
Abstract
BACKGROUND:
Cardiovascular disease is amongst the top three leading causes of mortality in South Africa and the world. The effects of cardiovascular disease can be seen in limitations of function within all spheres of life, including work function. Cardiac rehabilitation programs have been documented to improve functional abilities, however further research is required with regard to activity limitation, participation restrictions, facilitators, and barriers of return to work, after cardiac rehabilitation.
OBJECTIVE:
This qualitative study aimed to determine and explore the barriers and enablers of return to work for individuals with cardiovascular disease who completed a cardiac rehabilitation program in the Western Cape, South Africa. The qualitative exploration was part of a study that resulted in a return-to-work program for individuals with cardiac disease.
METHODS:
Qualitative methodology was employed for this study. Semi-structured interviews were used with 10 participants that attended a cardiac rehabilitation program. Thematic analysis of the qualitative data was completed.
RESULTS:
The participants described the barriers and facilitators of their return-to-work process and the factors that were of critical importance in the resumption of the worker role or the result of unemployment. The four major themes were 1) Cardiac conditions negatively affect function, 2) Being unemployed, 3) Participation in ADLs and lifestyle modification enhances one’s activity levels, and 4) Return to work.
CONCLUSION:
Lifestyle modification, vocational rehabilitation and reasonable accommodation were viewed as helpful in enabling a successful return to work after a cardiac incident.
Introduction
In 2019 cardiovascular disease (CVD) was the leading cause of death globally, representing 32% of deaths globally [1]. Health economic research identifies that the burden of disease as a result of CVD is growing [2]. Therefore, the need to increase awareness of participation in cardiac rehabilitation (CR) as well as to establish preventative and management strategies is imperative for individuals diagnosed with cardiac conditions [3]. International statistics reveal that less than 30% of appropriate candidates for CR actually participate in CR programs as a result of accessibility, socio-economics, and psycho-social issues [4]. In the Western Cape, South Africa, access to CR programs are limited and restrictive in terms of financial accessibility. To a large degree referral to CR is also limited due to the physician’s lack of understanding of the role of the occupational therapist in CR. According to Hegewald et al. [5] there is limited research that focus on reporting return to work (RTW) as an outcome particularly for individuals who have completed a rehabilitation program despite research evidence indicating that CR does enable individuals with cardiac conditions to RTW [6]. Furthermore, there is a void in the literature particularly from a South African context about the experiences of individuals diagnosed with cardiac conditions about the usefulness of CR programs in enabling them to RTW as well as reintegrate to their communities.
Research aim
The aim of the current study was therefore to explore the barriers and facilitators of return to work (RTW) for individuals with CVD after they completed a specialized CR program at a secondary hospital in the Western Cape, South Africa.
Research question
What are the barriers and facilitators of return to work (RTW) for individuals with CVD after they completed a specialized CR program at a secondary hospital in the Western Cape, South Africa.
Methods
The qualitative research methodology was used to describe the experiences of survivors of CVD about RTW after participating in a CR program. The sampling technique utilized in the study was convenient sampling, at the data collection site. This type of sampling was suited for the study as all the participants who attended the CR program were eligible to be selected as part of the sample. Ten participants who were willing and available were selected to participate in the study.
Participants
Individual semi-structured interviews were completed with 10 participants from the CR program, 6 to 12 months post their CVD incident. Their ages ranged between 39 and 56 years. Only one participant was under 40-years old. Four participants were between the ages of 40 and 50, five between the ages of 50 and 60. Seven of the participants were men and three were women. All of the participants were employed in a full-time capacity in the open labor market at the time of the cardiac incident. The primary diagnoses of seven participants were acute myocardial infarction (MI) (unspecified), two participants had acute transmural myocardial infarction of the anterior wall and one participant was diagnosed with unstable angina. With regard to job characteristics, three were employed in sedentary classified jobs, two in light classified jobs, and five in medium classified jobs. According to Jacobs [7] light work can be defined as work that involves lifting no more than 10 kg, with frequent lifting or carrying of objects up to 5 kg. Medium work involves lifting no more that 25 kg, with frequent lifting and carrying of objects up to 12.5 kg. The above is in comparison with heavy work that involves lifting no more than 50 kg, with frequent lifting and carrying of objects up to 25 kg. Seven participants returned to work and three did not. The length of time away from work after the cardiac incident varied, with one returning after three months, three returning after one month, two returning after two weeks, and one returning after one week. It has to be mentioned that the type of work that the participant had to return to could have also influenced their ability to return to work. Example jobs such as driving that required physical strength and coordination may have been difficult to return to. None of the participants had private health insurance, nor received government social grants.
