
Abstract
BACKGROUND:
The aging of the workforce is changing, but working conditions have not changed at the same exponential growth rate for senior workers. Such a situation can compromise the worker’s physical and cognitive capability, reducing the ability to perform work activities.
OBJECTIVES:
This study aims to understand the main functional capacity changes in senior workers in the automotive industry and to determine the contribution of working conditions on the decline of the functional capacity in senior workers.
METHODS:
To achieve the objectives of the study, a set of questionnaires (Sociodemographic Data, COPSOQ, Nordic Questionnaire, and Par-Q) and a battery of 4 functional capacity tests were used. Results: Work conditions, namely awkward postures, force demands and manual material handling, and age, were statistically associated to the functional decline in workers. Additionally, multiple linear regression showed that height, weight, seniority, and strength have predictive value to the handgrip decline (both positions HG2 and HG5).
CONCLUSION:
These results suggest that workers’ handgrip assessment should be considered as a future measure as an indicator of strength ability in the occupational field.
Introduction
Demographics of the active workforce are changing rapidly, leading to a 50% increase in 45-year-old workers in industrialized countries. It is expected by 2060 that the older workers will reach 20% of the total active worker population [1, 2].
The aging workforces can overwhelm financial systems such as social security and healthcare services, and this can be due to aging-related syndromes like sarcopenia and frailty, and its early onset may occur due to an imbalance between the tasks demands and the functional capacity of the workers [2–4].
There are several areas of the economic sector where exposure to work remains the same for younger workers (18–40 years-old) and older workers (>40 years-old), such as the automotive industry. The automotive industry in Europe plays an essential role in the economy. In this industry, the car assembly process stands out. The assembly work is characterized by highly physical demands, namely those related to the static load, the repetitive task of the distal ends, unfavorable postures (such as operations carried out inside the car, with asymmetrical positions of the trunk, work with the shoulders above head level and so on) and strenuous activities [5, 41].
The functional capacity is usually assessed by a set of standardized tests performed on a worker, with or without disorders, in order to determine and understand the factors related to functional capacity and demands placed on the worker [2, 9].
Because of this scenario, it is essential to evaluate the functional capacity of workers associated with risk factors at work, to promote an adequate adjustment of demands with a functional capacity in different age groups, but with more significant concern for senior workers [6, 11].
The aims of this study are: (1) to verify the reliability of four functional capacity tests; (2) to analyze the association of working conditions and the workers’ functional capacity; and (3) to determine the magnitude of biomechanical and organizational factors in the functional decline of senior workers in an assembly line of the automotive industry.
Materials and methods
This study is divided into two phases. The first phase was dedicated to the evaluation of the reliability (test-retest) psychometric property of the four functional capacity tests, in a subsample of workers. In the second phase, it was performed the assessment of the functional capacity of workers and the work conditions of their workstations in the same production area.
All workers were informed about the purposes and procedures of the study and gave their informed written consent. The study protocol was approved by the Ethics Committee of Faculty of Human Kinetics, University of Lisbon.
Design and procedures
Phase 1 – Reliability test-retest
The reliability assessment was focused in the four following functional capacity tests, from the twelve battery test [3, 4]: Lifting Low (LL), Lifting High (LH), Overhead Working (OW) and Handgrip (HG) (described in item 2.2). Thus, a prospective design study was conducted, divided into two collection periods, with a interval of 3 days between moment one and moment two.
In this phase, characterized by the sample of indirect collaborators and considering 5% alpha error, 80% power, effect size 0.5, and 20% Physical Activity Readiness Questionnaire [12], the sample should be 30 participants [13]. From the initial sample, only twelve workers were considered eligible for participation in the study.
The choice of the four (4) functional capacity tests were supported considering the main activities performed on the assembly line, such as lifting loads, working with the arm above head level and using grip strength [5].
Phase 2 – Predictive factors of functional decline.
About 1000 workers were invited to participate in the study. Only healthy workers from the assembly area took part in this study. For the sample selection purposes, it was used the Par-Q [12] to guarantee that all workers were healthy.
From the 1000 employees who received the questionnaire, 121 returned unfilled, eight delivered without identification, 325 were considered ineligible for the test, and 500 were eligible. In the present study, workers were stratified by age and gender, where age was categorized by workers under 40 and workers over 40 years-old.
