
Abstract
BACKGROUND:
Smartphones cause physiological problems due to inappropriate postures and extensive usage. India, being the second leading country with the highest number of smartphone users (492 million in 2021), has witnessed a significant rise in smartphone-related musculoskeletal disorders (MSD).
OBJECTIVE:
This study compared the effects of 60-min smartphone gameplay on head flexion angle, muscle activity, and loads at C7 on Indian adolescents.
METHODS:
A subjective assessment was conducted on 1659 participants, of which, 40 young male adults aged between 20–28 years performed the experimental trial. Muscle (Sternocleidomastoid) activity, head flexion angle, and load acting at the neck (C7) were analyzed through postural assessment, pre-and post-subjective analysis.
RESULTS:
Participants maintained an average of 28.46°±4.04° head flexion angle for more than 43 min (71%) in an hour while performing the task. The muscle activity increased to 23% (p < 0.001) of MVC at the end of the task compared to the beginning.
CONCLUSION:
The results indicated a significant increase in muscle activity (1.61 times), spinal loads (4.6 times) and subjective discomfort (2.9 times) after prolonged smartphone usage. It is evident that various aspects (duration, posture, content) play a vital role in smartphone-related MSD and there is a potential risk of cervical spine problems. The increased loads reduce muscle stiffness and increase intervertebral disc pressure.
Introduction
Smartphones are becoming an integral part of our daily life. Millions of users have reported musculoskeletal disorders (MSD) due to prolonged smartphone usage [1]. Approximately 3.5 billion individuals worldwide owned a smartphone in 2019 [2], 492 million in India alone [3]. However, with the COVID-19 pandemic, the utilization of smartphones rapidly increased by 45% globally in 2021 [3] and an increase of 39% in India with the usage of 6 hours 55 minutes per day [4]. Smartphone usage leads to problems such as shoulder pain, neck pain, vision defects, addiction, and fatigue [5–10]. Fatigue is caused by demographic, environmental, physical, and habitual risk factors [11, 12]. A higher level of muscle fatigue leads to musculoskeletal imbalance or MSD [13]. During smartphone texting, people usually bend over their phones; significantly straining their spinal area and leads to neck imbalance, thus causing neck pain [5].
Many studies have attempted to identify the correlation between text neck syndrome and muscle activity [5–8, 14–17]. To measure head flexion angle, sensors such as the inertial measurement unit [6, 14], accelerometer, and gyroscope [5] have been used. Few studies have examined the association between the duration of smartphone usage with the head tilt angle during web browsing [6] and texting [7] under natural movement, and postures [5]. Studies have observed that mechanical load on the neck increased by 3–5 times while using smartphones compared to neutral posture. Neck, shoulder, wrist, lower back, and thumb muscles are majorly involved in smartphone-related MSD [8–10]. Discomfort in the muscles was recorded through surface electromyography (SEMG) in the cervical electro spinae [7, 18], trapezius pars descendens (TRP) [15–17] and sternocleidomastoid (SCM) [15, 16] muscles. Muscle activity depends on the posture; an increased muscle activity increases the fatigue level [11, 12].
Recent studies have used 3D camera, a multi-object detection system, and photogrammetry [19] to estimate the flexion angles. Angle data were analyzed to examine the correlation of muscle activity with the flexion angle. For ergonomic evaluation/postural analysis, rapid upper limb assessment (RULA) is a convenient tool that assigns scores based on body posture while using a smartphone [20]. The load acting on the cervical spine increases with the head flexion angle. The calculated load acting on the cervical spine at 15°, 30°, 45°, and 60° was 12.24, 18.14, 22.22, 27.21 kgf respectively [21]. Some studies evaluated participants’ discomfort levels through subjective evaluation by considering their socio-demographic, usage patterns, and body posture maintained [22, 23]. Subjective data was evaluated through Q-factor analysis, Likert scale [24, 25] or the neck disability index [18] to assign a score to participants’ discomfort level.
The key findings from the past literature are (1) increased smartphone utilization increases the muscle fatigue induced, leading to MSD. (2) For head stabilization, TRP and SCM muscles play a significant impact on muscle forces acting on the cervical spine. (3) Researchers evaluated head flexion angle during smartphone usage using different techniques like motion sensors, image processing and chart-based methods, to correlate muscle activity with head flexion angle. (4) Many researchers collected questionnaire data from smartphone users, either pen-paper or web-based method to analyze the discomfort during smartphone use under different scenarios (postures, durations, age group and usage content).
The research gap from past developments state that, although many studies related to smartphones and their effects were conducted in different countries, India being the second-highest smartphone user, smartphone-related studies are still lacking in India. This study targets the effects of smartphones on Indian adolescents, as the anthropometry [26] and smartphone usage pattern [27] varies among different countries and significantly affect smartphone usage. Also, the previous studies [16, 29] reported the effects due to smartphones for 3–5 minutes of usage (4% of MVC on average), which is significantly less compared to this era of smartphone dependency or only the subjective assessment [1, 10] without any experimental trails. Hence it is important to address the effects of prolonged smartphone usage. Therefore, a correlative study is conducted to examine the relationship between neck muscle activity and 1-h smartphone usage in Indian adults. Although fatigue induced due to prolonged smartphone usage primarily affects TRP and SCM (responsible for head flexion) muscles, the SCM muscle is not studied extensively. This study elucidates the effects of prolonged smartphone usage on the SCM muscle by analyzing the muscle activity, head flexion angle, and load at C7 of Indian individuals. This study proposed two hypotheses: based on [15], (a) the muscle activity reaches 15% of MVC after 1-hour smartphone usage and (b) the head flexion angle is static during continuous smartphone gaming.
