
Abstract
BACKGROUND:
Neck-shoulder and arm musculoskeletal disorders in smartphone use have attracted increasing attention.
OBJECTIVE:
This study aimed to examine the effect of different lying postures and task types by comparing the electrooculography (EOG) responses, perceived discomfort, and the activity of neck-shoulder and arm muscles while using a smartphone on the bed.
METHODS:
Twenty participants were recruited to perform 30-min tasks (texting/ watching video) while holding the smartphone in three different lying postures (half-lying/lying/side-lying). Subjective discomfort, muscular activities including the abductor pollicis brevis (APB), upper trapezius (UT), and extensor carpi radialis (ECR), and EOG signals were simultaneously monitored.
RESULTS:
The results showed that the perceived discomfort of measured body parts increased significantly over time in all postures. Watching video significantly increases muscle activities of APB and UT and decreases blink frequency and blink duration. Compared to lying or half-lying, the side-lying posture has the highest blink frequency, blink duration, and muscle activities in ECR and UT.
CONCLUSION:
The findings of this study indicate that side-lying posture should be avoided while using a smartphone on the bed. It provides an understanding of the association between the postures of using smartphones on the bed and fatigue, which can help prevent muscle and visual fatigue in smartphone use.
Introduction
Nowadays, the smartphone has become one of the most convenient media for people in communication and entertainment [1]. Approximately 56% of the population of the United States uses smartphones, spending an average of 5.1 hours per day on smartphones [2]. With the enhancement of entertainment and smartphone portability, people can use smartphones anytime and anywhere. In this trend, using smartphones in bed before sleeping has also become a prevalent way [3]. However, evidence showed that along with the popularity of using smartphones, musculoskeletal disorders have been increasing rapidly, especially in the young population [4]. Musculoskeletal disorders were found in 18.5% of the participants, and these symptoms were most usually associated with body parts such as the thumb and elbow in mobile phone users [5]. Prolonged use of smartphones also might lead to musculoskeletal disorders in other body parts, including the shoulder [6], upper back [7], and neck [8]. In addition, it is harmful to vision to use a smartphone for a long time. The blue light emitted by smartphone screens can reduce blink frequency and lead to blurred vision, insomnia [9], and other visual problems [10].
Due to the dramatic increase in the prevalence of smartphone-related musculoskeletal disorders, numerous studies have been conducted to explore the relationship between using smartphones and musculoskeletal disorders. Syamala et al. investigated the effect of support on neck and shoulder muscle activity while sitting and using smartphones and found that backrests reduced neck and shoulder muscle activity [7]. Evidence has been found that the muscle fatigue of APB increased significantly over time during playing a smartphone game continuously for 30 min [11]. The relationship between daily calling duration and discomfort scores of the neck in young students has also been explored, and a positive correlation has been found between them [12]. Vahedi et al. evaluated the effects of task types (texting, watching a video, and reading) on muscular activity when using a smartphone while sitting or standing. The results showed that the reading task had the highest level of neck muscle activity, and sitting had a greater neck flexion for all tasks [13]. These studies suggest that the postures, duration, and task types of smartphone use may significantly influence the risk of musculoskeletal symptoms.
However, previous studies on the use of smartphones mainly focused on musculoskeletal disorders while sitting or standing. The use of smartphones with lying postures on bed has been rarely investigated, and the relationship between using smartphones and visual fatigue remains unknown. Although Exelmans and van Bulck [10] investigated the effects of using a smartphone on the bed, and the results suggest that using a smartphone at bedtime is negatively related to sleep outcomes in adults. However, their study mainly examined the effects of using smartphones before bed on sleep quality and health rather than the effects of musculoskeletal symptoms. To the best of our knowledge, only Ahn et al. [14] investigated the impact of smartphone use on neck muscle activity while watching videos in different lying postures. However, they only collected EMG data of 60 seconds and hardly provided insight into the effects of use duration. Furthermore, the effects of the half-lying posture and task types performed with smartphones on musculoskeletal disorders were not investigated in their studies.
Since there were few studies focused on the effects of using a smartphone on the bed, we proposed a mixed-design experiment combining subjective reporting, electromyography (EMG), and electrooculography (EOG) technologies to investigate the effects of lying postures, duration, and task types on users’ perceived discomfort, muscle activity, visual fatigue while using a smartphone on the bed. The findings will provide implications for using a smartphone on bed in health.
