
Abstract
BACKGROUND:
Exposure to workplace violence is associated with physical and/or psychological trauma. Despite its significant impact, little is known about front-line workers’ experiences of preventing workplace violence.
OBJECTIVE:
This study aimed to identify what workers identify as important to preventing workplace conflicts from escalating into violence.
METHODS:
We conducted seventeen qualitative focus-group interviews with fifty-eight workers at the Danish Prison and Probation Service and psychiatric hospitals. We applied thematic analysis to identify types of violence-prevention practices, and prerequisites for successfully preventing workplace violence.
RESULTS:
We identified two main categories of violence-prevention practices, and one main category of prerequisites for violence-prevention practices. Main category A), “the individual worker’s violence-prevention practices” included the sub-categories, 1) identify the causes of workplace violence and potentially violent situations, 2) establish relationships, state rules, and set clear boundaries and 3) display empathy and communicate respectfully. Main category B), “collaborative practices for preventing workplace violence” included 4) communicate with co-workers, and share information and observations, 5) coordinate work, avoid being played off against colleagues, and support colleagues. Main category C), “prerequisites for violence-prevention practices” included 6) managing one’s emotions, and 7) having sufficient time to do the job, and being a part of a stable team, whose members know each other and the inmates/patients”.
CONCLUSION:
This study contributes to a better understanding of the interplay among individual, collaborative, and contextual aspects of preventing workplace violence. We believe that an increased understanding of the complexity of preventing workplace violence in high-risk sectors is useful when designing comprehensive violence-prevention strategies.
Introduction
Violence and threats of violence at work are encountered in many occupational fields, but in sectors with a high degree of client contact, such as prisons and hospitals, the frequency of threats and violence against staff is high [1–4]. Psychiatric or psychological conditions, frustration, anger, and fear, may cause inmates or patients to react aggressively to staff. Therefore, staff who have direct contact with these individuals need to know how to prevent critical situations from developing into violent incidents.
Exposure to workplace violence is associated with physical and/or psychological trauma [2, 6], decreased job satisfaction and work engagement, increased probability of extended sick leave, and increased staff turnover [7–9]. Despite the impact of workplace violence on worker health, information about staff experiences of preventing violence from clients is sparse. Although de-escalation techniques, are described in the literature [10–12], increased knowledge of staff experiences with these techniques as well as other practices may help improve multicomponent violence prevention in these sectors.
In this study, we investigated workers’ experiences of preventing violence in two high-risk sectors: the Danish Prison and Probation Service, and Danish psychiatric hospitals. Next, we provide a short description of these two sectors.
In Denmark, all prisons are public, and prison officers are public servants of the criminal justice system. The prison system serves various purposes: it punishes offenses and protects society from people who are perceived as dangerous criminals, but also rehabilitates prisoners, to enable them to live without engaging in criminal activity after serving their sentence. Over the years, sociologists and criminologists have described an international trend of punitive populism, which has left its mark on prison practices in many countries. Punitive populism refers to the idea that public support for more severe criminal justice policies has become a central driver of policy-making and political elections, leading to increasingly harsher punishments, regardless of their effectiveness in reducing crime [13]. A punishment-oriented criminal policy trend has led to sentences with an intensified punitive element [13, 14]. Compared to developments in the United States, those in European societies have been more rhetorical than concrete [15]. However, over the years, changing policies have also affected inmates’ conditions in Denmark, and analyses of the development of Danish criminal policy indicate that a rehabilitation-oriented policy was replaced by a more repressive policy in the 1980s, 1990s, and early 2000s. Nevertheless, the idea of rehabilitation has not yet been abandoned in Denmark [16]. Prisons in Denmark cover several wings with various security levels. In this system, the prison officers try to balance security procedures and rehabilitative activities in their everyday work with the inmates. Prison officers’ tasks are to maintain order and supervise the standardized everyday life in the institutions, follow inmates to their workplaces in the prisons, eat or spend time with them, and inspect the prison cells. The inmates in Danish prisons have various cultural backgrounds and levels of language skills.
Danish hospitals are primarily public, and have psychiatric units that provide medical treatment and care to patients with a variety of psychiatric and psychological disorders. Patients in the Danish psychiatric units include children, adolescents, and adults. People are admitted to a psychiatric unit through a referral from their physician or a specialist. In exceptional cases—for instance, if they pose a danger to themselves or others—it may be necessary to admit people who do not wish to be admitted. Once admitted to a psychiatric unit, patients are diagnosed and treated for their psychiatric or psychological conditions. Psychiatric units in some Scandinavian countries, including Denmark, have implemented systematic risk assessments to predict aggressive behavior or to avoid aggressive outbursts and minimize the risk of injury. The aim of risk assessments is to help patients control their behavior, and reduce the need for restrictive, coercive measures [17]. Coercive measures, such as mechanical restraint, seclusion, and compulsory medication, are used in psychiatric institutions to manage patient behavior that may be harmful to patients themselves or to others [18]. In Denmark, about one in four patients admitted to a psychiatric ward is subjected to coercion. This number has remained substantially unchanged in recent years, despite significant political attention and local efforts to minimize coercion (Danish Health Authority, 2021).