Materials and methods
The participant selection process, experimental tools and techniques, data collection, and processing procedures are outlined in this section.
Subjects’ selection
Forty right-handed men having prior experience in smartphone gaming were recruited through advertisements, and their demographic data are listed in Table 1. Participants with MSD, especially neck, hand, and arm complaints, were excluded. Also, the participants were instructed not to perform any high muscle tension tasks on the day of experimentation.
Subject’s demographic characteristics (n = 40)
Subject’s demographic characteristics (n = 40)
M – Mean, SD – Standard Deviation.
The study was reviewed and approved by the Institutional Ethics Committee (Human Studies) of SRM Medical College Hospital and Research Centre under ethical clearance number: 1980/IEC/2020. The institute follows the Indian Council of Medical Research and Biomedical Research guidelines on human participants in accordance with the Declaration of Helsinki.
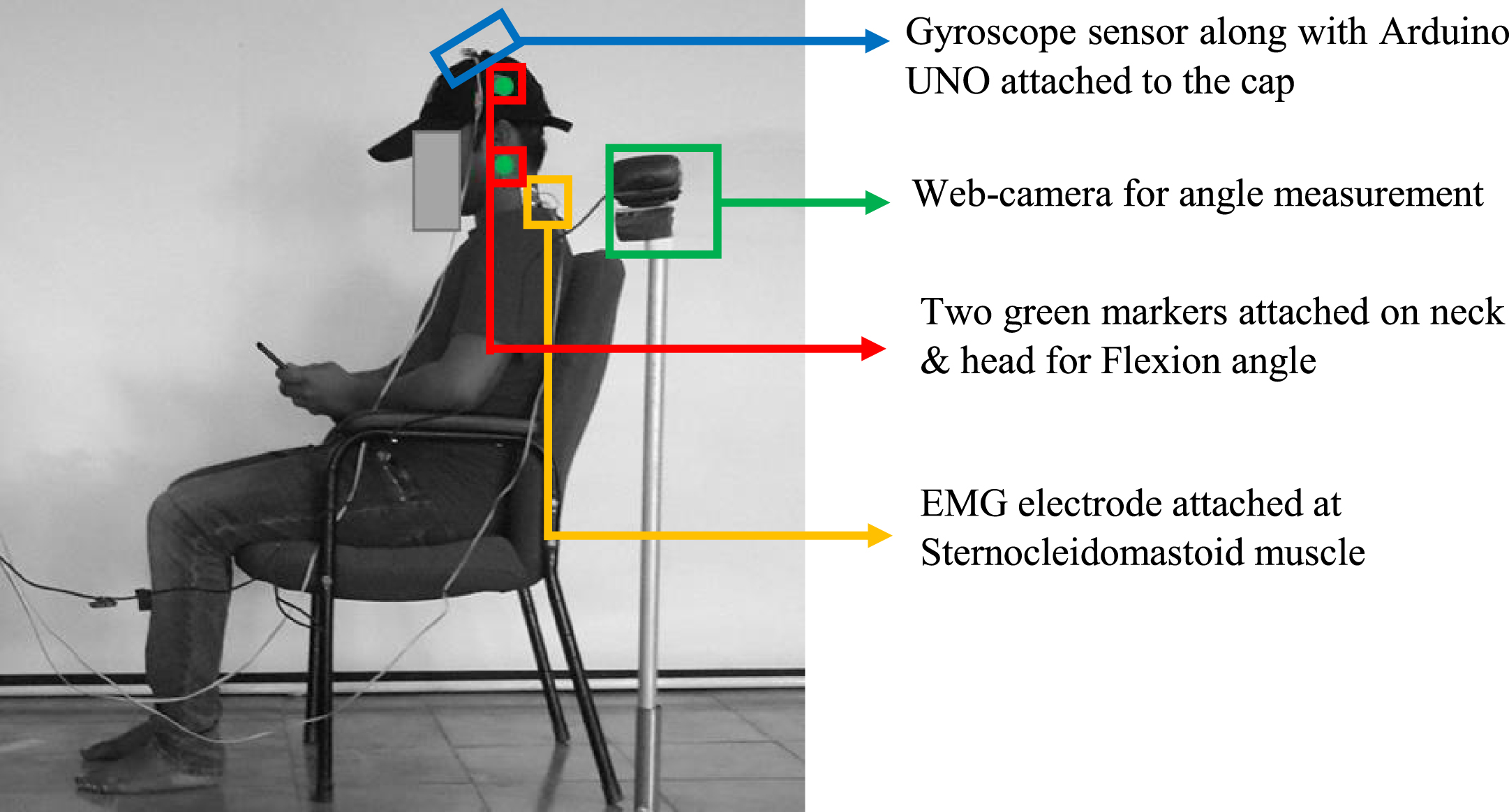
A Myoware-EMG sensor (AT–04–001 muscle sensor) [13, 30] was used to calculate SCM muscle activity. The SCM (neck) muscles are exhibited to considerable fatigue induced due to prolonged smartphone usage [8]. This sensor is a safe and wearable research device approved by Conformite Europeenne and applicable directives. The sensor detects a raw signal and an EMG envelope (rectified signal) [13]. An average error of 2.82% was noticed during calibration and the same was corrected in the final readings. A 42-mm-diameter and 1-mm-thick medico electrode (Msglt-8 G) coated with polymer Ag–AgCl gel were used. A webcam was utilized to capture the head tilt angle using OpenCV-Python algorithms. A gyroscope sensor (MPU-6050) with an accuracy of 0.1° was used to validate the flexion angle received through the webcam. A gyroscope is a secondary evaluation sensor for estimating the load acting on the C7 based on the head flexion angle. A smartphone weighing 170 g with a screen size of 5.9′′ (720×1440-pixel ratio, and 40–50% brightness) and a nonadjustable office chair with a forearm and back support were used.