Method
Participants
Twenty students (ten females) were randomly recruited from a local university as participants. One female participant was excluded because the sensor collecting data fell off during the experiment. The remaining (19) participants had an age range of 20–25 years (M = 22.3, SD = 1.84). The participants were all right-handed and did not have any musculoskeletal disorders. Of all participants, 8 had normal vision, and 11 had myopia of 300 degrees or less. All participants reported not wearing glasses while playing with their smartphones in bed. Therefore, all participants, whether myopic or not, did not wear glasses to correct their vision during the experiment. The study protocol was approved by the Ethics Committee of the local university. Informed consent was obtained from each participant, and each participant was given a $10 gift card as compensation for their participation after the experiment.
Experimental design
A mixed experimental design was adopted for this study. Half of the participants were asked to perform a texting task in three different lying positions (half-lying, lying, and side-lying). In contrast, the others were asked to complete a watching video task in the experiment. Bodin et al. indicated that letting individuals choose by themselves was better than “one-size-fits-all” recommendations about using the smartphone [15]. Therefore, the participants freely adjusted the details of the lying postures, such as arm height and eye angle, according to their habits of using smartphones in bed. The lying postures adopted by most participants are shown in Fig. 1. In the half-lying and the lying postures, the upper arms were placed on the bed. The line of sight was horizontal downward, and the viewing distance was about 30 cm (Fig. 1a and 1b). In the side-lying, the right arm was placed under the bed, and the left arm was on the top, the line of sight was horizontal down, and the viewing distance was about 30 cm (Fig. 1c). In the watching video task, the smartphone was placed horizontally. Participants were asked to hold the phone with both hands, and all participants watched the same video called “Your Name,” a Japanese animated romantic fantasy film with which the participants were unfamiliar. Participants were asked to type with both hands in the texting task, and the keyboard was set to 26 keys for typing.
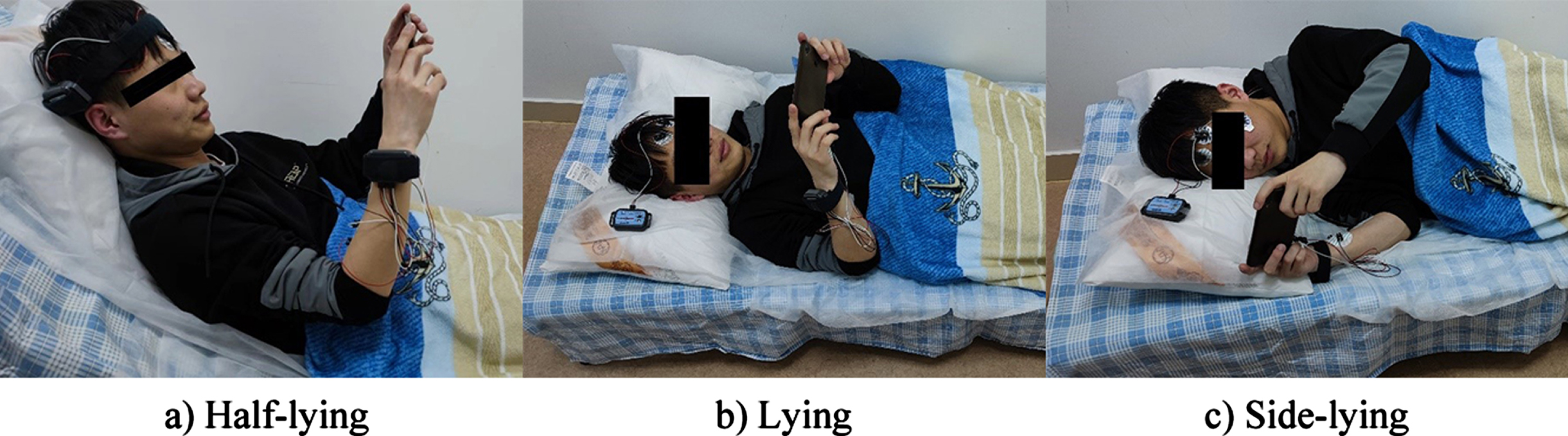
Three different postures of using the smartphone.
The independent variables of this experiment were lying postures, task types, and task duration. The dependent variables of this study were the perceived discomfort, visual fatigue, and muscle activities, including the abductor pollicis brevis (APB), the upper trapezius (UT), and the extensor carpi radialis (ECR). Previous studies have identified that the increase in the EMG root mean square (RMS) amplitudes indicate a more significant muscle activity [16], and the increase in the blink frequency and blink duration indicate visual fatigue [17]. Hence, the normalized EMG root mean square (NRMS) calculated from EMG signals was used to measure the muscle activities, and blink frequency and blink duration calculated from EOG signals were used to measure visual fatigue.
