
Abstract
BACKGROUND:
Physicians who suffer from poor sleep quality are at an increased risk of mistakes and poor decision-making. We deemed it noteworthy to assess sleep quality in practicing physiatrists, previously reported to be at higher risk of physician burnout, which was documented associated with sleep deprivation.
OBJECTIVE:
The aim was to estimate the prevalence of sleep disturbance among practicing physiatrists and evaluate the association of sleep quality with their sleep hygiene habits and depression.
METHODS:
Of the 101 study participants (77 females) who met the inclusion criteria, the majority was between the age of 25 and 40 years (70.3%); 62 (61.4%) were specialists and 39 (38.6%) were in training. In this cross-sectional study, practicing physiatrists were invited to complete an anonymous and voluntary web-based survey. The survey consisted of questions covering demographic information, nicotine and caffeine consumption, exercise habits, and three questionnaires: the Pittsburgh Sleep Quality Index (PSQI), the Beck Depression Inventory-II (BDI-II), and the Sleep Hygiene Index (SHI).
RESULTS:
Sixty-five (64.4%) respondents showed poor sleep quality (PSQI > 5), and 23 (22.8%) showed at least mild symptoms of depression (BDI-II>13). The mean PSQI, SHI, BDI-II scores were 6.85±3.09, 18.18±5.35, and 8.36±7.52, respectively. Poor sleep quality was significantly positively correlated with symptoms of depression and sleep hygiene misbehavior.
CONCLUSION:
We found that 64.4% of practicing physiatrists suffered from poor sleep quality, and 22.8% showed at least mild symptoms of depression. Considerable efforts should be directed toward sleep hygiene behavior and mental health improvement.
Introduction
Physical and rehabilitation medicine (PRM) is a medical specialty where physicians are known as ‘physiatrists’ or ‘PRM physicians’. Like other medical specialists, these physicians provide direct medical care managing various health conditions and need to receive training in different emerging methods, e.g., musculoskeletal ultrasonography [1] and robotic rehabilitation [2]. In addition, physiatrists are responsible for leading/coordinating the multiprofessional rehabilitation team, e.g., physiotherapists, occupational therapists, speech therapists, psychologists, nurses and social workers [3, 4]. Furthermore, PRM physicians interact with people of all ages with different disabling health conditions, e.g., spinal cord injury, stroke, multiple sclerosis, and polytrauma. Therefore, chronic occupational stress and emotionally challenging work, particularly when associated with inadequate reward, can result in physician burnout [5]. A career satisfaction rate of 75% was reported in the PRM specialty in 1997 [6]. Shanafelt and coauthors, seventeen years later, reported a 63.3% prevalence of burnout among physiatrists, with an unfavorably increasing tendency across time [7]. Later, in 2019 the prevalence of burnout among PRM physicians was reported as 51% [8]. Notably, burnout has also been reported to be reciprocally associated with sleep problems [9, 10]. Insomnia can be defined as an unpleasant experience of difficulty initiating sleep, maintaining sleep, and non-restorative sleep. Sleep quality is influenced by several factors, including depression, other comorbid diseases, sleep hygiene (habits around bed/bedtime to promote better sleep quality), and professional activities. Particularly, shift work was documented to be coupled with a higher risk of depression and sleep disorder development in night shift workers, e.g., physicians and nurses [11–14]. Another mechanism for developing sleep problems is work-related stress [15], which could be the main contributing factor in physiatrists. Importantly, tired physicians are at an increased risk of mistakes and poor decision-making [16]. Furthermore, a sleep disorder can lead to psychopathological impairment and other serious health problems (e.g., hypertension) [17]. The good mental shape of health care professionals is essential for their clinical work and academic performance [18]. Physiatrists’ mental health and professional satisfaction are major issues in our field that need to be investigated [19]. Although sleep disturbance has been reported in medical school students [20] and physicians across several medical specialties [21], no published studies addressed sleep patterns among physiatrists to our best knowledge. We conducted this study to evaluate sleep quality and habits and possibly associated symptoms of depression in PRM physicians.