Subjective assessment
A pre-subjective assessment consisting of 26 questions was developed using a standard questionnaire [22]. The questionnaire included questions on sociodemographic data, smartphone usage (duration, pattern, and posture), and knowledge regarding the effects of excessive smartphone utilization as listed in Table 2. A total of 1659 responses were collected, and the experiment was conducted on 40 participants. In the post-subjective assessment, another questionnaire was filled out by the participants’ related to discomfort level in their neck, shoulder, back, and wrists/fingers on a scale of 1 (very comfortable) to 5 (very uncomfortable) for every 15 min [25].
Pre-subjective questionnaire (26)
Pre-subjective questionnaire (26)
In this study, the right-handed individuals were included as test participants for the experiment, and the “subway surfers” game was selected; the participants were asked to play the smartphone game for 1-h in a sitting posture, which was the preferred posture by 59% of the participants. Subway Surfers game is an endless runner game and the most preferred (45%) among the test participants. It’s a visually animated game, involving motions of swiping right, left, up, and down to avoid crashing into obstacles. The participants react by tilting their heads in the real world, matching the movements of the character in the game with higher head flexion angles. First, the participants were allowed to comfortably sit in a nonadjustable office chair with a cap affixed with the gyroscope, and EMG sensor. Then, the participants were asked to play the game on a smartphone by using both thumb fingers with the hands resting on the armrests and maintaining their comfortable head flexion angle (Fig. 1) with an eye-screen distance of 30–40 cm. The experimental location was maintained with an illumination of 75–80 lux.
Subject’s posture maintained for smartphone gaming.
The experiment involved three stages. In stage 1, the procedure, technique, equipment, and data extracted were explained to the participants, and their written informed consent was collected prior to experiments.
In stage 2, the participants were prepared for testing. This study followed the guidelines of SENIAM and ISEK for standard electrode placement and procedure. To acquire a favorable EMG signal and reduce impedance, the skin was cleansed with alcohol, the hair on the muscle area was removed, and electrodes were attached to the dry skin. According to the protocol for the SCM muscle, both bipolar electrodes were placed 20–30 mm along the sternal portion, with the electrode center 1/3 of the distance between the mastoid process and the sternal notch. The reference electrode was placed the right acromion process [16]. The gyroscope sensor was attached to the head’s cap and a web camera was fixed at a 1-m distance from the participant at a height of 0.8 m for capturing motion and examining the head flexion angle. In addition, the participant was asked to set their head at a 0° angle, and two reflective green markers with a diameter of 4 cm were attached to the neck and cap (50 mm above the ear; Fig. 1).
In stage 3, three data signals were extracted from the muscle. First, the participants were asked to sit in a relaxed position, and data were recorded for 90 s; these data were considered RestEMG. Subsequently, the MVC, a standardized parameter used for measuring extreme muscle strength, was calculated for 10 s and considered MVCEMG. This study computed the MVC of the SCM muscle by using a headband attached to a rigid surface (Fig. 2). In each MVC test, the participants were asked to gradually exert their maximum force and pull the head for 3–5 s, hold the same position for 3 s, and progressively reduce the force in 3 s. After the MVC measurement, the participants rested for 20 min. Then, the participants were allowed to play the smartphone game by using both the thumb fingers with hands resting on the armrests for 1-h in the sitting posture. Both the flexion angle and EMG (TaskEMG) were recorded. The smartphone was set in flight mode and all electronics except the experimental equipment were turned off to prevent interference. After smartphone gaming, a post-subjective assessment form was filled by each participant.