The perceived discomfort measures, including muscle discomfort and visual discomfort, were also evaluated in this study. Muscle discomfort for the relevant body parts was measured using a 10-point scale, which ranged from 1 = extremely comfortable to 10 = extremely uncomfortable [18, 19]. Visual discomfort was comprehensively evaluated using the visual fatigue questionnaire proposed by Heuer [20]. The questionnaire consists of 6 items (I have trouble seeing things, I have discomfort around my eyes, my eyes feel tired, I feel numb, I feel headache, and I feel dizzy when I look at the screen). Participants were asked to use the 1–10 Likert scale in rating these items, and the scores of the six items were averaged as the discomfort score of eyes. All subjective measures were administered every 10 min over the 30 min period. Since playing with a smartphone in bed usually occurs before going to sleep, the experiment was conducted in a special laboratory with light, sound insulation, a room temperature of about 20 degrees Celsius, and a constant luminance of 75 lx to more realistically simulate the bedtime environment.
To control the influence of other non-essential factors, all participants in this experiment used the same smartphone, and the Honor Play smartphone was finally selected as the experiment material. The screen size of this smartphone is 6.3 inches, the length is 157.91 mm, the width is 74.27 mm, the thickness is 7.48 mm, and the weight is about 170 g. The screen brightness was set to 30%, the most suitable brightness for the experimental environment, and was determined by the default function of the smartphone’s automatic screen brightness adjustment function.
A Biopac MP150 EMG amplification system (Biopac, USA) was used to record the EMG and EOG signals. The signals were saved on the computer at a sampling rate of 1000 Hz by Acqknowledge 4.2 software (Biopac, USA), which can filter the raw EMG data for later analysis. Two electrodes spaced approximately 2 cm apart were placed to collect EMG signals in each of the three muscles (APB, UT, ECR). Positive, negative, and ground electrodes were placed above the left eye, below the left eye, and the forehead, respectively, to collect EOG signals. The skin for placing electrodes was cleaned with alcohol swabs.
Procedure
Upon their arrival, participants received a brief description of the experimental protocol and were required to complete a demographic questionnaire (including gender, age, and years of using smartphones). Then participants were asked to take off their shoes, then lie on the bed. The quilt and pillow with disposable sheets and pillowcases were utilized to simulate actual lying postures. The experiment was conducted in three blocks, each block requiring the participant to complete experimental tasks in one posture. Figure 1 shows the three different postures of using a smartphone. The order of the three blocks was counterbalanced among the participants. At least 24 h rest period was set up between each block to minimize residual fatigue [21]. Before the formal experiment, the participant was asked to relax and lie quietly flat on the bed for one minute. Physiological data for this period was recorded as a baseline to calibrate the recorded physiological data during the task. Perceived discomfort measures were collected every 10 min over the 30 min period. The experimental schema is shown in Fig. 2.
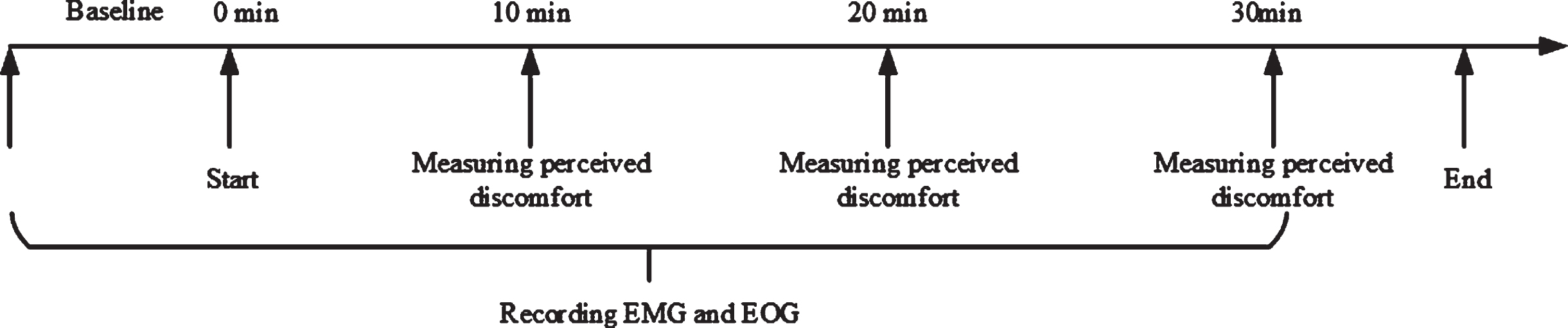
Experimental schema.
