
Abstract
BACKGROUND:
Low back pain (LBP) is a prevalent condition frequently leading to disability. Research suggests that self-management (SM) programs for chronic LBP should include strategies to promote sustainable return to work.
OBJECTIVES:
This study aimed to 1) validate and prioritize the essential content elements of a SM program in light of the needs of workplace representatives, and 2) identify the main facilitators and barriers to be considered when developing and implementing a SM program delivered via information and communication technologies (ICT).
METHODS:
A sequential qualitative design was used. We recruited workplace representatives and potential future users of SM programs (union representatives and employers) and collected data through focus groups and nominal group techniques to validate the relevance of the different elements included into 3 broad categories (Understand, Learn, Apply), as well as to highlight potential barriers and facilitators.
RESULTS:
Eleven participants took part in this study. The content elements proposed in the scientific literature for SM programs were found to align with potential future users’ needs, with participants ranking the same elements as those proposed in the literature as the most important across all categories. Although some barriers were identified, workplace representatives believed that ICT offer an appropriate strategy for delivering individualized SM programs to injured workers who have returned to work.
CONCLUSION:
Our study suggests that the elements identified in the scientific literature as essential components of SM programs designed to ensure a sustainable return to work for people with LBP are in line with the needs of future users.
Introduction
Low back pain (LBP) is a musculoskeletal disorder defined as pain felt primarily in the lumbar region, sometimes extending to the thigh and buttocks [1, 2]. LBP is a prevalent condition worldwide that will affect as many as 9 out of 10 people in their lifetime [3]. A large number of workers are affected by LBP, with some data showing that approximately 30% of all work-related injuries involve spinal disorders [4]. LBP may lead to work disability, which can be defined as health-related problems experienced by individuals trying to do their jobs or stay at work [5].
Evidence show that a significant number of workers who have completed a rehabilitation program and reintegrated their workplace have difficulty staying at work [6]. A follow-up of these workers would be an interesting strategy to improve this situation. However, in many countries insurance policies allowing the payment of rehabilitation services while workers are on sick leave, but this support usually ends when the injured worker resumes their regular work [7]. The time immediately following return to work is particularly critical, as most relapses occur within weeks of this return [8, 9]. One systematic review estimated that at least 73% of participants who have experienced an episode of LBP will have a second episode within the next year [10]. Other studies estimate that the annual rate of recurrence of symptoms in people who have recovered from an acute LBP episode at work varies between 50% and 60%, and that disability at work recurs in 12% of them [8–10]. Thus, staying at work immediately after an episode is problematic for many workers.
Self-management (SM) programs have been shown to reduce pain, improve function and decrease pain interference, and increase psychosocial well-being (e.g., decreased stress, depression and anxiety) in individuals with chronic painful musculoskeletal disorders [11, 12]. They can also be a useful strategy to reduce the recurrence of LBP and foster a sustainable return to work [13]. In the past, recommendations have been made regarding the essential content to be included in SM programs designed to manage workers with chronic low back pain (CLBP) [14, 15]. Although interesting, these SM programs, which aim to reduce symptoms and disabilities, do not specifically address stay-at-work strategies. Our team recently developed and validated a logic model for a SM program specifically designed to help workers with CLBP stay at work [16]. The evaluation of this model by clinicians working in rehabilitation highlighted the importance of incorporating the concept of “margin of manoeuvre” [17, 18] and suggested that the improvement of the workers’ perceived self-efficacy and communication skills were essential to integrate into the SM program, to ultimately help workers with persistent and disabling CLBP stay at work.
While the development and implementation of SM programs directly in the workplace may be realistic for large organizations, such a strategy remains more difficult for small and medium-sized enterprises [19], where the critical mass of injured workers is often too small to justify paying for healthcare professionals’ services in the workplace. The use of information and communication technologies (ICT) could provide a more accessible way of reaching persons working in these settings. ICTs represent “all technologies resulting from the convergence of computer science and advanced techniques of multimedia and telecommunications, which have allowed the emergence of more effective means of communication, improving the processing, storage, dissemination and exchange of information” [20]. They are part of telemedicine and telerehabilitation, where they can be defined as “the use of electronic information and communication technologies to provide and support healthcare when distance separates the participants” [21]. One great advantage of using ICTs over traditional methods is that they overcome geographical barriers, allowing more workers to be reached directly in their workplaces, facilitating access to healthcare services, and considerably decreasing service delivery costs [22–24].
