
Abstract
BACKGROUND:
Across the global landscape, mental health care still exhibits challenges because of the lack of human and professional resources to face its consequences. In Morocco, mental health problems affect mainly adolescents and young adults, with a clear impact on functional engagement in their daily lives. Occupational therapy, as a holistic and person-centered practice, may be an ideal mental health strategy to promote health and well-being through occupation, thereby enabling individuals to participate in regular daily activities.
OBJECTIVE:
To understand, from an intercultural perspective, the point of view of mental health professionals regarding the role and importance of occupation-based practices in Errazi Mental Health Hospital in Salé(Rabat) Morocco.
METHOD:
A qualitative research design was used for this study. Data collection consisted of semi-structured interviews with 12 mental health care professionals (non-occupational therapists). These results were used to gain an understanding of their perspectives regarding the main role of human occupation in mental health services in Morocco, and to incorporate an intercultural outlook in terms of occupational therapy. Data analysis was conducted in three phases, by following the grounded theory methodology.
RESULTS:
Two categories, “dimensions of occupation in Moroccan mental health” and “the interplay between traditional and western perspectives involving mental health” emerged from this research. Both categories included five subcategories.
CONCLUSION:
This study identifies how occupation-based services in Moroccan mental health care require considering not only the cultural perspective of mental health, and the sociocultural meaning rooted in occupations, but also the relevance of incorporating a community-centered approach. Moreover, it discusses how occupational therapy education in Morocco must incorporate an intercultural perspective of the therapy’s theory and practice.
Introduction
Identified as one of the top three leading causes of disability worldwide, mental health conditions often impose a considerable burden on human functioning and community participation [1, 2]. The disability experience associated with mental health problems and substance abuse is further increased by the social stigma and the treatment gap frequently present in mental health systems. In Morocco, clear epidemiological statistics on the disease burden connected with mental health conditions have not been published to date [2]. In 2014, the first national survey on disability indicated that 6.8% of Moroccans were disabled, with a higher prevalence among women and elderly individuals [3]. Although self-reported information on physical, cognitive, and intellectual impairments was gathered, mental illness was not specifically mentioned in this national report. However, a clear link between disability and the social determinants of mental health, including unemployment, limited education, and poverty, was highlighted. For instance, about 50% of Moroccans with disabilities are unemployed, a situation that may impede their participation in the community, triggering a distinct social impact [3].
Furthermore, the fact that people with mental health conditions are more susceptible to the deprivations of social opportunities, is a relevant issue [4]. In this regard, as a country in which poverty and inequality are still a big challenge, Morocco is facing the social problems derived from a high rate of people with mental illness problems [4]. This has a clear impact on the possibility of engaging in significant occupations connected with health and well-being, which in turn, aggravates the social problems of a particularly vulnerable and stigmatized population in this country [5]. Consequently, focusing on the prevention and promotion of mental health through occupation-based interventions may be an option to face this particular social problem in Morocco.
Occupational therapy services emphasize the use of meaningful occupation to promote participation within a variety of environments. That is why its distinct value is to promote, prevent, and offer intensive interventions throughout the person’s lifespan, by fostering participation in meaningful occupations for people with, at-risk of, and without any mental health challenges [6]. In fact, there is a full range of research regarding the effects of occupational therapy on mental health domains [6–11]. Kirsh et al. provided an overview of occupational therapy interventions in adult mental health services [7]. For this work, 50 peer-reviewed articles were analyzed to categorize occupational therapy interventions. These describe seven wide domains on which the practice may have an impact on people with mental health problems. Employment and education are part of the identified categories of intervention implemented by occupational therapists, which may enable participation within the community of individuals with these ailments [7].