The final sample was composed of 147 workers, and the total duration of the study was 16 weeks. It was applied a randomization method to define the sequence of the tests.
The inclusion criteria were based on the age between 18–65 years; the exclusion criteria were defined as: 1– PAR-Q validated to Portuguese language [39]. Whenever participants had, at least, one positive question, they were excluded from the test [12]; 2– Blood Pressure higher than 159×99 mmHg, measured before the start of functional capacity assessment; 3– To have the initial heart rate above 100 bpm, before the assessment sections; 4– To have a medical restriction, prescribed by the occupational healthdepartment.
Procedures
The test procedures performed were the same in phases 1 and 2, except for the grip strength test. After the end of phase one, it was found in the assembly area, which workers sometimes made use of bad grip to handle parts or tools. Thus, the dynamometer position five was added in the grip strength test, since the position is considered as a bad grip [14].
Before starting the functional capacity tests, blood pressure and heart rate were measured [15], to verify at the moment of the test, if the worker was able to perform them. As a safety measure, a heart rate monitor was placed on the worker to monitor him during the tests.
After checking blood pressure and heart rate, the procedure of each functional capacity test was explained and demonstrated by the examiner. Then the worker was asked to perform a demonstration of the activity to see if he/she understood the procedure correctly [4].The worker was informed that any symptoms of discomfort (severe pain, shortness of breath, dizziness, and others) should be reported to the examiner and the test immediately interrupted [4].
Functional capacity testing procedures are based on the protocol of Isernhagen et al. [4] and Soer et al. [3]. For each functional capacity test, a 2-minute rest was given. The tests Lifting Low (LL), Lifting High (LH) and Overhead Working (OW) were performed in a system composed of a structure with a fixed vertical bar (250 cm in height) and another horizontal movable bar (70 cm in width and length), which allows adjustment in height.
-
-
-
In Fig. 1 shows the Lifting Low and High tests and the Overhead Working.
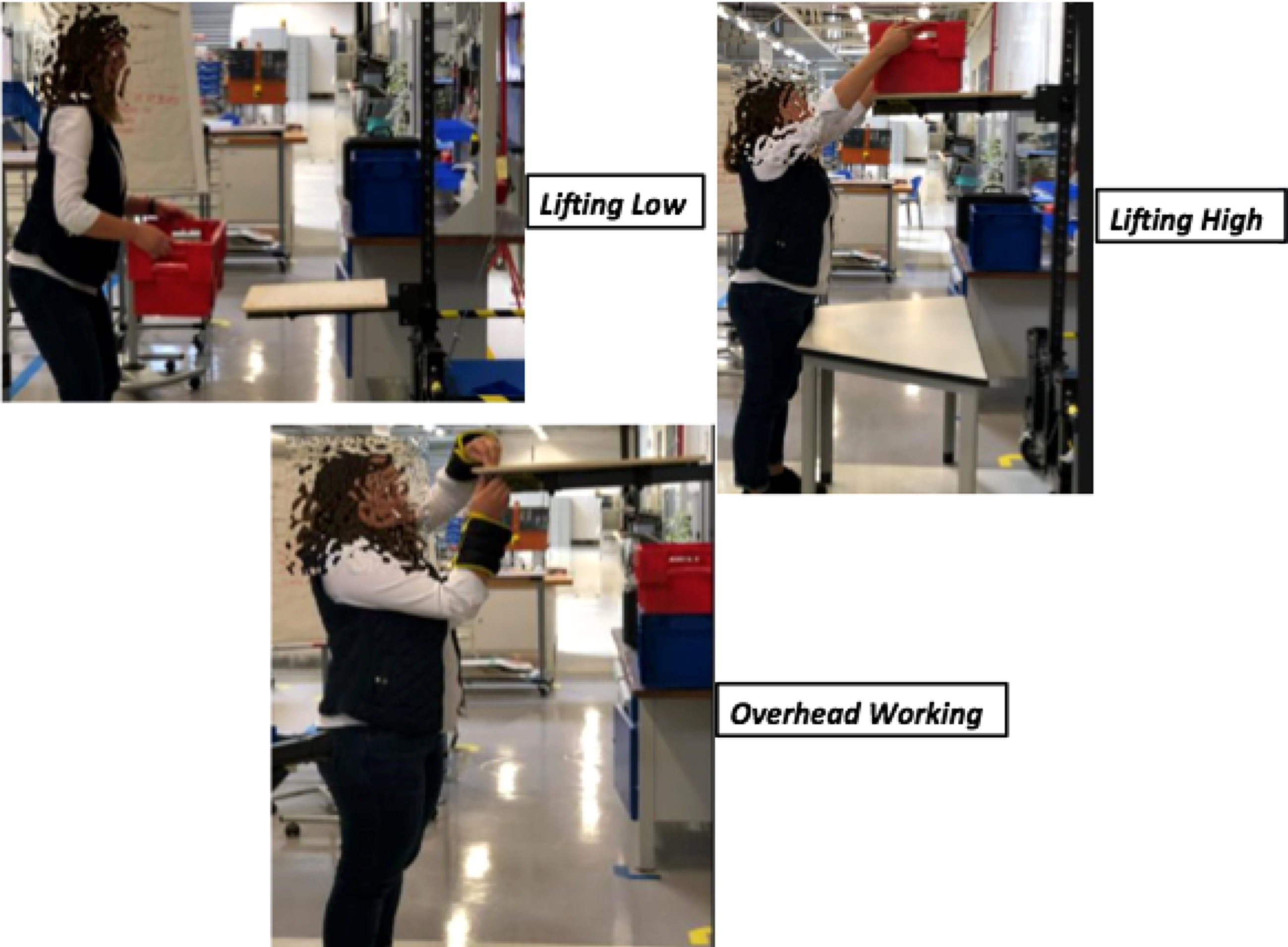
Examples of functional capacity test used in the study.