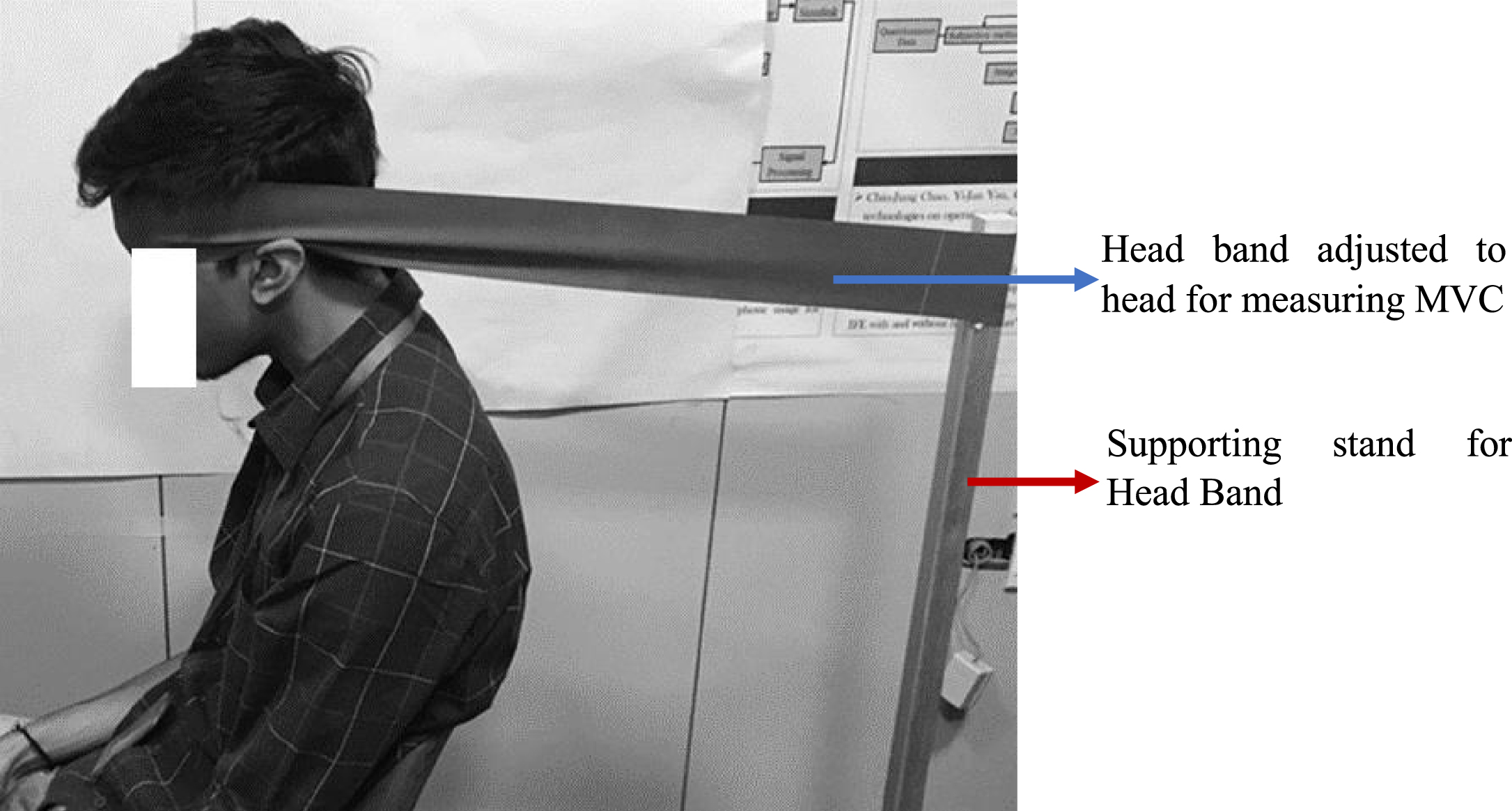
MVC measurement technique for sternocleidomastoid muscle.
The Myoware EMG and gyroscope sensors were connected to the laptop through a microcontroller and recorded data were exported to Excel. Finally, the datasheet was analyzed to correlate changes in the flexion angle with those in muscle activity.
First, the raw signal received from the EMG was amplified and subjected to common-mode rejection. Then, Fourier analysis was performed to estimate the frequency potential and related muscle fatigue. The signal was collected at a sampling rate of 1000 Hz, and a Butterworth second-order band-pass filter was utilized with a cutoff range of 20–500 Hz. Later, the signal was refined through full-wave rectification, followed by the smoothing process of the root mean square (RMS) method. During the smoothing process, the time window width of 50 ms was used to recognize fast movements and reflex actions. Thus, the RMS of EMG was directly related to fatigue. Finally, MVC-based normalization was performed to compare the data between the participants [16].
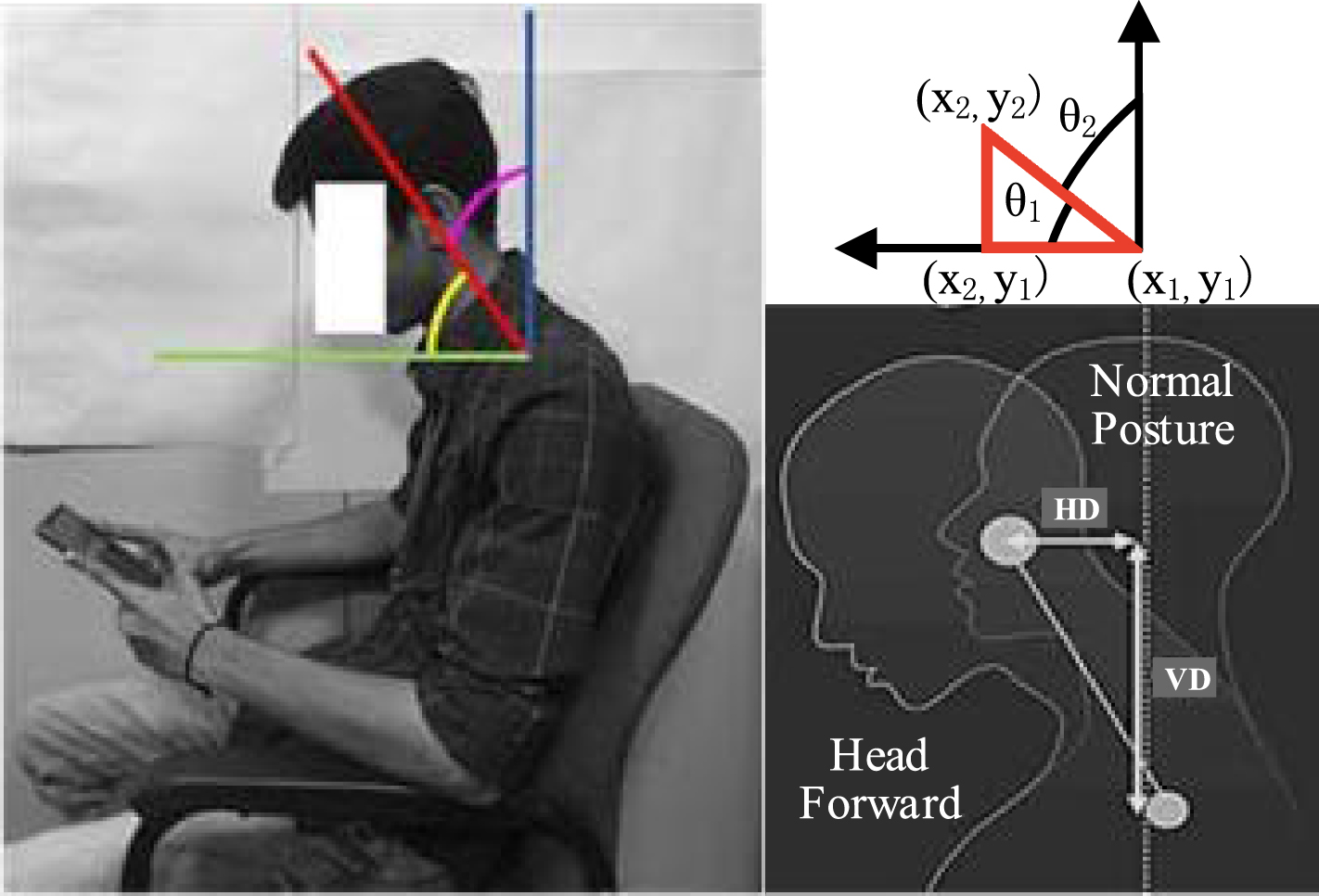
This postprocessing method utilized the RMS value at the task condition (i.e., TaskEMG) to normalize subsequent EMG data values. The result is presented as a percentage of normalized EMG, as shown in equation (a), which is utilized to establish the common ground while comparing the fatigue level of the participants. Green markers (i.e., region of interest [ROI]) were detected and tracked using the hue saturation value algorithm in OpenCV. The angle was identified between the two marks by using equation (b) (Fig. 3) where (x1, y1) are marker coordinates in the neck region and (x2, y2) is on the cap.