Characterized by its holistic perspective and a person-centered approach, occupational therapy interventions are often community-based, established within the individual’s natural environment [12]. There is evidence that this further supports occupational engagement and community inclusion of people with mental health problems [12]. As a result, an integrated occupational therapy practice within the mental health care system is highly recommended for the recovery of adults with serious mental illness [12]. The inclusion of occupational therapy practitioners as mental health service providers in interdisciplinary healthcare teams, as well as continued research to further investigate the effectiveness of occupational therapy interventions for patients with psychiatric disorders, are crucial [12]. In a meta-analysis, the effectiveness of occupational therapy interventions for mental health conditions was examined across high-quality studies [6]. In this study, the performance of people with mental health conditions was found to improve in occupations such as parenting, work, home management, and maintenance, as well as in social participation. This approach also seems to enhance individual well-being, by improving occupational functioning in daily life and reducing the persistence of symptoms in individuals with serious mental illnesses [13, 14]. From this perspective, occupational therapy practice is a relevant approach to address the psychiatric disabilities of people of various ages [10, 16].
Indeed, to obtain optimal outcomes, occupational therapy in mental healthcare for adolescents and adults, should integrate diverse methods, such as cognitive remediation, combined with other top-down approaches, including support for employment and education, family psychoeducation, skills training, and environmental adaptations, among others [15, 16]. In reality, one of the main purposes of occupational therapy is to focus on supporting occupational engagement [17]. Hence, engagement in meaningful occupations represents a core facilitator to develop recovery-promotive identities in people with serious mental illness [12, 13]. To achieve this goal, occupational therapy works with people and communities to enhance their ability to engage in the occupation they want, need, or are expected to do, or by modifying the occupation or the environment to better support their occupational engagement [16].
In Morocco, the experiences of people with mental health problems are severely aggravated for two main reasons [18]: First, the lack of facilities and community-based services to address mental health problems. Therefore, an occupational therapy approach would contribute to the community inclusion of people with mental health problems, which is key within the context of Moroccan society as it is mainly community-centered [12]. Second, the limited resources— material and human— in the Moroccan mental health system [18, 19]. As we stated earlier, the mental health care system in Morocco has limited resources, and also, qualified occupational therapists are underrepresented among mental health practitioners [1, 19].
Actually, the first promotion of occupational therapists— recently graduated in 2020— afforded the first seventeen clinical practitioners in the whole country. Nevertheless, only two of them practice in mental health care settings. This is clearly insufficient considering the mental health care needs across the country [1, 19]. In addition to lack of funding, no research has been performed in Morocco regarding the impact and effectiveness of occupation-based therapeutic approaches grounded on quality evidence. These would have to be incorporated into the mental health system as soon as such investigations take place. In Morocco, mental health settings do use activities as a means of entertaining people during hospitalization, heightening the lack of comprehensive occupational analysis and its therapeutic advantage for people in psychiatric settings. Indeed, the predominance of the biomedical approach in treating serious mental illnesses further underscores those biopsychosocial interventions, such as those developed in occupational therapy, may face challenges in the Moroccan mental health care system [19].
However, occupation, as a therapeutic method, has a distinct value for improving health and quality of life, by enabling participation and engagement in meaningful occupations, and in activities of everyday life [7]. For this purpose, occupational therapy professionals are distinctly qualified to practice occupation-based interventions due to their expertise in occupational performance, activity analysis and design, environmental analysis, neurophysiology, psychosocial development, and group dynamics, among others [12].
Therefore, the aim of occupational therapy services in mental health settings is to help all individuals develop and maintain positive mental health, prevent mental illness, and recover from mental health challenges in order to live meaningful lives [7, 13].
Although the inclusion of occupational therapy practice in Moroccan mental health care is highly encouraged, it is important to consider how the professional culture of occupational therapy could clash with the local approaches and beliefs in addressing mental health conditions and occupations [17, 20].
For instance, the very notion of meaningful occupation is mainly defined according to social norms and values and may be perceived differently from one country to another [17, 18]. Actually, most of the occupational therapy literature and practice guidelines are, to date, highly influenced by western countries [18]. Several studies have explored the intercultural differences regarding mental illness experiences and the recovery process within Arab cultures, of which Morocco is a part [21]. The main differences noted involved religion and spiritual practices, the role of the family and traditional healers, and the impact of feelings of shame and victimization endured by individuals living with mental health problems [22]. That is why occupational therapy, from an intercultural perspective, needs to incorporate diverse theories around the core concepts guiding the practice [17, 20]. For this reason, culturally relevant occupational therapy in Morocco should identify how occupation is conceived and what the role of occupational engagement is on health and well-being [17].
