
Abstract
BACKGROUND:
Active patient engagement and adherence are essential for successful rehabilitation outcomes, particularly in complex cases such as work-related musculoskeletal injuries. Although the therapist-patient relationship is a significant component of successful care coordination, there has been limited examination of this relationship within upper extremity musculoskeletal rehabilitation.
OBJECTIVE:
To explore therapists’ perspectives on how the therapist-patient relationship intersects with engagement and adherence in the provision of holistic and collaborative rehabilitation services.
METHODS:
Data were collected from four therapists over three months. Descriptive statistics were generated from the Sport Injury Rehabilitation Adherence Scale (SIRAS) and the Rehabilitation Therapy Engagement Scale (RTES) completed by therapists following visits from a sub-sample of patients (n = 14). Weekly semi-structured group interviews (n = 13) were analyzed using an iterative grounded theory-informed process. Emerging themes were identified, refined, and situated within the context of quantitative results.
RESULTS:
SIRAS scores averaged 14.4 (SD: 1.0) and RTES scores averaged 42.5 (SD: 3.5), indicating high perceived patient engagement and adherence. Four themes emerged from therapist interviews: (1) dynamic power; (2) co-constructed engagement; (3) emotional states; (4) complementary therapy contexts.
CONCLUSION:
In this engaged and adherent setting, therapist-patient relationships were complex and intimate, and extended beyond education and physical interventions. Careful management of this relationship was central to active patient participation and engagement. Incorporating holistic techniques may provide more structure for managing and communicating these aspects of care. These findings provide a preliminary understanding of the impact of therapeutic relationships on engagement and collaborative care.
Introduction
Collaborative and holistic approaches to physical rehabilitation have been highlighted in recent literature in conjunction with patient-centered care patient reported outcomes [1–3]. Within this paradigm, patients are viewed as engaged collaborators situated within unique personal contexts [4–6] and adherence has replaced compliance as the medium through which to achieve positive therapeutic outcomes [5, 7]. The practitioner-patient relationship has been identified as crucial to adherence [5, 9], patient-centered goal-setting, and positive patient outcomes[10–12].
Therapeutic relationships develop from the interaction between individual factors of each healthcare provider and patient [5] and, together with dynamic states of engagement and adherence, create a complex and interdependent system best explored at the level of these interactions, rather than as a sum of individual components [13–15]. That is, therapist and patient contributions to the therapeutic relationship (and their interaction with engagement and adherence) are inseparable aspects of a shared process within the context of rehabilitation.
For patients with work-related upper extremity (UE) injuries, active patient engagement and adherence within this complex system are especially critical for successful functional outcomes. The consequences of nonadherence for patients with conditions commonly treated in UE rehabilitation can be devastating and costly [16–18]. For this population, successful return to work and other meaningful activities is a multifactorial process that requires not only physical improvement [19, 20], but also consideration of widely varying patient presentations, experiences, and contexts [21, 22]. It is imperative that therapists work with patients to develop safe and efficacious treatment plans that are also realistic and sustainable within patients’ unique circumstances. Furthermore, limited reimbursement, visit frequency, and treatment duration for physical rehabilitation demand strategic approaches to efficiently work toward optimal outcomes that matter to patients’ work and home lives and empower patients to continue recovery after discharge [17, 24]. As UE rehabilitation continues to work toward evolving beyond singularly biomechanical approaches [6, 25–28], it is pertinent to critically re-examine the therapist-patient relationship and its impact on active patient engagement and adherence within these settings.
Multiple studies have explored the therapist-patient relationship in rehabilitation settings [15, 29]. These relationships have been reported to influence patient adherence [8], help clinicians understand patients’ illness experience through empathetic listening [30], and facilitate patient expectations of active roles in therapy [31]. However, few studies include detailed analyses of evolving relationship processes. In fact, only one narrative analysis explored the therapist-patient interaction in one dyad, finding that the therapist was primarily responsible for creating an environment in which this relationship could develop, but that equal contributions resulted in a successful therapeutic experience and outcome as compared to unidirectional instruction and acceptance [32]. Despite these foundational and emerging theories from other rehabilitation settings, there is a paucity of research examining the details and mechanisms of this relationship in UE rehabilitation.
Purpose
This study explored the perspectives of therapists specializing in upper extremity musculoskeletal rehabilitation to identify factors within the therapist-patient relationship that facilitate collaborative therapeutic engagement and active patient participation.
Methods
Design and participants
This observational study was conducted over a 3-month period at a university-affiliated, hospital-based, outpatient hand therapy clinic to elicit therapists’ perspectives on the therapeutic experience. We used a parallel, mixed-methods design [33], collecting both qualitative and quantitative data across the study period. This study was conducted in compliance with ethical standards set by the Office for the Protection of Research Subjects (OPRS) and Human Research Protection Program (HRPP) as approved by the institutional review board of the University of Southern California (HS-16-00148, approved 3/14/2016). All participants provided informed consent.
A convenience sample of four occupational therapists working full- or part-time within the hand therapy clinic were recruited at the beginning of the study. Therapist 1 was a woman in her mid-50s at an advanced stage in her career in UE rehabilitation and with a post-professional doctorate in OT. Therapist 2 was a woman in her late-30s mid-way into her clinical career and with a Bachelor of Science in OT. Both therapists were clinical faculty at the university and held the title of CHT. Therapists 3 and 4 were male and female post-professional OT doctoral students completing their residencies at the clinic. As study participants, therapists did not receive additional training and their typical care practices were not altered.
