
Abstract
BACKGROUND:
Early self-assessment for work-related musculoskeletal disorders (WMSDs) is crucial in preventing severe symptoms and long-term consequences. Accessible tools are necessary for proactive management.
OBJECTIVE:
To validate the OfficeCheck web application as a screening tool to classify office workers as capable of self-management for specific symptoms of WMSDs or requiring professional consultation.
METHODS:
This study was conducted to determine the criterion-related validity of OfficeCheck using physical therapy assessment as the reference standard. In total, 223 office workers who work with a computer more than two hours a day with or without symptoms of WMSDs participated in this study. All of them were classified by self-assessment on the OfficeCheck process flow (Kappa = 0.841) and physical therapy assessment, respectively. For statistical analysis, classification numbers were calculated for sensitivity, specificity, false positive rate (FPR), false negative rate (FNR), positive predictive value (PPV), and negative predictive value (NPV).
RESULTS:
A total of 223 workers with a mean age of 38.9±9.0 years and mean body mass index (BMI) of 24.3±5.2 kg/m2 were illustrated. The most common areas of complaint were neck/upper back and lower back/hip. The results indicated that OfficeCheck had high sensitivity (95.1%), low specificity (42.0%), low PPV (38.0%), and high NPV (95.8%). The FPR was 58.0% and the FNR was 4.9%.
CONCLUSION:
OfficeCheck was found to have high sensitivity to classify office workers as capable of self-management for specific symptoms of WMSDs or requiring professional consultation. The use of OfficeCheck is thus recommended for self-detection and management to stop the consequences of WMSDs.
Introduction
Computer work often involves prolonged and awkward postures, coupled with repetitive tasks [1–3]. These factors can contribute to increased inflammation and decreased extensibility in structures such as muscles, nerves, and tendons [4]. The resulting work-related musculoskeletal disorders (WMSDs) initially manifest as localized symptoms, including pain, tingling, numbness, paresthesia, swelling, stiffness, restricted range of motion, and loss of strength. If left unaddressed, these symptoms can worsen and spread to other parts of the body [5].
Research has shown that the prevalence of WMSDs among office workers is significantly higher for individuals using computers for extended periods, particularly for over two hours daily [6]. In recent years, the increased adoption of remote work arrangements in response to the COVID-19 pandemic has further exacerbated WMSDs rates. The prevalence of WMSDs has been reported to be 63.0–77.6% overall, 38.0–50.0% for the neck, 15.7–50.2% for the shoulder, 16.0–38.0% for the upper back, and 34.0–58.1% for the lower back [3, 5, 7–10]. These rates increased to a range of 52.6–70.0% for the neck, 41.0–49.6% for the shoulder, 39.0–50.0% for the upper back, and 45.3–60.0% for the lower back during the work-from-home period [11–14]. Key contributing factors include poor posture, stress, and extended computer usage, especially when using laptops instead of ergonomically designed desktop setups [15–17]. It is therefore crucial for remote workers to prioritize early detection and prevention of WMSDs to ensure better management and long-term well-being.
Several postural assessment tools and self-report questionnaires have been developed to detect WMSDs, including the Ovako Working Analysis System (OWAS), Rapid Upper Limb Assessment (RULA), Rapid Entire Body Assessment (REBA) [17, 18], and the standard Nordic musculoskeletal questionnaire [7, 9, 11, 12, 14]. The modified Nordic questionnaire [5, 19], graded chronic pain scale [20], subjective severity of pain/stiffness [21], and the online self-reporting questionnaire on computer work-related exposure [2, 10] are also available. While these tools can provide valuable insights, they often require professional interpretation, which limits their accessibility and usefulness for many workers.
Optimal management of WMSDs involves prevention, which necessitates detecting symptoms at an early stage, such as work-related aches or pain that subsides after work [19]. Workers may struggle to identify these early signs or dismiss them until they worsen. This highlights the importance of making detection tools and resources more accessible and comprehensible to employees.
Current management strategies for WMSDs often tend to be area-specific rather than person-specific, which potentially limits their effectiveness. Examples of such strategies include Wellnomics WorkPace [20, 21], Stop and Stretch [22], I-preventive software [7], Break and exercise reminder software [23], and Artificial Intelligence– Assisted Health Programs [18]. However, Fioratti et al. (2022) demonstrated that symptom-specific self-management outperformed general recommendations in improving pain and function [24]. Consequently, a more personalized approach to WMSDs management is warranted.