Therefore, this study explores the occupational therapy perspectives held by health care professionals in mental health services, and specifically the relevance of the occupation-based practice in Errazi Mental Health Hospital in Salé(Rabat) Morocco. This will set the groundwork to unfold the new profession, the arrival of new occupational therapists in care facilities, and the subsequent intercultural adaptations to occupational therapy interventions in Morocco.
Method
Study design
Grounded theory is crucial to gain an in-depth understanding of concepts or processes during an investigation. That is why a qualitative research design based on such theory was chosen to answer the research questions [23]. Therefore, we used a constant comparative method of analysis until a saturation point was reached. Through this process, categories emerged, and these were linked by applying constant comparison [24].
Participants and recruitment
The interviews involved mental health care professionals from Errazi Mental Health Hospital in Salé (Rabat) Morocco (near the capital city Rabat, Morocco) and the Occupational Therapy Education Program in Rabat. To guarantee the emergence of various perspectives the following inclusion criteria were used: discipline (nurses, social workers, psychiatrists, occupational therapists), services (geriatric and pediatric psychiatry, addiction, and mental health day hospitals), and at least three years of experience in mental health. Exclusion criteria included mental health care professionals without contact with occupational therapy students and no knowledge of the occupational therapy profession.
The recruitment process was performed by the fourth author (JB), who worked for ten years in Errazi Mental Health Hospital. He was aware of the professionals’ profiles and hospital procedures. That is why convenience sampling was used for this study. Data gathering was performed between April 25 and May 15, 2019, by the first author (IZ) with the support of JB. In total, twelve participants were recruited, ten of whom were health care professionals at the mental health hospital, and two foreign professors linked with the Occupational Therapy Education Program (when data was collected there were no Moroccan occupational therapy graduates yet) (Table 1).
Participant characteristics
Participant characteristics
Semi-structured interviews were used to collect the data. IZ was responsible for collecting the data with the support of JB. The researcher is an occupational therapist with experience in qualitative methodology and is also familiar with Moroccan culture for she lived one year in the country. Before collecting any data, the researcher informed participants of the purpose of this research. Moreover, before the interviews, all participants signed informed consent forms, including authorization to audio-record the interviews. The quotations collected were coded by the letter P (participant) and a number assigned identifying the participant.
Each interview began with general questions related to the participants’ training in the field of health, years of experience, and their role at Errazi Mental Health Hospital. After these general questions, data gathering incorporated open-ended questions (Table 2). Interviews were conducted for an average of 90 minutes. The data was gathered and analyzed in French. No translators were involved in this research because four members of the research team and all participants spoke French fluently.
Semi-structured interview questions for mental health professionals
Semi-structured interview questions for mental health professionals
The interviews were audio-recorded and transcribed. All transcriptions were shared with the authors. Three authors were involved in analyzing the data (first, third and fourth). Initially, each researcher analyzed the data separately, and afterward, they compared their codes and established a common coding system.
Pursuant to the grounded theory methodology, data analysis was conducted in three phases, establishing a coding system that provided open, axial, and selective coding [23, 24]. In the first phase, two researchers performed verbatim transcriptions of all interviews. Before analyzing the data derived from each participant, the transcripts were read several times to get a clear notion of the content. Second, after completing the interviews, relevant parts were grouped under summarizing headings to identify various preliminary categories. Two researchers were involved in this process at the same time. Third, the data was compared with previous parts, and categories were related to their corresponding subcategories in terms of their properties and dimensions. During these analyses, it was considered relevant to return to earlier data in a constant comparative process. Finally, the categories and subcategories that emerged were refined. Based on this analysis, two categories were constructed, which explain the topic studied. Finally, to ensure plausibility, the research team discussed their interpretations. In terms of credibility and as a means of peer debriefing, the analysis process was reviewed by the research team to verify consistency in how findings were reached.