Head flexion angle measurement utilizing OpenCV method with representation.
Statistical analysis was performed for the average head flexion angle, muscle activity, and load acting on the C7 vertebra. One-way repeated measure analysis of variance (r-ANOVA) was performed to investigate the effect of the usage duration on muscle activity and flexion angle. Before the analysis, we tested the normality of the variables and the result showed that all the variables are normally distributed using Shapiro-Wilk test of normality. Also, the sphericity check was performed using Mauchly’s sphericity check and sphericity was violated with p < 0.00 indicating the rejection of null hypothesis. The epsilon (ɛ) parameter is used for correction work of degree of freedom of F-value of the Greenhouse-Geisser procedure. The significant effect of the duration and body posture was estimated by performing Greenhouse–Geisser correction with Bonferroni post-hoc analysis and using SPSS 25.0 software.
To examine the posture, RULA was performed on retrieved angle data. The load acting on the cervical C7 vertebrae was theoretically calculated using the head flexion angle at 0°, 15°, 30°, 45°, and 60°, using equation (c). The load was estimated concerning the head weight of the individual at 0°. The head weight was assumed to constitute approximately 8% of the total body mass [31]. As shown in Fig. 3, HD represents the lateral distance between the C7 and the center of mass (i.e., moment arm), VD represents the longitudinal distance between the C7 and the center of mass, and θ represents the head flexion angle.
