to normalize them to a maximum voluntary contraction (MVC), expressing them as percentage of the MVC.
OBJECTIVE:
The objective of this study was to compare different recommended MVC exercises for the latissimus dorsi and identify the exercise that elicits the highest EMG amplitude.
METHODS:
Fifteen male participants were recruited. Five recommended MVC exercises were investigated, including chest-supported shoulder extension, prone shoulder extension, lat-pull down, abducted shoulder flexion, and internal shoulder rotation.
RESULTS:
Chest-supported shoulder extension reported the highest mean EMG, which was not significantly different from the mean EMG of prone shoulder extension. Both of these exercises led to significantly greater EMG means than the other exercises. Sixty percent of the participants achieved their highest EMG amplitude with chest-supported shoulder extension and 40% with prone shoulder extension. None of the other exercises elicited the highest EMG amplitude in any of the participants.
CONCLUSIONS:
Both chest-supported shoulder extension and prone shoulder extension proved to be effective MVC exercises, with the former showing more consistency in eliciting the highest EMG amplitude. If the true MVC is desired, the authors recommend performing both exercises and then using the overall highest EMG amplitude for normalization purposes.
Introduction
Surface electromyography (EMG) has been used extensively in the ergonomics literature to assess biomechanical loads during physical tasks, in order to investigate the causes of work-related musculoskeletal disorders (WMSD) and propose interventions. One common condition for analyzing and interpreting EMG data is to normalize them to a reference contraction [1–3], with the most popular being the maximum voluntary contraction (MVC) [4–6]. This technique is favored, especially in ergonomics, for its physiological relevance, in that it translates EMG data from a bioelectrical variable (micro- or milli-volts) into a biomechanical variable (% MVC) [5, 8]. It expresses the EMG results as a percentage of the muscle’s MVC, providing information about the activation level of a muscle relative to its maximal physical capacity [9–12]. However, a major challenge with this technique is selecting an appropriate exercise that truly elicits the muscle’s MVC. If an inaccurate MVC is used, then the normalized EMG signals may at times exceed 100% MVC, incorrectly implying that the muscle is active beyond its maximum physical capacity [5, 13]. In such cases, the MVC will actually be operating as a sub-maximal voluntary contraction (sub-MVC), diminishing the inherent advantage of the MVC method. Therefore, it is essential that an accurate MVC is selected for normalization, in order to maintain the physiological benefit of this method.
This research explored different recommended MVC exercises specifically for the latissimus dorsi muscle. This muscle was of particular interest because it serves as both a back and shoulder muscle [14], two of the most affected body regions by WMSDs. Together, they accounted for over 50% of all WMSDs in 2016 [15]. Furthermore, the latissimus dorsi is the largest muscle on the back, connecting the spine to the humerus and occupying the majority of the lower posterior thorax [16, 17]. It is responsible for shoulder movements, such as medial (internal) rotation, adduction, and extension of the shoulder joint, and it also participates in back movements, such as rotation, lateral flexion, and extension of the spine [14]. Given its functions, this muscle has frequently been employed in ergonomics research for examining WMSDs of the shoulder and back [14, 17].
The literature presented different recommended MVC exercises for the latissimus dorsi, lacking a consensus on the most appropriate MVC. Beaudette et al. [18] examined four MVC exercises and concluded that the most effective MVC to be chest-supported shoulder extension (or chest-supported row). Prone shoulder extension (or humeral extension) also performed relatively well as an MVC for the latissimus dorsi, in that it was not significantly different from chest-supported shoulder extension [18]. Konrad [19], on the other hand, recommended a lat-pull down as the MVC for this muscle, which mimics a pull-up action. Furthermore, the lat-pull down in another study by Park and Yoo [13] was shown not to differ significantly from prone shoulder extension in eliciting the highest EMG amplitude of the latissimus dorsi. Findings of Boettcher et al. [20] supported completely different MVC exercises for this muscle, which included abducted shoulder flexion (or internal rotation 90°) and internal shoulder rotation (or internal rotation 0°).
The lack of consensus on the MVC for the latissimus dorsi is largely due to the fact that previous research investigated different sets of MVC exercises and therefore had different recommendations. A more comprehensive research that examines the different recommended MVC exercises with respect to one another is needed. Therefore, the purpose of this study was to test and compare the recommended MVC exercises of the latissimus dorsi and identify the MVC that elicits the highest EMG amplitude for this muscle.