Procedure
In the Western Cape there are 428 public primary care facilities, 32 district hospitals, six regional hospitals, and three tertiary hospitals. The study was conducted at a district hospital in the southern suburbs of Cape Town, South Africa. This district hospital is known for its high standard of care and sees an average of 330 outpatients a day and 3000 emergency patients a month. This hospital is currently the only public health facility that offers a CR program. All patients with MI are referred for CR. At this stage other CVD are not included in this CR program. The CR program at the hospital is an education-based program, aimed at lifestyle modification. Weekly talks are arranged in a three-week cycle, which focuses on education regarding the use of medication, healthy eating, graded exercise that can be done at home and participation in activities of daily living (ADL), as well as psychological aspects that can arise after a cardiac incident. The program is facilitated by the occupational therapist and physiotherapist. Talks by consultant physicians and dieticians are included in the program. Most of the patients would participate in the CR program ranging from 2 weeks to 2 months post cardiac incident. The procedure that was followed, commenced with the collection and analysis of data for the study. The semi-structured interview schedules were predetermined and facilitated the line of inquiry. The questions focused on exploring perceptions of the participants regarding the barriers to RTW after they completed the CR program and facilitators that helped them in RTW after they participated in the CR program (see the semi-structured interview guide in the Appendix).
The semi-structured interviews were conducted after the participants completed the 3 week CR program. However, interviews would continue until no further themes or patterns emerged or data saturation occurred. Saturation occurred at the end of the interviews conducted with the 10th participant. The researchers could clearly see that recurring themes were occurring with reference to the aim of the current study. The interviews were audiotaped during face-to-face interviews which took place at the occupational therapy department or the researcher’s private office, as well as during telephonic interviews. Interviews varied between one hour and one and a half hours. The interviews were transcribed by one of the researchers verbatim. The researchers also utilized a reflective journal. The authors independently analyzed the transcriptions, thereafter a discussion would occur between the researchers in order to finalize the common themes as emanated from the study.
Analysis
In this study, Tesch’s eight steps of data analysis guided the analyzing of the data. Tesch believes that data analysis is an eclectic process [8]. The process commenced with reading all the transcripts independently by the researchers, noting down ideas that were emerging and compared thereafter. This was proceeded by the selection of one interviewee’s transcript at a time to extract meaning from the information. This resulted in similar topics being grouped together. Abbreviating the topics as codes, with the codes being noted next to the appropriate segment of text, the organized data led to new categories and codes emerging. Descriptive wording for the topics was used to develop categories. The abbreviation of each category and code was arranged alphabetically. Preliminary analysis was performed with the information from each category. The researchers identified individual codes, that were seen as units of information significant to the study, these codes were clustered into sub categories, categories and the actual themes for the study (Please see Fig. 1, describing the themes and categories). The process concluded with the actual names of the themes that related to the experiences of the research participants about RTW after a cardiac incident. The researchers conducted a member checking interview with each research participant after they conducted the collective 10 interviews with all the study participants. The member checking allowed the researchers to verify the findings of the study.
