
Abstract
BACKGROUND:
Promotions in academic medicine are frequently based on number of publications and leadership positions held. While prior study has established women publish less than men, many evaluations are limited to individual specialties and do not evaluate involvement with educational activities.
OBJECTIVE:
To compare gender differences in academic output, intramural leadership positions, and educational leadership positions of academic physicians.
METHODS:
The curriculum vitae and de-identified demographic data of all permanent physicians employed at a multi-site academic medical center were reviewed from April to May 2020. Multivariable logistic and Poisson regressions evaluated leadership positions and number of publications.
RESULTS:
Of 3,359 physicians in the demographic database, 32.3% (n = 1,087) were women and 72.5% were white (n = 2,510). Of the 3,015 physicians in the curriculum vitae database, 32% (n = 962) were women. Women were more likely (p < 0.001) to be assistant professor (54% vs. 42.7%) and less likely to be associate (18.1% vs. 20.3%) or full professor (14.6% vs. 29.1%). Women assistant professors published 22% fewer articles (ratio estimate = 0.78, p < 0.001), associate professors 18% less (coefficient = 0.82, p < 0.001), and full professors 23% less (coefficient = 0.77, p < 0.001). Fewer women were program directors for residencies (1.6% vs. 2.9%, p = 0.02) or fellowships (5.4% vs. 7.4%, p = 0.04), and held fewer division or department leadership positions (OR 0.8, 95% CI as [0.6, 1.0], p = 0.03).
CONCLUSION:
Women physicians do not outperform men across any education, leadership, or publication category. A cultural shift is needed to redefine traditional metrics for leadership appointments if academic medicine hopes to achieve equity.
Introduction
Women in academic medicine hold disproportionately fewer leadership positions than men, a trend which has persisted for over four decades [1–4]. At most institutions, eligibility for leadership positions is tied closely to academic rank. As publications have long been the most important currency for academic rank, the leadership gap is often attributed to women publishing less often and with less impact [1, 2]. The persistent publication difference between genders has led to various efforts to increase women’s publications, such as more targeted mentorship, earlier exposure to formalized research training, and expanded networking opportunities [3, 6]. In addition, some have suggested academic promotions or hiring committees should view candidates’ academic activities more broadly, to include increased recognition for clinical excellence or educational endeavors [2, 8]. Such recommendations stem from the idea that women may dedicate more of their energy to these professional pursuits, and better recognition of these activities could speed women’s promotions [2, 8].
Understanding the promotion process in the workplace is important for the recruitment and retention of women in medicine. Physicians who achieve higher academic rank and leadership positions such as department chair or dean are often rewarded with larger salaries and greater access to research funding and other resources [5]. Conversely, physicians who fail to advance in academic rank and secure prestigious leadership positions within certain timelines are viewed as inept or uncompetitive, which contributes directly to burnout [9]. Overall, the failure to advance women in the workplace harms the progress of academic medicine and ultimately affects patient care.
While multiple measures have been taken to improve women’s productivity in terms of publications and leadership positions, there are few data documenting how more recent generations of women compare to older generations. In addition, gender differences in involvement with educational activities is not well studied, as published evaluations have generally been limited to individual specialties [8, 10–13]. Without these data, it is difficult to determine whether targeted efforts to increase women’s publications are likely to translate into more leadership positions, whether increasing the weight placed on teaching and educational roles is likely to improve women’s relative standing in academic ranks, and ultimately, whether either of these strategies are likely to increase the number of women holding leadership roles in academic medicine. This study aims to address these knowledge gaps. First, we evaluate the leadership involvement of women physicians compared to their male counterparts. Second, we examine gender differences in publications. We believe our study contributes valuable information to the conversation around gender equity by providing granular data on academic productivity, thereby informing the path forward.
Methods
This was a cross-sectional study of physicians currently employed within the health system of a multi-site academic medical center. All physicians are compensated using a non-negotiable structured salary-only plan; there is no tenure or additional financial incentives for publishing, achieving academic promotion, clinical productivity, or external recognition. Although many primary care services are offered, the institution is mainly a specialized, tertiary care center.