A sample of patients being treated by the therapists at the hand therapy clinic were also prospectively enrolled to enable discussion and data collection related to therapy sessions during the time of the study. Patients did not directly participate in the data collection described in this manuscript. Patients were recruited if they met the criteria of: at least 18 years old, English-speaking, access to a computer with internet, and scheduled for at least 4 weeks of rehabilitation sessions. We enrolled a total of 16 patients, 2 of which did not return to therapy after one week (Table 1). Total sessions attended by patients ranged from 4 to 16 (8.3±4.1). Patients were primarily white (92.9%), non-Hispanic (85.7%), and female (64.3%), with injuries to their non-dominant hands (57.1%). Diagnoses included a combination of repetitive strain, traumatic, and post-operativeconditions.
Characteristics of patient participants
Characteristics of patient participants
*Participants 1 and 10 did not continue beyond first week of therapy and were not included in the study; Note: d, dominant; nd, non-dominant.
To provide context on levels of adherence and engagement for patients being treated by participant therapists, quantitative survey data was collected from therapists after each patient participant therapy session. The Sport Injury Rehabilitation Adherence Scale (SIRAS) [34] and Rehabilitation Therapy Engagement Scale (RTES) [35] were used to capture therapists’ perceptions of patient adherence and engagement, respectively. The SIRAS is a 3-item Likert-style scale (3–15 total score) that measures a therapist’s perception of how adherent the patient was to instructions and treatment protocols during the session. The RTES is a 15-item Likert-style scale (0–45 total score) that measures the therapist’s perception of the level of involvement of a patient during the therapy appointment. For both measures, a higher score indicates higher adherence or engagement. The SIRAS [34, 37] and the RTES [35] have both demonstrated adequate reliability and validity in rehabilitation contexts.
We engaged the therapists in 13 semi-structured group interviews that ranged from 16 to 56 minutes in length (40±12). Group interviews were chosen due to the increased convenience for the participant therapists and feasibility for data collection. Each interview included at least two of the therapists, but the group composition varied session-to-session. All interviews were performed by the senior author, audio-recorded, and transcribed verbatim. An interview guide was used to elicit therapists’ perspectives on therapy processes, unique patient concerns and progress, patient participation, and adherence outside of therapy. However, interviews were also iteratively directed by therapists’ responses, generating evolving research questions. Interview content centered on therapists’ experiences with the participating sample of patients, though therapists also engaged in more general discussions of other therapy encounters. At the outset, interviews were more structured with a focus on therapists’ general perspectives on engagement and adherence. For example, therapists were asked what they thought were indicators of active patient engagement during therapy sessions and what strategies they used to facilitate increased patient engagement. Over time interviews progressed to therapist-driven narratives of therapy sessions and therapist-patient interactions. For example, therapists were asked how they would describe their patients’ involvement and response to therapy and what their sense was of what was happening with patients outside of treatment.
Analysis
Descriptive statistics were generated from SIRAS and RTES scores to contextualize and triangulate [38] interview data. Measures of centrality and variability were calculated within and across patients to determine general therapist-perceived levels of patient engagement and adherence. Principles of constructivist grounded theory [39] were used to analyze interview audio and transcript data post study completion. Grounded theory uses inductive reasoning and sense-making to identify larger concepts and trends from segments of observed data and then develop plausible explanations [39]. Through this process, our goal was to identify areas to problematize or refine to facilitate a more active, collaborative therapeutic experience.
Coding and thematic development were completed primarily by the first author (K.L.). Audio recordings of each interview were reviewed in chronological order, with concurrent initial line-by-line coding of transcriptions. Constant comparison was used to iteratively reevaluate, update, and solidify codes as more data was examined. Next, themes were developed and linked together by identifying patterns of similar, frequent, and unexpected codes. This process constructed an overall picture of the therapist-patient relationship and its role in the therapy experience, including engagement and adherence. Emerging codes and results of constant comparison were discussed at regular meetings between the first author and authors 2 and 3 (S.R. and M.H.). Differing opinions among research team members were resolved with thorough discussion and debate during these meetings, with the first author having ultimate discretion for final coding and thematic development. Reflective memos were used at each stage of this process to explore connections between, meanings behind, and categorizations of codes, as well as to engage in reflexivity about positionality and data interpretation and positionality.
Positionality
The first author is an occupational science PhD student at the university with which the study’s clinical setting is associated. She also is an occupational therapist (OT), is a certified hand therapist (CHT), and has eight years of clinical experience in therapist-owned outpatient upper extremity rehabilitation working with other OTs. The second author is an OT with over 20 years of experience and the principal investigator of a musculoskeletal rehabilitation-focused research laboratory at the same university with extensive experience with quantitative and mixed-methods research in UE rehabilitation. The third author is an OT and academic researcher at a university in the southwestern US with expertise in mixed-methods clinical trials. The author team approached the study with the first-hand experience of understanding that adherence and engagement are important elements of hand therapy.
Results
All patients were perceived by the therapists to have consistently high levels of adherence and engagement. The mean SIRAS score was 14.4 out of 15 (SD = 1.0) and the mean RTES score was 42.5 out of 45 (SD = 3.5) across all appointments for all patients. Individually, patients’ mean SIRAS scores ranged from 13.0 to 15.0, and mean RTES scores ranged from 39.8 to 44.9 (Fig. 1). Within the context of this highly engaged, adherent environment, qualitative results were analyzed to explore the inner workings of therapist-patient interactions contributing to it. Four main themes surrounding the therapist-patient relationship emerged from the interviews: (1) dynamic power; (2) reciprocal, co-constructed engagement; (3) emotional states; and (4) complementary therapy contexts. These themes were found to exist within one transactional system within the therapeutic environment.

Sport Injury Rehabilitation Adherence Scale and Rehabilitation Therapy Engagement Scale scores by patient. Mean participant scores are indicated by circles and minimum/maximum scores are indicated by brackets. Participants sorted in ascending order, and participants 1 and 10 did not continue beyond the first week of therapy and were excluded from analysis.
For the purposes of this manuscript, we use the term power to succinctly refer to one’s ability to effect change in the direction or content of the therapeutic plan of care. Power expressed within therapist-patient relationships was described as continuously fluctuating between the two individuals, as well as other healthcare professionals and constructs of the greater biomedical environment.