In response to this need, the OfficeCheck web application was developed to detect symptoms and provide personalized self-management through self-assessment. The application addresses factors such as resting pain, pain with movement, limited range of motion, and special tests for musculoskeletal conditions. By offering a more individualized approach to WMSDs management, OfficeCheck aims to empower workers to take charge of their health and to enable them to identify and address potential issues before those issues become more severe. This proactive approach to WMSDs management is particularly crucial for remote workers, who may not have access to the same ergonomic resources and guidance available in traditional office environments.
This study aimed to validate the web application for classifying office workers using self-assessment. It was hypothesized that OfficeCheck would be sensitive as a screening tool for classifying office workers as either capable of performing self-management on specific symptoms of WMSDs or requiring professional consultation when necessary.
Materials and methods
A cross-sectional study was conducted to determine the criterion-related validity of the OfficeCheck web application, using physical therapy assessment as the reference standard. This study was approved by the Institutional Review Board of Mahidol University, Thailand (Reg. no. MU-CIRB 2018/242.1212).
Participants
The participants in this study were office workers from two company settings who attended an annual physical check-up. Individuals who met the criteria were invited to participate if they engaged in more than two hours of computer work daily, with or without WMSDs, and had internet access. Those who were unable to read and understand the Thai language were excluded from the study, as the first draft of the OfficeCheck web application was developed in Thai.
Sample size calculation
The sample size for this study was calculated based on a 63% prevalence of WMSDs from a study conducted in the same target population [5]. The formula used was:
where:
n is the sample size
Z α/2 is the Z-value corresponding to the desired confidence level (1.96 for a 95% confidence level)
P represents the prevalence of the condition (0.63 or 63% for WMSDs)
Se stands for the desired sensitivity (0.8 or 80%)
Sp represents the desired specificity (0.8 or 80%)
E refers to the desired level of precision (0.05 or 5%)
The estimated sample size was 221 office workers. A more recent study reported a 77.9% prevalence of WMSDs, resulting in a slightly smaller sample size of 196 office workers [9].
Physical therapists
The qualifications of the physical therapists were of utmost importance, as they served as the reference standard for this study. The five physical therapist examiners had graduated with at least a graduate diploma, master’s degree, or PhD in musculoskeletal physical therapy. They had work experience ranging from 10 to 30 years in the field of musculoskeletal physical therapy. All of them were informed about the study’s objectives, data collection protocol, inclusion/exclusion criteria, and assessment flow (i.e., red flags, chief complaints, stage of WMSDs, active movement, repetitive movement, other assessments, and, particularly, the severity and irritability of pain throughout the tests or movements). They were also given the operational definition of office workers who could perform self-management on specific symptoms of WMSDs and those requiring professional consultation.
The researcher provided mock cases and demonstrated how to conduct data collection (i.e., gender, age, weight, height, red flags, conditions of precaution, chief complaints, stage of WMSDs, pain scale, and pain irritability). The physical therapists were instructed to make decisions to classify cases as office workers capable of self-management on specific symptoms of WMSDs or requiring professional consultation.
Instruments
The study utilized the OfficeCheck web application, accessible at https://office-checker.web.app. Initially, the OfficeCheck flow was developed from a WMSDs self-assessment algorithm comprising questions on risk factors, chief complaints, excluded conditions, stages of WMSDs, pain severity scale, active movement tests, and active special tests [25]. This algorithm was validated by 12 professional physical therapists who had at least one publication in orthopedics or ergonomics within the past five years and worked in related fields for over 15 hours per week. The percent agreement for each self-assessment was over 80% using the modified Delphi technique, which involved face-to-face discussions in the first round and iterative questionnaires in the second and third rounds [25].
To develop OfficeCheck, language customization, video clip demonstrations, and questions related to self-assessment were adjusted for communication with software developers as a user interface. An example of the OfficeCheck interface is shown in Fig. 1. Before deploying OfficeCheck, its test-retest reliability was assessed in a focus group of 25 office workers. These workers were asked to register, log in, and follow the assessment instructions provided in the OfficeCheck web application. The process was repeated a day later at the same time. The correlation between the first and second outcomes of the reliability test was found to be 0.841 for the target classification (able to perform self-management or requiring professional consultation).