EMG and EOG data were processed by NeuroKit2, a python-based physiological signal processing software [22]. The EMG data was band-pass filtered at 20–450 Hz using a sixth-order Butterworth filter [23]. The RMS value of the EMG signal was calculated by selecting 10 s of EMG data from the measurement timestamp respectively. Then the RMS values were normalized by dividing the values by the average of three baseline values, respectively, for each block [24].
The EOG data was band-pass filtered at 1.5 15 Hz using a fourth-order Butterworth filter. Then the two-minute EOG data between the two adjacent timestamps were extracted, and the blink detection method implemented in brainstorm was used to calculate the blink frequency and the average blink duration [25].
In this study, the effects of tasks, postures, and duration on the dependent variables were assessed using a group by task (2×2) two-way repeated measures analysis of variance (ANOVA). The analysis was conducted using JASP 0.16.2 [26] with an α level of 0.05. Post-hoc analyses with Bonferroni adjustment were used for multiple comparisons.
Results
Perceived discomfort
Tables 1 and 2 show the statistical descriptions and ANOVA results of perceived discomfort scores of hand, arm, neck, and eye, respectively. Figure 3 shows the variation of perceived discomfort scores of hand, arm, neck, and eye over time in different postures and task types. Regarding the discomfort score of hand, the ANOVA results showed that there is a significant difference in time points [F(1.086, 18.469) = 57.390, p < 0.001, η p 2 = 0.771] and Post-hoc test results showed that the discomfort score increased significantly over time. Although the average discomfort score of the texting task was higher than the watching video task, no significant difference was found in task types [F(1, 17) = 3.555, p = 0.077, η p 2 = 0.173] and postures [F(1.662, 28.246) = 0.815, p = 0.432, η p 2 = 0.046]. No significant interaction effects were found between time points, postures, and task types.
Mean and standard deviation of perceived discomfort scores in different body parts
Mean and standard deviation of perceived discomfort scores in different body parts
The results of ANOVA analysis for perceived discomfort scores in different body parts

Perceived discomfort scores. a) discomfort score of hand. b) discomfort score of arms. c) discomfort score of the neck. d) discomfort score of eyes. Error bars represent the standard error.
Regarding the discomfort score of the arm, the ANOVA results showed that there is a significant difference in time points [F(1.192, 20.27) = 89.569, p < 0.001, η p 2 = 0.84] and post-hoc test results showed that the discomfort score increase significantly over time. No significant difference was found in task types [F(1, 17) = 1.950, p = 0.181, η p 2 = 0.103] and postures [F(1.845, 31.371) = 3.042, p = 0.066, η p 2 = 0.152] and no significant interaction effects were found between time points, postures and task types.
There is a significant difference in time points for the perceived discomfort of the neck [F(1.157, 19.677) = 70.619, p < 0.001, η p 2 = 0.806], and post-hoc test results showed that the discomfort score increased significantly over time. No significant difference was found in task types [F(1, 17) = 2.075, p = 0.168, η p 2 = 0.109] and postures [F(1.745, 29.659) = 0.916, p = 0.399, η p 2 = 0.051] and no significant interaction effects were found between time points, postures and task types.
Results showed that there is a significant difference in time points for the perceived fatigue of eyes [F(1.086, 18.468) = 50.742, p < 0.001, η p 2 = 0.749] and Post-hoc test results showed that the discomfort score increased significantly over time. No significant difference was found in task types [F(1, 17)<0.001, p = 0.995, η p 2 < 0.001] and postures [F(1.730, 29.417) = 1.004, p = 0.368, η p 2 = 0.056] and no significant interaction effects were found between time points, postures and task types.
Tables 3 and 4 show the statistical descriptions and ANOVA results of the NRMS of APB, ECR, and UT, respectively. Regarding muscle activity of APB, the ANOVA results of normalized RMS showed that there are significant differences in task types [F(1, 17) = 6.833, p = 0.018, η p 2 = 0.287] and time points [F(1.934, 32.884) = 3.331, p = 0.050, η p 2 = 0.164]. No significant interaction effects were found between time points, postures, and task types. The Post-hoc test result showed that the texting task has a lower normalized RMS than the watching video task (p = 0.018). The differences in normalized RMS were marginal significance at the two time points of 10 min and 20 min (p = 0.081), with the value at the time point of 20 min being higher than at the time point of 10 min. No significant differences were found at the time points of 10 min and 30 min (p = 0.144) and the time points of 20 min and 30 min (p = 0.787).