PAR-Q: This questionnaire has been widely used as a mean of screening individuals for the practice of physical activity (mild to moderate intensity level) [12]. The questionnaire covers 7 questions, dichotomous (Yes and No) related to cardiovascular problems (question 1 to 3 and 6), musculoskeletal problems (question 5) and pulmonary and metabolic disorders (questions 4 and 7) [12]. Sociodemographic Data, Health, and Life Habits questionnaire, aiming to collect data related to birth date, seniority in the work, gender, weight, height, health status (Hypertension, Diabetes, Exhaustion, and others). Copenhagen Psychosocial Questionnaire (COPSOQ): validated for the Portuguese language, was used to characterize the psychosocial factors of the population [16, 17]. Considering in the occupational context of the study, the following domains were questioned, in a total of 23 dimensions using the short version of the COPSOQ questionnaire: Quantitative requirements, Work Rhythm, Cognitive demands, Emotional demands, Influence on work, Possibility of development; Significance at Work; Commitment at work; Predictability; Transparency in work; Rewards; Social Support; Job satisfaction; Labor insecurity; Work / Family Conflict; Justice and respect; Quality of leadership; Social community at work; Job Satisfaction; General health; Self-efficacy; Stress; Burnout; Sleeping problems. All items were rated on a 5 point Likert scale (1 – Never / Almost Never, 2 – Rarely, 3 – Sometimes, 4 – Frequently and 5 – Always or 1 – Nothing / Almost Nothing, 2 – A Little, 3 Moderately, 4 – Very and 5 – Extremely) [17]. The Work Ability Index (WAI) analyzes whether or not the worker is fit for a certain type of work demands [18]. The structure of the questionnaire is divided into 7 dimensions, such as: work-related requirements, physical, mental, beyond worker’s health status and resources and points are awarded for each item [18, 19].
A study was carried out with 12389 workers between 40 and 65 years old, to verify if there were statistically significant differences, applying the entire WAI questionnaire or apply only the last question contained in the questionnaire. The last question is the score regarding the perception of the worker regarding his work ability (WAS), through a score ranging from 0 to 10, being 0 inability to work and 10 maximum capacity for work. [20]. As a result of the study, only WAS can be used as it was considered statistically significant (rs = 0.63;OR = 0.71, 95% CI 0.61–0.84) [20]. Therefore, the present study used WAS to verify workers’ perception of their ability to work.