In April 2020, de-identified demographic data for all physicians were collected from human resources database, including age, race, ethnicity, gender, marital status, number of children, academic position, and full-time status. Descriptive analysis was performed.
In addition, an institutional database was accessed to review the curriculum vitae of all physicians employed at any of the practice sites. Physicians who graduated medical school more than 50 years ago were excluded. The following data for each employee were manually extracted by authors JT and SG: time to promotion to assistant, associate, or full professor from medical school graduation; number and type of intramural leadership positions held (department/division chair; department/division education, research, or practice chair); number and type of educational leadership positions held (medical school clerkship director, assistant/associate clerkship director, Accreditation Council for Graduate Medical Education (ACGME)-accredited fellowship or residency director, assistant/associate fellowship or residency program director, or medical education committee position); and publication data (number of total, first-author, and senior-author when mentoring a trainee peer-reviewed publications). Primary care was defined per ACGME guidelines as community internal medicine, family medicine, general internal medicine, geriatric medicine, hospital internal medicine, pediatrics, and primary care internal medicine. Due to the low number of physicians filling these positions, medical school deans, CEO/CME/COO and Vice Presidents were excluded from analysis.
De-identified demographic data for all physicians were collected from a separate human resources database as a single data pull. Descriptive analysis was summarized for the two separate cohorts. Median (IQR) and count (%) were calculated for continuous and categorical variables respectively with Wilcoxon rank sum and chi-squared tests used as appropriate. Median publications and total number of leadership positions held between men and women were reported in 3-year increments since medical school graduation. Multivariable logistic regression was used to investigate the difference between male and female physicians with educational leadership positions and intramural leadership positions as outcomes, individually adjusted for highest academic rank, number of peer reviewed publications, and years since graduation from medical school. Multivariable Poisson regression was applied to examine the association between the outcome number of peer-reviewed publications and physician gender, along with other independent variables including years since graduation from medical school, highest academic rank. We also investigated the interaction between physician gender and highest academic rank achieved.
All study procedures were deemed exempt by the Institutional Review Board. The analysis was conducted by SAS 9.4 (SAS Institute, Cary, NC, USA). All tests were 2-sided, and P values < 0.05 were considered significant.
Results
Within the demographic database (Table 1), 3,359 physicians were included, of whom 1,087 (32.3%) were women. Physicians identified as White (72.5%), Asian (17.7%), Hispanic or Latino (5.9%), Black or African American (2.3%), American Indian or Alaskan native (0.4%), or two or more races (1.1%). Overall, 70% of women were white vs. 74% of men. The mean age of women was 46.6 years, compared to 51.6 years for men. Most physicians were married, including 77.6% of women and 90.8% of men. Men and women had similar numbers of children (median 2.0 for both). Women were more likely to work in primary care, with 23.6% of women compared to 12.9% of men in a primary care specialty. For men and women, being married was associated with holding academic rank, including assistant (OR 1.479), associate (OR 1.709), and full professor (OR 2.09).
Comparison of physicians by gender (2020 HR data)
Comparison of physicians by gender (2020 HR data)
Missing data excluded from analysis; *: Other races included in analysis include Black non-Hispanic, Hispanic or Latino, Asian or Pacific Islander, Native American or Alaskan native. HR: Human Resources.
Within the database of curriculum vitae, 3,015 physicians were included, of whom 963 (32%) were women. Overall, women published fewer peer-reviewed articles than men, including fewer first-author and mentored senior-author articles (Table 2). Per Poisson regression, women published fewer articles than men at every academic rank, approximately 22% fewer for women assistant professors (ratio estimate = 0.78, p < 0.001), 18% fewer for women associate professors (coefficient = 0.82, p < 0.001), and 23% fewer for women full professors (ratio estimate = 0.77, p < 0.001).
Comparison of physicians by gender (2020 CV data)
Comparison of physicians by gender (2020 CV data)
1Wilcoxon rank sum p-value; 2Chi-square p-value; CV: Curriculum vitae.