Researchers’ backgrounds
The research team has a diverse knowledge of and background in Moroccan culture and occupational therapy. Four of the six researchers are occupational therapists with different backgrounds; one from Spain, three from Morocco, two of whom live in the United States and one in Canada. Also, two nurses are part of the research team, one from Morocco specialized in mental health, and another from Spain specialized in sociology.
Ethical considerations
The research adhered to the Declaration of Helsinki. The Biomedical Research Ethics Committee at the University Mohammed V in Rabat (Morocco) approved the study protocol (ref. 22/20). Confidentiality was assured throughout the research process. Written informed consent was obtained from all participants.
Results
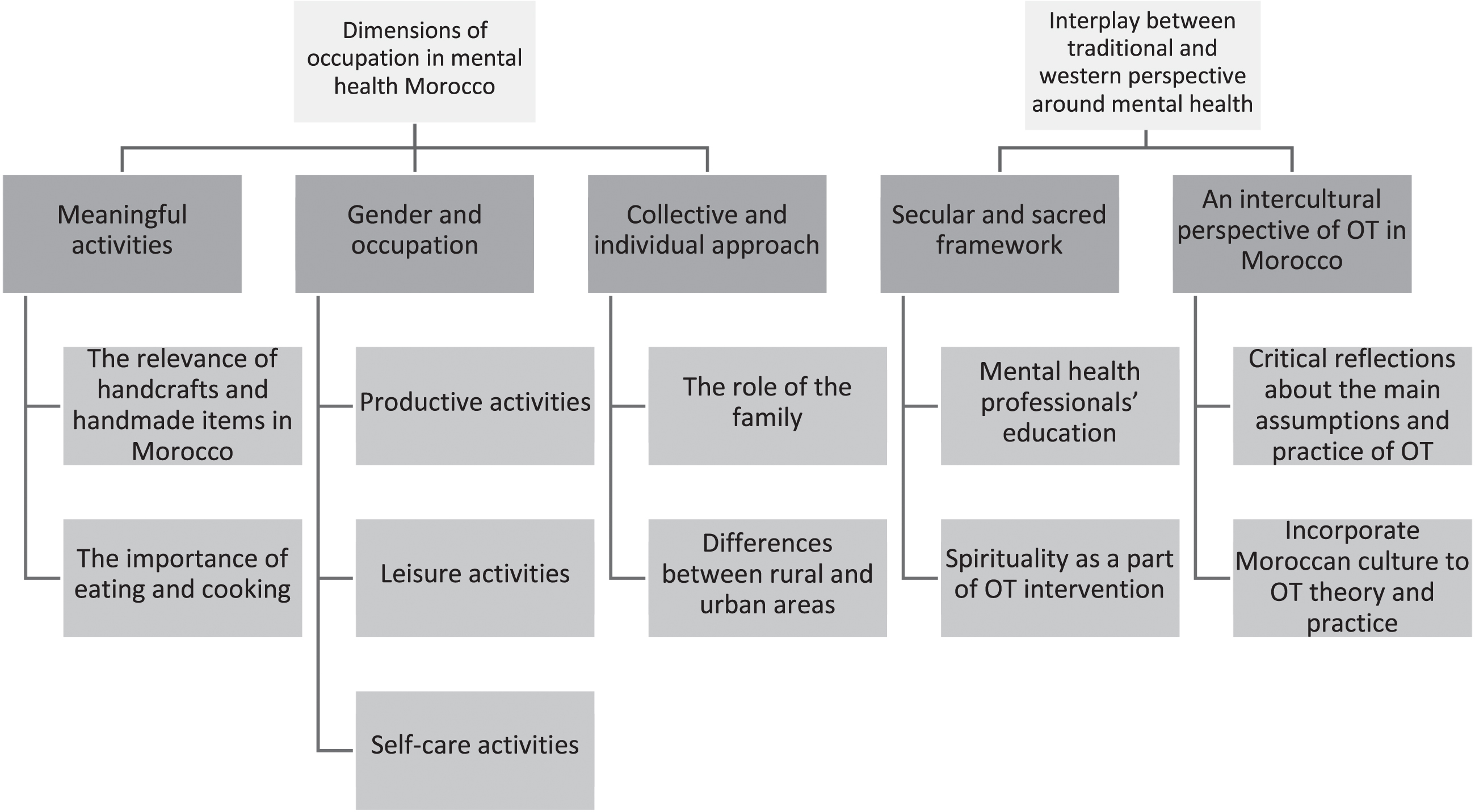
A total of two categories and five subcategories were identified throughout the iterative process of comparative analysis. One category is dimensions of occupation in Moroccan mental health, and it includes three subcategories: meaningful activities, gender and occupation, and collective and individualistic approaches. The other category that emerged is the interplay between traditional and western perspectives involving mental health and it includes two subcategories: secular and sacred frameworks and intercultural perspective of occupational therapy in Morocco.