To summarize, in both sectors addressed by this study, the aim is to use the least possible force when treating psychiatric patients and imprisoning criminals. At the same time, staff must be ready to use force or coercion, if it is necessary to prevent inmates/patients from escaping from the institution, to maintain order, administer essential treatment, or ensure that an inmate or patient does not harm him- or herself or others. Therefore, work in both these sectors requires workers to execute everyday tasks in a way that ensures the safety of the patients/inmates, and themselves and their colleagues. However, little is known about these workers’ experiences of dealing with the challenge of workplace violence and, in particular, with preventing conflicts from escalating into violence.
Traditionally, researchers who have studied prisons or psychiatric hospitals have primarily focused on the inmates or patients, to present the effects of imprisonment and institutionalization on these groups [19–21]. However, over the years, the daily work life of staff in these institutions has received more attention. For instance, researchers have examined various aspects of the roles of prison officers, including how order in a prison is often attained and maintained through positive relationships between inmates and prison officers [22–24]. Also, research in psychiatric units has emphasized the importance of good relationships between staff and patients [25]. In contrast to the research on prisons, research on psychiatric units has focused more on de-escalating practices that prevent patients’ threats and violence [12, 26]. De-escalation is defined as “a complex interactive process by which the patient is directed toward a calmer personal space” [27], and includes four important aspects: knowing yourself, knowing the patient, knowing the situation, and knowing how to communicate [27, 28]. Besides empathy and respect, verbal and non-verbal skills, interventions (engaging with the patient, knowing when to intervene, ensuring safe conditions for de-escalation, and strategies for de-escalation) have also been identified as important aspects of de-escalating practices [29]. However, conflicting results have led recent reviews to conclude that standalone training and structured education programs have only a limited positive impact [11, 12]. Instead, owing to the complexity of the aspects that may contribute to workplace violence, it seems that to effectively combat this, organizations must implement multicomponent interventions [12]. In other words, research suggests there is a need to look not only at the individual worker’s specific de-escalation strategies, but to combine these with other workplace components that may influence the risk of violence against staff.
Despite a growing interest in the circumstances surrounding work in prisons and psychiatric units, and much information about the importance of relationships and de-escalation practices, a strong understanding of staff experiences of handling potential violence is often missing.
Quantitative studies have identified associations between work environment factors and work-related violence [30, 31], but these studies do not provide insights into what specific practices the employees find important to decrease the risk of threats and violence. Furthermore, they do not provide information about the employees’ perceptions of prerequisites to prevent violence. This knowledge is crucial, as it may increase our understanding of violence prevention in high-risk sectors, and help us to develop multicomponent interventions. Investigating this area may help to bridge the knowledge gap in the de-escalation literature discussed by Somani and her colleagues [12]: how to integrate de-escalation strategies with other strategies/components, to preventviolence.
This article aims to identify violence-prevention practices, and prerequisites for violence-prevention practices, that staff at psychiatric wards and in prisons identify as important for preventing situations from developing into violent incidents.
We used qualitative interviews with staff in the Prison and Probation Service (henceforth, PPS) and psychiatric hospitals in Denmark to answer the following questions:
What practices do workers find important to preventing situations from developing into violent incidents?
What do workers see as prerequisites for these preventive practices?
This study is based on the understanding that workplace violence is caused by several factors, and occurs between individuals in specific situations, but also occurs in a broader organizational context that may influence the incident [32]. Furthermore, this means that we must examine not only how workers explain the way they handle specific situations, but include workers’ perceptions of the roles of colleagues and work conditions, when it comes to preventing workplace violence.
Methods
We conducted a qualitative interview study to provide in-depth insight into the practices that workers find important to preventing workplace violence. We used interview data from a Danish intervention study. The intervention study aimed to increase collaboration about violence prevention in the Danish PPS and in psychiatric hospitals [33]. Sixteen institutions (eight from each sector) in various regions of Denmark were recruited for the intervention study. In this study, we use qualitative data that was collected prior to the intervention. At each of the sixteen institutions, we conducted focus-group interviews with frontline workers who interact with patients/inmates during their workday. In the PPS, the interviews were conducted primarily with prison officers; in the psychiatric units the interviews were conducted with nurses and other healthcare staff who treated adults. We conducted seventeen focus-group interviews. At one psychiatric unit, we divided the focus-group interview into two smaller group interviews, which made it logistically easier for the staff to participate. Overall, we interviewed fifty-eight workers, twenty-eight from psychiatric wards and thirty from the PPS. In qualitative studies the number of participants is dependent on the richness of the data not the number of participants. In this study, we believe, that we have collected enough data to achieve the purpose of the study and that we have achieved data saturation (Table 1).