Methods
Participants
Fifteen healthy university-aged male participants were recruited for this study. An orientation to the experimental procedures was provided to the participants, and their signatures were obtained on informed consent forms approved by the Institutional Review Board (IRB). The Physical Activity Readiness Questionnaire (PAR-Q, British Columbia Ministry of Health) was used to screen participants for cardiac and other health problems, such as dizziness, chest pain, or heart trouble [21]. Any participant who answered “yes” to any of the questions on the PAR-Q was excluded from the experiment. The average age, weight, and height of the participants were 20.8 years, 75.6 kg, and 179.4 cm, respectively.
Equipment
Raw EMG signals were collected using a Tringo wireless EMG system (Delsys Inc., Boston, MA, USA). The surface EMG electrode was a Trigno sensor (Delsys) with a single differential configuration, a parallel bar (99.9% pure silver) contact area, and a fixed inter-electrode distance of 10 mm. It was set at a band-pass filter of 20–450 Hz and a common mode rejection ratio of 80 dB. Data was collected at a sampling rate of 2000 Hz and processed using the root mean square method with a time window of 0.125 s and an overlap of 0.0625 s [3, 19]. The EMGworks software (Delsys Inc., Boston, MA, USA) was utilized for processing and analyzing the collected data. Also, an electrically-adjustable therapy table (55 cm×190 cm) was used to facilitate the performance of the MVC exercises.
Experimental procedures
Participants were provided with an orientation, which introduced them to the purpose of this research, the equipment, the data collection procedures, and the specifics of the experimental tasks. They began with a warm-up session for three minutes consisting of different stretches for the joints involved. The EMG electrode was then attached to the latissimus dorsi, 4 cm below the inferior tip of the scapula and midway between the spine and lateral edge of the torso [14]. Figure 1 shows the electrode site on the latissimus dorsi, as adapted from Criswell [14]. The skin was prepared before attaching the electrode by shaving the area over the muscle site and cleaning it with alcohol. Next, participants performed five different MVC exercises that were identified in the literature to elicit high EMG amplitudes from the latissimus dorsi. These exercises included the following:
Chest-supported shoulder extension (Fig. 2a): this exercise began in a standing position and a flexed back with the chest supported on an examination table. Then shoulder extension was performed against manual resistance at the elbow [18]. Abducted shoulder flexion (Fig. 2b): this exercise began with the shoulder abducted 90° and the elbow flexed 90°, with the arm parallel to the ground. Participants then performed shoulder flexion against manual resistance at the wrist [20]. Internal shoulder rotation (Fig. 2c): this exercise began with arms at the sides and the elbow flexed at 90°. Then participants rotated their shoulder inward against manual resistance at the wrist [20]. Lat-pull down (Fig. 2d): this exercise began in a seated position with the participant grabbing onto a fixed horizontal bar overhead (shoulders abducted 90° and elbows flexed 90°). Participants then attempted to pull down the bar, as the experimenter stabilized them with manual resistance over the shoulders [13, 19]. Prone shoulder extension (Fig. 2e): this exercise began in the prone position on an examination table with arms at the sides and palms facing upwards. Then shoulder extension was performed against manual resistance at the elbow [13].