Sources of power
Therapists agreed that collaboration within the therapist-patient relationship was ideal, though language choices did not always reflect an equal power balance. During interviews, therapists often identified patients by diagnosis or by which therapist was working with them (e.g., “the carpal tunnel syndrome patient” or “Therapist 2’s patient”). These identifiers were frequently used before more patient-centered ones such as patient roles, occupations, or interests. Therapists also noted the rare need for more authoritarian approaches, especially for patients they perceived as unmotivated or resistant to adhering to treatment plans. One therapist stated, “when people aren’t motivated… I usually just say to them, “You know if we’re not seeing progress, we can’t keep continuing to see you.” However, this approach was described as a last resort in response to a specific perceived patient need.
Though therapists reported being primary decision-makers throughout the therapeutic process, the plan of care and therapeutic approach were often influenced by patient personal factors such as complications from comorbidities, family responsibilities, or major life events or decisions. Specifically, patients demonstrated power through requests to review exercises or education, identification of specific difficulties during daily routines, affinity for certain exercises or activities, desire for novel experiences, or requesting measurements to track progress. Therapists reported that sessions were often structured around occupations meaningful to individual patients, and functional tasks related to these occupations were often simulated in-clinic. When discussing simulating a work task with a patient, one therapist said:
Her problem is with her left and she’s throwing or pitching [books] with her left the whole time. So, I made suggestion of… switching it up and throwing with the right once in a while instead of telling her to stop the activity all together… she enjoys this activity, she thinks it’s stress relieving, so I don’t want to take away something that might be… helping her, actually!
Aspects of the greater medical environment were identified as limiting the power of both the therapist and the patient within the therapeutic process. Physicians often dictated what activities were considered “safe” within and outside of therapy. Safety seemed to be a primary concern and a strong limiting factor for therapeutic activity choice and goal setting. As one therapist described, “…it’s safer for me to look at him and for me to give him feedback right now so that he knows… [he’s] not ready for this.” Additionally, insurance coverage was frequently identified as a limiting factor for duration of therapy, occasionally impacting prioritization of functional activities performed in-clinic, type of measurements taken, and goal setting.
Negotiation of power between competing interests
Occasionally these different loci of power would conflict, requiring the therapist to mediate between them. This most often resulted from mismatches between patients’ desires and doctors’ expectations. A therapist described one such situation:
…the doctor told her she won’t be able to box again and… she told me that she felt like punching him… her goal is to get back to boxing anyway. And so, I went to the doctor and said… “she wants to box” and he looked at me and he said, “She cannot box”… so there’s going to be a disconnect… I have her shadow boxing, I have her do mirror therapy.
The dynamic nature of power within the therapeutic relationship and environment was highlighted by therapists describing the need to encourage patients to actively participate in therapy. Patients were often scared to begin using their arms again or were acclimated to unidirectional relationships in healthcare environments from previous experiences. As a therapist noted, “I think our role is to have the patient believe that they are an active participant.” By taking action to change patients’ beliefs about their roles in therapy, therapists are attempting to increase patients’ agency within theserelationships.
Regardless of the dynamic ebb and flow of power throughout the therapeutic process, patients ultimately had the power to decide whether to continue participating in therapy or adhere to recommendations. Therapists acknowledged this with phrases such as, “I think if they show up to therapy, that’s like 50% of the battle” and discussed several situations in which patients ceased attending therapy due to changing life situations, decreased symptoms, or unknown reasons. In this way, what could be considered the most basic patient behavior is paradoxically also an expression of power.
Co-constructed engagement
Though engagement related to therapy activities and processes has previously been conceptualized as a patient-specific phenomenon, therapists in our study identified their own active engagement in the therapy process as not only important to successful therapeutic interventions, but also as being reciprocal with active patient therapeutic engagement. Therapeutic engagement seemed to be co-constructed on a foundation of complementary therapist and patient roles using the building blocks of reciprocal therapist and patient characteristics and behaviors.
Therapist and patient foundational roles in co-constructed engagement in therapy processes
The therapist’s comments indicated that they perceived their foundational role in constructing mutual engagement as relatively straightforward. Specifically, this role involved demonstrating and communicating clinical competence, expertise, and skills. As one therapist described, “[as a patient] you do have to trust to move forward with it if you’re scared… does the therapist know what they’re doing? Do they sound… professional?” As a complement to this therapist role, it was often noted that the patient role involved providing expertise on personal context and identifying specific challenges within daily routines.
Beyond personal context expertise, the patient’s role in mutual engagement was primarily characterized as physical and mental presence. There was consensus among the therapists that consistent therapy attendance was a sign of patient engagement. When discussing a patient, one therapist noted, “…this patient drove from far away to come here. He drove over an hour… he was making an effort to be here.” Conversely, there was some disagreement among therapists regarding mental presence as a sign of engagement. Factors contributing to this difference throughout the discussions included the level of mental attention required for engagement among different therapeutic activities (e.g. therapeutic ultrasound vs. home exercise program education), how mental attention could be secondarily assessed (e.g. visual or verbal interaction), and how to interpret signs of detractors or facilitators of mental attention (e.g. cellphone use to take notes vs. as a distraction).
Therapist and patient building blocks for co-constructed engagement in therapy processes
Therapists helped construct mutual engagement in therapy processes on the most fundamental level by directing supportive attention towards patients. That is, demonstrating they cared by actively listening to and acknowledging patients’ needs. As one therapist described, “…we really care about… the clients here and they know. They can tell we’re not checking out… We’re not… sipping coffee talking about our problems… We are focused on them.” In addition to demonstrating care, therapists felt adaptability and problem solving were critical to building and maintaining engagement in therapy. Therapists were able to change or tailor treatment approaches moment-to-moment based on evolving needs or circumstances. One therapist described changing her initial treatment approach to accommodate a patient’s persistent desire to perform a specific exercise: “… he said, ‘can I do a push up?’ I said no and he said, ‘okay fine I’ll just do it at home’… so then I said, ‘fine, let’s do push-ups’ because I’d rather see him do it versus him just be non-compliant and doing push-ups at home on his own.”