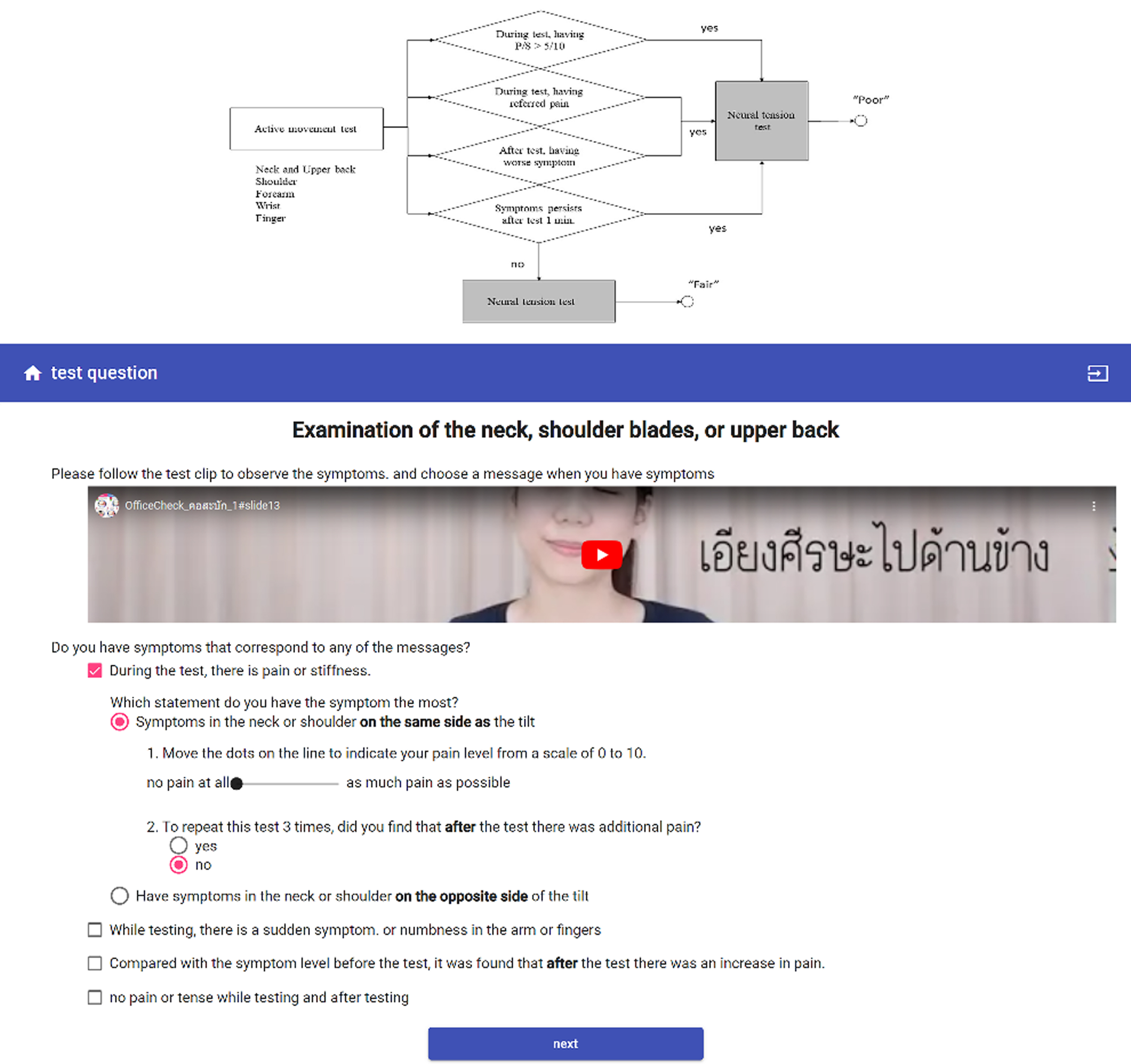
(Top) Process flow of a partial section of “the WMSDs self-assessment algorithm”. (Bottom) The application flow and arranged for developing OfficeCheck. Remark: The web application was originally in Thai but has been translated into English for publication.
Eligible participants were recruited through the company’s occupational health department. Those who met the inclusion criteria were informed about the study’s aims and protocol and asked to sign an informed consent form. To prevent learning bias that could influence their self-assessment, all participants were initially asked to complete the OfficeCheck web application. They were instructed to answer the questions as accurately as possible, reflecting their symptoms.