Our research group recently conducted a mapping literature review to synthesize the evidence regarding the essential content elements of SM programs designed to help workers stay at work following a long-term sick leave for an episode of CLBP [25]. These essential content elements included personalized strategies incorporated into a biopsychosocial perspective. Biological strategies include exercises, awareness of posture, and pain management; psychological strategies include problem-solving and the use of cognitive strategies such as pacing or relaxation; and social strategies include work accommodation and peer support. We also previously identified that an optimal SM program should incorporate 1) the development of essential SM skills that revolve around a problem-solving process personalized to the individual’s needs, 2) the users’ acquisition of knowledge about their condition through various education techniques, and 3) the identification and application of basic problem-solving skills as well as the utilization of resources [26].
Although this work has made it possible to establish the conceptual elements to be included in such a SM program, it remains essential, at this stage, to validate these elements with employer and workers’ representatives. Accordingly, the aims of this study were to validate and prioritize the essential content elements proposed in the scientific literature in light of the needs of potential future users (employers and workers) and identify potential facilitators and barriers to overcome when developing and implementing a SM program delivered via ICT.
Methods
Study design
A sequential qualitative design (QUAL-QUAL) was used to achieve the study objective. Data was first collected through focus groups, as this method is particularly useful for exploring people’s knowledge and experiences [27]. The focus groups were immediately followed by the nominal group technique (NGT), an approach that focuses on generating several ideas about a subject, grouping the similar ones together, and then prioritizing the remaining ideas. This method is known to minimize researcher bias, ensuring equitable participation of all group members [28].
Setting and participants
In this study, we sought the input of potential future users representing work environment’s stakeholders: employer’s (administrators) and workers’ (union) representatives. The employer and union representatives were all employed by the same large organization in the health sector. The inclusion criteria for employer representatives were: (1) workplace representatives with responsibilities associated to disability management of injured workers, and (2) ability to communicate in French (orally and in writing). The inclusion criteria for worker representatives were: (1) union representatives for a minimum of one year of experience, with good knowledge of the organization and its particularities/stakes, and (2) ability to communicate in French (orally and in writing). No exclusion criteria were set.
Recruitment process
Through purposeful sampling, 2 key-informants helped the research team to recruit potential participants. Thirteen (13) potential participants were solicited by the research team. Eleven (11) responded and showed interest in the project, while the other 2 were not available for the proposed date. The meeting took place with the 11 interested and available participants during regular working hours.
The recruitment period lasted for 3 months (beginning of July 2017 to end of September 2017).
Data collection process
The data was collected by two experienced researchers (coauthors YTL and GL) and a research assistant (CL). The group session was recorded in digital audio mode and lasted for approximately two hours.
After obtaining informed consent, all participants completed a questionnaire that collected information about their age, subgroup (employer or worker representative), and years of experience in their position. The group session was then divided into three phases. For the first two phases (contextualization of the project and presentation of the essential content elements of an SM program based on the scientific literature), data was collected through a focus group technique, whereas for the third phase (potential usefulness of ICT for delivering a SM program), the NGT was used. The combination of those two approaches allowed us to determine the relevance of the essential content elements proposed in the scientific literature, which lead to adding, removing and prioritizing ideas accordingly.
Phase 1: Contextualization of the project
The project context was presented to the participants (Fig. 1). The group was then asked if the contextual elements presented were representative of their workplace realities and were invited to add additional contextual elements posing challenges for workers suffering from CLBP. Participants answered these questions individually, in writing.