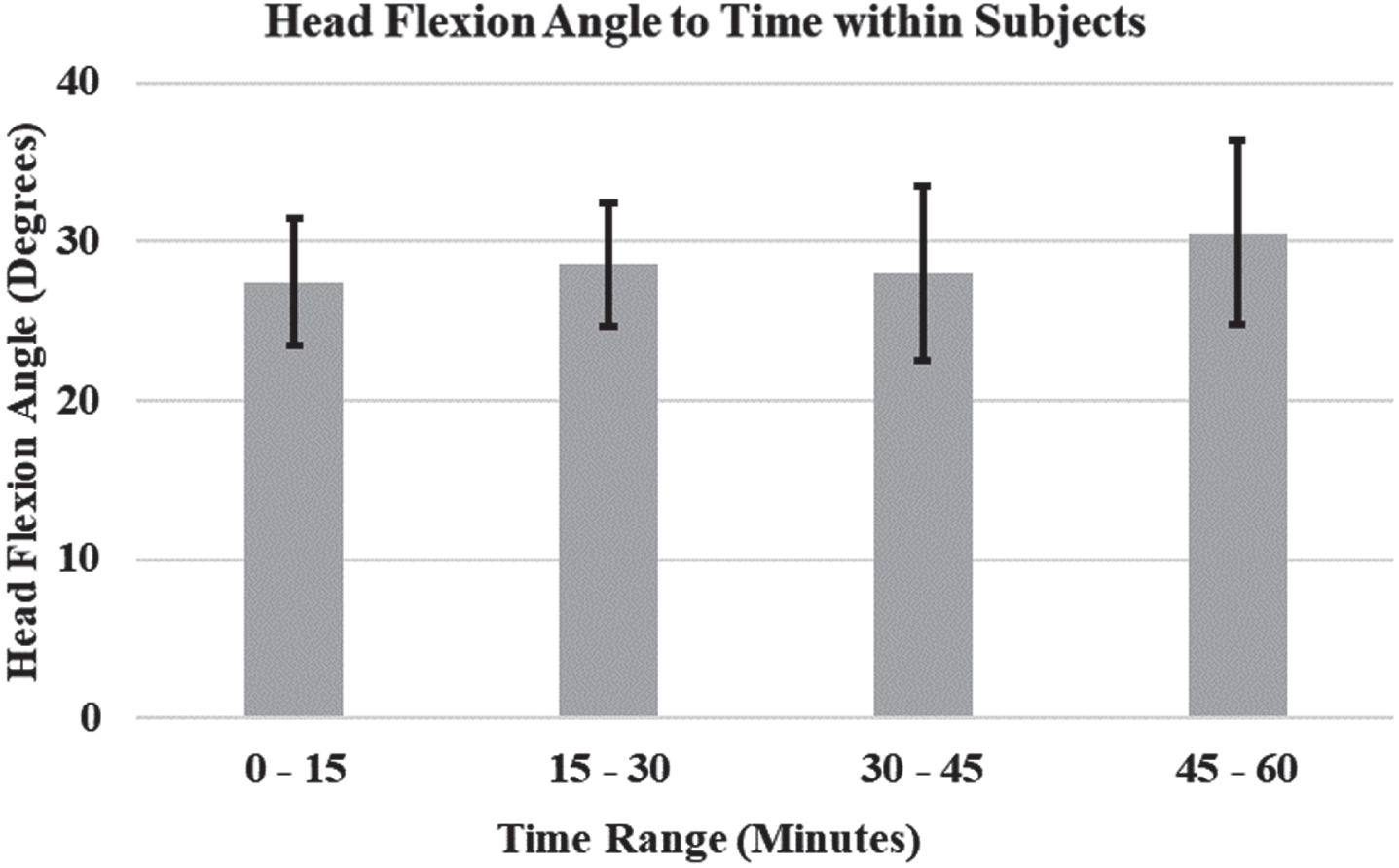
The pre-subjective data indicated that 94.7% of the participants utilized smartphones from a moderate to a very high level as part of their daily work practice. These findings of the pre-subjective assessment are demonstrated in Table 2. The average head flexion angle and muscle activity maintained by the participants at different time ranges are presented in Figs. 4 and 5. The load acting on the neck at 0°, 15°, 30°, 45°, and 60° of the head flexion angles was theoretically calculated and is presented in Fig. 6. The average discomfort level in the neck, shoulder, wrist and lower back experienced by the participants is illustrated in Fig. 7. One-way r-ANOVA with Bonferroni post-hoc test was performed utilizing Greenhouse–Geisser correction with pairwise comparison, and the results are summarized in Table 3. The average muscle activity significantly differed among different time ranges and the load acting on C7 significantly differed among different flexion angles (p < 0.01; Figs. 5 and 6) and pairwise comparison results are reported in Table 3. No significant difference in the head flexion angle was noted among different time ranges. Although a significant difference (p < 0.01) was observed in the discomfort level in the neck, it is not presented in Fig. 7 for legibility.
Head flexion angle to time within subjects.
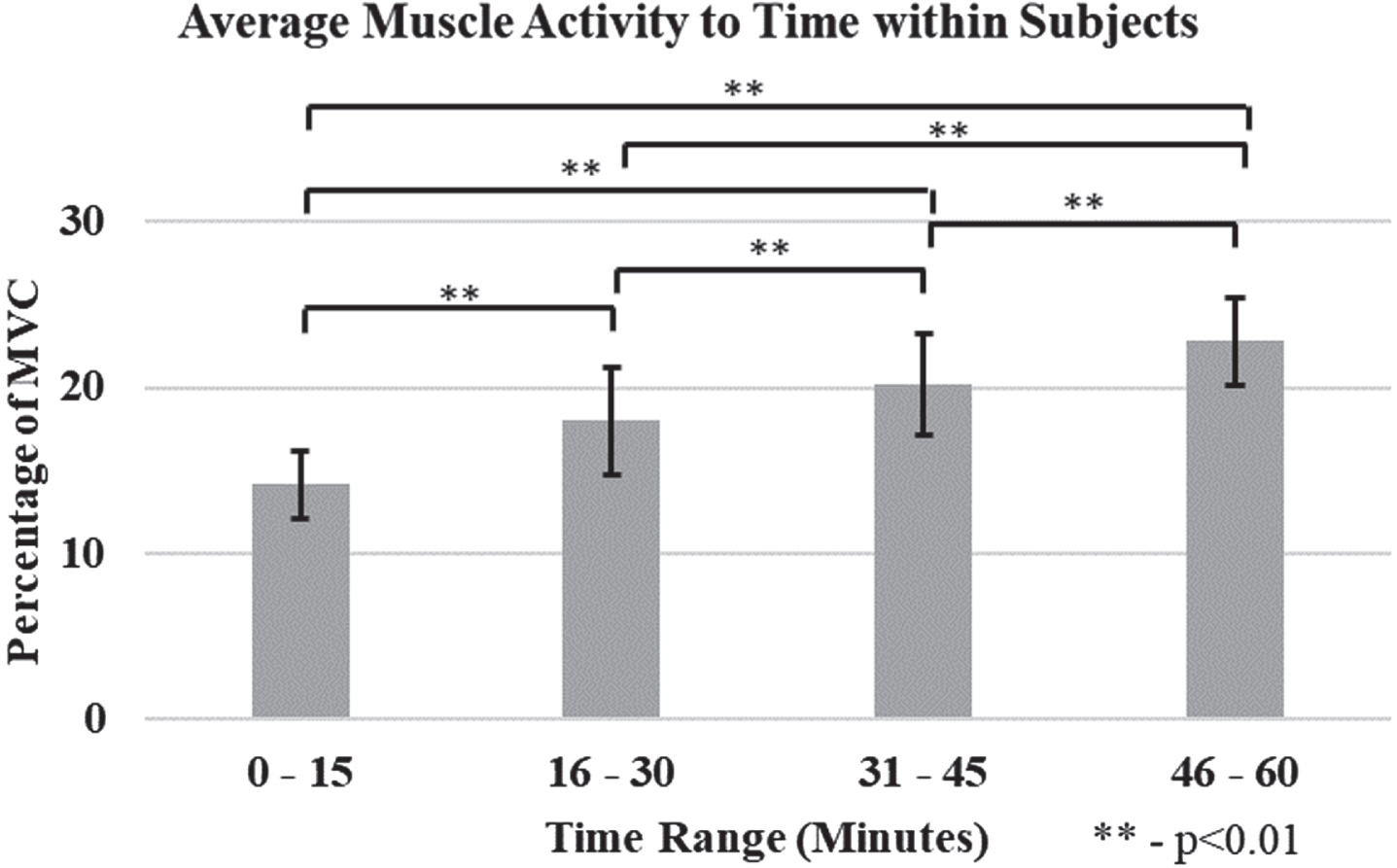
Muscle activity within subjects.