Though therapists universally agreed that flexibility was important, they did not agree on the degree of flexibility when it involved balancing competing interests such as patient preference and safety. In this way, adaptability was described as a skill developed through experience. As one OTD resident described:
I’m still learning to adapt my own kind of therapeutic use of how I… interact, how I speak with patients, how I can make recommendations, how I respond to frustration… as I get my hands on experience. And I think… a more experienced therapist… they’ve had more time to learn how to adapt… Whether that’s… a patient expresses frustration, or the patient might even disagree with something the therapist does… putting the therapist in awkward positions sometimes. How to roll with the punches so to speak. I think I’m learning how to do that.
Therapists believed that patients helped construct mutual therapeutic engagement through motivation to move beyond their current conditions. This meant anything from returning to work to learning to manage symptoms or adapting activities. The therapists felt that motivation alone would not ensure engagement in therapy and made a distinction between motivation in general and buying-in to the therapeutic process. That is, patients needed to believe that they would benefit from the specific approach being taken. A therapist describing one of her patients said, “…she was game, she was like yeah, I want to do it… and she really liked those activities, those simulated things and she understood why we’re working on proximal strengthening.”
Co-construction of mutual engagement in action
Patients’ and therapists’ ability to fulfill roles and enact behaviors needed to build mutual engagement were reciprocal and together constructed mutual engagement. Therapists identified that demonstrating clinical expertise and competence was crucial to facilitate patient motivation and gain trust and buy-in. Patients in turn communicated personal context details and priorities, which provided opportunity for problem-solving and adaptability from the therapists. Buy-in was thought to be further cultivated through this problem-solving and adaptability, as patients believed therapists were fully invested in their individualized care. This would hopefully result in patients taking initiative in therapy and incorporating therapy concepts into daily life. One OTD resident therapist illustrated the reciprocal, co-constructed nature of therapist and patient engagement in the therapy process when he described how patients’ perceived attitudes toward therapy encouraged him to be more creative in treatment planning: “when you have somebody in here who really wants to get back to what they’re doing… that really challenges you to come up with new ideas and ways for them to get to that point too.”
In contrast, when patients viewed therapists as less competent or skilled, or as only going through the motions during therapy, they may not have felt motivated or bought-in to the therapeutic approaches. Therapists described themselves as reverting to more textbook answers in response to patient questions or taking more rigid approaches to treatment when they perceived patients were in this state. In this situation both therapists and patients were generally described as closed off and less engaged.
Emotional states
Throughout the therapeutic process there is a complex balance of psychosocial and emotional states in both therapists and patients. Therapists expressed that these states could change drastically over the course of therapy and within each session. Discomfort-inducing emotional states such as uncertainty, fear, frustration, and sadness were highlighted as powerful influences on the therapeutic experience and were discussed more frequently than other emotional states such as happiness, excitement, or satisfaction. This is perhaps due to therapists viewing the overall environment as positive, making uncomfortable emotions, or those perceived as contrasting with the overall environment, more noticeable. As Therapist 2 noted, “…I feel like we’re positive. [Therapist 1] and I are both very positive. We have fun. We have fun with each other. And I think patients see that, like this is a fun place. This is a fun, safe, happy, good-energy place.” Therapists described these emotional states both as barriers and facilitators in the therapeutic process.
Emotional states as barriers
Uncomfortable emotional states were often described as barriers to engagement and active participation in therapy for both therapists and patients. In patients, this included emotional states both related to and outside of recovery from conditions. Feelings of anxiety, frustration, and sadness could emerge from slower than expected progress, setbacks, or difficulty resuming meaningful activities. They could also result from life events such as the loss of a family member or pet. In one case, the two sources of emotion collided as a patient experienced a significant hand injury from a dog bite, requiring her dog to be euthanized, and then also was in the process of moving to a new home because she would no longer need the yard for the dog.
Therapists reported attempting to manage patient emotional states over the course of therapy through the processes of venting, reframing, and humor. Venting consisted of therapists absorbing patients’ expression of these emotions as a form of patient relief or liberation from them. One therapist described a patient who was afraid to return to daily activities and resume social relationships and how this was addressed: “The fear and anxiety, I mean a lot of it was just through talking with her, it was just socializing with her and letting her explain it, kind of venting her,” and “Sometimes they just want to vent. They don’t really have any other safe place, their family is sick of it, so they vent a little and then they get on with it.”
Reframing involved providing perspective to situate patients’ current circumstances within the greater context of therapy to highlight patients’ continued progress. Discussing the same patient, another therapist mentioned using this process:
…she would say, “I’m just so down I can’t even drive… for more than 3 minutes.” And I would say, “Remember a week ago… you weren’t even able to move the shifter in and… now you’re able drive around the block once or twice. Look at how far you’ve come.” Reinforcing that she is making progress… she would… look back and say, “You know what? You’re right, I am making progress.”
Humor was used to distract patients from the weight of their emotions and promote what were perceived as positive emotional states. For example, therapists described a comical-looking green chicken that both served as a prop for simulation of feeding tasks as well as an object of humor. “[The patient] gave a good laugh when I offered her the chicken” one therapist remarked. The overall clinical environment was also described as promoting humor: “We make everything more light-hearted, and it takes the seriousness or the heaviness of injury out of the way.”
Therapists themselves also seemed to be affected by uncomfortable emotions, though they were not as explicit in their description of these within themselves. Therapists reported experiencing fear related to patient safety and frustration or uncertainty related to patient setbacks, lack of progress, and perceived lack of motivation or adherence. Therapists also seemed to internalize uncomfortable emotions from patients, especially when those patients had been through particularly traumatic experiences. They used phrases such as “sometimes it’s depressing you know for me.” Therapists did not discuss negative emotions arising from their personal lives as factors in the therapeutic process, though they also did not rule them out.