After completing the OfficeCheck assessment, participants were physically examined by one of the five physical therapists using a convenience sampling method. Importantly, both the participants and the physical therapists were blinded to the results of the OfficeCheck assessment to ensure unbiased evaluation.
Data management and analysis
The criteria for both conditions were established. Office workers requiring professional consultation were identified based on the presence of any of the following factors: red flags, impaired sensation, muscle weakness, symptoms outside the studied areas (neck and upper back, shoulders, arms, forearms, wrists, or hands), pain levels exceeding 5/10, or worsened symptoms during or after testing. Office workers considered capable of self-managing specific symptoms of WMSDs were those who either did not have symptoms or had symptoms that did not meet the criteria for requiring professional consultation. For participants with symptoms in multiple areas, the area with the most severe symptoms was used for analysis.
Statistical analysis was performed using the Statistical Package for Social Science (SPSS) Software for Windows, version 23.0. Two-by-two tables were created for both office workers able to self-manage specific symptoms of WMSDs and office workers requiring professional consultation, comparing the results from the OfficeCheck assessment and the physical therapy approach. Sensitivity, specificity, positive predictive value, and negative predictive value were calculated from these tables.
Sensitivity refers to the proportion of true positive results among all participants with the condition (requiring professional consultation), while specificity is the proportion of true negative results among all participants without the condition (able to self-manage specific symptoms of WMSDs). Positive predictive value (PPV) represents the proportion of true positive results among all positive results, and negative predictive value (NPV) denotes the proportion of true negative results among all negative results.
The false positive rate (FPR) is calculated as the ratio of false positive results to all individuals without the condition, and the false negative rate (FNR) is calculated as the ratio of false negative results to all individuals with the condition. These measures help evaluate the performance of the screening test or diagnostic tool and assist in determining its accuracy and usefulness in identifying and managing the target conditions.
Results
A total of 223 computer workers, with or without body complaints, participated in this study. There were 114 men (51.12%) and 109 women (48.88%), with a mean age of 38.9±9.0 years. Their body mass index (BMI) was 24.3±5.2 kg/m2 (mean±SD). The participants reported that their most common complaints were situated in the neck and upper back, low back and hip, shoulder and forearm, wrist, and hand, through both approaches (Table 1).
Characteristics of participants (n = 223)
Characteristics of participants (n = 223)
The data classifying office workers as being able to perform self-management for specific symptoms of WMSDs and office workers requiring professional consultation were reported by both the OfficeCheck web application approach and the physical therapy approach. There were 94 false positives, 3 false negatives, 58 true positives, and 68 true negatives (Table 2).
Numbers of cases comparing OfficeCheck and reference standard
These results were used to calculate the sensitivity (true positive rate), specificity (true negative rate), FPR, FNR, NPV, and PPV. The sensitivity was calculated as 58 / (58 + 3)=0.951, or 95.1%. The specificity was calculated as 68 / (68 + 94)=0.420, or 42.0%. The PPV was calculated as 58 / (58 + 94)=0.380, or 38.0%. The NPV was calculated as 68 / (68 + 3)=0.957, or 95.7%. The FPR was calculated as 94 / (68 + 94)=0.580, or 58.0%, and the FNR was calculated as 3 / (58 + 3)=0.049, or 4.9%.
The results of this study indicated that the OfficeCheck web application had high sensitivity (95.1%). This can be interpreted as the application being good at identifying positive cases (office workers requiring professional consultation), with only 3 false negative results out of a total of 61 actual positive cases. However, the specificity was low (42.0%), which means that the tool is good at identifying positive cases but not good at ruling out negative cases. OfficeCheck was as sensitive as a screening tool for the hypothesized classification of office workers capable of self-management on specific symptoms of WMSDs and office workers requiring professional consultation. For screening tests, high sensitivity is preferred, as it lowers the possibility of missing positive cases [26]. Similarly, OfficeCheck was developed to detect early symptoms of WMSDs in office workers.
However, a high sensitivity may also lead to a high number of FPR (58%). There were 94 false positives, which indicated that OfficeCheck generated many false alarms that could cause patient anxiety and unnecessary extra testing [27]. However, WMSDs are less life-threatening than other serious diseases such as cancer. Thus, having positive results from the application may help to improve awareness among workers about managing WMSDs, and health professionals can handle the cases more easily because they are not too severe. In addition, the high FPR might occur because positive cases (office workers requiring professional consultation) were set at low cut-off criteria, as self-testing considered users’ safety first. For example, the question “Do you have any numbness, tingling, or weakness?” was one condition that could lead to a high FPR, as symptoms of numbness are considered a neurological sign that requires specific assessment [28, 29]. Similarly, a low PPV at 38% indicated that a positive result was more likely to be a false positive result. To make these rates more acceptable, the cut-off criteria may need to be adjusted.