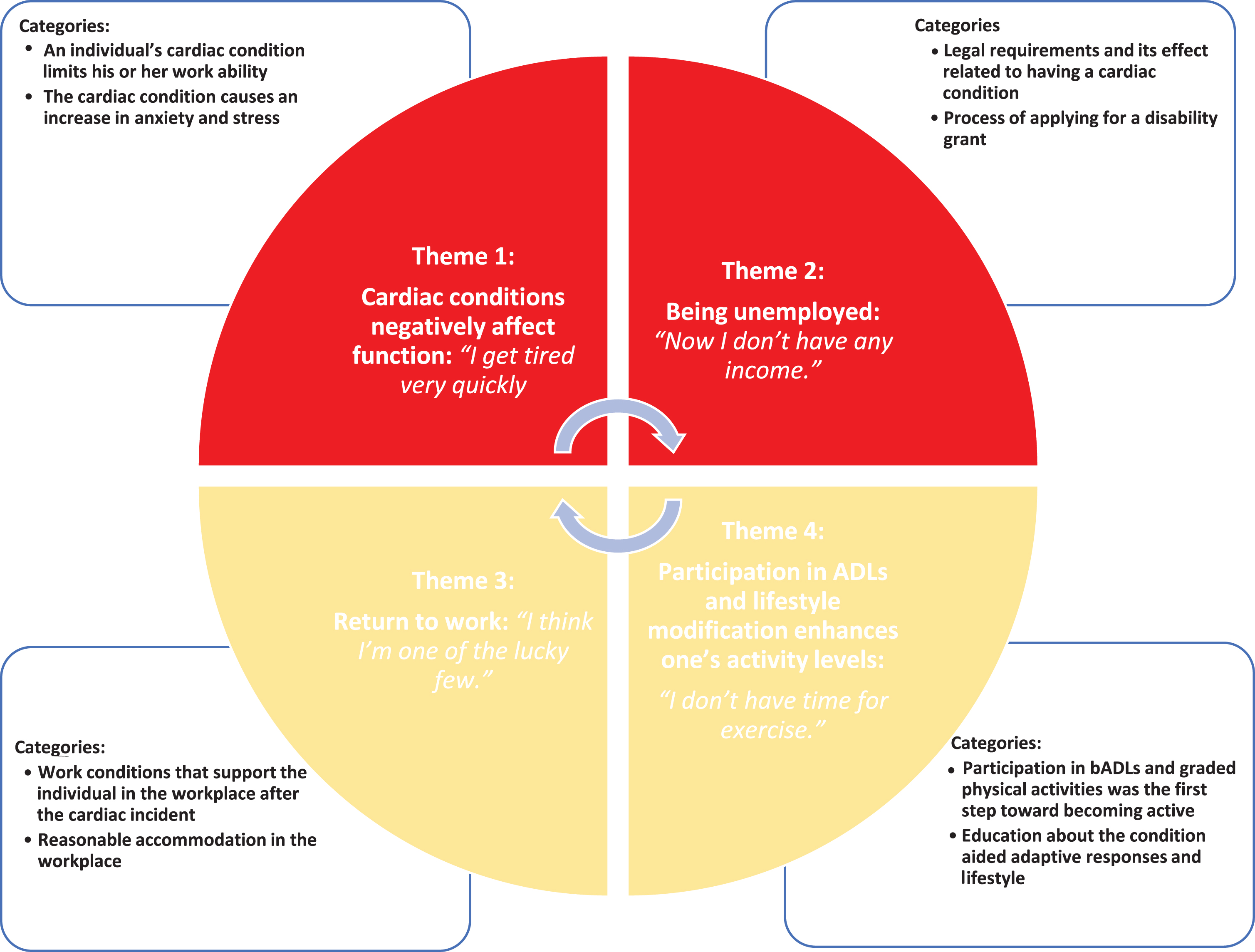
Themes and categories.
The WHO [1] ethical guidelines promoted the ethical conduct of research, through the enhancement and protection of the rights of the research participants. The researcher commenced with the study only after approval from the academic institution’s Research Ethics Committee and the Department of Health was obtained.
Results
The participants described the barriers and facilitators of their RTW process and the factors that were of critical importance in the resumption of the worker role or the result of unemployment. Four themes emerged from the study, namely,
This theme represents the participants’ physical and emotional journey after the cardiac incident, changes that occurred in their health and the need to adapt in order to return to functional work activities. The theme is described by the following categories: Category one: An individual’s cardiac condition limits his or her work ability and Category two: The cardiac condition causes an increase in anxiety and stress.
The category describes how cardiac conditions negatively affect function as well as how it limits an individual’s ability to work. One participant despondently described this change of being able to engage in work tasks when he said:
“ ... before I did all the work, now I have to manage and do less physical work and I have someone with me all the time.” P2
After the cardiac incident many participants experienced anxiety and stress, particularly when resuming their previous tasks. Participants highlighted that the cardiac incident had as much of an emotional effect as it did a physical one. One participant said:
“Once I came home, you know you tend to slow down, thinking that you know you don’t want to experience another heart attack ... So, as I said my physical condition was more determined by my mental condition.” P3
For many working in South Africa, providing for one’s family is the main priority, and the responsibility placed on the breadwinner, often supersedes any health concerns. For one participant, her inability to perform work tasks as she previously did, provoked much stress as she worried how this reflected on her ability to be an asset to the company. She said,
“I didn’t want them to think I was weak or damaged goods. And I stressed about the fact that I couldn’t work as I did before and worried about being medically boarded.” P7
This theme represents the barriers experienced after the cardiac incident when participants were not able to return to work. The theme is described by the following categories: Category one: Legal requirements and its effect related to having a cardiac condition and Category two: Process of applying for a disability grant.