Combined these represent the participants’ viewpoints regarding the main role of human occupation in Moroccan mental health services, with the purpose of incorporating an intercultural perspective of occupational therapy in this country (Fig. 1). The results, supported by illustrative quotations, are presented for each category and its subcategories.
Categories and subcategories which emerged.
According to mental health care professional participants, the most meaningful activities in the Moroccan context are related to creativity. For this reason, several participants reported that in terms of mental health it is relevant to offer activities in which body, mind and spirit are engaged. In this sense, handicrafts and manual activities are considered significant in Moroccan culture to promote mental health.
“Handicrafts in Morocco are highly developed and valued . . . mainly activities that they [the patients] can work with their hands.” (P10)
Moreover, a participant who supported creative activities explained these allow them to express feelings and establish communication outside the mental health institution.
“Make a small escape, a space of freedom which goes beyond the premises, which goes beyond the walls, the person with mental illness can express everything they have inside.” (P1)
Therefore, for people with mental health problems, using occupation as therapy provides not only expression but also empowerment.
“When you express what is inside of you through an activity, you become somewhat clear-headed, things slowly clear up, and you can be ready to make decisions . . . ” (P1)
Gender and occupation: “These activities are part of women’s identity/daily life.”
In Morocco, the influence of gender in occupations is one of the most significant aspects to understand its dimensions in mental health. Three interconnected subcategories related to the impact of gender in occupations were identified based on the participants’ perspectives: production, self-care, and leisure activities. One participant explained how most occupations in the country are separated by gender.
“We are used to separating everything for women and men . . . even at the hospital women and men are in different buildings and participate in two different therapeutic activities . . . never do we propose mixed activities at this hospital.” (P6)
Some occupations in Morocco, performed in private or public scenarios, are dependent on gender as well. In connection with this, men are seen much more in public areas and women are mainly in private ones.
“[ . . . ] men have several chances to relax from stress, they live in cafes, but women, given their role of caring for the children and cleaning the house, are more stressed than men and must usually stay at home. For them, it is not possible to go out alone and have coffee or go for a walk . . . ” (P9)
Collective and individualistic approaches: “We are in constant connection with others, but individualism is also just here.”
The relevance of family and tradition is still essential in Moroccan culture. However, there is a vast difference in lifestyle between rural and urban areas. In Morocco’s main cities, there is a much more individualistic attitude and connection to the extended family is not as prevalent as in rural areas.
“Morocco is not an individualistic society; here we depend on family and the community. The extended family is particularly relevant to celebrate and participate in essential rituals . . . but at the same time, over the last decades, there has been a sort of individualism that is permeating our way of life . . . ” (P3)
Likewise, there is a tradition to gather the family on Fridays because it is a sacred day in the Islamic religion, and usually families share couscous during the main meal of the day. Also, other dishes, like tagine, are an integral part of family gatherings and traditions.
“[ . . . ] certain dishes, tagine, couscous are shared, and we discuss partaking with the family, the grandfather, the father, and the children... makes no sense to me to be alone to eat these dishes because it is time to be and feel part of my family.” (P6)
Secular and sacred frameworks: “The Quran is a shelter in a modern and secular world.”
In Morocco, religion is an essential part of life, and daily occupations revolve around the five daily prayer times. However, knowing how to balance these two frameworks— secular and sacred— is quite a challenge in a country where many Moroccans are faced with the dilemma of finding a middle ground between these two symbolic frameworks.