For therapists, strong emotions could sometimes lead to reverting to formulaic, rigid, or repetitive interaction with patients. An OTD resident described his experience with a patient that he perceived as being hostile:
The first couple times I felt like my engagement went down… I didn’t know how to respond, so… if she questioned me, I would just give… a textbook answer. And even now, I’m still trying to work through how to respond to something like that. As a therapist still learning the ropes, I feel like I could very easily just shut down and do my job. And then, with minimal conversation… just tell her what she needs to hear and then move on.
Therapists’ uncomfortable emotions seemed to be modulated through current or anticipated patient progress. This progress could be biomechanical, functional, or even improved patient personal outlook or emotional state. Therapists also seemed to use humor to help themselves cope with the gravity of dealing with emotionally strenuous situations. At one point while describing a difficult situation with a patient, one therapist joked to the other, “you get all the criers”, and the two laughed. No explicit strategies to address therapists’ emotions werediscussed.
Emotional states as facilitators
In certain situations, uncomfortable emotions served as catalysts for mutual engagement. Therapists reported that, for some patients, fear of loss of function or uncertainty about symptoms was described as motivation to seek treatment and adhere to exercise routines: “they might have just enough… questions where it’s worrisome for them and they think something might be wrong. So, they go see… the doctor and the doctor refers them here.” Within treatment sessions, discomfort-provoking emotions sometimes prompted patients to take a more active role. One therapist described a situation in which a patient was fearful of flexing her wrist during activity after being told it would increase her symptoms, explaining, “she would always come in and ask, ‘can we review my exercises?… specifically, I want you to look at my wrists.”’ In this case the patient’s fear motivated her to request specific interventions. Therapists also described using consequences to induce uncomfortable emotional states with the goal of motivating patients, improving buy-in, or increasing adherence. This often involved warning patients that symptoms may worsen, impairments could become permanent, or discharge from therapy would be imminent if circumstances did not change.
For therapists themselves, emotions such as uncertainty about or dissatisfaction with current or anticipated patient progress could prompt further problem-solving and flexibility, such as modifying or fabricating an orthosis or updating exercise programs. While discussing a patient who was feeling depressed after a traumatic injury and a difficult family event, a therapist expressed that she was saddened by his circumstances and commented on how the patient’s demeanor impacted her motivation to help him: “I want to help him… I’m not turned off by that… it’s the reverse. Okay, how can I engage him… and let him know we care.”
Therapists also seemed to believe that expressions of uncomfortable emotions during therapy signified and reinforced patient trust. Rather than hide their emotions, patients were described as feeling safe enough to be vulnerable with or vent to therapists. Therapists could respond by validating patients’ feelings and providing comfort, release, or perspective. In this way, even emotions viewed as barriers to the therapeutic process provided opportunities to strengthen therapist-patient relationships.
Emotional states and perceived progress
Notably, when patients were thought to be experiencing emotional states as barriers, descriptions of these states seemed to take precedence over other descriptors of current status or progress (e.g., physical symptoms, range of motion, or functional use). In contrast, patients who were viewed as having a positive outlook were more often described in terms of these measurables, rather than by their psychological characteristics. In this way, barrier emotions seemed to be viewed as needing to be overcome before actual therapy could begin, rather than a legitimate focus of therapeutic intervention in and of themselves.
This phenomenon also extended to descriptions of activity participation. When discussing patients they believed were impaired by emotional states, therapists more often described engaging in meaningful activities as the general participation. However, when this was not the case, engagement in functional activity was described as achieving specific segments of activity, such as gripping a steering wheel or dog leash. Furthermore, patients described as “doing well” seemed to correlate with perceptions of more positive patient emotional states, even when progress with physical or functional aspects of recovery was less than ideal.
Complementary therapy contexts
Therapist and patient experiences and the nature of therapeutic relationship changed throughout the therapy process within different physical and temporal contexts. These often were discussed as complementary pairs: social vs. private, within vs. outside of the clinic, and during therapy vs. after discharge. These changing situations could be used to help manage the trajectory and flow of therapy through manipulation of therapist and patient expressions of power, emotional states, and mutual engagement, and needed to be accounted within the treatment plan
Social vs. private
In the clinic, the social environment existed within the communal treatment area where multiple therapist-patient pairs worked simultaneously. Therapists reported that relationships within this context involved camaraderie, socialization, and humor. The dyadic therapist-patient relationship was often described as expanding to include other patients and therapists, which could provide emotional support and encouragement. As one therapist explained: “we’ve created this… social fun environment… and everyone’s in conversation with each other.” Conversely, the private environment involved a separate room or space wherein the therapist-patient dyad could interact away from others. This space was described as calm and safe and was often where patients were taken to vent and confide in their therapists. One therapist described using this type of environment for a distressed patient: “he used to come in and just burst out crying and I’d have to put him in a private area, and I was really glad he felt safe.” Therapists emphasized the need for both spaces to balance changing patient emotional states, sometimes within a single therapy session. “If they look like they’re about to break down then we’ll move them to a private space,” a therapist explained.
Within vs. outside of the clinic
Therapeutic environments within vs. outside of the clinic seemed to create dramatically different balances of power and responsibility between therapists and patients. Within the clinic therapists reported that they engaged with patients in collaborative education and problem-solving. As previously noted, influence over the therapeutic process within the clinic setting was dynamic, though ultimately mediated by therapists. Therapists tailored this environment to each patient to facilitate positive patient outcomes. Outside of the clinic patients typically possessed more power, responsibility, and sometimes more control over the environment. In this context patients had to navigate the translation and carryover of clinic-learned education, skills, and adaptations to more complex and sometimes chaotic situations. This was evidenced by therapists’ responses of uncertainty when asked if certain patients were performing their therapeutic programs correctly (or at all) at home, especially for one particular patient who was described as perpetually focusing on barriers to performing exercises at home. Therapists also described the importance of patient problem-solving for integrating and prioritizing consistent performance of home programs within the flow of busy lives.