Functional capacity evaluation (FCE), defined by the American Physical Therapy Association (APTA) is an “objective measure of an individual’s safe functional abilities, compared to work requirements”. The purpose of this tool is to evaluate the capacity of the worker in the work context. However, the same battery can be used in the context of rehabilitation to evaluate the best course of treatment and the evolution of the patient after the end of treatment [3, 21].
The actions that constitute the battery of tests of functional capacity are transport, push, hold, coordinate hands, climb, sit, walk, and others tasks [4]. The complete battery of the functional tests is composed of 12 tests [3, 4]. However, for the present study, it were selected four functional capacity tests based on the protocol elaborated by Isernhagen et al. and Soer et al. [3, 4]. In order to verify the handgrip strength, it was used the Jamar Smart Digital Hand Dynamometer, which is considered “gold-standard” to verify the handgrip strength and it is recommended by the American Association of Hand Therapists [14, 22]. For the evaluation was built a set-up with features of the automotive industry.
European Assembly Worksheet (EAWS). Data on the biomechanical risk factors of workstations was collected using ergonomic assessments by the European Assembly Worksheet method [7].
This tool of ergonomic analysis was originally used in the evaluation of the assembly work in the automotive industries. The EAWS was developed and implemented in a high number of automotive manufacturers and suppliers in Europe, mainly in Germany. These method considers 4 criteria’s: physiological and biomechanical factors, medical and epidemiological data, the psychological factor, and compliance with other international methods and standards. EAWS is a tool developed to evaluate the physical workload and has intensive training since it is a screening of complex elements [7].
EAWS includes of four assessment sessions: (a) Work Posture and additional movements of low physical effort (30–40 N or 3–4 kg); (b) Whole body strength (4 kg) or hand system (3 kg); (c) Manual Material Handling (MMH) that encompasses the lift, carry, push and pull movements, had to be performed; (d) Repetitive loads of upper limb. The fourth session is based on the medical and epidemiological data, which is based on the OCRA method [23]. After analysis by the ergonomics team, partial scores are generated called Extra Points (Additional Low Physical Effort Movements), Force (Body and hand system), Posture (Repetitive Loads of Upper Limb), MMH and the final score that covers all partial scores [7].
For this study, we performed the weighted average of the partial and final scores of the workday of each worker. This topic was used only in phase 2 because the objective of phase 1 was only to evaluate reliability, while the results given by the tool are essential to achieve the goals of the phase 2.
– Blood Pressure, Heart Rate, Height and Weight: For the monitoring of the heart rate it was used the Polar H10 HR M-XXL. According to Office of Disease Prevention and Health Promotion (OPHP) the heart rate target, in moderate and vigorous efforts is defined by 70 at 85 percent of the maximum heart rate. Thus, the formula: 220-age×0.70. [15]. To check blood pressure it was used the HEM-7200-E OMRON – Omron M3 Intellisense blood pressure monitor. The position was seated, with his arm resting on a firm, heart-level surface with his/her palm facing upward, uncrossed legs, feet resting on the floor and back resting on the back of the chair [15] with the standard protocol of anthropometry and weight balance [24]. The height protocol was used, with the participant positioned in relation to the stadiometer, with the feet in vertical position (together or slightly apart) and the arms extended along the body. The head was oriented according to the Frankfurt plan, parallel to the floor. The participant is asked to perform the “grow or unwind” inspiration while the board is positioned over the participant’s head, exerting constant pressure on the scale was used [24].
Data analysis
Phase 1 – Reliability
To verify the reliability test-retest it was used on Intraclass Correlation Coefficients (ICC) and its 95% confidence interval for the 2-way error model. The ICC is interpreted as [25]: ICC greater than 0.90 considered excellent and sufficient for testing. ICC between 0.75 and 0.90 good and sufficient for testing. ICC less than 0.75 is poor and not acceptable for testing.