The category describes how South Africa has regulations that aim to protect individuals from harming themselves in specific jobs. In particular is the law related to being medically fit before obtaining a Public Drivers Permit (PDP) in South Africa in order to continue working as a driver. The participant reported that he was not allowed obtain a PDP driver’s license due to his cardiac condition. The participant said:
“I had a PDP license but now I know I won’t qualify now. It’s dangerous because you can get a heart attack behind the wheel, then what about the passengers ... I now receive a disability grant.” P5
The category describes how individuals with cardiac conditions despite having functional limitations may not qualify for disability or ill health benefits as they do not meet state hospital criteria to qualify for a disability grant. One participant articulated,
“The doctor said that I was medically unfit to work but I don’t receive a disability grant, so now it’s very difficult financially.” P10
Participants indicated that due to not having an income, they could not purchase their medication (tablets) that was needed post cardiac incident. One participant said:
“Now I don’t have any income. I am supposed to get my tablets every month, but I can’t afford to get to the clinic so now I don’t take tablets and my heart is not doing well ... maybe getting a grant at least then I can pay transport to get to the clinic to get my tablets and to go for my appointments. Maybe if I take my tablets my heart will be better and then I can work.” P6
This theme is an illustration of how a supportive and adaptive work environment can aid the resumption of work successfully. The theme is described by Category one: Work conditions that support the individual in the workplace after the cardiac incident and Category two: Reasonable accommodation in the workplace.
The participants indicated that having an employer and colleagues that understood their medical condition helped them to adapt to their worker role. A participant said:
“Yes, they were. They actually got me an assistant. I think I’m one of the lucky few. Now that I think about it ... the conditions have changed. They actually did realize that it was a contributing factor to the heart attack. The stress, the hours and I have a huge portfolio and they realized that this was one of the reasons why I had the heart attack.” P7
The participants indicated that employers that understood the importance of their employees attending CR aided them in returning to their worker roles. A participant said:
“Well, he allowed me to attend the rehab program ... that definitely helped. My boss was very accommodating.” P1
Fundamentally when returning to work after a cardiac incident, one is not always able to resume the same pace of work and sometimes a change in work routine is needed. When this type of reasonable accommodation is possible and implemented, individuals with cardiac conditions transition back into their worker roles with ease. One participant explained that his managers understood that he had to do work tasks at a slow pace. He said,
“Yes, they do (understand). They fully support me. When I need to relax and take it slow then they understand.” P4
Another participant said,
“...he tried to streamline the work so that there is less physical strain on myself ... And even sharing tasks, divided the stress amongst those who work in the office.” P1
This theme represents the process participants pursued toward more active lifestyles after the cardiac incident. The theme is described by the following categories: Category one: Participation in basic activities of daily living (bADLs) and graded physical activities was the first step toward becoming active and Category two: Education about the condition aided adaptive responses and lifestyle modification.
Category one describes how participation in ADLs was the first step toward becoming active and that graded physical activities positively influenced their adaptation to their medical condition. One participant said,
“I could still bath and dress but had to do things very slowly with lots of resting.” P6
The participation in bADLs was also enhanced by the use of cardiac medication as described by a participant,
“Since I have been on that medication, it did help a lot.” P8
Category two describes how the participant’s knowledge about the risk factors for cardiac diseases helped them in changing their lifestyle. Participants indicated that leading a healthy lifestyle helped them adapt to life after their cardiac condition. One participant said:
“ ... it was very helpful. I learnt how to change my diet and take things a bit easier, manage my stress and stop smoking.” P5
Discussion
In the following section the enablers and barriers that affected the individual living with a cardiac diagnosis in RTW will be discussed.