“He [person with mental illness] found prayer and the Quran were a refuge for him; he became a mentor of Alcoholics Anonymous [ . . . ], as soon as he started praying, he became abstinent and he still is today, 8 years later.” (P5)
For this reason, certain participants suggest incorporating specific knowledge related to medical anthropology, in the interest of fully understanding how these two frameworks could contribute and be combined to promote mental health among the Moroccan population.
“It is because I am curious about it that I decided to study medical anthropology, but during all my studies nothing of this nature was addressed . . . I think this knowledge should be a must in the medical education program . . . ” (P7)
In the mental health area, the rationale behind mental illness as regards spiritual beliefs remains undeveloped. Incorporating a spiritual dimension in rehabilitation programs— as an occupational therapy approach— holds great promise.
“The way we look at occupational therapy... if we consider occupational therapy on a body, we have to change the body or the context . . . if it is done from a more global approach, OT will provide us a lot and perhaps, we can incorporate Islamic beliefs and practices with other OT concepts... spirituality is very underdeveloped / underappreciated in occupational therapy practice, but . . . Morocco is a strong spiritual context where we can learn how to do it. If OT in Morocco can harmonize both worlds (sacred and secular), it would be fantastic for all of us and for the OT discipline... Otherwise... we will colonize knowledge and practices ignoring the diversity of this context.” (P12)
An intercultural perspective of occupational therapy in Morocco: “Every occupation is global and local.”
Introducing occupational therapy into mental health services in Morocco requires a critical reflection regarding the main assumptions around occupation and the practical approach of this profession. To this end, incorporating the main aspects of Moroccan culture into the occupational therapy practice is required if this profession wishes to satisfy occupational needs and promote mental health through meaningful activities in mental health services.
“I think occupational therapy must combine a local and global reality . . . that is why, when Moroccan occupational therapists finish their degree, they need to be able to question and critically reflect upon theories and practices . . . The majority of occupational therapy lectures come from outside Morocco . . . We have the possibility of rethinking (occupational therapy) theories and practices to expand our occupational knowledge... it is questioning, it is wealth.” (P12)
Discussion and implications
This qualitative study focused on the role and importance of occupational therapy in mental health services, and it is the first research on this subject conducted in Morocco. In general, Morocco’s health care system faces many challenges especially in terms of mental health care [25]. The WHO Atlas report cites that there are approximately six inpatient beds per 100 000 population in Morocco [25]. Occupational therapy interventions in mental health can improve the health care system in the country by improving people’s engagement in daily occupations. However, as mentioned above, there are only 17 qualified occupational therapists for a country of over 30 million people. Only two of them are in mental health services.
Nevertheless, a holistic therapeutic approach to occupational therapy can improve the well-being of individuals with mental health during their stay at inpatient mental health facilities [26]. In addition, occupational therapy services can provide support to people suffering from mental health disorders, who are in transition from inpatient mental health settings to community ones [26]. This is truly relevant in a country where community and family are central to daily life. For this reason, and with the purpose of incorporating an intercultural perspective of occupational therapy intervention in Morocco, this research focuses on analyzing the role and importance of occupation in the mental health approach within this context. Research in other countries, such as South Africa, reveals that where novel occupational therapy practices are emerging, a defining process considering the cultural context must take place, by integrating adequate occupations for individuals and community requirements [27, 28].
In terms of meaningful activities, the participants in this study indicated the importance of crafts in Morocco, particularly those made by hand. According to Hammell [20], handcrafting has long been a form of significant engagement, and it is considered the bedrock of occupational therapy intervention in different cultural contexts. Therapeutic use of art as a mental health intervention has a successful track record in many mental health settings around the world. In this sense, Australian art programs are an example in which the themes discovered as an outcome of art engagement include the development of spirituality, empowerment, and self-validation [29]. This is also clearly stated herein: A health care worker believes that some people in mental health services are able to express their feelings and communicate with people outside the mental health institution through meaningful creative activities, which is not surprising since Moroccans are still able to make and buy handcrafted items to be used in almost all daily activities. This is particularly evident in older cities, such as Fes, Marrakech, Meknes, and Rabat. Moreover, Moroccans all over the country use handicrafts for cooking, cleaning, and other day-to-day chores.