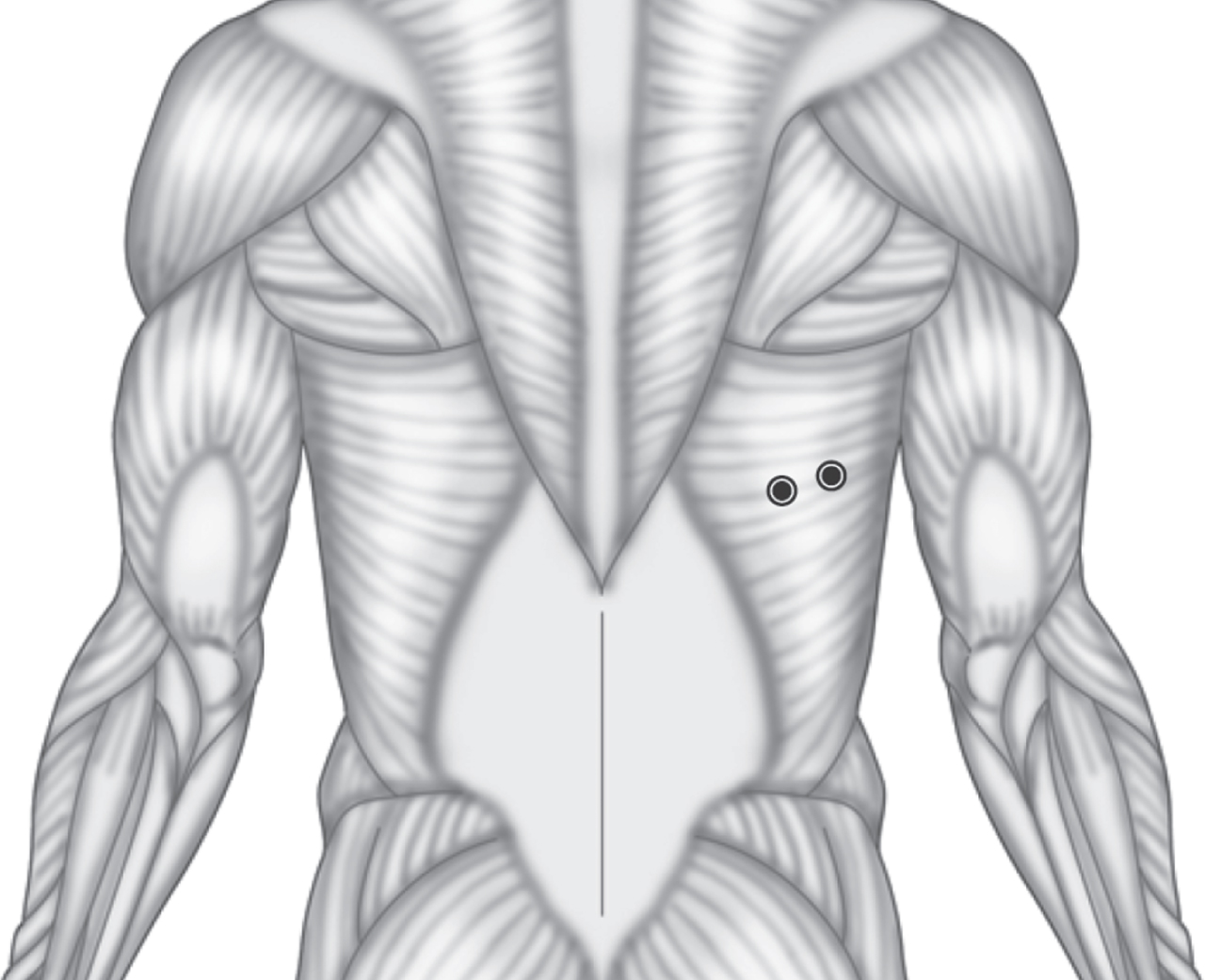
EMG electrode site on the latissimus dorsi. Adapted from Criswell [14].

Pictures of the MVC exercises for the latissimus dorsi muscle: (a) chest-supported shoulder extension; (b) abducted shoulder flexion; (c) internal shoulder rotation; (d) lat-pull down; (e) prone shoulder extension; the white arrows represent the forces of the participant, and the gray arrows represent the resistance of the experimenter.
Participants were trained on each exercise before data collection to ensure correct performance. Clear instructions were given to them to perform maximum contractions. They were asked to gradually exert up to their maximal force in 3 to 5 s, hold it for 3 s, and gradually decrease the force in 3 s [19]. However, EMG data was collected for a slightly longer time period (15 s) to avoid rushing participants and the examiner in performing the MVC exercises. Since the maximum EMG signals were the only measures of interest, this increased duration did not affect the analysis. The order of exercise presentation was randomized among the participants. Three repetitions were performed per exercise, and the average of the maximum EMG signals was computed. For each participant, the MVC exercise associated with the highest average was used as a reference to normalize EMG data [6, 13]; that is, EMG data were expressed as a percentage of each participant’s true MVC (% MVC). Repetitions per exercise were separated with 30 to 60 s of rest, and the different MVC exercises were separated with 2 minutes of rest [19].
A repeated measures, one-way analysis of variance (ANOVA) was used to assess the effects of the MVC exercises on the latissimus dorsi’s maximum activation capacity. The independent variable in this study was the MVC exercise, which consisted of five levels. The dependent variable was the maximum, normalized EMG amplitude of the latissimus dorsi. The experiment consisted of 15 trials, accounting for three repetitions per exercise. Post-hoc pairwise comparisons were performed using the Tukey test to determine the source(s) of the significant effect. A significance level (α) of 5% was used.
Results
Figure 3 presents the EMG means associated with each of the five MVC exercises for the latissimus dorsi. The ANOVA results showed a statistically significant difference between EMG means with a p-value < 0.001. The post-hoc pairwise comparisons are summarized in the form of letter groupings as shown in Fig. 3. MVC exercises sharing the same letter grouping indicated that they were not significantly different from each other (p > 0.05); whereas, exercises with different letter groupings suggested a statistically significant difference in EMG means (p < 0.05). Chest-supported shoulder extension was associated with the highest EMG mean, and prone shoulder extension was not significantly different. Both of these exercises achieved significantly higher EMG means than the other three exercises. The lowest EMG mean, on the other hand, was associated with abducted shoulder flexion, which was not significantly different from the lat-pull down exercise. Table 1 shows the number and percentage of times each MVC exercise elicited the highest EMG amplitude among the fifteen participants. All participants attained their highest EMG activity in either chest supported shoulder extension or prone shoulder extension (60% and 40% of participants, respectively). None of the other three exercises elicited the highest EMG amplitude in any of the participants.