Phase 2 – Predictive factors of functional decline
Statistical analyzes were separated, in a first stage in Men, Women and total sample, dividing them in under 40 years and over 40 years. However, after applying the statistics, it was found that there was no significant difference between men and the women groups and therefore, only the final population was divided into groups under 40 and over 40 years. The following steps were fulfilled:
Descriptive statistics: absolute and relative frequencies for nominal variables, and mean and central tendency for the quantitative ones were determined; The normality distribution of the continuous variables was verified using Kolmogorov-Smirnov; In order to verify if there were statistically significant differences between groups, (<40 years and > 40 years), the Student T Test was applied for the parametric variables and the Manny-Whitney test for the non-parametric variables. Pearson to parametric variables and Spearman correlations tests for nonparametric variables were applied to verify the relationship between EAWS and COPSOQ variables with functional capacity tests. Inferential analysis of the work and personal determinants of workers’ functional decline was determined by multiple linear regressions (method stepwise).
All statistics analysis were performed with SPSS (version 22.0; IBM, Armonk, NY, USA) and a critical level of p < 0.05 was set as significantly.
Results
Phase 1 – Reliability
The study involved the participation of 12 people of both gender (seven men and five women), with a mean age of 35.1±10.6 years-old, mean seniority at work of 6.00±7.89 years, mean height of 172±0.08 cm and mean weight of 72.0±9.80 kg.
The descriptive analysis and the ICC of the test results at moments 1 to 2 is presented in Table 1.
Descriptive analysis and Interclass Correlation Coefficient (ICC) of test retest
Descriptive analysis and Interclass Correlation Coefficient (ICC) of test retest
LL (lifting low); LH (Lifting High); OW (Overhead Working); HG (Handgrip).
The results for all tests between the moment 1 and 2 were quite similar, with an increase of 3 kg for LL test and a decrease of 1 kg for HG test. Regarding the reliability between the two moments, it was observed a very good results between the first and second assessment, regardless the functional test (ICC≥0.90). The time between the moment 1 to 2 was 3 days.
The sample was composed by 147 workers (121 men and 26 women). Based on the definition of senior workers, the sample was divided in two groups: under 40 and over 40 [1]. The variable gender did not have significant differences either and, therefore, both sexes incorporated within the age groups, p < 0.05.
The group of workers aged < 40 years comprised 102 employees, with a mean age of 28±5.29 years and with a mean seniority of 1.70±3.12 years. The average anthropometric measures of weight and height were 74.9±14.7 kg and 174±0.08 cm, respectively. The functional capacity scores had an average value of 24.6±1.20 kg (LL); 22.9±3.30 kg (LH); 2.73±0.49 min (OW), 48.1±10.6 kg (HG2), 33.0±9.26 ((HG5). The mean values of the work exposure assessment by EAWS scores were: Extra-Point: 3.51±2.15; Posture: 14.9±5.97; Force:5.61±3.51; MMH: 2.53±3.35 and the Final Score: 26.51±5.92.
The group over 40 years old was composed by 45 workers with a mean age of 44.8±3.62 years and mean seniority of 14.4±9.36 years. The anthropometric measurements of weight and height were 74.2±11.5 kg and 171±0.07 cm, respectively. The mean results for functional capacity were: 24.4±1.70 kg (LL); 22.2±3.94 kg (LH); 2.58±0.04 min (OW); 48.8±9.77 kg (HG2); 32.2±8.56 kg (HG5). The exposure to job demands (EAWS) has the following mean values: Extra-Point: 3.40±2.10, Posture: 11.9±6.70, Force: 4.15±2.87, MMH: 0.98±1.67 and the Final Score: 20.1±7.92. The complete descriptive data are presented in the Table 2.
Descriptive Analysis of individual parameters and occupational exposure factors
Descriptive Analysis of individual parameters and occupational exposure factors
*EAWS (European Assembly Worksheet).
The mean results from the psychosocial factors are presented in the Table 3. It was possible to observe that younger workers present lower mean scores in the work rhythm and influence dimensions, when compared to older workers (Table 3). Regarding the work ability index, the mean score of younger workers is quite similar to the older ones. This means that, although older workers could have a lower functional performance, they don’t perceive this decline.
Descriptive analysis of the psychosocial factors and work ability index, stratified by age group, divided by age groups
* COPSOQ (Copenhagen Psychosocial Questionnaire); WAS (Work Ability Score).
Table 4 did not consider the OW test, as there were no statistically significant findings in both age groups. Regarding the correlations between functional capacity performance and weight, height, seniority in the company, WAS, cognitive variable for COPSOQ and work conditions Extra-Point, Posture, Force, MMH, Final Score it was observed.