When comparing median physician publications based on years since medical school graduation from 0 to 50 years, men published more than women for every cohort until 36–38 years from graduation, which was the only cohort in which women published more than men. The results of median number of publications stratified by year since medical school graduation are reported in Fig. 1.

Median number of peer-reviewed publications by years from graduation, men vs. women, 2020. A total of 3,015 physicians currently employed or affiliated as listed in the curriculum vitae database as of April 2020 were included. Median numbers of total peer-reviewed publications of men vs. women were stratified by three-year increments beginning with year of medical school graduation and ending at 50 years from graduation.
Compared to men, women were more likely to be assistant professor and less likely to be associate or full professor (Table 2). More women than men had not achieved any academic rank (13% vs. 8%). The median time to achieve assistant professor was nine years for both women and men. Women took a statistically significantly longer time to achieve associate professor (median 26 vs. 21 years) and full professor (median 43 years vs. 36 years).
After adjusting for years of service, number of peer-reviewed publications, and academic rank, there were no statistically significant differences in likelihood of holding an educational leadership position between women and men (OR = 1.20, 95% CI [0.98, 1.47], p = 0.07). Women were less likely to serve as overall residency program directors (1.6% vs. 2.9%) or fellowship program directors (5.4% vs. 7.4%), and more likely to serve as assistant or associate program directors for residency (5.1% vs. 4.6%) and fellowship (7.6% vs. 4.4%, Table 2).
After adjusting for years of service, number of peer-reviewed publication and the highest academic rank, women were less likely than men to hold any division or department leadership position (OR = 0.8, 95% CI (0.6, 1.0), p = 0.03). This persisted throughout every year since medical school graduation (Fig. 2).
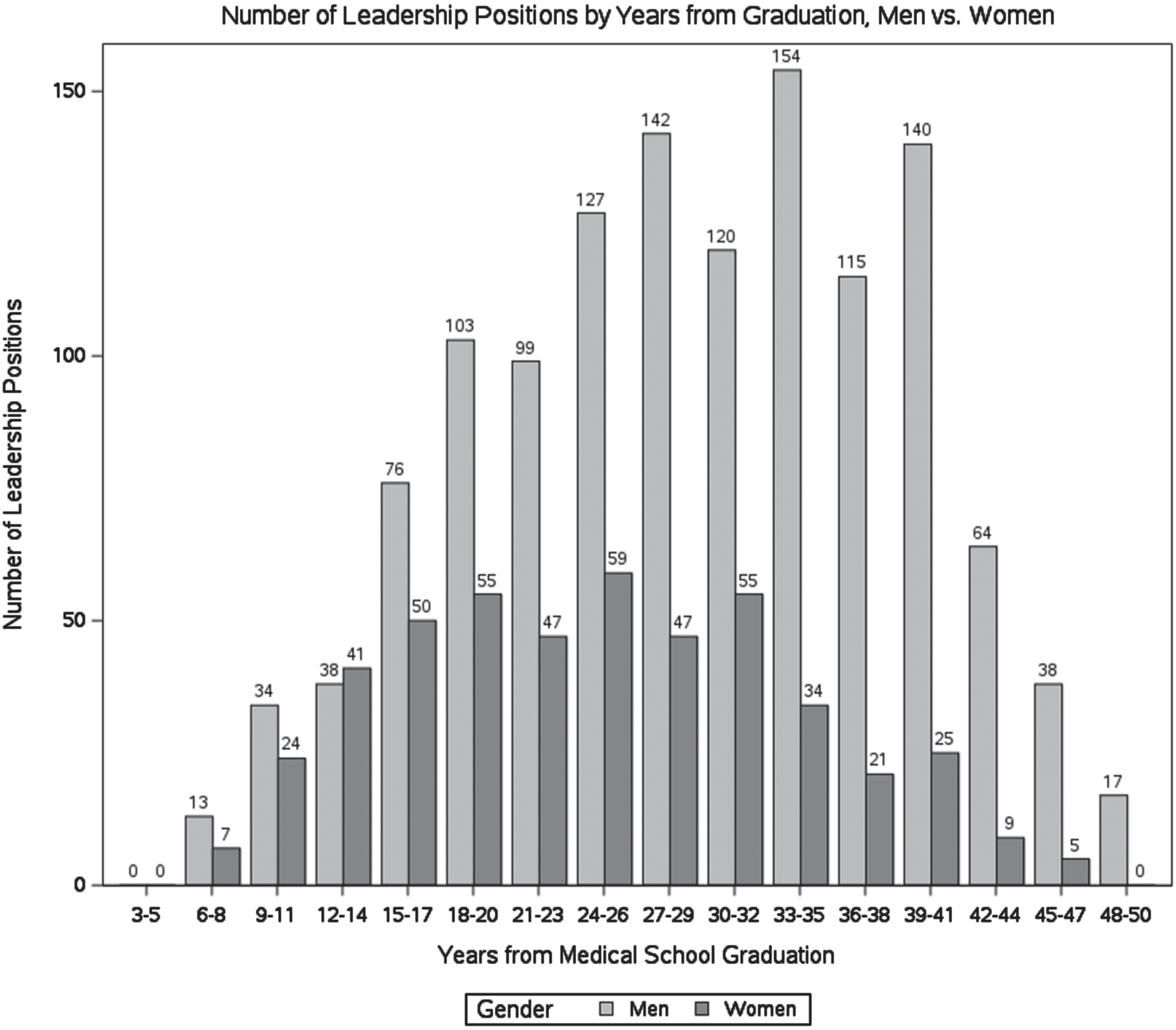
Total number of any leadership positions by years from graduation, men vs. women, 2020. A total of 3,015 physicians currently employed or affiliated as listed in the curriculum vitae database as of April 2020 were included. Total numbers of positions held by individual physicians for men vs. women were stratified by three-year increments beginning with year of medical school graduation and ending at 50 years from graduation.