Enablers
Resuming participation in bADLs and instrumental ADLs (iADLs)
The majority of participants reported in theme four, namely, “Participation in ADLs enhances one’s activity levels” that re-engaging in occupation after a cardiac incident started with the participation in bADLs, which led to the participation in iADLs, namely work and leisure. Dreyer and Dickson’s [9] editorial on RTW after MI, states that emerging research highlights the imperative nature of being able to RTW after acute myocardial infarction (AMI) as being a motivating factor in recovery and day-to-day self-care. Within this study, it was also highlighted that needing to RTW encouraged study participants to begin their journey by first participating in bADLs and then progressing to iADLs, once their strength increased.
The use of cardiac medication enables participation in bADLs and iADLs. The understanding and use of these medications are therefore integral to adapting after the cardiac incident. As mentioned in the results, interview participants found that active use of medication to control their cardiac conditions was a positive contributing factor. Bahall and Khan’s [10] study found that improved quality of life was linked to surgical intervention and the use of medication. Participation in work activities was positively viewed as a form of exercise. Many also found that participation in a leisure activity such as carpentry or gardening was more motivational than a formal exercise program. In the article discussing cardiovascular disease prevention and implications for worksite health promotion programs in Brazil, healthy physical activity was described in terms of participation in work, locomotion, household tasks, and recreational activities, since these activities could yield moderate-intensity energy expenditure that maintains cardiovascular health and in turn return to functional lifestyle and maintenance of the worker role [11]. This is in congruence with the findings of this study as participants indicated that they enjoyed participating in work and leisure activities more than formal exercise regimes.
Supportive employers and colleagues
Theme three, namely, “Return to work” highlighted how employers and colleagues that support the individual with the cardiac condition in the workplace are significant enablers to the RTW process as reported by the study participants. Similarly, Fiabane et al. [12] describe employer social support and the presence of a supportive social environment as positive factors for RTW. For employers and colleagues to be supportive, they need to be educated regarding cardiac conditions. In a study researching traumatic brain injury, employers expressed the need to learn more about the condition in order to have realistic expectations of the individual and to accommodate the worker’s needs [13]. Enhancing the insight of employers regarding the cardiac condition of their employees may enable a better adaptation to their worker role and may improve the RTW rate of individuals diagnosed with a cardiac condition.
Reasonable accommodation in the workplace
Theme three furthermore described that individuals who were diagnosed with a cardiac condition and were afforded reasonable accommodation in their workplace, experienced successful RTW. A change in work pace was usually necessitated upon RTW after a cardiac incident, which allowed the easing into returning to work for participants and sometimes changing work tasks. Smedegaard et al. [14] found that employers were more willing to accommodate employees in senior positions, who had been with the company for a longer period but stated that this was not the same for the younger employees who had more employable years ahead while being at risk. According to the Job Accommodation Network (JAN) people with heart conditions may develop some limitations but not necessarily all and therefore accommodations must be considered on an individual basis [15]. Furthermore, JAN states that accommodations to be considered for individuals with heart conditions are related to 1) fatigue, 2) balance, 3) lifting, 4) medication, 5) walking, 6) dizziness, and 7) temperature.
Attending CR
The findings of theme three, namely, “Return to work” indicated that the participants felt employers who understood the role of attending CR in the process of restoring the worker role, aided the re-establishment of this function. In a systematic review on the barriers for nonparticipation and dropout of women in CR programs, it was found that in the last decade employment restrictions were a concerning barrier to CR participation [16]. In the randomized controlled trial by Pack et al. [17] on the employment status and participation in CR, it is stated that participating in CR programs does not influence RTW, however vocational rehabilitation does. This implies that a merger between the two would be beneficial to individuals with cardiac conditions. Furthermore, in a study on patients’ expectations of RTW, comorbidities, and work capacity from CR, it was found that for participants of employable age, comprehensive CR with a focus on work capacity and vocational reintegration was a fundamental step in coping with disease [18]. Similarly, the study on RTW return to work after acute coronary syndrome states that participants of CR are more likely to RTW if work-related factors are addressed in CR programs [19]. Therefore, based on the comments of the above authors it could be argued that CR programs that are designed to suit the needs of patients and that are context specific may be viewed as being very helpful in enhancing the patients or client’s functional skills.