Overview of number and participants of focus-group interviews in the two sectors
Overview of number and participants of focus-group interviews in the two sectors
The workers in each unit were selected by their manager, to ensure representation of various professional groups and levels of seniority. Most of the study participants who worked in the psychiatric units were women, whereas most of the prison officers were men, reflecting the dominant gender representation in each of these two sectors.
We conducted focus-group interviews and asked the study participants about the causes of workplace violence and existing preventive practices. To guide the conversation, we used a semi-structured interview guide, where the researcher has latitude to adapt questions to the specific direction of responses. We chose this form of interview guide to allow for new information to come up in the interviews, that the researcher did not consider beforehand and to create more intuitive and natural conversations between researchers and participants. The interview-guide consisted of general topics and the researchers asked open-ended questions related to these topics. The overall topics were: Experience of threats and violence, risk factors of violence, preventive behaviors, context of the unit. The interview guide included a question that asked the workers to describe one specific, potentially violent situation, where they had managed to prevent a violent incident, and to reflect on what they had done, what their colleagues had done, and what the management had done, and to describe conditions that were important prerequisites for these behaviors. This study is mainly based on workers’ descriptions of situations where it was possible to prevent workplace violence, but workers’ general descriptions of workplace-violence prevention from other parts of the interview have also been included.
All interviews were recorded, and transcribed verbatim. We employed a thematic analysis [34], where we began our analysis by reading each interview. Then we coded workers’ descriptions of a potentially violent situation that they had managed to prevent from developing into a violent incident. In detail, we coded descriptions of 31 specific situations. Based on the understanding that the broader organizational setting may influence an incident [32] we deductively coded 1) how the workers characterized their own behavior and 2) what their co-workers had done in these specific situation. Next, we coded 3) their descriptions of what they perceived as important conditions that enabled them to act as they had. In addition to our analysis of specific incidents, we coded sections in each interview where workers described important aspects of preventing workplace violence in more general terms, and then integrated this information into the three previously-mentioned main codes. By investigating the descriptions of the workers, we observed patterns throughout units and sectors. Based on these patterns, we developed subcategories for each of the three main categories. We decided to analyze the descriptions from the two sectors together, and without a more detailed analysis of the two sectors from which the descriptions came. We based our decision on the finding that workers’ descriptions from various units and sectors were very similar.
We obtained the study participants’ informed consent before the start of each interview, and they were informed about the use of interviews and our research project. Prior to our data collection, this study was approved by the National Research Centre for the Working Environment on behalf of the Danish Data Protection Agency (Journal no. 2015-57-0074). According to Danish regulations, the approval of the Danish National Committee on Biomedical Research Ethics was not required, as we did not collect any biological material.
We organized the workers’ descriptions of their violence-prevention practices into three main categories. Main categories A and B include descriptions that indicate which practices are needed to prevent situations from developing into violent incidents. Category A focuses on individual practices, whereas category B focuses on collaborative practices. Category C presents what workers describe as prerequisites for their violence-prevention practices. The following sections will present the detailed results of each of the three main categories and the sub-categories (Fig. 1).