Materials and methods
Design
An online survey was conducted in this cross-sectional study from 8th to 22nd January 2021 using Survio Platform (Survio s.r.o., Brno, Czech Republic). The survey comprised 67 questions in total. The questionnaire was composed of general information about the study and consent form, sociodemographic variables (gender, age, working experience, career stage, institution category, night shifts), physical activities, nicotine and caffeine consumption customs, and household members. Furthermore, the questionnaire covered questions from the Sleep Hygiene Index (SHI), the Pittsburgh Sleep Quality Index (PSQI), and the Beck Depression Inventory. The work described has been carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans. This study was approved by the Institutional Review Board (IRB) of the General Teaching Hospital in Prague. The first page of the questionnaire consisted of the consent form. Participants were informed about the study and that clicking the 'agree' button will be considered their informed consent. Study participants always had the right to leave the survey by closing the browser window. The survey platform that we used allowed secure data collection and protection.
Participants
Respondents were physiatrists working in the Czech Republic who voluntarily agreed to complete the questionnaire. An anonymous web-based questionnaire was distributed via researchers' personal email address lists. Our mailing list comprised about 80 physiatrists working in the Czech Republic. Furthermore, we shared the questionnaire link within two Facebook groups relevant to the field of physiatry. One Facebook group in which we shared the questionnaire is focused on young physiatrists' needs, education in particular. There were 437 members in this group. The second group had 134 members, and was oriented on PRM in general. All study participants were asked to answer the questionnaire only once, regardless of whether they received the invitation in more different ways. The inclusion criterion for this study was current full-time employment as a physiatrist. Excluded were pregnant women and those on parental leave.
Outcome measures
The Sleep Hygiene Index (SHI), an instrument designed to assess for sleep hygiene misbehavior [22]. Mastin and coauthors derived those items from the inadequate sleep hygiene diagnostic criteria outlined in the International Classification of Sleep Disorders [23]. In total 13-item scores were summed, thus providing an overall evaluation of sleep hygiene malpractice (Appendix A). Higher summaries meant worse sleep hygiene status. Items were rated on a 5-point Likert scale (0-4) and summed to achieve a global SHI score ranging from 0 to 52.
The Pittsburgh Sleep Quality Index (PSQI) was used to measure sleep quality and patterns over the last month [24] PSQI components derived from 19 questions measured seven subscales: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, sleep-promoting drugs, and daytime dysfunction. Participant responses were framed on a 4-point Likert scale (0-3) [25]. Sum of scores ranged from 0 to 21, with higher values indicating poorer sleep quality. A global PSQI score > 5 was deemed the clinical cutoff in differentiating good and poor sleepers [24].
The Beck Depression Inventory-II (BDI-II), consisting of 21-questions, was used to measure the severity of depression. All items were scored using a 4-point Likert scale (0-3) over the last two weeks. Higher scores indicated more severe depression. Scores were summed to achieve a total score, while 0-13 was considered minimal or no depression, 14–19 mild, 20–28 moderate, and 29–63 was counted as severe depression [26].
Statistical analysis
Data analyses were performed using the IBM SPSS statistics software (SPSS) version 25.0 for Windows (SPSS Inc., Chicago, IL, USA). The Shapiro-Wilk test was used to determine whether the continuous variables had a normal distribution. Continuous variables were presented as means, standard deviations, and medians. The nonparametric Mann-Whitney U test was used to compare continuous and ordinal variables between two independent groups and the Kruskal-Wallis test for more than two groups. The degree of association between two continuous or ordinal variables was determined using Spearman’s rank correlation coefficient. The relationship between nominal variables was assessed with the Chi-square or Fisher’s exact tests. We used linear regression analysis for testing dichotomous with continuous variables. The significance level was set at p < 0.05.