Pack et al. [17] also noted that being employed and being insured were predictors of CR in the USA. In the current study context and amongst study participants, all of whom were employed, none of the participants had access to insurance and only a few had sick leave to use for CR attendance. In the Pinkstaff et al. [20] article on the Affordable Care Act, which is currently implemented in the USA, they state that partnerships between employers and CR programs are mutually beneficial as they help reduce time off from work and still achieve objectives from CR when the program is implemented at the workplace. Bresseleers and De Stutter [19] express that a contributing factor to the successful RTW is communication between the healthcare providers and company physicians. Within the current study, there were no company physicians; however, communication between healthcare providers and employers could serve as a bridge between the CR and vocational reintegration process.
Barriers
Fatigue
Theme one described the barriers that individuals with a cardiac condition experiences, namely, fatigue. After a MI, fatigue is the most common symptom influencing health-related quality of life [21]. Fatigue post MI is associated with illness-related symptoms such as breathlessness and chest pain [22]. As described in theme one, namely, “Cardiac conditions negatively affect function” regarding the negative effects of having a cardiac condition, RTW for many in this study was the first indication that the cardiac incident had an effect on their function. Upon discharge, many participants thought they were adjusting well until they returned to work. For some study participants, the negative effects of fatigue on work performance resulted in the loss of jobs. In a retrospective cohort study, fatigue after a cardiac incident is seen as a typical response to the physiological healing process but is also related to psychological functioning and proper therapeutic remediation which relies on identifying underlying factors [23]. Allen and Spertus’ [24] study on the endpoint for comparative effectiveness research in heart failure also found that symptoms such as fatigue impair quality of life, inhibit the individual’s ability to perform ADLs, and may contribute to a poorer prognosis.
Stress and anxiety
Theme one further describes how increased levels of stress and anxiety after the cardiac incident were acknowledged during the qualitative interviews as a factor that affected RTW by participants. In a mid-western and southern USA multi-center comparative study of 1167 participants to determine the prevalence of anxiety, depression, and hostility among elderly patients with cardiac conditions, with a reference group of healthy elders, it was found that a higher prevalence of anxiety, depression, and hostility was associated with cardiac patient groups rather than with healthy elders, thus asserting that the higher level of emotional distress was related to the cardiac condition and not part of normal aging [25]. In a study conducted by Dreyer et al. [26], it was found that it was less likely for women to RTW due to more compromised psychosocial (depression, stress, and social support) risk profiles and having more caregiving and household demands.
The stress of having another cardiac incident resulted in debilitating anxiety and impacted the resumption of function. Dreyer and Dickson [9], in their article that focuses on the patient’s perspective of return to work after acute myocardial infarction, articulate that AMI is life-changing and is often accompanied by complex emotions, anxiety being one of them, which can impact successful recovery and return to work. Furthermore, a study done on the importance of RTW for acute coronary syndrome patients found that occupational reintegration is negatively affected by the fear of harming oneself because of work-related physical or emotional stress [27]. This study’s CR program allowed for active practice of stress and anxiety minimizing techniques during sessions and the brainstorming of how to handle real-life stressful situations with an occupational therapist. The participants in the study commented that stress and anxiety management were very helpful in preparing them for reality. The results of the current study in conjunction with studies on stress and anxiety after a cardiac event reinforce the need to address stress and anxiety in the early stages of rehabilitation and carry it through till the end stages as the stress and anxiety manifest themselves in different ways when in different contexts of life. Reibis et al. [27] likewise state that vocational reintegration of patients after AMI is less affected by the cardiac disease but rather by the psychosocial aspects such as stress, anxiety, and depression and therefore suggest that psychometric testing be done in the early stages of CR.
Description of the demographics of participants for semi-structured interviews
Description of the demographics of participants for semi-structured interviews
P*- Participant.