Spearman and Pearson correlation
LL (lifting low); LH (Lifting High); OW (Overhead Working); HG2 (Handgrip position 2); HG5 (Handgrip Position 5), CD (Cognitive demands by COPSOQ questionnaire), E.P (Extra Points by EAWS); * statistically significant; # Pearson correlation.
A strong correlations and statistically significant only in the group of employees over 40 years old, in the HG2 tests with weight (r = 0.60 p = 0.05); height (r = 0.54 p = 0.01) and Cognitive Demands (CD) (r = 0.59 p = 0.01), Force demands (r = –0.58 p = 0.05), weight, height and CD were also correlated with HG5, in the group of over 40 years old. In the group under 40 years old, the most significant moderate correlations were found in the HG2 and HG5 tests with weight and height. The LH performance was correlated with weight (r = 0.30 p = 0.01) and height (r = 0.41 p = 0.01).
The multiple linear regression was used to verify if the variables age, height, weight, seniority, CD and the EAWS measure, are predictable variables of functional decline through the LL, LH, HG2, HG5 outcomes. The results are described in Table 5
Predicable factors (individual and occupational parameters) of functional decline of LL, LH, HG2 and HG5
*Statistically significant. LL (lifting low); LH (Lifting High); HG2 (Handgrip position 2); HG5 (Handgrip Position 5); CD (Cognitive demands by COPSOQ questionnaire), Force by EAWS.
The HG2 and HG5 tests deserves special mention, where the variables weight, height, seniority in the company, force measure (EAWS), and cognitive demands (COPSOQ) were considered predictive measures. The equation that describes this relation is: HG2 = –38.2 + 0.20. (height) + 0.36. (weight) + 0.23 (seniority) –0.42. (force) + 0.20 (CD). Also, the predictors for the LL test were weight, height, seniority and CD (COPSOQ) and the predictors of LH were height and weight. The full description is presented in the Table 5.
The aim of phase 1 was to evaluate the reliability of a battery of 4 functional tests of the workers in the automobile industry.
In this study, the intra-rater reliability from the ICC (>0.92) was considered excellent for the application test and also used the protocol by Isernhagen Work System 28 tests [4]. In other studies that aimed to verify also intra-rater reliability of 28 IWS protocol tests, ICC results were considered good to very-good: ICC 0.75–0.87 [26] and ICC 0.78 [27].
In the present study, only 4 tests of IWS protocol were used, since they were the ones that most correlated with the activities performed on the automotive industry assembly line, thus avoiding deviating from what they are the actual and specific requirements of the work [6,28, 6,28]. Moreover, in order to avoid fatigue and the learning effect, in phase 1 participants, a 3-day interval was set from moment 1 to moment 2 [29].
In the Phase 2 the aim was to determine the predictive factors of the functional decline of senior workers.
Regarding the analysis of the association of working conditions with functional capacity tests, in both groups, only HG2 and HG5 tests were statistically correlated with the Force and Posture measure, based on EAWS, which incorporates the work conditions and work demands.
The data mentioned above is very interesting since the force measurement approached by the EAWS incorporates the forces exerted by the whole body and hands and fingers when performing the task. Therefore, it is closely related to the Handgrip measure. This becomes even more interesting because these correlations between the force measure and the Handgrip test have a negative correlation, so when the force exerted during the tasks is of higher intensity, the Handgrip force decrease.
Although there were differences, about of the functional capacity test in the group of workers over 40 years, but these were not statistically significant when compared to the group of young workers.
For the lifting tests, the variables height and weight were correlated with the lifting capacity and were predictive of functional capacity decline. The same results were found in a study by [9, 21] concluding that the height, weight, aerobic capacity, sex, physical activity practice and physical workload have predictive value for the LL and LH. However, it confirms the need for a more in-depth study of the interaction of these components [21, 30]. Even in the lifting tests, there were no significant differences in the decline of the functional capacity of the older workers. In both groups, almost all the workers reached the load limit imposed for the tests (25 kg), mainly in the LL test. This observation was made based on the effort criterion, which analyzes the use of the accessory muscles for the test [4,8, 4,8]. However, in the LH test only 4 workers (3 in age group < 40 years-old; 1 in age group > 40 years-old) could not reach the limits of 25 kg. The load limitation to 25 kg is the threshold restricted in the automotive industry, and therefore, the healthy workers of this study, younger and older, can perform the tasks that have the lifting characteristics.