To transcend the barriers between these spaces and facilitate continued progress, therapists reported that they dynamically interacted with patients and negotiated treatment approaches. Actions taken within each space impacted what happened or what was possible in the other. This was demonstrated by a therapist describing a situation in which she had modified a patient’s splint:
…on visit number two she brought me another wrist brace… she wanted me to look at it and evaluate her wrist position and so that’s another indication that, “You helped me with this wrist brace, and I like the modifications you made so can you please check my other wrist”
Another therapist went on to say:
I’ll say… “I’m just your coach or I’m only here twice a week for an hour you can do this on your own… Bring in any other questions we can get anything answered, or if you thought of something after we left bring it in next time” so that they know they can collaborate and consult…
In general, treatment approaches were provided during therapy with the understanding that they would be then implemented outside of the clinic. After trialing these interventions outside of the clinic, patients assessed fit and reported back to therapists during follow-up visits. Patients and therapists then further problem-solved solutions, continuing the cycle. Any interruption of this process could interfere with the overall progression and continuity of therapy plans.
During therapy vs. after discharge
The time periods during therapy and after discharge juxtaposed intimate relationships with the sudden absence of any relationship. Over the course of therapy, therapists and patients often formed close bonds as the therapists helped guide patients toward recovery. The trust and vulnerability demonstrated by patients could reach similar levels to those of close personal relationships. After discharge, this connection abruptly disappeared. Navigating this change was sometimes difficult for patients, especially in the absence of strong external support systems. One therapist described this painful transition, “there are some people who, when we have to discharge them, [say,] ‘no, no I want to keep coming.”’ Therapists highlighted the importance of setting realistic expectations about the nature and progression of the relationship over the course of therapy to facilitate healthier discharge transitions. “I try to prepare them weeks prior to discharge,” one therapist noted.
Transactional system
Based on our therapist interviews, all four main thematic dimensions of the therapist-patient relationship (power, engagement, emotional states, and context) were closely connected in a complex, transactional system (represented in Fig. 2). Therapists and patients engaged in continuous processes of reciprocal actions and reactions involving both them and their environments. Therapists had to mediate between different sources of power within this relationship and the greater medical environment, while simultaneously balancing their patients’ and their own emotional states through different environments and the arc of the relationship over the course of therapy. Patients’ beliefs, emotions, and actions directly impacted therapists’ own emotions and their ability to participate in mutual engagement. The experience of the therapeutic process was co-constructed between therapists and patients and was greater than the individual perception of each participant. Finally, the physical, social, and temporal spaces played a significant role in this experience, dynamically changing the fundamental nature of the relationship in the moment and over time.
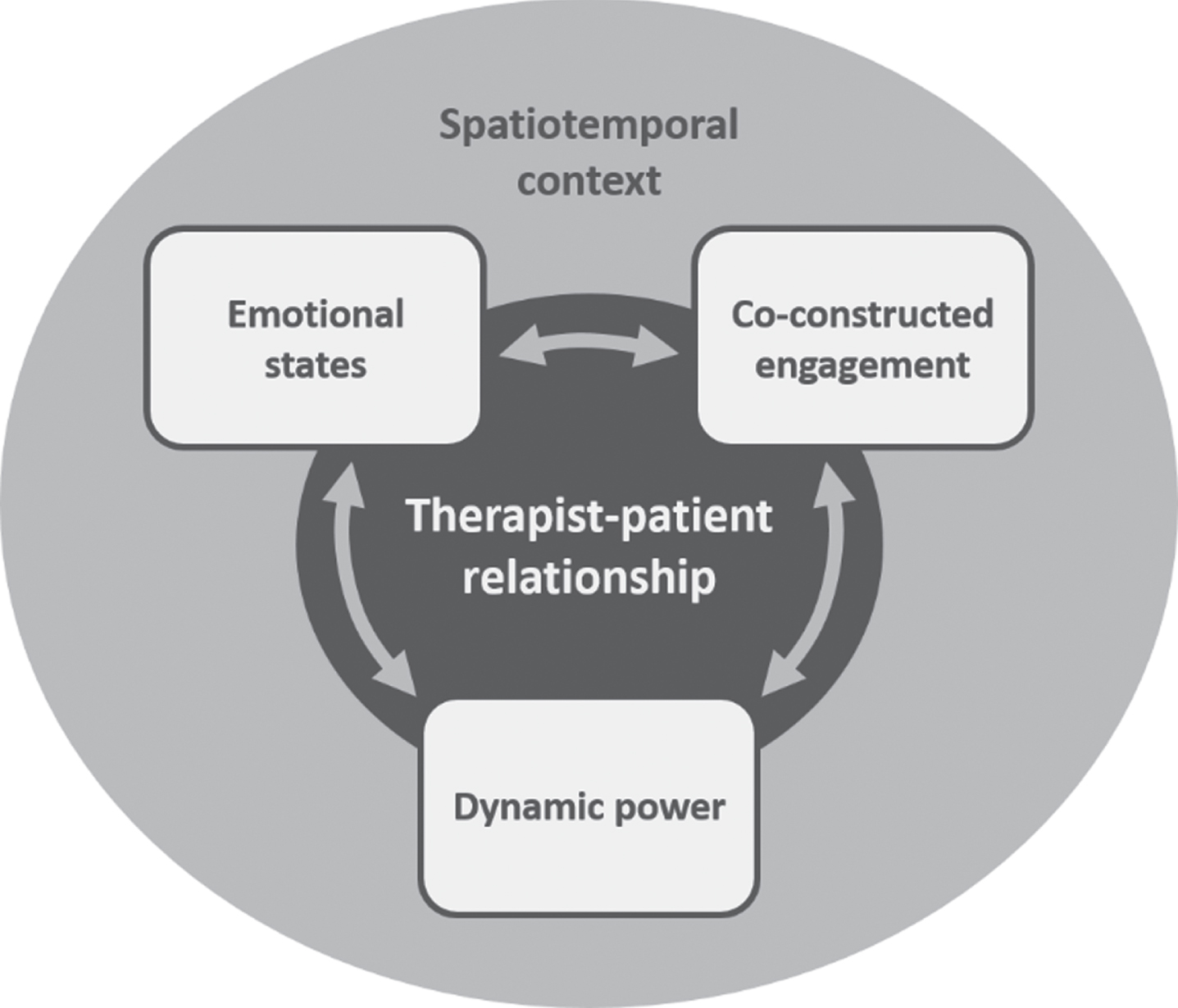
Thematic model representing components of the transactional system created by the therapist-patient relationship in an upper extremity musculoskeletal rehabilitation clinic.