Mean and standard deviation of the NRMS of APB, ECR, and UT
Mean and standard deviation of the NRMS of APB, ECR, and UT
The results of ANOVA analysis for the NRMS of APB, ECR, and UT
The ANOVA results of muscle activity of ECR showed that there was a significant difference in postures [F(1.06, 18.015) = 17.117, p = 0.001, η p 2 = 0.502], and no significant interaction effects were found between time points, postures and task types. The result of post-hoc tests showed that side-lying has a higher normalized RMS than lying (p = 0.003) and half-lying (p = 0.001). No significant differences were found between lying and half-lying.
Regarding muscle activity of UT, the ANOVA results of normalized RMS showed that there are significant differences in task types [F(1, 17) = 10.044, p = 0.006, η p 2 = 0.371] and postures [F(1.482, 25.191) = 9.568, p = 0.002, η p 2 = 0.360]. No significant interaction effects were found between time points, postures, and task types. The post-hoc test result showed that the texting task has a lower normalized RMS than the watching video task (p = 0.006), and side-lying has a higher normalized RMS than lying (p = 0.016) and half-lying (p = 0.008). No significant differences were found between lying and half-lying. Figure 4 shows the NRMS of APB, ECR, and UT at measured time points in different postures and task types.
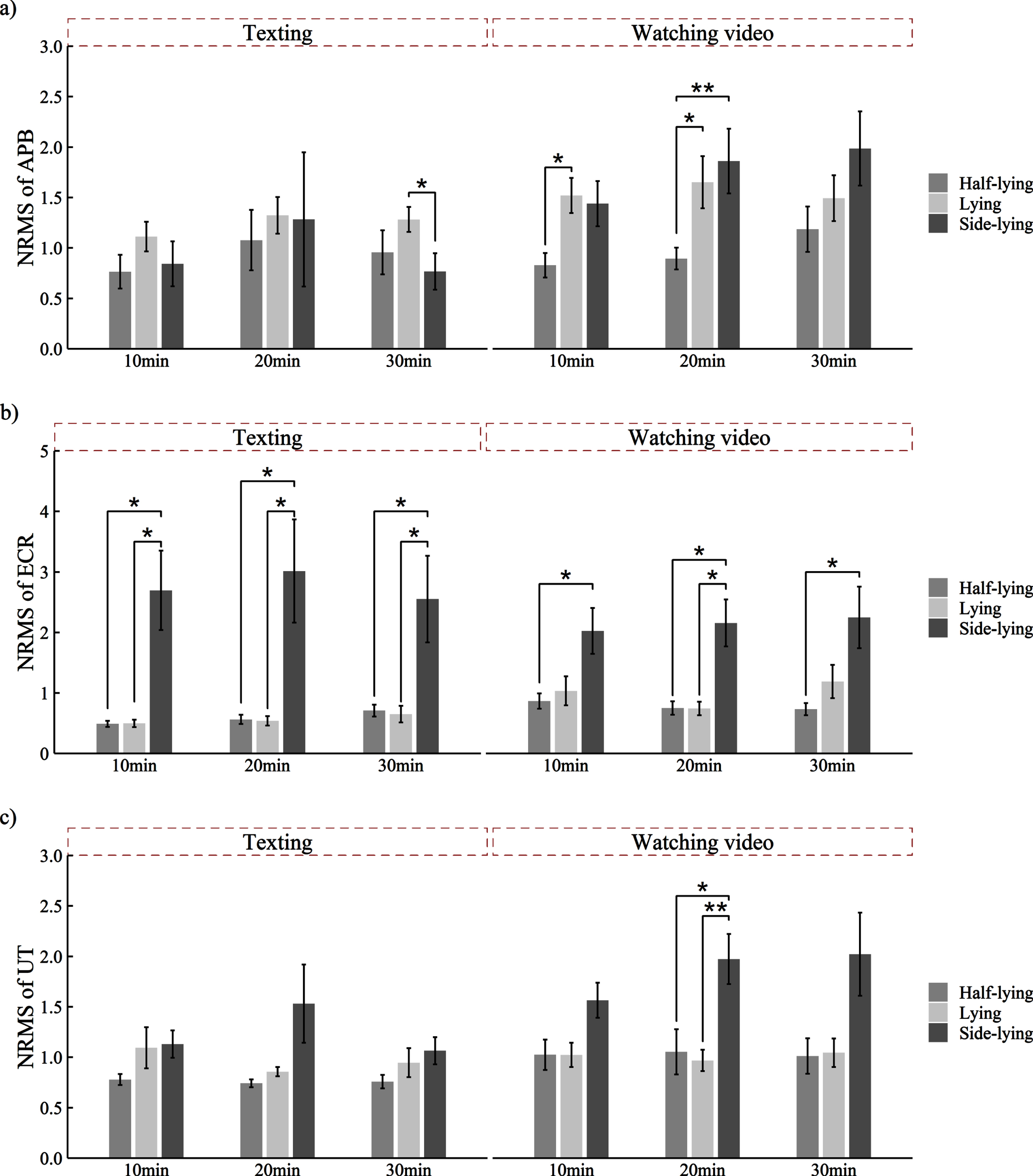
The NRMS of APB, ECR, and UT. a) The NRMS of APB. b) The NRMS of ECR. c) The NRMS of UT. Note: error bars represent the standard error, and *depicts p < 0.05, **p < 0.01, and ***p < 0.001.