Load acting at different head tilt angles.

Discomfort level - post-subjective analysis.
Statistical analysis of muscle activity, flexion angles, load acting on C7 and subjective discomfort level
Pre-subjective questionnaire
In the pre-subjective assessment, 99% of the participants indicated that they used the smartphone for a minimum of 2-h per day and 97% reported they are sending a minimum of 25–50 messages per day. Besides calling, 86% and 80% of the participants reported texting and gaming as the major smartphone usage. Also, 95% of participants reported that they use a smartphone before sleeping which leads to insomnia [5]. Furthermore, 80% of participants felt excessive smartphone usage could lead to various physical and mental issues, of which, only 29% are following precautions. In other studies, participants reported that they were addicted and could not survive without smartphones [22] and 76% of the respondents confirmed that their smartphone usage was more than 4 hours [25].
Head flexion angle
On average, the participants maintained different head flexion angles (Table 3) throughout the test period [28° (0–15 min) < 29° (15–30 min) > 28° (30–45 min) < 31° (45–60 min)]. Although the head flexion angle maintained by the participant varied with time, no significant difference in the head flexion angle was noted among different time ranges (0–15, 15–30, 30–45, and 45–60 min). For the 1-h period, most of the participants used an average of 28.46°±4.04° for a duration of 43 min (more than 71% in an hour) in sitting posture. Hence, it is considered as maintaining increased head flexion angle or flexed posture for a prolonged period. A study reported that the flexion angle varied from 27.3° to 34.2° for one-hand browsing and from 35.7° to 41° for two-hand texting while walking [6]. While utilizing a smartphone, the head flexion angle reached up to 53.7° in 8-h of school duration [14]. The flexion angle is restricted to 15° while browsing on computers, whereas it can be between 20° and 37° while using a smartphone [20]. When measured using a 3D motion camera, the flexion angle ranged from 33° to 44° during texting in the sitting posture [19].
Muscle activity
The activity at the SCM muscle reached an average of 23% of MVC after 1-h continuous smartphone usage. Compared with the average muscle activity throughout the period, an increase of 14.13% (0–15 min), 17.99% (15–30 min), 20.16% (30–45 min), and 24.82% (45–60 min) was observed. When comparing muscle activity between the initial (0–15 min) to the end (45–60 min) of the experiment cycle, the muscle activity increased by 1.61 times. A significant difference (p < 0.01) with pairwise comparison was observed in average muscle activity among different time ranges. This increased muscle activity caused an increase in fatigue levels, which is in line with published studies [13, 16]. Excessive smartphone usage produces significant pain and stress on SCM muscle [8], leading to deformation in anatomical structure and nerve compression [32]. In a study, the muscle activity was 2.4% in the SCM muscle while using a smartphone for a 5-min duration [16], similarly, SCM muscle showed dominant results and experienced more fatigue in taping conditions while utilizing smartphones compared with non-taping conditions [15]. During a 10-min laptop typing, the SCM muscle activity increased to 1.64% in flexed head posture and 1% in neutral head position [29]. While lifting 10 kg for 1–2 s, the muscle activity reached 44% of MVC. However, in the current study, the muscle activity reached up to 23%, even without handling heavy loads, which is solely due to prolonged smartphone usage in flexed posture. This increased muscle activity would lead to severe damage or reduction in muscle stiffness [33].