Mean EMG amplitudes (% MVC) with standard error bars of the MVC exercises for the latissimus dorsi (CSE = chest-supported shoulder extension; ASF = abducted shoulder flexion; ISR = internal shoulder rotation; LPD = lat-pull down; PSE = prone shoulder extension); means that do not share the same letter grouping are significantly different from each other.
The number and percentage of times each exercise elicited the highest EMG amplitude in the latissimus dorsi among all participants
This research compared five recommended MVC exercises for the latissimus dorsi muscle, in order to determine the overall most effective exercise(s) in eliciting this muscle’s MVC. The findings favored chest-supported shoulder extension and prone shoulder extension as MVC exercises, with the former slightly performing better (Fig. 3 and Table 1). The effectiveness of chest-supported shoulder extension as an MVC for the latissimus dorsi is supported by Beaudette et al. [18], who also found that it did not differ significantly from prone shoulder extension. The latter exercise also proved to be effective by Park and Yoo [13]. Both of these exercises in the present study were associated with significantly greater EMG activities than the other investigated exercises. A couple of studies have supported the effectiveness of internal shoulder rotation and abducted shoulder flexion as MVC exercises for the latissimus dorsi [20, 22]; however, these studies did not compare them with neither chest-supported shoulder extension nor prone shoulder extension. The lat-pull down test did not perform as well as its superiors in eliciting MVC. Unlike the results of the present study, Park and Yoo’s [13] showed that the lat-pull down did not differ significantly from prone shoulder extension. Yet, Beaudette et al. [18] reported similar findings as the present study. As past research have suggested [5, 6], this study confirmed that there is no one exercise that will consistently achieve the highest EMG amplitude in all participants. Both the chest-supported shoulder extension and prone shoulder extension would have to be performed if the true or most accurate MVC is desired.
This research consisted of several limitations that may be explored further in future research. First, the findings of this study are limited to surface electrode EMG. Generalizing the findings herein to needle electrode EMG may be inaccurate. Second, a single electrode site was used to record the latissimus dorsi EMG. Using a different electrode site may lead to different results; however, this research considered a frequently adopted electrode site as recommended by Criswell [14]. Third, the study sample was limited to male participants, since they were required to be topless during the experiments. Fourth, the method followed in this study for generating MVCs was designed for healthy subjects with no musculoskeletal pain. Thus, the results of this work may not apply to individuals with musculoskeletal pain or dysfunction. In such cases, a sub-maximal voluntary contraction (sub-MVC) may be more appropriate and reliable as a reference contraction [23, 24]. Lastly, this research did not consider MVC exercises other than those published in the literature. There may be exercises that have not yet been developed that are even more effective in eliciting the MVC of the latissimus dorsi. For example, Al-Qaisi and Aghazadeh [25] proposed new MVC exercises, however, for two shoulder muscles, which they proved to be more effective than accepted MVC exercises in the literature. Similarly, in the case of the latissimus dorsi, there may be exercises that are even more effective than those already presented in the literature. For example, given that the latissimus dorsi is a shoulder and back muscle [14], a combination of actions that utilize the shoulder and spine (e.g. lateral flexion of the back and extension of the shoulder) may result in even greater EMG amplitudes.
Conclusions
This research investigated five different recommended MVC exercises in the literature for the latissimus dorsi muscle, in hopes of converging to one recommended MVC exercise. However, both chest-supported shoulder extension and prone shoulder extension proved to be effective MVC exercises. The former exercise was slightly favored more for eliciting the highest EMG amplitude in more participants (60% vs 40%). The authors do not recommend using any of the other three exercises as MVCs (i.e. abducted shoulder flexion, internal shoulder rotation, and lat-pull down), because none of them elicited the highest EMG amplitude in any of the participants. If the true MVC is desired – in order to maintain the physiological benefit of the MVC method – we recommend performing both chest-supported shoulder extension and prone shoulder extension and then using the overall highest EMG amplitude from both exercises for normalization purposes. However, if time is limited and the experimenter is restricted to using only one exercise, we recommend using chest-supported shoulder extension.
Footnotes
Acknowledgments
This study was made possible through generous support from the University Research Board at the American University of Beirut.
Conflict of interest
None to report.