Tables 5 and 6 show the statistical descriptions and ANOVA results of blink frequency and blink duration, respectively. Regarding the blink frequency, significant differences were found in different tasks [F(1, 17) = 5.624, p = 0.03, η p 2 = 0.249] and postures [F(1.961, 33.329) = 11.858, p < 0.001, η p 2 = 0.411] and their interaction effect [F(1.961, 33.329) = 4.205, p = 0.024, η p 2 = 0.198]. Further analysis of the simple effect of task types showed that the texting task had a lower blink frequency than the watching video task (p = 0.001) when the smartphone was used in the side-lying posture. However, the difference was insignificant when the smartphone was used in the lying posture (p = 0.301) or half-lying posture (p = 0.561). The simple effect of postures showed that side-lying had a higher blink frequency compared with the lying (p < 0.001) half-lying (p < 0.001) in the watching video task, and no significant differences were found between postures in the texting task.
Mean and standard deviation of blink frequency and blink duration
Mean and standard deviation of blink frequency and blink duration
The results of ANOVA analysis of blink frequency and blink duration
Regarding the blink duration, the ANOVA results showed that there are significant differences in task types [F(1, 17) = 5.949, p = 0.026, η p 2 = 0.259] and postures [F(1.999, 33.978) = 6.909, p = 0.003, η p 2 = 0.289]. No significant interaction effects were found between time points, postures, and task types. The Post-hoc test result showed that the texting task has a lower blink duration than the watching video task (p = 0.026), and side-lying has a higher blink duration than lying (p = 0.011) and half-lying (p = 0.016). No significant differences were found between lying and half-lying. Figure 5 shows the blink frequency and blink duration at measured time points in different postures and task types.

The blink frequency and blink duration at each time point in different postures and task types. a) The blink frequency. b) The blink duration. Note: error bars represent the standard error, and *depicts p < 0.05, **p < 0.01, and ***p < 0.001.
In a mixed-design experiment, this study examined the effects of lying postures, duration, and task types on perceived discomfort and muscle activity while using a smartphone on the bed. EMG and EOG signals were recorded during this experiment. The results showed that the discomfort score of measured body parts had significant differences at the three measured time points. However, duration had insignificant effects on the muscle activities of ECR and UT, blink frequency, and blink duration apart from the muscle activity of APB. Postures had significantly diverse effects on the muscle activity of ECR, and task types had significantly different effects on muscle activity in the APB. Both had significantly various effects on the muscle activity of UT and blink frequency and blink duration.
Effect of lying postures
In this study, no significant differences were found in the perceived discomfort and muscle activity of APB between different postures. However, side-lying has higher muscle activities in ECR and UT as well as blink frequency and blink duration compared to lying and half-lying. In the side-lying posture, the body was turned to the right, and the right arm was placed on the bed. When participants held the phone with both hands, in addition to the weight of the smartphone itself, the weight of the left arm also was loaded on the right arm, which increased the force exerted on the right arm. Therefore, it can be inferred that this is probably the reason for the muscle activity increase.