Results
A total of 102 responses were received. One questionnaire was excluded as it contained data potentially compromising the anonymization. Most of the respondents were females (76.2%), and the majority was aged between 25 and 40 years (70.3%). The sample consisted of 62 PRM specialists and 39 trainees. The median experience as a physician was eight years. Most participants (47.5%) lived with spouses and children or spouses without children (32.7%). Thirty-six (35.6%) physiatrists performed night shifts. The sociodemographic data of the participants are given in Table 1. The prevalence of significant sleep disturbance (PSQI > 5) was 64.4%, and the prevalence of symptoms of depression (BDI-II>13) was 22.8%. The mean PSQI, SHI, BDI-II scores were 6.85±3.09, 18.18±5.35, and 8.36±7.52, respectively. The scores for the PSQI, SHI, and BDI-II concerning gender, household characteristics, training status, and age are presented in the chart diagrams (Figs. 1 and 2). All PSQI, SHI, and BDI-II showed a significant mutual positive correlation at the level of significance p < 0.001. The type of professional activity (outpatient care vs. inpatient care vs. spa department) (p = 0.812) showed no relationship with sleep disturbance (Table 2). When comparing trainees with specialists regarding nightshifts, we found a significantly (p = 0.031) worse score in the SHI for those who regularly worked nightshifts only within the trainees’ group (Table 3). Among the PSQI questionnaire’s seven components, we observed a significant (p < 0.001) positive correlation of subjective sleep quality and sleep latency with SHI and BDI-II. Sleep duration and sleep efficiency were positively correlated with SHI (p < 0.001). The components assessing sleep disturbance, use of sleep medication, and daytime dysfunction were significantly positively correlated with BDI-II (p < 0.001) (Table 4). When evaluating the SHI individual questions, poor sleepers showed a significant association with emotionally burdened activities before bedtime (p < 0.001), frequent use of the bed for non-sleep associated activities, and allowing mental activities to occur in bed (both p < 0.05). Sleeping in an inappropriate bedroom (p < 0.01) and performing activities requiring high levels of attention shortly before bedtime (p < 0.05) was associated with the male gender. Living alone was associated with mental activities, such as using the internet or playing video games close to bedtime (p < 0.01) (Table 5).
General characteristics of the study participants
General characteristics of the study participants

A chart presents values for the Pittsburgh Sleep Quality Index (PSQI), Sleep Hygiene Index (SHI), and Beck Depression Inventory-II (BDI-II) regarding household characteristics and gender.
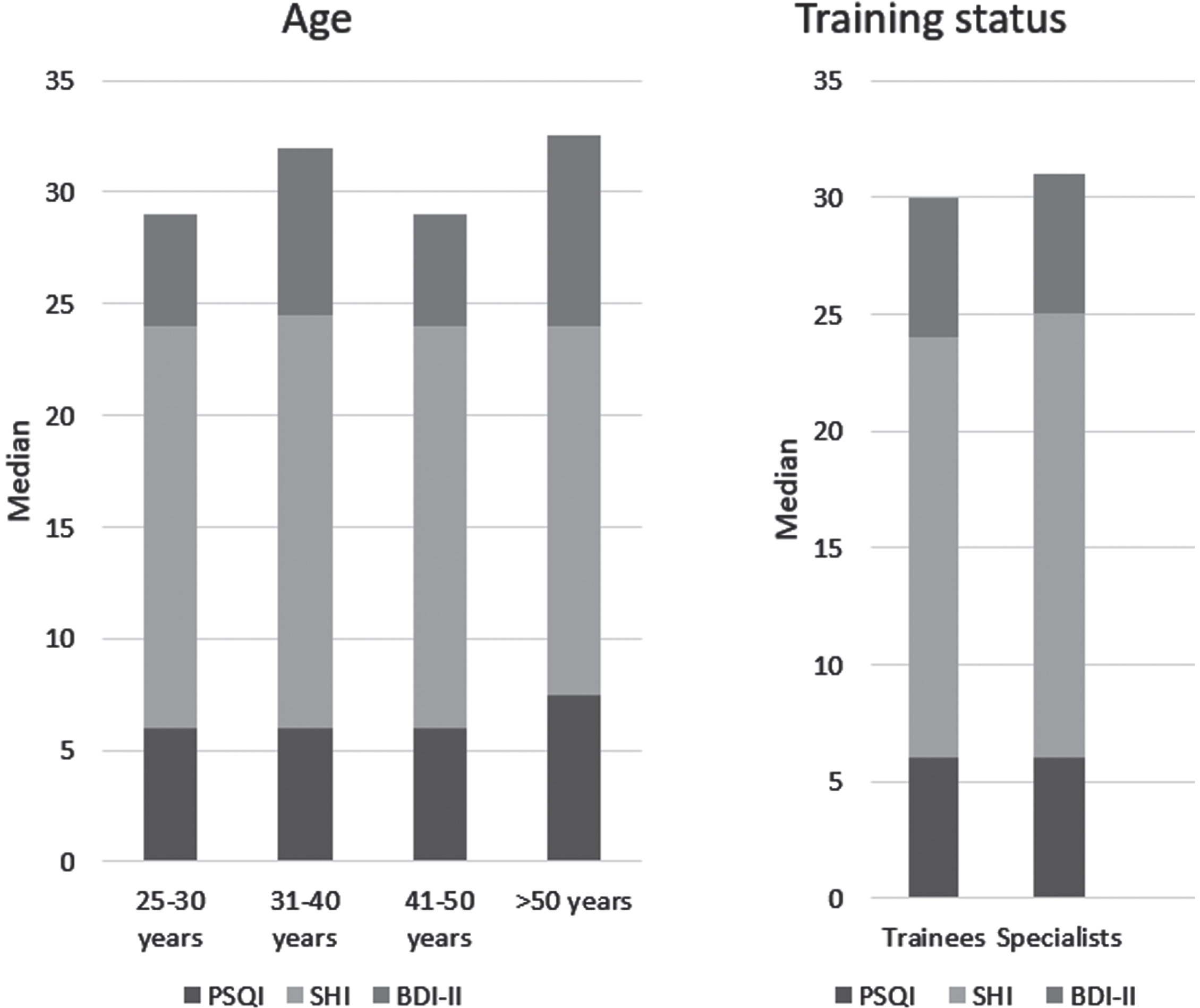
A chart presents values for the Pittsburgh Sleep Quality Index (PSQI), Sleep Hygiene Index (SHI), and Beck Depression Inventory-II (BDI-II) regarding age and training status.
The association between sleep quality determined by the Pittsburgh Sleep Quality Index (PSQI) score treshold (PSQI > 5 for poor sleepers and PSQI≤5 for good sleepers) and the study variables
Bold p values show significance. *p < .05. +Excluded were those participants who reported a combination of two or more activity types (n = 18).
A comparison of selected study variables between trainees and specialists
Data are given as mean±SD, and [median]. Bold p values show significance. *p < .05. SHI, Sleep Hygiene Index; PSQI, Pittsburgh Sleep Quality Index; BDI-II, Beck Depression Inventory-II.