The NPV was 95.7%, which meant that 95.7% of negative results (office workers being able to do self-management on specific symptoms of WMSDs) from OfficeCheck identified office workers who can truly determine to do self-management. The FNR was 4.9%, which indicated that OfficeCheck did err in reporting negative results (office workers capable of self-management on specific symptoms of WMSDs) when the office workers were actually reporting positive results (i.e., they required professional consultation), but this value may be at an acceptable level because WMSDs are non-threatening diseases. Additionally, re-assessment within two weeks after receiving the specific recommendation was suggested to determine the change after following the recommendation from the application.
The findings from this study suggest that OfficeCheck could be used as a screening tool, but not as a diagnostic tool or a substitute for seeing physical therapists or medical professionals. Office workers who are concerned about their symptoms, particularly in the neck, upper back, shoulder, forearm, wrist, hand, lower back, and hip areas, can use OfficeCheck straight away. OfficeCheck can determine and classify the severity level of WMSDs in workers, indicating whether they can manage the disorders by themselves or need to see physical therapists or medical professionals. In contrast, previous tools were used only for identifying prevalence, risk factors, prevention, and general management [2, 5, 7, 9–12, 14, 18, 30, 31]. Additionally, there is software available on workers’ desktop PCs or laptops to provide regular breaks and exercises for computer users [7, 18, 20–23]. However, those software programs do not specifically focus on classifying the disorders as the current tool does. This current tool can also exclude red flags for musculoskeletal system disorders, which can indicate serious concerns and require specific investigation.
According to the prevalence of WMSDs, the most common areas of complaint were in the neck and upper back, low back and hip, shoulder and forearm, and wrist and hand, as reported by both the OfficeCheck and physical therapy approaches. Similarly, previous studies have illustrated that the most common areas of symptoms are also the neck and low back regions [3, 5, 7–14]. However, the number of cases reported by the physical therapy approach in each area was higher than the number reported by OfficeCheck. This difference may arise from the fact that physical therapists can holistically evaluate the whole-body system and treat the symptoms according to the causes rather than the local symptoms [32, 33].
The limitations of this study include the fact that OfficeCheck was initially developed and tested in Thai. For further studies, OfficeCheck should be developed in other languages to facilitate widespread use. The effects of using OfficeCheck as an intervention in reducing the incidence and prevalence of WMSDs, direct and indirect costs, sick leaves, and the workload of physical therapists or medical professionals could be of interest and warrant further investigation. The cut-off criteria for detecting cases should be adjusted to reduce the FPR. Because the assessment protocol in OfficeCheck was derived from musculoskeletal tests, it may also be applicable to other target populations, such as workers involved in sedentary work and manual material handling.
An implication of this study is that utilizing OfficeCheck can help determine which workers can perform self-management for specific symptoms of WMSDs and which workers require professional consultation. This has the advantage of allowing early detection of WMSDs that can be managed by workers, potentially leading to a reduction in the workload for medical professionals. By identifying and addressing WMSDs early on, this tool can contribute to improved workplace health and well-being, ultimately benefiting both employees and employers.
Conclusion
OfficeCheck demonstrated high sensitivity and a low FNR, which indicates its potential as a screening tool for detecting symptoms of WMSDs in office workers. This tool can aid in the early identification of individuals who may be capable of self-management or those who need professional consultation for managing WMSDs, ultimately contributing to improved workplace health and well-being.
Footnotes
Ethical approval
This study was approved by the Institutional Review Board of Mahidol University, Thailand (Reg. no. MU-CIRB 2018/242.1212).
Informed consent
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional research committee. Informed consent was obtained from all participants included in the study.
Conflict of interest
The authors have no conflicts of interest to declare.
Acknowledgments
The authors express their sincere appreciation to the Faculty of Physical Therapy, Mahidol University, Thailand for their support and encouragement throughout this study. They also extend their appreciation to the physical therapy seminar organizing team for providing the opportunity to meet with participants and engage with experts.
Funding
The authors are grateful for the financial support of the National Research Council of Thailand under the Young Researcher Development Program (NRCT748261).