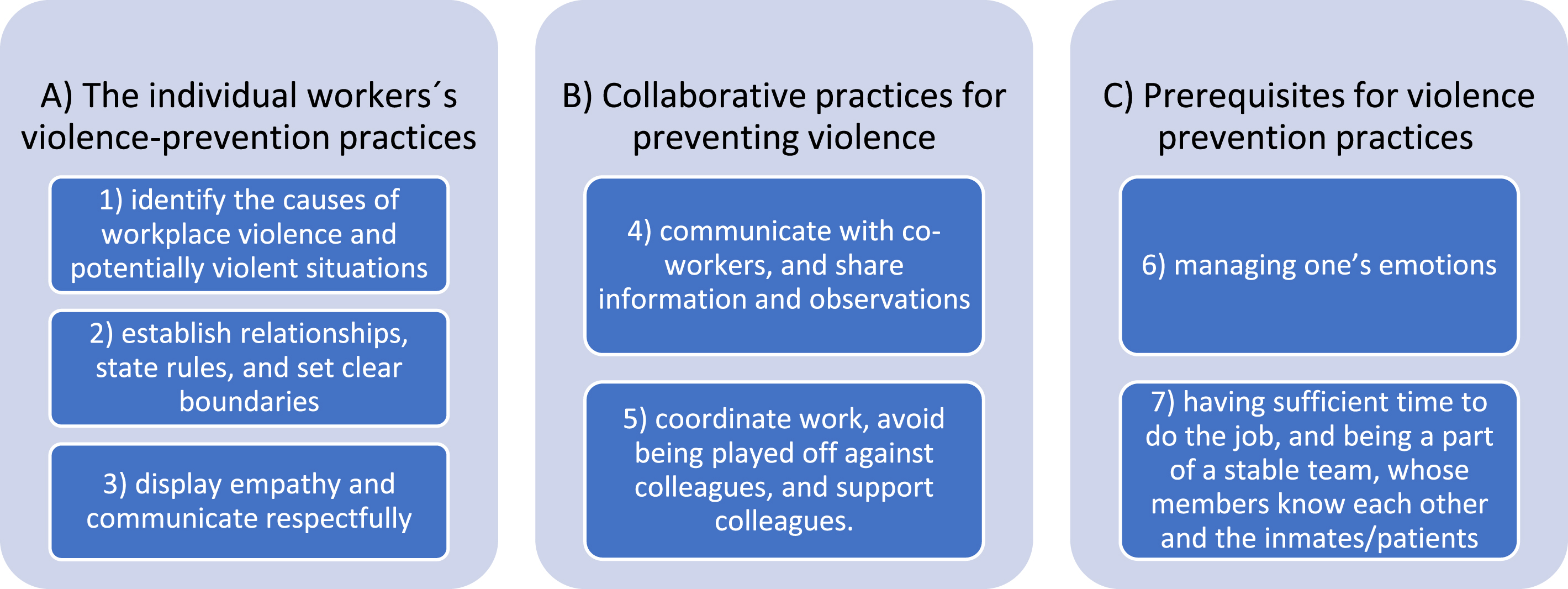
Overview of the identified three main categories and the related sub-categories.
The main category, “the individual worker’s violence-prevention practices” consists of the following three sub-categories: “identify the causes of workplace violence and potentially violent situations,” “establish relationships, state rules, and set clear boundaries,” and “display empathy and communicate respectfully.”
Identify the causes of workplace violence and potentially violent situations
Workers demonstrated a complex understanding of the causes of workplace threats and violence, and a variety of elements that they regarded as reasons why workplace violence occurs. Being able to identify these causes made it easier for them to determine where to focus their attention, to prevent workplace violence. The following three sections describe in detail how workers analyze potentially violent situations.
3.1.1.1 The patient/inmate’s emotional/mental state. Workers explained that certain of the inmates’ or patients’ emotional states may lead to threats and violence. They reported that threats and violence occur when patients or inmates are feeling unwell, are frightened or frustrated, or when they have difficulty expressing themselves. Several members of psychiatric-unit staff explained that patient threats and violence could be seen as the result of an unmet need in the treatment of their psychiatric conditions. According to these workers, their conditions cause patients’ violent reactions. Similarly, PPS staff mentioned that the circumstances have an impact on the behavior of the inmates. They mentioned drug abuse, and some of them noted that inmates who were frustrated during their confinement caused many of the violent incidents; others referenced some of the inmates’ histories of violence, meaning that reacting with violence was normal for them.
3.1.1.2 Situational/environmental causes of workplace violence. Several workers explained that inmates’ and patients’ unmet requests can lead to risky situations. Psychiatric-unit staff explained that threats and violence often occur during discussions between patients and staff about the organization of the day. Similarly, PPS staff mentioned ungranted requests as increasing the risk of threats or violent behavior from the inmates. Such situations may arise when patients refuse to take their prescribed medication. If the medication is necessary, staff may have to use force or coercion to implement treatment. Similarly, in the PPS, to avoid prison breaks or to stop violence between inmates, prison officers may use force to impose order. In these situations, the risk of threats and violence against staff may increase.
Some workers reported that the physical environment could also affect the risk of aggressive behavior. Staff from one psychiatric unit explained that dividing a ward into smaller physical spaces may be beneficial for psychiatric patients who need limited stimuli. However, it may give patients the sense of not having enough space, and consequently, they may act violently. PPS workers mentioned that being locked up in a small room makes it difficult for inmates to calm down. Some workers explained that inmates or patients sometimes influence each other to be more violent to staff, and that they sometimes pick up aggressive behavior from each other.
3.1.1.3 Planned or ordered assaults. In the PPS, threats and violence sometimes occur because of planned or ordered assaults, when an inmate lower in the hierarchy has been told by another to act violently to staff, thereby making the violence unexpected. Apart from these planned assaults, or reactions from patients/inmates that staff felt demanded specialized staff training, the workers in our study seemed confident in their ability to identify situations with the potential for threats and violence against them. This ability to understand and identify causes and potential situations seemed to be an essential aspect of their ability to prevent violent situations.