Correlations between individual Pittsburgh Sleep Quality Index components (P1-7) and Sleep Hygiene Index (SHI), and Beck Depression Inventory-II (BDI-II)
Data are given as mean±SD, and median. Bold p values show significance. *p < .05, **p < .01, ***p < .001.
The association between individual SHI (Sleep Hygiene Index) components and Sleep Hygiene Index score (SHI), and sleep quality determined by the Pittsburgh Sleep Quality Index (PSQI) score treshold (PSQI > 5 for poor sleepers and PSQI≤5 for good sleepers) and the selected study variables
Data are given as mean±SD, or median (min-max). Bold p values show significance. *p < .05, **p < .01.
This study showed that almost 65% of the physiatrists who volunteered in the present study had unsatisfactory sleep quality (as defined by PSQI > 5). Notably, a relationship between poor sleep quality and sleep hygiene misbehavior and symptoms of depression was found. In the general population, the reported prevalence of sleep disturbance was 36% [27]. Previous studies indicate an increased risk of sleep disturbance development among some medical specialties. Carvalho Aguiar Melo et al. reported unsatisfactory sleep quality in 59.3% of psychiatry residents [28]. The reported prevalence was even worse than 46.1%, as previously documented among anesthesiologists [29] and obstetrician-gynecologists, where 29% of physicians showed very or fairly bad quality of sleep [30]. Recently, Gustavsson et al. reported a nearly 40% prevalence of less satisfactory sleep quality among primary care physicians. Interestingly, those who worked overtime but not on night duties were at higher risk of sleep unsatisfaction than those who worked overtime and took night duties [31]. We observed a worse score in the SHI for those who regularly worked nightshifts only within the trainees’ group. We can assume that this asymmetry in sleep hygiene behavior between trainees and specialists can result from the different workloads of trainees during the night shift. Nightshifts of trainees in the PRM typically comprise duties in the PRM department and, e.g., emergency medical service. Interestingly, PRM trainees who worked night shifts did not develop sleep problems as determined by the PSQI. This effect can be due to a young age, making younger trainees more resistant to insomnia. Another study showed sleep problems in 35% of primary care physicians, with a significantly higher prevalence (40%) among women [32]. Medical specialty with an alarmingly high risk for burnout (ranging between 25% and 77.8%) [33] is emergency medicine. In this specialty, Alhifzi and colleagues reported poor sleep quality in 83.8%, determined as PSQI scores≥5 [34]. Importantly, the prevalence of hypnotic drug use reached nearly 20% of emergency physicians, based on data from 1,097 emergency physicians working in Taiwan [35]. Regarding pediatricians, a survey from the United States reported good sleep quality in 71.2% of the respondents. However, their methodology for evaluating sleep was limited to only one question regarding the duration of sleep. The authors considered it sufficient when the self-reported time was≥7 hours [36]. When speaking about non-physician members of the rehabilitation team, a study from Brazil by Lino and coworkers reported poor sleep quality in 88% of frontline working physiotherapists during the COVID-19 outbreak. In nonfrontline workers, the reported prevalence was lower at 78% [37]. On the other hand, in their survey, Whelehan and colleagues mentioned that 63.3% of physiotherapists responded that they did not feel that their practice impacted sleep [38].