Despite highlighting the importance of navigating multidimensional interactions, therapists had difficulty communicating how this was achieved and quantifying progress of patient agency, engagement, and emotional status. This contrasted with detailed descriptions of biomechanical or functional outcomes (e.g., ROM, symptom reduction, task-specific function, or using adaptive strategies).
Although therapists sometimes identified general techniques to manage patient emotional states and facilitate engagement (e.g., venting or reframing), they typically used vague descriptors such as “psych-OT.” When asked to elaborate on what these approaches involved, one therapist answered that she would tell the patient, “You’re safe to cry here that’s fine, it’s an outlet” adding, “just talking about stress in general and how it can affect your body.” She also described providing activity choices to give the patient “some control of what’s going on.” This explanation, while more precise than the original, still does not describe specific effects of stress on the body or why the patient should be aware of them, specific datapoints used to determine the need for these interventions, theories or frameworks informing them, or expected patient outcomes. Similarly, therapists did not discuss specific indicators for moving between social and private spaces (beyond the overt indicator of a patient crying), nor specific approaches to prepare patients for therapy discharge. Therapists also often expressed uncertainty about whether techniques were translated successfully from clinical to home environments.
Conversely, when therapists discussed addressing biomechanical factors, they detailed strategies such as specific exercises (often demonstrating or describing them without prompt), dynamic orthosis fabrication, or increasing force when mobilizing individual joints. They also discussed the specific rationale, timing, and appropriateness of these strategies, highlighting factors such as inflammation, tissue stiffness, pain, joint integrity, physical comorbidities, ease of use or performance, and expected tissue recovery timelines. One therapist described her approach for a patient with a stiff hand:
It’s… like math. I take their measurements all the time and then I track the numbers and see if it is enough improvement after a visit or two visits or three visits… after the last visit [with the patient], I thought… this is not going fast enough… I decided… to make her a static progressive flexion orthosis, which is basically going to stretch her fingers down into a fist.
When therapists discussed progress with patient psychological status or active engagement, they used phrases such as “doing better,” while biomechanical progress was described as specific degree measurement gains. There was also uncertainty surrounding interpreting the emotional states of certain patients, with therapists sometimes disagreeing in their perceptions of them, or reporting that their initial impressions were incorrect.
Discussion and implications
In this study, we aimed to understand therapists’ perspectives on how the therapist-patient relationship within UE musculoskeletal rehabilitation facilitates collaborative therapeutic engagement and active patient participation. Our analysis of SIRAS and RTES results indicates that the therapists within this setting viewed their patients overall as highly engaged and adherent. This agreed with therapists’ overall description of their patient population in the interviews, which contextualizes our qualitative thematic analysis. In this engaged and adherent environment, therapists prioritized careful management of therapist-patient relationship elements. These therapist-patient relationships were complex, intimate, and dynamic, extending beyond patient education and application of physical interventions. The resulting transactional system incorporated power balances, co-constructed understanding of therapeutic engagement, and individual emotional states all embedded within shifting spatial-temporal contexts.
Power to influence the direction of care fluctuated between the therapist, patient, and other parties within the medical environment. Though therapists were primarily responsible for directing the plan of care, patients frequently influenced interventions through unique needs and therapy preferences. Therapists often had to negotiate between competing interests within this system to create a plan of care acceptable to all involved. Despite calls for patient-centered care, power dynamics within UE rehabilitation have not been widely examined. Limited examples discuss empowering patients to develop recovery narratives through active listening [30] and therapeutic relationships based on a mutual exchange or partnership [32]. Though in these examples the therapist ultimately bears the responsibility of ensuring active patient involvement through their own actions. Within the broader context of rehabilitation, power has been discussed as difficult to balance on both interpersonal and institutional levels [40]. Specifically, interpersonally balancing patient preferences with clinical approaches and institutionally balancing therapy meaningful to patients versus a more biomedical focus on safety. Mirroring our findings, therapists have been reported to be the primary mediators between these competing interests[41].
Engagement was constructed between therapists and patients, rather than as isolated experiences separate to each individual. Engagement required therapists and patients to fulfill the respective roles of competent clinical expert and present personal expert; and then to reciprocally build mutual engagement through engagement-promoting behaviors unique to each role. Therapists achieved this through demonstrating caring toward patients and being flexible to evolving patient needs. Previous UE and general physical rehabilitation literature has described therapists’ attention towards patients as acts of caring or listening, and as observing and responding to patient actions [32], and has found that perceived therapist expertise is important for facilitating patient trust [42]. From the therapists’ perspectives, patients needed to demonstrate motivation to progress beyond their current state and buy-in to the therapeutic process. Patient buy-in or belief in the value of therapeutic approaches has been found to contribute to patients’ willingness to engage in therapy and adhere to therapeutic plans, especially in rehabilitation plans requiring significant patient involvement or time commitment [7, 44]. Additionally, literature within the field agrees that perception of patient outlook can positively or negatively impact therapists’ ability to carry out engagement-promoting behaviors[32].