Establish relationships, state rules, and set clear boundaries
Good relationships between inmates and staff were often mentioned as the reason staff had managed to prevent situations from escalating. Staff explained that good relationships with patients and inmates made it easier to know what to do in critical situations. One psychiatric-unit worker explained, “We try to get to know the patients as well as possible [...] then we know what works (Psych 3).” Similarly, PPS staff described how developing relationships with the inmates is the most important element for preventing violent incidents. One of the workers elaborated:
If you have a good relationship with an inmate, he does not become as violent as quickly [...] If you have a good relationship, and know about him, and there is a conflict, then you can calm him down by talking with him. (PPS 7)
Another PPS worker explained how knowing an inmate makes it easier to predict his/her actions, and makes it possible to adjust communication with him/her and thereby prevent situations from developing into violent incidents. This is also addressed by this PPS worker:
We are quite good at handling them [...] And we cut them some slack when it is needed. In this unit, we know them all pretty well, and we know how to handle them. Knowing the inmates is essential. (PPS 6)
In psychiatric units, staff mentioned various ways of preventing situations from developing into violent incidents, for example, by shifting a patient’s attention to something else through simple acts, such as offering a cup of coffee or a warm blanket, to make him/her more comfortable and relaxed. In both sectors, staff mentioned that they had more positive experiences when talking to the inmates or patients, instead of being “tough,” although they sometimes had to use restrictive methods to keep behavior from escalating. Therefore, they had to be ready to implement sanctions, and use force or coercion if they perceived it as necessary to prevent inmates/patients from escaping from the institution, to maintain order, exercise treatment, or to ensure that an inmate or patient did not harm anyone. They explained that it sometimes helped to mention to the inmate/patient that certain behaviors had consequences if repeated.
Display empathy and communicate respectfully
Workers described how demonstrating understanding, and acknowledging patients or inmates were important factors for minimizing the risk of violent incidents. A worker at a psychiatric unit explained:
If you [the patient] do not feel understood, then it may escalate, and continue to smolder beneath the surface, and consequently, you get hit! So, I think acknowledgement and understanding will take you far. (Psych 2)
Another worker stated that it is important to listen to patients’ needs, and ensure that you misinterpret neither the need nor the situation, because then the situation may escalate. Similarly, a PPS worker mentioned the importance of listening to the inmates’ needs and frustrations for de-escalating situations. He explained that taking time to listen to the inmates made a great difference. The importance of displaying empathy was also stressed, when staff discussed the importance of communicating with respect. They explained that they try to understand the inmates’ or patients’ feelings, and respond to them in such a way that they feel acknowledged and respected. Moreover, they sometimes tried to communicate with the patients and inmates with a sense of humor, to change their negative moods into more positive ones.
Collaborative practices for preventing workplace violence
The main category, “collaborative practices for preventing workplace violence,” consists of the following two sub-categories: “communicate with co-workers, and pass on information and observations,” and “coordinate work, avoid being played off against colleagues, and support colleagues.”
Communicate with co-workers, and share information and observations
Staff described the importance of communicating with each other if certain inmates or patients seemed to present an increased risk of acting violently. Part of this communication was formalized, other parts were more informal. To estimate potential risk, some of the workers described how they used risk-assessment tools and scores. Some psychiatric units created patient arousal profiles and examined reaction patterns, to identify the signals displayed by specific patients. Some PPS workers described how they scored the inmates on a daily basis, so they could identify potential risks of violent behavior. Knowing the state of a patient or inmate was described as important, because it made it possible for staff to adjust their behavior and approach the inmates/patients appropriately. This is illustrated in the following statement by a PPS worker: “It is important to pass on your knowledge of things [...] then your co-workers have that knowledge, and can approach the situation in another way.” (PPS 7) Similarly, a worker from a psychiatric unit explained, “It is particularly important that we pass on the information, [...] then we are all more on guard.” (Psych 7)
Coordinate work, avoid being played off against each other, and support colleagues
Staff reported that in specific situations, they manage to de-escalate tensions by coordinating tasks and roles when approaching potentially violent patients or inmates. In the PPS they described how they coordinate the number of workers in various situations, for example, who is to be in front and leading the dialogue with an inmate, and who does what, if the situation escalates.
In general, workers were aware of the importance of avoiding a situation where inmates or patients played them off against each other. A PPS worker explained that this is not unusual: “Very quickly, they try to play us off against each other. If it is possible to get away with saying things like, ‘Usually, we are allowed to... ”’ (PPS 6) Similarly, a worker from a psychiatric unit reported, “It can easily escalate. Then suddenly (a patient may say): ‘Your co-worker allowed me to do it, why don’t you allow me to do it?”’ (Psych 1) According to staff in both sectors, it was important to avoid such conflicts by establishing a fundamental agreement among staff concerning how to manage the general aspects of the job, and under which conditions it was accepted to make some minor exceptions to existing procedures and agreements.