This large, multi-specialty evaluation demonstrates that, when compared to men, women had lower levels of activity and achievements across all leadership, educational, and scholarly activity metrics evaluated. We specifically assessed women’s involvement in educational endeavors to evaluate previous suggestions that women physicians may be more involved than their male counterparts in the educational sphere [2, 10]. Within our data, men and women held educational roles such as clerkship director and residency director with similar frequencies, though men more often held higher-level leadership roles and women were more likely to be at the assistant or associate level. Therefore, our results do not support the theory [2, 8] that more heavily valuing educational endeavors during the leadership appointment process would help reduce disparities between genders.
When we compared results between this study and a review conducted in 2007 at the same institution, the data demonstrated minimal progress for women. The 2007 study examined 25 women physicians and 50 male physicians with at least twenty years’ experience [7]. Although direct comparisons between the studies are limited due to differences in methodology and the small sample size of the prior study, we can attempt to make some comments on positive progress over time within this institution. For example, in our sample women twenty years from medical school graduation published a median of 36 articles compared to 18 in the prior study [7]. In the 2007 study, while not statistically significant, women took longer than men to reach all levels of academic rank. In this study, women who graduated less than 20 years ago reached assistant professor slightly faster than men, though continued to reach associate and full professor more slowly. This may suggest some progress toward gender equity but also highlights that advancement to higher ranks, which are most strongly associated with leadership opportunities, remainsdisparate.
Our data also demonstrated fewer women in this health network are married, and having a spouse may be associated with holding academic rank including assistant, associate, and full professor. Other research has revealed that women, especially in specialized medical and surgical fields, are less likely to be married than their male colleagues [14–16]. A national census of Canadian physicians found no differences in reported work hours between men and women when unmarried; once married, however, women worked fewer hours than men and spent twice as many hours working from home [17]. These differences became more pronounced once there were children at home [17]. If marriage is beneficial to academic promotion, as our data suggest, men may be disproportionately benefiting.