Furthermore, due to the muscle activity of UT being associated with the weight of the upper limb [27], more force exerted on the neck may increase the muscle activity of UT. In the side-lying and lying postures, participants held the phone with both hands similarly, and there was no significant difference in the muscle activity of the APB, ECR, and UT. These findings showed that the force exerted on the right arm was an important factor resulting in muscle activities. Moreover, the weight of the heads and necks of participants was supported entirely by the pillow in the lying and half-lying position. When the body part was supported, it would effectively reduce muscle activity [28, 29]. However, the body was turned to the right in the side-lying position, and the neck could not be supported entirely by the pillow. The bending of the neck resulted in the muscle activity of UT increased [14]. Continuous muscle activation is a key contributing factor to chronic musculoskeletal disorders. Correcting awkward postures while using mobile devices is an essential strategy for reducing or preventing musculoskeletal disorders in mobile device users [30]. This study’s results show that the side-lying posture is the least recommended when playing a smartphone in bed compared to the half-lying and lying postures.
No significant difference was found between lying and half-lying in this study. A potential explanation is that the postures of using the smartphone in lying and half-lying are similar, such as the neck being supported by a pillow and the arms being unsupported, and the similar postures elicited similar muscle activities. However, Udomboonyanupap et al. [31] found that a bed with a trunk angle of around 120–140 degrees was preferable for using a smartphone on the bed, which is inconsistent with the findings of this paper. In their study, the leg’s discomfort significantly affected the participants’ evaluation, which contributed to differences in results. The effect of lying and half-lying postures on muscle activity in other body parts can be further compared in the future. In addition to differences in muscle activity, the higher blink frequency and longer blink duration were detected in the side-lying position. Side-lying sleeping postures usually do result in significant elevations of intraocular pressure (IOP) [32], which easily induces eye fatigue and results in differences in blink frequency and blink duration. Although there was no significant difference between postures in perceived discomfort, side-lying might not be a good posture for using a smartphone regarding muscle activity, blink frequency, and blink duration.
Effect of task types
Gustafsson et al. investigated APB’s muscle activity during the texting and talking tasks and found APB’s muscle activity was significantly lower than the talking task [33], which is consistent with the findings of this study. In this study, texting has lower muscle activities in APB and UT compared to watching video task. To avoid obscuring the screen, the participants had to hold the smartphone’s edges with their fingers in the watching video task. In contrast, screen obscuring did not affect text input in the texting task, participants could support the phone with their palms, and less grip force was needed to hold the phone. One of the main functions of the thumb is to grip [11], and more grip force caused higher muscle activity in the APB while watching video. Vahedi et al. [13] found that texting with a one-handed grip increased muscle activity in the right UT muscle compared to a two-handed grip, which is consistent with the findings of the present study. In addition, participants continuously pressed keys with both thumbs in the texting task, which increases thumb movements, and moderate exercise can reduce muscle fatigue [28, 34].
However, some studies investigating the effects of using smartphones in sitting or standing postures have shown that texting resulted in the highest level of neck flexion and higher muscle activity of neck muscle [35, 36], which is inconsistent with the findings of the present study. An important reason is that the participants’ neck was supported by a pillow in this study regardless of the postures, which provided support to the neck and limited head movements. Previous studies have demonstrated that body support can significantly reduce muscle activity. For example, shoulder straps [6], chairs with armrests and back support [7], or other support devices [21] can reduce muscle load and perceived discomfort in the neck and shoulder regions.
It is worth noting that perceived discomfort was generally higher in the texting task compared to the watching video task in this study, although it did not pass the statistical tests. A potential reason is that texting is more complex than watching video task since participants must constantly search for letters on the keyboard and look and read the recently typed word [13]. Due to the high level of concentration required for accomplishing the texting task, the perceived discomfort was higher. It is supported by the fact that the blink frequency and blink duration of texting were significantly lower than watching video task. When confronted with a visually demanding task, the blink frequency decreases significantly [37]. However, as it was mentioned that moderate exercise could reduce muscle fatigue due to more slight head movements, the texting task has lower muscle activity in the UT than watching video.
Effect of duration
In this study, the perceived discomfort of measured body parts increased significantly over time. However, there were no significant differences in muscle activities of ECR and UT, as well as blink frequency and blink duration between measurement points, apart from the muscle activity of APB. The NRMS of APB increased and then decreased over time, and there was a higher muscle activity of APB at the 20-minute time point compared to other measured time points. Wang et al. [11] examined the effect of duration on muscle activity of APB during playing smartphone games continuously for 30 min and found the muscle fatigue of APB increased significantly over time, which is inconsistent with the findings of the present study. In their study, the EMG median frequency (MF) was used as an indicator of muscle fatigue, and the decrease in MF indicates muscle fatigue [16]. However, in this study, RMS was used as an indicator of muscle activity and did not always increase linearly with muscle fatigue [38]. Although the perceived discomfort of the hand increased significantly over time, the RMS of APB may decrease due to prolonged experimental tasks [39]. In addition, as it was mentioned that body support could reduce muscle activity, due to the participants’ arms and neck being supported by the bed, the changes in muscle activities of ECR and UT were insignificant over time. Previous studies have shown that sustained static postures have the potential to contribute to the development of neck, shoulder, forearm, or thumb disorders [40, 41]. The effects of prolonged smartphone use in bed on muscle activities should be further investigated.