In our sample of relatively young physicians, we did not find any relationship between age and sleep quality. Notably, more than 90% of participants in our sample were < 50 years old. The absence of a larger number of older physicians is a relative limitation of this study. Kováčová et al. published a research where sleep quality was assessed using an actigraphic bracelet. In this study, the authors found better sleep quality in young women. Notably, gender differences were not evident in older participants [39]. Regarding sleep hygiene, we found its misbehavior to be more prevalent in trainees who regularly took nightshifts, males, and those who lived home alone. The higher prevalence of sleep hygiene malpractice is in line with the results reported for medical students. Interestingly, according to the study with medical students, married males had worse sleep quality [40]. Another recent study found, regardless of the profession, that older women living alone had poorer sleep quality than older men [41]. We did not notice any association between smoking and sleep disturbance. That is in line with another study; the results suggest that smoking is not associated with poor sleep hygiene or sleep quality [42]. This is in contrast with a study by Wetter et al., who reported an association between smoking and difficulty initiating sleep, and symptoms suggestive of sleep fragmentation [43]. We found that 22.8% of our respondents suffered from symptoms of depression. The observed significant correlation between symptoms of depression and poor sleep quality is in agreement with other studies published in the literature [44]. Observed sleep impairment might be due to poor sleep hygiene and symptoms of depression, which showed a significant mutual relationship.
Study limitations
Our study had several limitations. The design of our research was cross-sectional in nature. As such, we cannot infer any causality based on this data. Further, in both Facebook groups where the questionnaire was distributed, some members were medical students, physiotherapists, and other rehabilitation professionals. Notably, there was also overlap between members' lists of those two Facebook groups. Practically, it was not possible to determine the exact number of unique physiatrists within those groups. The response rate could not be determined in light of those mentioned above. There are subjective (sleep questionnaires and sleep diaries) and objective (e.g., actigraphy and polysomnography) tools to assess sleep. Because our study was based on questionnaires, another limitation could be a lack of objective assessment of sleep variables. An important limitation would be the study period during the COVID-19 pandemic in 2020/2021. As such, our results might have been influenced by a different workload and stress related to the pandemic. Regarding depression, the diagnosis upon self-administered questionnaire, without in-person examination, should be taken with caution. As such, we instead preferred the term 'symptoms of depression' to describe higher scores in BDI-II.
Conclusion
The present study found a high prevalence of poor sleep quality among physiatrists. Factors associated with an increased risk of poor sleep quality were depression and sleep hygiene misbehavior. BDI-II showed a significant mutual positive correlation at the level of significance p < 0.001. Considerable efforts should be directed toward sleep hygiene behavior [45] and mental health improving in practicing physiatrists. Sleep hygiene education can be one of the options to improve sleep quality. Last but not least, organizational strategies and individual-focused interventions, and the development of health-promoting activities should be adopted to mitigate physician burnout [46] and improve well-being. One of the promising approaches can be, e.g. animal-assisted therapy [47].
Ethical approval
Ethical approval for this study was obtained from the Ethics Committee of the General Teaching Hospital in Prague (86/21 S-IV).
Informed consent
Participants consented to participate in the study before filling out the questionnaire.
Conflict of interest
None to report.
Footnotes
Acknowledgments
None to report.
Funding
This study was supported by MH CZ DRO-VFN 64165.