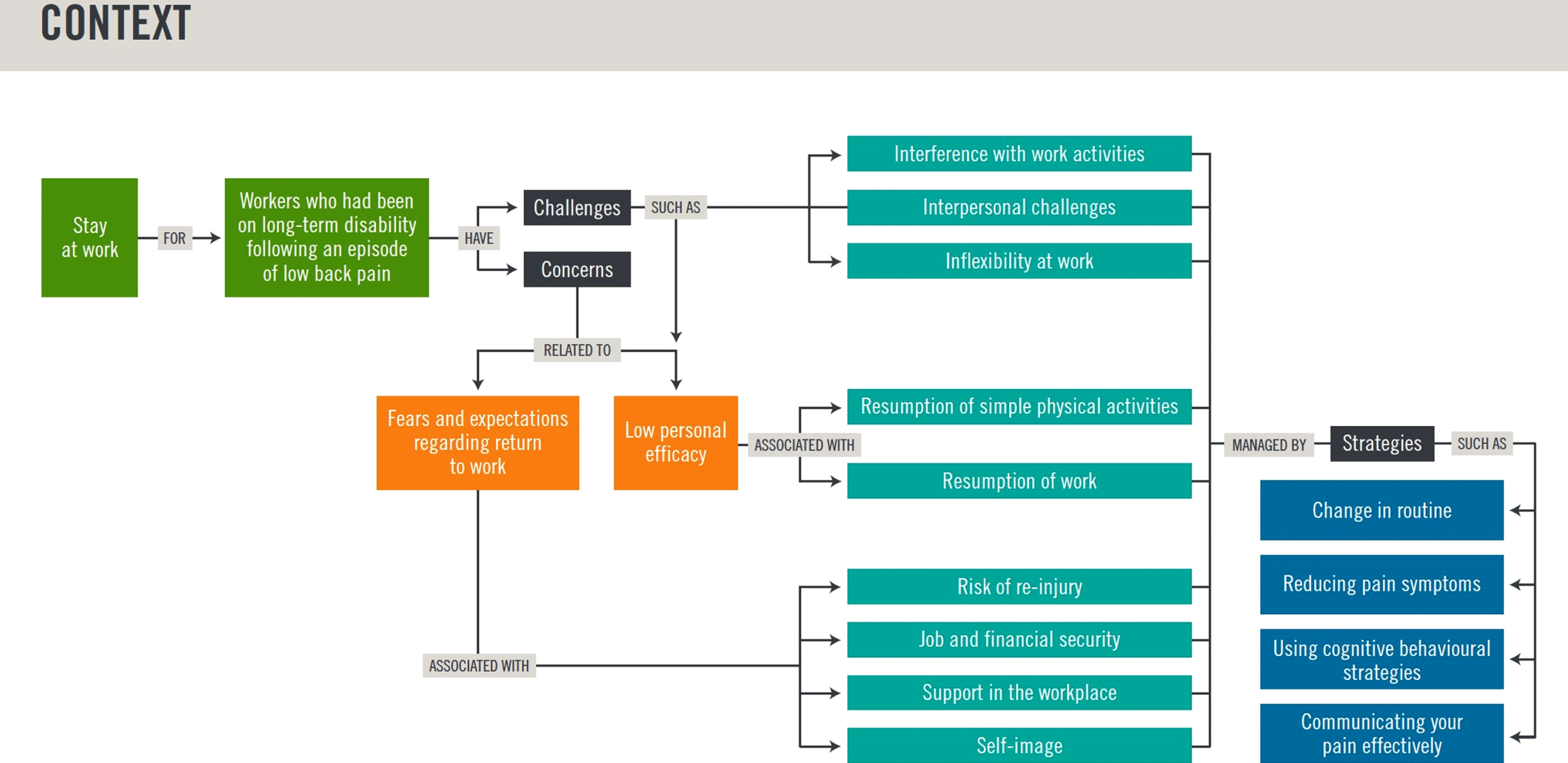
Contextual elements presented to the participants.
The essential content elements of a SM program, as determined by the research team on the basis of scientific literature [25], were then presented to the participants. The overall objective of the proposed SM program was to develop workers’ SM skills to support their sustainable return to work following a disabling episode of LBP that required long-term sick leave. The specific objectives were to give workers the skills they need to: (1)understand the problem; (2)learn ways to control it, and (3)apply SM principles/strategies in everyday life. The fourth specific objective was to foster the injured workers’ motivation (an important factor in the success of the three previous specific program objectives). The findings of our mapping review [25] were presented in relation to each specific objective (see Fig. 2).