In the HG2 and HG5, in both age groups were statistically significant with height, weight, age the force parameters in the predictive value (Table 5) It stands out as a variable that must be measured along with the Handgrip. Height has been a measure currently associated to the Handgrip force, because there is evidence that for every 10 cm of body height, there is an increase of 2 to 4 kg of average grip strength and affirm the importance of measuring body height when assessing HG [31].
In the group of workers older than 40 years, it was found the interaction of functional capacity with the psychosocial factors. This finding is highly relevant because, as people get older, changes in cognitive aspects occur, mainly associated with attention and memory [32]. However, it well known that the cognitive issue differs from person to person, and also in many cases, senior workers in tasks requiring attention can outperform young people due to the experience factor [32–34].
We can state that the phenomenon of the healthy worker may have occurred, as a bias worker considered healthy tend to stay longer in their occupational activities, and this may be closely associated with the individual’s basal health condition. This situation may be associated with early interventions to prevent musculoskeletal disorders, proper health maintenance with regular screening and practice of physical exercise [35]. In the automotive industry where the study took place, the ergonomics team periodically screened the workplace conditions as well as the occupational health department’s screening of health conditions, and this practice may have influenced the healthy maintenance of workers.
Another factor that influences the response of the functional capacity in older workers may be related to the practice of rotation plans incorporated in the automotive industry to avoid fatigue and disorders musculoskeletal. The rotation plans are adopted during the work shift. For example, the person is not exposed to more than 2 : 30 hours in the same task and each worker has training in multiple skills. Besides, variation in work reduces fatigue and the risk of musculoskeletal disorders [36, 37] as long as job changes involve an effective change in work muscle groups being used [36–38].
The handgrip strength measure, found in the present study, can be incorporated by the automotive industry to make decisions both in terms of working conditions and in the clinical conditions of its workers.
Being possible to design the conditions work processes associated with the predictive values of HG2 and HG5, to identify the critical tasks related to the high application of grip strength and provide changes both in the scope of tools and in the scope of the product, and the implementation of the workers’ clinical surveillance system through periodic tests of handgrip strength.
Thus, it would be necessary for future studies to establish normative values of handgrip strength for workers in the automotive industry.
Limitations
We can say that the healthy worker phenomenon may have occurred as a bias because workers considered healthy tend to stay longer in their occupational activities which are related to the individual’s essential health condition. This may be associated with early interventions in the face of work-related musculoskeletal disorders, adequate health maintenance with regular screening, and physical exercise [42, 43].
Another factor that may be influences the response of functional capacity in older workers is the practice of rotation plans incorporated in the automotive industry to avoid fatigue and work-related musculoskeletal disorders. Rotation plans are adopted during the work shift. For example, a worker is not exposed to more than 2 hours and 30 hours in the same activity and there is an investment in the diversity of skills of the various workers, in order to ensure variability in occupational exposure.
Conclusion
The simplified battery of 4 tests showed an excellent reliability for the functional capacity workers assessment in the automobile industry. Force demands (relative to workload), height, weight (anthropometric measures) and seniority are predictive factors for functional capacity decline: LL, LH, and specially the Handgrip, in both groups. In addition, psychosocial factors have important role in the worker’s response to the functional performance, especially for the Handgrip, in senior workers. In further research and in the field context of occupational medicine and ergonomics, Handgrip force assessment should be integrated as a single measurement of functional decline. In this study, don’t have differences statistically significant between the younger and older groups with regard to functional capacity tests. However, the handgrip test, in this study, is a significant predictor in the older group, in relation to functional decline.
Footnotes
Acknowledgments
The authors are grateful to all workers who voluntarily participated in this study.
Conflict of interest
The authors declare no conflicts of interest.
Funding
This study was supported by the Coordination of Superior Level Staff Improvement (CAPES, Brazil). This work was partly supported by Fundação para a Ciência e a Tecnologia (CIPER - Centro Interdisciplinar para o Estudo da Performance Humana (Unit 447) [UIDB/00447/2020].