In Morocco, as clearly stated by eight of the participants in this study, gender separation is still present in many daily activities and routines. Pooremamali et al. [30] sustain that the cultural perspective affects mental health treatment and establishes barriers in the therapeutic relationship. For example, an occupational therapist may suggest a homecare task that may make Moroccan men feel disrespected, such as asking them to prepare a meal or wash dishes as part of their therapy, for these are commonly gendered roles in Morocco [31]. This is also apparent in leisure activities and hobbies. For example, women may refuse to sit outside in a caféwhere they are visible or if there are many men in that café. Gender separation is important to understand Moroccan culture.
In contemporary Moroccan society, mainly in urban areas, individualistic and collective perspectives of society coexist. However, Morocco is still a collective society in which the family is central to it. For this reason, Moroccans can sacrifice a great deal to be with their families and prefer to live near them. Even in most major cities, there is only one nursing home to provide services for older adults because Moroccans believe in taking care of their parents and putting them in a nursing home is highly unlikely [32]. At least 75% of Moroccans live with their extended families even after the person has married and has had children. This is still evident in rural areas and to a lesser degree in urban ones [33]. Getting together with the family on a weekly basis is a tradition all over the country. This became apparent from the participants’ responses, in which most of them emphasized the importance of getting together for a meal on Fridays to share couscous, a national Moroccan dish.
In this country, the conflict between traditional and western perspectives involving mental illness is still a challenge [34]. Morocco is considered a spiritual society. In addition, Islam, as a religion, is believed to be central to life. Many people in the country seek to recover from a mental illness through their religion exclusively, or as a complement to biomedical prescriptions issued by mental health professionals. As some participants stated, resorting to religion can be a tool to combat addiction. Thus, including spirituality in occupational therapy interventions, in adult mental health services, should be discussed for in the Moroccan context spirituality is at the core of daily living [30, 34].
For these reasons, an intercultural perspective of occupational therapy education and practice is required in Morocco to understand what the main occupations in this context are and how to incorporate them to promote and foster mental health. Including Moroccan culture in occupational therapy intervention is crucial for its successful development in the country. No occupational therapy theories, models, or frames of reference used in relevant educational programs were developed in Morocco or in any other Arab country with similar characteristics. This calls for the need to develop theories, models, and frames of reference that originate in Arab countries.
Strengths and limitations
A strength of our study is the inclusion of views from different stakeholders involved in occupational practices, which has provided valuable information to pave the way for the development of occupational interventions in Morocco.
Our study has two limitations. First, we must recognize that recruiting participants from other mental health resources might have perhaps enhanced certain aspects regarding the relevance of occupation in mental health settings. However, the research team considered that for most of the topics discussed, the information obtained was sufficient to answer the research questions posed. Second, all our findings may not apply to other health care systems. Nonetheless, from a sociocultural perspective and community-centered approach, this is the first study in Morocco that intends to obtain a description of the role an occupational therapist performs in mental health services.
Conclusion
This study identifies how occupation-based services in Moroccan mental health care require considering not only the cultural perspective of mental health, and the sociocultural meaning rooted in occupations, but also the relevance of incorporating a community-centered approach. Moreover, it discusses how occupational therapy education in Morocco must incorporate an intercultural perspective of the therapy’s theory and practice. For this reason, a critical reflexive stance in terms of the practice and main assumptions of occupational therapy is required in relevant educational programs in Morocco. This research is also an invitation to continue investigating how an occupational therapist, as part of an interdisciplinary health care team in the mental health domain, is useful and effective in helping people with mental health problems and their communities to handle the performance of daily activities.
Footnotes
Acknowledgments
The authors would like to thank all professionals at the Errazi Mental Health Hospital in Salé (Rabat), especially those who generously participated in this research explaining and sharing their daily lives and occupations.
Conflict of interest
None to report.