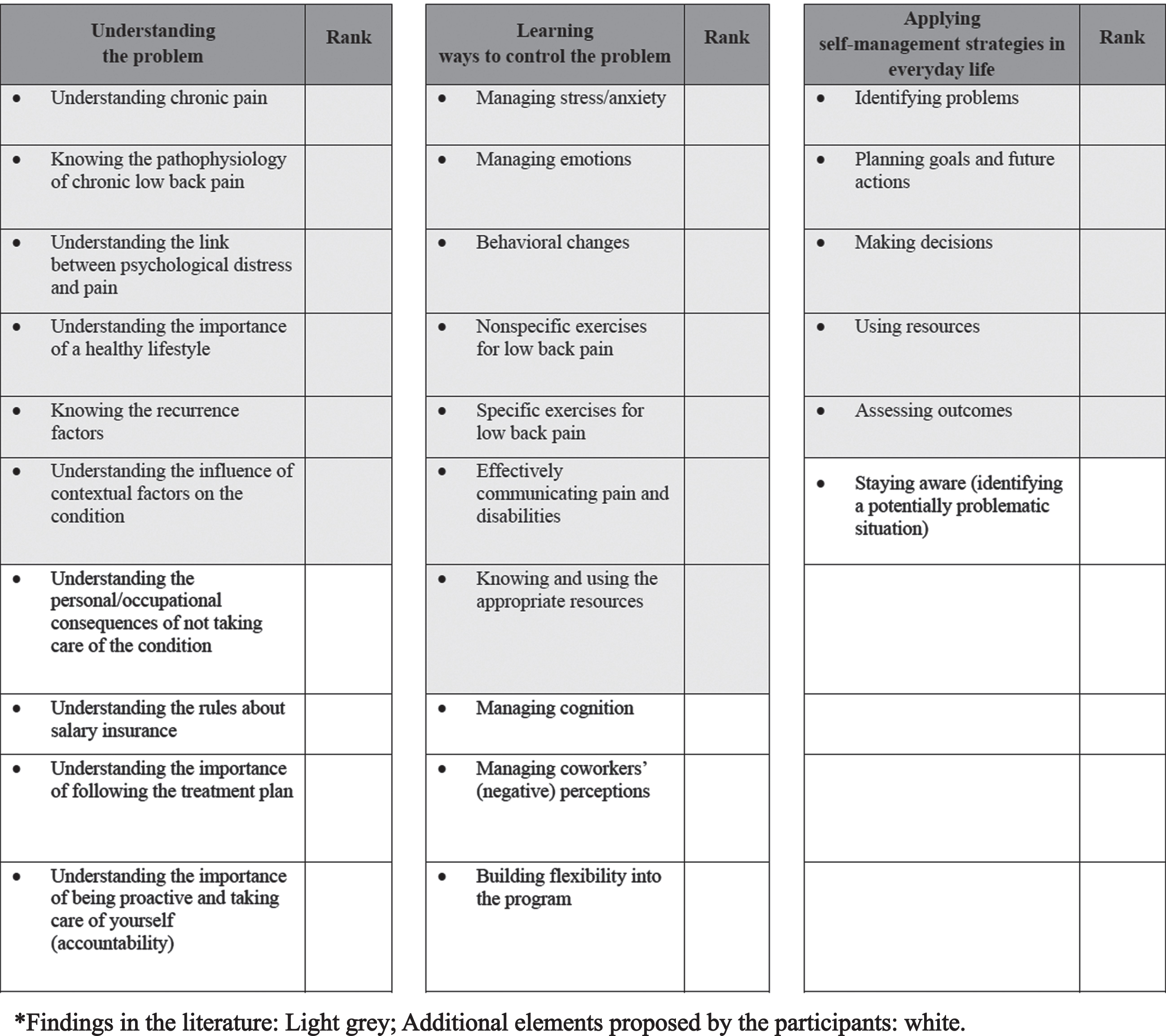
Summary sheet used with the participants to prioritize the essential content elements to be included in a self-management program designed to ensure sustainable return to work of workers following long-term sick leave due to low back pain.
Next, for each broad category of content elements, participants were asked to validate the relevance of each element and to add other elements they thought should be included in a SM program. They were then asked to individually prioritize the elements pertaining to each broad category (i.e.,Understand, Learn, Apply) on a sheet of paper, and to determine the optimal relative proportions (expressed as percentages) of each of the three broad categories mentioned above that a SM program should contain.