Mover, although the perceived discomfort of eyes increased significantly over time, the blink frequency and blink duration were not significant between measured time points in this study. One potential reason is that a 30-minute experiment duration does not always result in visual fatigue. Yin et al. [42] investigated the changes in blink frequency and blink duration while watching a 120-min video on a laptop; the difference was found only in the last 30 minutes. In addition, variables other than task duration may also affect blink frequency, such as perceptual and cognitive demandingness of tasks [43, 44]. Another potential explanation is that the participants in this study freely adjusted the details of lying postures, and the participants usually placed the smartphone in a position where they looked comfortable. The gaze angle was adjusted to a suitable angle for using the smartphone, and the size of the visual object was similar to usual, which reduced the load on the ocular muscles [45, 46]. It has also been proposed that the viewing distance adopted by the participants may decrease over time [47, 48]. Participants might have adjusted the viewing distance dynamically during the experiment. Therefore, no significant differences were found in blink frequency and blink duration.
Implications and limitations
The current study provides several implications for using a smartphone on the bed. When using a smartphone on the bed, the side-lying posture should be avoided as much as possible, as it increases muscle fatigue in the hand and neck and visual fatigue. The prolonged non-movement should be avoided while using smartphones on the bed, and moderate exercise can reduce muscle fatigue. Moreover, when using smartphones during a static activity like watching videos, it is advisable to use devices such as a phone holder to support the phone and reduce the force exerted on the hands.
The present study had some limitations. First, this study primarily aims to investigate the effects of lying postures on muscle activities and visual fatigue while using a smartphone on the bed. To simulate the posture of using a smartphone more realistically, the details of the lying postures, such as arm height and eye angle, were freely adjusted by the participants according to their habits of using the smartphone in bed. That might affect part of the experimental results. In future research, more efforts should be made to investigate the effects of arm height and eye angle on muscle activities and visual fatigue. Secondly, this study did not record the changes in the viewing distance of the participants during the experiment. The viewing distance might influence the measurement of visual fatigue. The changing pattern of viewing distance while using a smartphone on the bed should also be explored in the future. Thirdly, this study investigated the muscle activities of APB, ECR, and UT, which are primary body parts involved in using smartphones in bed. However, some studies suggested that different lying positions may influence leg discomfort [31]. Moreover, muscle activity was measured only on the right side of the body and did not investigate the effect of smartphone use on left-sided muscle activity. Future research should include recording muscle activity of the leg and left side to understand better the relationship between using smartphones and muscle activity. Finally, the participants were young college students rather than individuals of various ages, which might limit the scope of this study. The effects of playing with a smartphone while lying in bed should be further explored among people of different ages.
Conclusion
This study examined the effects of lying postures and task types and duration on muscle activities, perceived discomfort, and visual fatigue while using a smartphone on the bed. The perceived discomfort of measured body parts increased significantly over time. The side-lying posture has higher muscle activities in ECR and UT due to increased force exerted on the arm. Moreover, the side-lying position may be more likely to cause eye discomfort. Compared to texting, the watching video task has higher muscle activity, resulting in more discomfort due to keeping a static posture for a long time. The lying or half-lying position is better while using a smartphone on the bed. When watching a video, it is advisable to use devices such as a phone holder to support the phone and reduce the force exerted on the hands. This study provides an understanding of the association between using a smartphone on the bed with different postures and fatigue, which can help prevent muscle and visual fatigue in smartphone use. The effects of activities that require more arm support, such as playing games and reading novels, on fatigue can be further explored in the future.
Ethics approval
The study protocol was approved by the Northeastern University Research Ethics Committee (approval number: NEU-EC-2020B003).
Informed consent
Written informed consent was obtained from all participants prior to enrollment in the study.
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
The authors thank the participants for their time and involvement in the experiment.
Funding
This work was supported by the National Natural Science Foundation of China (Grant nos. 72071035 and 71771045).