Staff also stressed the importance of supporting and defending each other. They reported feeling safe because they knew that their co-workers were nearby to give support. For example, this is expressed in a PPS worker’s statement: “Even though you cannot see them [...] because they are standing behind you: well, it makes you feel safe knowing they are right there.” (PPS 2) Similarly, a worker from a psychiatric unit explained, “We are deeply dependent on each other in some situations. That the co-workers come when we call for them.” (Psych 7)
Prerequisites for violence-prevention practices
The main category, “prerequisites for violence-prevention practices,” consists of the following two sub-categories: “managing one’s own emotions” and “having sufficient time to do the job, and being a part of a stable team whose members know each other and the inmates/patients.”
Managing one’s own emotions
Several workers stated that when they experienced stress, they found it more difficult to prevent situations from escalating. A worker in a psychiatric unit explained that a lack of resources or stressful work conditions sometimes led staff to use harsh language, which negatively affects the patients. One worker explained, “It is also because sometimes they push you to the limit, and [...], then you may snap the words, and then the patient becomes angry because of that.” (Psych 4) A worker from another psychiatric unit explained that if you are not calm, and you feel you lack resources and are impatient, you may express yourself in a way that you do not want to, and this may escalate situations. PPS staff also found that staff stress may affect inmates, and lead to escalations of conflicts. This is addressed in the following statements from two different workers in the same interview. One worker noted, “When you are stressed, you make mistakes. Then you say things to an inmate a bit more harshly.” (PPS 7) And the co-worker elaborated, “And this can escalate a conflict, because you are stressed.”(PPS 7)
Having sufficient time to do the job, and being a part of a stable team, whose members knows know each other and the inmates/patients
Several workers described how a lack of time affected their treatment of inmates/patients, and sometimes this increased the risk of threats and violence against them. A PPS worker explained that sometimes, if he was under a lot of pressure, and did not have the time and the mental energy, he would just “cut off and close the door” to inmates. He described how a lack of time and resources, and a lack of mental energy increased the risk of violence. This demonstrates that it may be difficult for staff to find the time to talk to patients or inmates because of heavy workload, and that this may prompt negative reactions. Staff identified another prerequisite for preventing workplace violence, which concerned the characteristics of the work group. Prison and psychiatric-unit staff explained that an experienced team of workers who knew each other, and the inmates or patients, was a prerequisite for preventing situations from developing into violent incidents. They explained how frequent staff turnover and temporary workers at these workplaces may lead to an increase in threats and violence. In such situations, patients/inmates encounter new staff with no established relationships, which are often important for managing difficult situations. Also, new staff may have different ways of approaching patients/inmates, potentially leading to staff being played off against each other.
Discussion
In this study, we identified what staff in two high-risk sectors find important for preventing workplace conflicts from escalating into violent incidents, and what staff feel are prerequisites for their violence-prevention practices. The results of our study contribute to a better understanding of the complexity of preventing workplace violence in high-risk sectors in three ways. The results nuance de-escalation behaviors of the individual worker, describe how one needs to integrate individual de-escalation strategies into what we categorized as “collaborative practices,” and contribute to a better understanding of the complexity of preventing workplace violence by highlighting the prerequisites for violence-prevention practices.
Our findings confirm, and add nuances to, the vast body of literature on de-escalation literature. Staff descriptions of preventing workplace violence resemble the findings of studies that investigate the use of de-escalation techniques, and in particular, the importance of knowing the patients/inmates, the situation, and how to communicate [28]. Moreover, this study confirms previous findings that identify good relationships as a key component of violence prevention [22–25]. Our results contribute to this literature by increasing the understanding of why these aspects are so important. Staff demonstrate that knowing the patient/inmate and his/her situation make it easier to understand their perspectives. When staff understand their inmates’ or patients’ needs, they may more easily access and handle a risky situation constructively, because this helps them to focus their attention on the aspects that are most likely to help the patient/inmate to calm down. Staff who know their inmates or patients well can better decide when to show understanding, when to “cut them some slack,” or when to invoke rules or restrictions to prevent situations from escalating. In other words, when staff can see the inmates’ or patients’ perspectives, and use these perspectives to analyze a given situation, they increase their understanding of how and why threats and violence happen, and thereby increase the likelihood of preventing violent behavior.
Our study reveals that besides the interpersonal aspects of de-escalation, preventing workplace violence sometimes involves more restrictive methods to prevent inmates/patients from escaping from the institution, to maintain order, exercise treatment, or to ensure that an inmate or patient does not harm him- or herself or others. This demonstrates that to prevent workplace violence, staff must be able to establish relationships and empathize, while simultaneously being capable and firm about implementing rules. The descriptions of balancing various strategies and being able to make the right decisions at the right moment illustrate the complexity of violence prevention in the daily practices of front-line workers in high-risk sectors. With regard to this, Price and Baker [29] also noted the importance of knowing when to intervene to mitigate violence.