The research team discussed the potential usefulness and challenges of ICT as a means of delivering a SM program. They suggested that the program could be delivered via a website and/or be made accessible on several platforms (tablet, smartphone, laptop, offline and online use). They also provided examples of what could be included on the website/platforms.
In light of this presentation, the research team used the NGT to elicit the participants’ thoughts and priorities regarding possible facilitators of and barriers to the use of ICT in the workplace [29]. Participants had to write each of their ideas on a separate piece of paper (one idea per sheet). Next, they took turns sharing one of their ideas with the group. The process continued until there were no new unshared ideas. Similar ideas were pooled to form categories. Each participant was then asked to rank (prioritize) the elements in each category.
Lastly, participants were asked individually (1) to propose solutions to the previously identified barriers and (2) whether they thought that a smartphone or tablet-accessible website or application would be a realistic way to reach workers in their workplace (yes or no, with explanations).
Data analysis
This section details the methods used to analyze the data according to different steps of the project. Data obtained from the focus group were both qualitative and quantitative. Qualitative data refers to the addition of new content elements to the SM program, while the prioritization of the content elements or determination of the optimal proportion of each of the broad categories were analyzed quantitatively.
For Phase 1, the participants had to rate the relevance of the contextual elements presented by the researchers on a scale from 0 (not relevant) to 100 (extremely relevant). Results for the phase 1 are presented as means and median level of agreement scores.
For Phase 2, participants had to prioritize the list of content elements pertaining to each broad category; all elements – including the elements presented to the participants and those proposed by them – were ranked from the most important to the least important by each participant. Each element was then scored by totalling the ranks given to it by all participants, with the highest total score being attributed to the most important element (i.e., rank 1). For example, for the categoriesUnderstand andLearn, which included 10 elements each, 10 points were awarded for rank 1, 9 points for rank 2 and so on, down to 1 point for rank 10. The same method was used to score the broad categoryApply (6 elements). Finally, the optimal proportion of each broad category (Understand,Learn,Apply) of content elements in a SM program was estimated on a scale from 0% to 100%, where the sum of 3 proportions (each expressed as a percentage) had to total 100%.
For Phase 3 (identification and prioritization of factors facilitating or hindering of ICT), the quantitative aspect of the NGT – which relates to the prioritization of content elements via the assignment of a rank – was used to ensure that each element had the space it deserved in the program [30]. For the prioritization of the factors facilitating or hindering the use of ICT, rank 1 was attributed to the most important element. The same method that was used for the content elements (see above) was used to score factors facilitating (8 elements) and hindering (5 elements) ICT use.
Results
Characteristics of participants
Of the 11 participants who agreed to take part in the study, 7 were employer representatives and 4 were union representatives (same union). Nine (9) of the 11 participants answered all questions regarding age, and years of experience. These 9 individuals were between 30 and 60 years of age (average age: 47) and most were women (8 out of 9). They averaged 15 years of experience in their position. For the purpose of this study, representatives of both categories were grouped and presented together – they will subsequently be referred to as “workplace representatives”.
Relevance of the contextual elements
The average level of agreement with the contextual elements presented was 78% and the median level of agreement was 87%. Participants reported additional contextual elements that they thought should be considered during the program design phase. These elements included workers’ return-to-work motivation, pain management abilities, worker’s perception of his or her condition, and employer’s failure to comply with the return-to-work conditions.
Prioritization of the content elements
The elements that had to be prioritized for inclusion in a SM program comprised those found in the literature and those proposed by the participants.
Understand
Table 1 shows the results of the workplace representatives’ prioritization of the content elements in theUnderstand category.Understanding chronic pain, Knowing the pathophysiology of chronic low back pain, andUnderstanding the link between psychological distress and pain were ranked (in this order) as the top three elements.
Workplace representatives’ prioritization of the content elements in the “understand” category
Workplace representatives’ prioritization of the content elements in the “understand” category
Exercises for low back pain, Behavioral changes, andManaging stress/anxiety were ranked (in this order) as the top three content elements in theLearn category. Table 2 shows the complete results of the workplace representatives’ prioritization of the elements in this category.
Workplace representatives’ prioritization of the content elements in the “learn” category
Workplace representatives’ prioritization of the content elements in the “learn” category
Table 3 shows the results of the workplace representatives’ prioritization of the elements in theApply category.Identifying problems andStaying aware were ranked (in this order) as the two most important elements.