Theme two further describes contextual barriers that limited the individual with a cardiac condition’s ability to RTW. In theme two, namely, “Being unemployed” it is explained that legislation in South Africa regarding the return to work after injury or hospitalization does not support the RTW process and time required for rehabilitation of individuals with cardiac conditions. As a result, study participants had to risk losing their jobs while recovering or attending CR, while others returned to work when they were not yet fit to do so. Temporary disability grants are only awarded to individuals who are not fit to work for 6–12 months. Recovering from an acute cardiac incident and RTW ranged between one week to three months for this study population. This meant that some individuals on the recovery journey went to work immediately without consultation from a doctor, some took sick leave whereby others lost their jobs. During the period of recovery some individuals do not receive paid sick leave, which had a profound financial impact on their lives. Dreyer and Dickson [9] state that financial constraints in affording medication impacts on health status, which refers to symptoms, functioning, psychological factors and quality of life. The 2030 healthcare plan for the Western Cape, can facilitate the process of individuals with CVD accessing immediate and rehabilitative care. Access to rehabilitative programs can enable individuals with CVD to work towards resuming their worker role [28]. The World Health Organization (WHO) has pledged to address CVD head-on through its commitment to reduce non-communicable disease by 25% by the year 2025. In 2019 the WHO published CVD risk charts for 21 global regions to help enhance accuracy, predictability, and sustainability of effects to reduce the burden of CVD [29]. In their article on Brazil’s cardiovascular disease prevention programs, Cipriano et al. [30] state that the Brazilian government has an emergent interest in developing and promoting CVD preventative strategies through worksite health and wellness programs as a viable means to address the increase of disease burden in Brazil. Information from such projects is valuable to assist countries such as South Africa in developing their own strategies for low-middle income communities. In Canada (2001–2002), the Cardiac Rehabilitation Pilot Project (CRPP) was established to evaluate the effectiveness of a regional model of CR service, using satellite centers and it was found that 60% more patients received CR services, with an improvement in overall cardiac risk profiles [31]. The move from larger hospitals to facilities based in communities would eliminate the traveling aspect that is fundamental for a successful CR program in the Western Cape and South Africa as a whole. In Finland, the North Karelia Project was launched in 1972 and it was found that by the year 2014, CVD mortality was reduced by 84%, through the implementation of population-based prevention with cost-effective and sustainable control of CVD [32].
Financial stress
The findings related to theme two, namely, “Being unemployed” referred to the financial stress accompanied by incapacitation after the cardiac incident. For some this resulted in RTW very early after the incident in order to maintain an income. For others this meant losing their job due to no sick leave benefits and no financial support. As mentioned above, there is no accommodation in the legislation that would allow government financial support after a cardiac incident as the recovery period is too short to qualify for a temporary disability grant. In a study done in Durban, South Africa, to determine the associations between depressive symptoms in patients with MI, it was found that 51% experienced financial stress [33].
Limitations to the study
More men were represented in this sample than women therefore the perspectives of women, may be underrepresented. Only convenient sampling was possible in the study setting, this may have been a limitation of the study as study participants who may not have attended the program on a specific day would also have been excluded.
Conclusion
In conclusion, the themes derived from the semi-structured interviews illustrate the barriers and facilitators of RTW after a cardiac incident. Physical and emotional effects of the condition can hinder one’s return to functionality and therefore it is vital to address within CR. However, education regarding the cardiac condition, how to accept the changes that need to take place and learning strategies of coping has aided many individuals diagnosed with a cardiac condition to successfully RTW. Employer support is a much-needed facilitator in the process and is demonstrated to be an integral part of the RTW journey. Participation in bADLs was a stepping-stone to becoming more active, and participation in work and leisure activities was a means of maintaining a healthy lifestyle. The laws of a country can enhance or deprive individuals of successful RTW.
Ethics statement
The participants of the study were informed about the requirements of the study verbally and in writing. They voluntarily consented verbally and in writing before they participated in the study. The study was approved by the Institutional Review Board of the University of the Western Cape (Ethics number: BM 17/6/9).
Conflict of interest
The authors have no conflict of interest to report.
Footnotes
Acknowledgments
The authors would like to thank the staff (especially Dr. Nasief Van Der Schyff) and patients of Victoria Hospital (Cape Town, South Africa) for their contribution in collecting data linked to the project.
Funding
The authors obtained funding from the National Research Fund (NRF) of South Africa in order to complete the study.
Appendix: Semi-structured interview questions
Can you describe any challenges/problems that you experienced after the cardiac incident? Can you describe the challenges that you experienced when returning to work after the cardiac incident? Can you describe the factors that have helped you in the work environment? What processes did you follow when returning/adapting to the worker role? What suggestions do you have to enable other cardiac patients to better adapt to their worker role? Could you describe your coping strategies that you have used to enable your returning to work?