Our findings help to understand how de-escalation strategies must be combined with other elements, to prevent workplace violence. As mentioned, several elements of workplace-violence prevention were defined as the way forward in a recent systematic review of de-escalation training [12]. Our study contributes to this literature on preventing workplace violence, by highlighting the importance of collaborative practices as an important element, an important aspect of preventing workplace violence. To the best of the authors’ knowledge, this aspect has not received much attention in intervention studies of workplace-violence prevention. According to the workers in our study, collaboration, and communication concerning inmates and patients, are crucial for better predicting and handling potentially critical situations. Collaboration and communication may increase the likelihood of the individual worker to introducing methods for preventing violent incidents. This finding fits into the set of risk-assessment tools for preventing workplace violence, which aim to document/present information about how patients have felt during the day, to assess the risk of aggressive reactions [17]. Our study emphasizes that communication and cooperation between colleagues go beyond formalized risk assessment, and are also found to be useful in the daily routine of communicating minor observations to co-workers. Our study also demonstrated the importance of clear agreements between co-workers, concerning how to apply rules and regulations, and thereby reduce the risk of being played off against each other. This is consistent with a recent review by Weltens et al. [35], who found that a well-functioning team was a protective factor, in terms of preventing workplace violence.
Our study contributes to a better understanding of preventing workplace violence by highlighting the prerequisites for violence-prevention practices. An interesting finding is that staff regard managing their own emotions as an important element of successfully preventing violent incidents. When staff try to prevent a violent incident, they often try to calm the patients or inmates by talking to them, communicating with respect, listening to them, showing understanding, and acknowledging their needs. That is, they empathize, to change their inmates’ or patients’ moods. However, to accomplish this, they need to control their own emotions and remain calm. Empathy and remaining calm were also identified as important factors in a recent study of violence prevention in hospitals, which identified positive approaches to, and challenges associated with managing aggressive patients [36]. Janzen et al. found that positive approaches to managing aggressive patients included behavior such as empathizing with the patient, exhibiting a calm demeanor, and not taking things personally. Our study resembles this, and describes how emotion management seems to prevent conflicts from escalating. Thus, our study contributes to the literature on preventing workplace violence by presenting violence prevention as a practice of emotion management, where staff must manage others’ emotions while controlling their own. Our study shows that such emotion management may be emotionally demanding. In some cases (when they experience stress or high workload), it may be difficult for staff to show understanding or other emotions that a situation requires of them. The discrepancy between required and felt emotions [37, 38] has been defined as emotional dissonance, and studies suggest that this regulation of feelings at the workplace increases the risk of staff feeling exhausted [38, 39] and may lead to sick leave [40]. Paradoxically, this demonstrates that successfully managing one psychosocial stressor (violence) may make increased emotional demands of the worker. However, other research indicates that emotional work does not necessarily has negative consequences for staff [41]. Schaible and Six find that empathy and seeing others’ perspectives reduce alienation and depersonalization at work, and that a professional distance in tragic events may counteract emotional strain [42]. This suggests that de-escalation initiatives could be accompanied by efforts that support workers’ management of emotional demands. Although the workers in our study mostly report successful emotion management, one interesting finding of this study is that some workers sometimes feel that they themselves contribute to workplace violence, when they fail to keep their own emotions under control. This is often due to a lack of resources, which causes stress and thereby diminishes the worker’s capacity to manage his or her emotions. Similarly, Morphet et al. found that poor verbal and non-verbal communication, and compassion fatigue (i.e., lack of empathy for patients), may contribute to workplace violence and a general attitude, including tone, which might initiate or exacerbate acts of violence [43]. Andersen et al. also found had statistically significant associations between great emotional demands and high levels of work-related violence [30]. Similarly, other studies have suggested that elevated levels of emotional exhaustion and depersonalization may well leave staff more vulnerable to assault and threatening behavior [44]. Emotional exhaustion was found to reduce police officers’ self-protective behavior, which in turn increased their risk of being victimized [9]. The link between emotion management, stress, and violence prevention calls for more attention in future intervention studies.
Our study also shows that due to occupational stress, time constraints on tasks, and the replacement of team workers with temporary workers, it is difficult for workers to implement violence-prevention techniques that prevent situations from developing into violent incidents. These preconditions at the workplace influence workers’ ability to establish relationships, manage their emotions, collaborate, and get to know the patients/inmates. The importance of contextual factors for preventing workplace violence has also been mentioned in other studies [45]. For instance, Janzen et al. noted that barriers to preventing violent incidents in hospitals included the competing needs of other patients [36], whereas Weltens described higher bed occupancy levels, busy places in the wards, walking rounds, a lack of structure to the day, and a lack of patient privacy [35] as risk factors for violence. Moreover, McKeown et al. described how staff that experience reduced staffing puts pressure on them, which has an impact on the quality of care, which in turn increases levels of frustration with patients [46]. They concluded that staffing levels were associated with perceived problems related to violence and aggression, and their attendant responses [44]. Similarly, Andersen et al. suggested that risk prevention may also demand improved work conditions for staff [31].