Workplace representatives’ prioritization of the content elements in the “apply” category
Workplace representatives’ prioritization of the content elements in the “apply” category
Working individually, participants estimated the optimal proportion (percentage), of each category of content elements to be included in a SM program. Based on all the results combined, the group thought that the optimal proportion of each category would be 40% forUnderstand, 27% forLearn, and 33% forApply.
Factors facilitating and hindering the use of ICT to deliver SM programs
Table 4 shows the facilitators and barriers identified by the participants regarding the use of ICT to deliver SM programs. More facilitators (n = 8) than barriers (n = 5) emerged from the nominal group. Notions related to time and access appeared in both categories. These notions figured among the top three facilitators and barriers.
Factors facilitating and hindering the use of ICT to deliver self-management programs
Factors facilitating and hindering the use of ICT to deliver self-management programs
Proposed solutions for the barriers to the use of ICT
Participants were asked to propose possible solutions for the barriers raised by the previous questions (section 3.4). Twenty-seven (27) solutions were initially proposed; similar solutions were grouped, reducing the final number to 10. Table 5 shows these solutions and the constraints they aimed to resolve. All the participants (100%) reported that a website or an application would be a realistic way to reach workers in their workplace. However, many of them expressed concerns. Most cited the importance of including facilitators in the process of finding solutions to the barriers previously identified. Only 1 participant expressed a doubt that did not refer directly to the facilitators or barriers: the potential difficulty of using technology for some individuals facing computer literacy challenges.
Proposed solutions for barriers to the use of ICT
Proposed solutions for barriers to the use of ICT
The aim of this study was to validate and prioritize the SM content elements identified in the scientific literature to support workers’ sustainable return to work following a disabling episode of LBP. Content elements were divided into three broad categories: (1) understanding the problem; (2) learning ways to control the problem; (3) applying self-management principles and strategies in everyday life. The study also sought to identify the main factors facilitating and hindering the use of ICT according to potential future users of a SM program in a workplace context within public healthcare system.
Based on the high percentage of relevance found in Phase 1, the essential content elements of an optimal SM program that were identified in the literature appear to align with potential users’ needs. We also found that ICT appears to be an effective mean to deliver SM programs, according to stakeholders. The factors identified by our study participants as facilitating or hindering the use of these technologies and the solutions they proposed concurred with those identified in the literature [31, 32]. These elements should be considered when developing and implementing such programs.
Contents of the program
Most participants (∼80%) agreed with the contextual elements, i.e., they agreed with the previously identified needs and concerns of future users and stakeholders. The additional ideas proposed by the participants (i.e., understanding the importance of being proactive and taking care of yourself, managing coworkers’ negative perceptions) could help improve the list of contextual elements, while increasing our understanding of the context surrounding the problem, thus positively influencing the development of future SM programs.
When comparing our results, we observe that participants’ prioritization of the content elements is consistent with the results of a recent mapping review conducted by our research team [25]. This review highlighted that the patients need specific physical and cognitive strategies to support a sustainable return to work, and that improving the patient’s understanding of their condition is an important part of SM programs. But perhaps the key point is outright and simply self-efficacy – patients must have confidence in their capability to “apply” these strategies in order to manage their condition and, ultimately, stay at work.
Still, one element identified by the participants – and not explicit in the literature – was ranked as one of the two most important: Staying aware from the Apply category (which was ranked second). This observation could be explained by the meaning of Staying aware, as it was defined by the participants as “being able to identify a possibly problematic situation”. Hence, for our study participants, Staying aware represented the step prior to Identifying problems.
The three categories (Understand, Learn, Apply) were almost equally important for the participants, although Understand appeared to be somewhat slightly more important than the other categories. This highlights the importance of having a good understanding of the problem before trying to apply problem-solving strategies. This finding is comparable to the results of Heisler et al. [33]. Although their findings were found in a context of diabetes self-care, it is interesting to note that these authors observed that self-management was strongly and independently associated with a greater understanding of the disease [33]. Yet, understanding (enhancing knowledge) is not sufficient. Patients need specific strategies to help them manage their pain and disability and need to learn to apply these before they RTW [16]. These strategies could also be facilitated by a supporting work environment. When needed, for example, employer could use a tool adapted for workplaces (TS-GRTW) [34], to promote the margin of manoeuvre. This concept represents the opportunity or latitude a worker is given to develop different work methods in order to meet production requirement without harming his or her health [35].