Logistical regression model: coefficient estimates and odds ratio estimates by variable for educational and leadership positions
Logistical regression model: coefficient estimates and odds ratio estimates by variable for educational and leadership positions
There are several hypotheses as to why women are not as academically productive as men, and therefore appointed to leadership roles less often. Women may bear the majority burden when it comes to childcare and household chores, which could impact early career academic productivity, job satisfaction, and burnout, thereby making it more challenging for women to be productive in mid-career [18–20]. The socialization of women physicians in the workplace may make women less willing to pursue leadership positions, due to aversion to self-promotion, lack of mentorship, or feelings of incompetence and doubt [21–24]. Men may also be better at networking [2, 23–25], leading to greater access to leadership opportunities, workplace support, and productive publication groups which can enhance scholarly output. Consider, for example, the range of total publications for men (0 to 1233) vs women (0 to 686) in this sample. Finally, women may be hindered by implicit bias in hiring committees and in the peer review process of academic journals [3, 8].
Prior research suggests women leaders may have a more transformational and possibly more effective leadership style than men [26]. A review of thousands of business leaders by the Harvard Business Review found women were viewed–even by their male colleagues—as being more effective than men. In particular, they outscored men in drive, taking initiative, resilience, integrity, and honesty [27]. Therefore, barriers that preclude women from active engagement in leadership discussions may adversely impact institutional success and productivity. Despite these described benefits of women in leadership, this large-scale review of thousands of physicians reveals current, widespread gender disparities.
This study involves several limitations. First, although we controlled for publications, rank, age, and full-time status when comparing leadership involvement between men and women, we acknowledge there are likely many other variables which may moderate or confound this relationship. Perhaps future study could attempt to identify these variables through more detailed data sets or qualitative work. The metrics for determining leadership positions may differ across institutions and limit the generalizability of these results. Additionally, physicians or their designee provided all information on the curriculum, creating opportunities for inaccuracies. Second, demographic data were limited to self-identified gender as either man or woman, which did not allow for an inclusive analysis of non-binary physicians. Third, the demographic and academic databases could not be linked, limiting our ability to associate demographic information including race/ethnicity and full-time status with academic performance. Finally, the data are from a single institution and may lack generalizability to other institutions.
Poisson regression model: Ratio estimates between female and male physicians by rank
While the factors contributing to gender inequity in leadership positions may vary across institutions and among individuals, the persistence of these disparities despite years of attention on this problem highlights the need to reevaluate pathways to leadership in academic medicine. The current appointment process appears to preferentially reward physicians— usually men— who are able to make significant time investments early in their careers; this deters those who may have conflicting responsibilities outside the workplace— usually women— such as maternity leave, raising children, or caring for aging family members [3, 20]. The current metrics for success and leadership appointments prevent women from succeeding and may also deter young, aspiring women leaders from even applying.
In light of this, we suggest reconsidering academic rank as a pre-requisite for leadership positions. While publishing papers, earning grants, speaking at conferences, and other traditional qualifications for academic appointments are appropriately tied to academic rank, there are few data supporting the association of these metrics with performance as a leader. Rather than narrowing the leadership candidate pool by eliminating those who have not checked all the boxes to achieve the requisite rank— a strategy that disproportionately affects women— institutions should develop distinct qualifications for leadership positions that translate more directly to the requirements of the roles in question. For example, problem-solving abilities, emotional intelligence, and communication skills may be considered more important than the number of manuscripts published or grants awarded. Rethinking traditional metrics and replacing them with the traits and skills of successful leaders stands to benefit not just women but the institutions and patients around them. While other strategies to address gender disparities may add value, they may not be sufficient to meaningfully impact gender inequity without also questioning the traditions upon which these disparities have been built.
Conclusions
This large-scale analysis includes robust and granular leadership and publication data, including many physicians at different points within their careers and across a broad range of specialties. We also examined progress within this institution over time. Our results demonstrate women physicians do not outperform men across any education, leadership, or publication category despite the increased attention on these gender gaps over the past decade. A cultural shift is needed to redefine the traditional metrics for the leadership appointments of physicians if academic medicine hopes to achieve gender equity. Women cannot hope to thrive at work if the very structure in which they work is inequitable.
Ethics statement
This study was deemed exempt from institutional review board approval on 8/29/2019 (19-006122).
Footnotes
Acknowledgments
The authors have no acknowledgements.
Conflict of interest
The authors declare they have no conflict of interest.
Funding
The authors report no funding.