This study’s findings support the suggestion that workplace-violence prevention must be addressed by combining strategies that also support each other. Violence prevention should not focus only on individual skills, but also on collaborative practices and structures in the workplace. This suggests the need for a shared understanding of preventing violence in a work group, and collaborative practices where staff share information and observations, support each other, and avoid being played off against each other. Agreements between co-workers concerning the application of rules and regulations seem to affect the behavior of the individual worker. And the individual worker’s compliance with agreements may affect the collective cooperation or behavior related to violence prevention. Finally, the prerequisites for preventing workplace violence suggest the importance of leadership-level involvement, in which top-level management ensures conditions that support individual and collaborative workplace-violence prevention. Sufficient time to do the job and a stable work team that allows co-workers to effectively communicate and collaborate, and also gives them the opportunity to get to know the inmates or patients, are beyond the control of the individual worker. These important work conditions must be provided by the workplace, for staff to be able to implement violence-prevention strategies.
One strength of this study is that it is based on actual workplace-violence prevention experiences of front-line workers in two sectors that present a significant risk of violence from patients and inmates. Investigating these workers’ experiences contributes to an insight into the complexity of preventing daily workplace violence, which is missing from some of the intervention studies that attempt to improve workplace-violence prevention, as these studies tend to test the effects of a specific approach. The workers’ descriptions of violence prevention show a much more diverse spectrum of practices as usually focused on in violence prevention programs or trainings. Especially the collaboration with colleagues, the possibility of relation building and the prerequisites (in particular time and continuity of personal) that are needed for employees to actually conduct violence prevention. Our study contributes to a better understanding of the interplay between numerous aspects that successfully prevent workplace violence. This knowledge may contribute to the reduction of the risk to be exposed to violence at work, if used for the design of more comprehensive violence prevention programs. A possible limitation of this study is that we presented the workers descriptions of violence-prevention from the two sectors together, without providing a more detailed analysis of each of the sectors from which the descriptions came. We made this decision when we became aware that workers from both sectors mentioned the same general aspects. By focusing on these similarities, we have highlighted the more general experiences of workers in high-risk sectors, and therefore, see this decision as a strength that may make it possible to extrapolate our findings to other high-risk sectors. Another limitation of this study may be that we studied only the perspectives of the workers, and did not include interviews with patients or inmates. But this study developed from another study that focused on violence prevention for workers, therefore interviews with patients or inmates were outside the scope of this study. This study is based on the experiences of 58 workers, assessed through 17 focus-group interviews. There may be other workplace-violence-prevention strategies that are not captured by these interviews. However, the similarity between the two sectors confirms that we identified a number of general aspects that are experienced by staff in work places with an increased risk for violence from inmates or patients. The workers who participated in the interviews were selected by their managers, which was thought to ensure the representation of various professional groups and levels of seniority; however, this may have led to a selection bias that favored workers with more positive views/specific types of violence-prevention practices. However, the interviews revealed a variety of aspects that staff found important to preventing violence in their daily work, including staff reports that suggested that they could have done better, and descriptions of deficiencies in the work environment (e.g., not enough time). Therefore, we believe that the results are not overly biased toward positive views.
Conclusion
By analyzing workers’ descriptions of their everyday violence-prevention practices, we identified a variety of individual and collaborative practices that workers in high-risk sectors use to prevent situations from developing into violent incidents. With few exceptions covering specific situations workers feel confident about their abilities to predict and prevent most incidents of threats and violence. However, stress, lack of time or resources, and unstable teams make it difficult to prevent critical situations from escalating. The results of this study therefore contribute to a better understanding of the interplay between individual, collaborative, and contextual aspects of preventing workplace violence. We believe that increased understanding of the complexity of preventing workplace violence in high-risk sectors will be useful for designing comprehensive violence prevention strategies in Denmark and elsewhere. Although different countries will have different context that might need to be considered, we believe that all violence prevention needs to be comprehensive and cannot only focus on one particular aspect.
Ethical approval
Not applicable.
Informed consent
Informed consent was obtained from the study participants before the start of each interview, and they were informed about the use of interviews and our research project.
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
The authors would like to thank the study participants for their willingness to describe their experiences preventing workplace violence.
Funding
This study was supported by The Danish Working Environment Research Fund (grant number 24-2016-03-2016510563).