Use of ICT
Based on our mapping review [25], it appears that the benefits of ICT (effectiveness in delivering the message, being able to reach workers directly at their workplace, and allowing the collection of large amounts of valuable data) are viewed positively by governments, administrative boards and researchers, which is not necessarily the case for users. The results of our study extend beyond the results of our mapping review [25], by describing workplace representatives’ views of the factors facilitating and hindering the use of ICT to deliver SM programs. The most important facilitators and barriers revolved around three main themes: access, time, and computer literacy.
These themes (access, time, and computer literacy), which refer to ease of use and familiarity with technology, are convergent with previously reported results in three previously published reviews, including two systematic reviews [36–38]. One of these reviews focused on factors and barriers to the implementation of ICT use by healthcare professionals [36], while one of the other two reviews documented the barriers and facilitators of implementation of shared electronic health records among various users (physicians, healthcare professionals, workplace representatives and patients) [37]. As reviews synthesize the findings of many studies, many more barriers and facilitators were identified in these publications. However, the barriers and facilitators identified by these authors are not entirely applicable to SM programs, as population and contexts are unique. For example, implementing a program for employers returning to work after long-term sick leave can be less demanding and costly than implementing electronic medical records. It should also be mentioned that none of these reviews prioritized barriers and facilitators, as this study does.
Strengths and limitations
One important strength of this study relates to the involvement of stakeholders of SM programs in the validation (based on their own perceived needs) of content elements found in the scientific literature. In addition to improving the content of SM programs, early involvement of stakeholders should help promote the implementation of such programs within organizations. To our knowledge, this is the first time that the content elements of a SM program for CLBP and the facilitators/barriers to ICT use have been prioritized by potential stakeholders. Their prioritization of the content elements could potentially and significantly contribute to the development of SM programs that are in line with users’ needs. We believe that the mixed methods used to collect data (focus group and NGT) and the type of data collected (both qualitative and quantitative) bring more depth to the results.
One important limitation of the study was the absence of workers in the sample of participants. As the target population of this study was workplace representatives, it would be relevant to validate these results with workers. Still, the inclusion of union representatives can help compensate in part for the absence of workers and suggests that our results can provide a solid foundation for the next steps. Because of the small number of participants, some results may not be generalizable to all future users of SM programs and should be considered as exploratory. Moreover, our results apply primarily to the health sectors. Future projects, involving different (or diverse) sectors could be beneficial to generalize the findings to other contexts.
Practical considerations
Our results support the development of self-management programs based on stakeholders’ needs and solid scientific knowledge. A positive perception of the use of ICT is reassuring as to the relevance of deploying them to deliver such programs. As the most important facilitators and barriers revolved around three main themes (access to the technology, time and computer literacy), it is probably better to address these barriers during the development of an ICT-based web application (versus addressing thema posteriori), keeping in mind that any ICT-based web application should be field-tested before it is implemented.
Conclusion
Our findings suggests that the elements identified in the literature as essential components of SM programs designed to ensure a sustainable return to work among workers following long-term sick leave due to LBP are in line with users’ needs. We divided these elements into three broad categories:Understand,Learn, andApply. For potential users,Understand is the category that could be considered the most important component. They considered ICT as a very effective way to deliver this type of program, providing that facilitators and solutions for the barriers (such as lack of time or of access to technology) are available.
Ethical approval
Ethical approval for this study was granted by the CIUSSS Estrie – CHUS Ethics Review Board (#2018-2524).
Informed consent
All participants gave their informed consent prior to the meeting.
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
The authors gratefully acknowledge Amélie Loiselle for her help with this research project.
Funding
This work received financial support from the Quebec Rehabilitation Research Network (REPAR) and theInstitut de recherche Robert-Sauvéen santéet en sécuritéau travail (IRSST). GL is supported by the Fonds de recherche Santé (FRQ-S, Québec, Canada). CL received a scholarship from REPAR, the IRSST and theOrdre professionnel de la physiothérapie du Québec.