Studies advocating for patient-centered care recognize the importance of therapist adaptability from moment-to-moment in UE therapy [12, 31]. As healthcare providers, therapists are responsible for guiding the multidimensional therapeutic process to facilitate engagement and adherence, and therefore clinical expertise in UE rehabilitation requires much more than knowledge of biomechanics, implementation of individualized treatment plans, activity analysis, and problem-solving functional adaptations. In fact, much of the relationship seems to fall within the psychosocial realm. In particular, therapists discussed uncomfortable emotions as both barriers and facilitators in therapy. They predominantly focused on how they managed patient emotions with venting, reframing, and humor, or harnessed them to facilitate motivation and adherence. Yet, therapists also seemed to be both positively and negatively impacted by their own uncomfortable emotions. Patient emotional states appeared to impact how therapists evaluated and communicated patient progress andoutcomes.
Our findings on patient emotional states agree with previous UE rehabilitation literature that these factors are prevalent within this population [45, 46] and can significantly alter patient experiences and impact functional outcomes [46–48]. Though, much of this research is cross-sectional, limiting causal inference, and similarly focuses on psychological states categorized as negative [48]. Emotions such as fear have also been previously discussed as motivators for adherence [7]. In contrast, therapists’ emotional states and their relation to patient interactions has not been widely investigated. The sparse literature that does exist on this topic focuses on feelings in response to patient interactions rather than their impact on therapy [32].
Strategies to manage patient emotions have some representation in UE rehabilitation literature. Reframing patient situations has previously been discussed in the context of promoting hope or decreasing perception of severity of condition through social comparison among patients [32], though not explicitly as an intentional action by therapists. Humor has been discussed as relieving negative emotions for both therapists and patients by lightening the context and promoting reciprocity [32]. To our knowledge, venting or emotional release has not been explicitly investigated in this setting, though cathartic emotional release is not a new approach to handling negative emotional states in other fields [49].
Throughout the therapeutic process, complementary physical and temporal contexts created changes in therapeutic relationships and therapist and patient experiences. Social vs. private clinical spaces could provide alternating camaraderie and positivity or calmness and safety as needed to manage patient emotional needs. Additionally, the environment within the clinic foregrounded the abilities and responsibilities of therapists, while outside environments challenged patients to translate treatment concepts to complex personal situations. Lastly, therapists had to carefully manage patient expectations to facilitate successful transitions from the intimacy of the therapeutic relationship to the complete absence of one.
Therapists’ descriptions of social and private spaces mirror findings from Crepeau & Garren [32], though the therapist in their study had a strong preference for treating patients in the social environment. They also discuss the intimacy of the therapist-patient relationship, noting that a patient who considered himself a private person developed a very close relationship with his therapist. However, to our knowledge, there is no physical rehabilitation literature explicitly discussing difficult patient transitions from therapy to discharge, nor exploring the impact of the diverse therapeutic environments or social-temporal circumstances on engagement, balances of power, or patient psychological states.
Considering the complexity of evolving therapist-patient relationships and their apparent value to an engaged, collaborative UE rehabilitation clinic, further investigation is warranted in additional settings with more diverse patient populations. It may be especially fruitful to compare our results to similar investigations conducted in settings with more variability in perception of patient engagement and adherence. Foregrounding interpersonal and psychosocial aspects of care in research may illuminate opportunities to better understand patient needs as a whole, which can inform the expansion of therapists’ toolboxes to help patients achieve the complex goals of returning to work and other life roles. Specifically, this may help identify pertinent approaches from other rehabilitation practices to supplement conventional UE rehabilitation interventions focusing on body function, symptoms, and activity performance [26, 27]. Some examples of potential approaches include therapeutic use of self [50, 51]. emotional intelligence [52], mindfulness [53, 54], narrative medicine [30], or interventions focused on habits, roles, and routines [55, 56].
Limitations
Coding and thematic analysis was completed primarily by the first author, though triangulation was achieved through iterative conceptual reviews with the second and third authors. Additionally, while the first author’s non-involvement in data collection prevented some generative grounded theory processes, it also mitigated potential biases. Moreover, enrolled patients were rated as highly engaged and adherent with little variability which could have impacted the nature of the therapeutic relationships in which they engaged. It is possible that patients with the highest levels of psychological distress, or who were less engaged and adherent, may have avoided participating in the study. Lastly, as patient perspectives were not included, our results are limited to the perception of clinicians. This highlights the need for continuing research on the therapist-patient relationship in UE rehabilitation settings, including future incorporation of patient experiences.
Conclusion
Our study analyzed therapists’ perspectives on the association between therapist-patient relationships, active engagement in therapy processes, and collaborative care in an outpatient UE rehabilitation setting. Within this highly engaged and adherent environment, therapists emphasized the importance of carefully managing complex and evolving therapist-patient relationships. These relationships extended beyond surface-level clinical activities and were intertwined with a transactional system of power balances, co-constructed engagement, and emotional states all embedded within shifting spatial-temporal contexts. These findings provide a preliminary understanding therapist-patient relationships and highlight the need for further investigation into management of dynamic elements of care in diverse UE rehabilitation settings. Understanding these phenomena is crucial to continue to evolve therapeutic approaches toward more collaborative and holistic care and increase the efficacy of UE rehabilitation to achieve real-world goals such as returning to work.
Ethical approval
This study was conducted in compliance with ethical standards set by the Office for the Protection of Research Subjects (OPRS) and Human Research Protection Program (HRPP) as approved by the institutional review board of the University of Southern California (HS-16-00148, approved 3/14/2016).
Informed consent
All participants provided informed consent prior to participating in the study.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
The authors report no funding.