Load acting
The load acting on the neck region (C7) was calculated for various head flexion angles; the load increased with the head flexion angle (i.e., 4.89±0.79 kgf at 0° to 22.60±3.64 kgf at 60°). The load at the neck increased to 10.13 kgf (15°), 15.06 kgf (30°), 18.45 kgf (45°), and 22.60 kgf (60°) compared with the neutral head position (5 kgf at 0°). A significant difference (p < 0.01) was observed with pairwise comparison in the load acting on C7 among different flexion angles. For the 1-h period, most of the participants used an average of 28.46°±4.04° for a duration of 43 min (more than 71% in an hour) in sitting posture, at 30° flexion angle the head weight increased to 15.06 kgf (3 times of actual weight). It resembles that a constant load of additional 10 kgf was acting on C7 for a duration of 43 min. This is because the change in the head flexion angle caused a shift in the center of gravity and gravitational pull [5, 21]. The findings indicated that an increase in the head flexion angle increased the load acting on the neck region (C7). This increased load at C7 could increase the intervertebral disc pressure and shear forces [34]. This behavior leads to capsular ligament laxity of the faced joint [33]. According to the RULA chart, a head flexion angle of > 20° is a high-risk factor and not an acceptable posture [20]. Thus, a low head flexion angle should be maintained.
Post-subjective analysis
The results of post-subjective analysis indicated that 80% of the participants reported a score of > 4 (uncomfortable) for the neck on a 5-point Likert scale. A significant difference (p < 0.01) was observed with pairwise comparison in the post-subjective analysis among different time ranges. The discomfort level at the neck increased exponentially while comparing discomfort at the neck between the initial (0–15 min) to end (45–60 min). Similarly, 18.8% stated that they developed MSD [18] and 95% experienced pain in the neck and upper extremities [25], which lead to increased discomfort [24] due to smartphone use.
The results of this study demonstrated that muscle activity increased after the prolonged usage of a smartphone, thus leading to muscle fatigue and discomfort. These results can be even implemented for the industrial workers working in flexed head and upper body postures of soldering, mems assembly, chip designing and assembly. The angle observed using the gyroscope and OpenCV showed that the participants maintained an average of 28.46°±4.04° for 43 min in the sitting posture. From the Table 3, it resembles that smartphone usage does not have significant effect on head flexion angle over time. But the smartphone usage of 1-hour has significant effect on muscle activity and post subjective assessment. Muscle has the ability of elasticity, where the muscle regains its original length after the removal or release of external force. The human musculoskeletal system comprises two types of fibers: (i) slow-twitch and (ii) fast-twitch. Slow-twitch fibers are suited for minimal forces with prolonged periods such as postural maintenance, whereas fast-twitch fibers are suited for short bursts of intense activities such as weightlifting and fast running [35]. Slow-twitch muscle fibers can resist fatigue for longer durations compared with fast-twitch muscle fibers. In this study, only slow-twitch fibers were considered. Hence, our finding of the increasing trend of muscle activity indicates that with extended smartphone use, the SCM muscle loses its resistive support movement due to postural maintenance. Therefore, maintaining the same posture for a prolonged period can increase muscle activity and lead to muscle fatigue. As shown in Fig. 4, the high standard deviation observed in the head flexion angle, particularly for 30–45 and 45–60 min, could result in the loss of resistive support movement in the SCM muscle. This reduction in resistive support movement in the SCM muscle can lead to pain/discomfort, causing individuals to alter or adjust their head flexion angle. This study demonstrated a finer correlation between flexion angles and muscle activity. The discomfort level at the neck increased gradually due to muscle fatigue. The theoretical estimation indicated that mechanical loads on C1–C7 increased by 4.62 times at 60° head flexion angle. In line with previous results, our findings indicated that an increase in the flexion angle leads to (i) an increase in mechanical loads on the neck by 3–5 times [21, 28] and (ii) more musculoskeletal and spinal disorders [5].
Limitations
In the pre-subjective evaluation, the participants reported different tasks, postures, and usage duration (3–4 h), this study examined the effects of only 1-h smartphone gaming in the sitting posture with a nonadjustable office chair on 40 male participants aged between 20 and 28 years. However, few other studies reported muscle fatigue–related analysis with a time range between 5–20 min [16, 29]. Furthermore, the analysis was limited to only one muscle (SCM) with male participants. In addition, only theoretical estimation of loads acting on C1–C7 was performed by using equation (c). In future female participants and more smartphone contents can also be included to have a better understanding of gender differences and content-based disorders.
Conclusion
An experiment was performed on 40 subjects, where the participants were allowed to play a smartphone game by using both the thumb fingers with hands resting on the armrests for 1-h in the sitting posture. The muscle activity at SCM muscle reached an average of 23% (p < 0.001) of MVC after 1-h continuous smartphone usage. Although many studies related to smartphones and their effects were conducted in different countries, India is still lacking in smartphone-related studies. This paper targets the effects of smartphone gaming on Indian adolescents. Therefore, this study analyzes the head flexion angle and muscle activity during smartphone gaming for a prolonged period of 1-h. The findings indicated that the prolonged usage of a smartphone with flexed angles caused a significant increase in muscle activity (1.61 times; p < 0.001), spinal loads (4.6 times; p < 0.001), and discomfort (2.9 times; p < 0.001) causing severe damage or reduction in muscle stiffness, MSD and increase in loads on the cervical vertebra. It is evident that various aspects (duration, posture, content) play a vital role in smartphone-related MSD and there is a potential risk of cervical spine problems. The methodology of the study can be implemented in various fields such as human-computer interaction, rehabilitation, industrial workers fatigue and athletes.
Ethical approval
The study received ethical clearance from the SRM Medical College Hospital and Research Centre (number 1980/IEC/2020) and was conducted in accordance with the Declaration of Helsinki.
Informed consent
Informed consent was obtained from all subjects involved in the study.
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
The authors thank the Robotics Lab of the Department of Mechanical Engineering and E-Mobility Research Centre from the SRM Institute of Science and Technology, Kattankulathur, India, for providing the required facilities for this research study.
Funding
This research received no external funding.