
Abstract
BACKGROUND:
Studies are available on physician burnout and job satisfaction (JS) in relation to the specific income structure of the country of residence. However, no studies exist that investigate burnout of immigrated physicians taking into account the income structure of their country of origin (IS-COO) as well as duration of immigration.
OBJECTIVE:
To determine the influence of IS-COO on JS, income satisfaction, and critical burnout thresholds in the domains of emotional exhaustion (EE), depersonalization (DP) and reduction in personal accomplishment (RPA) among urologists with a migrant background working at German hospitals.
METHODS:
A questionnaire (Survey-Monkey®/101-items) was conducted among urologists of German hospitals with a migrant background. The online questionnaire was open for study participation from 1 August to 31 October 2020. The study included all physicians with a migration background who were born in a country other than Germany and were currently employed in a German department of urology. Physician burnout (Maslach-Burnout-Inventory) and JS were assessed using validated instruments. The influence of IS-COO and different covariates on the designated endpoints was tested using multivariate-models.
RESULTS:
96 urologists with a median stay in Germany of 7 years participated and were stratified according to low (LIC/41.7%), middle (MIC/36.5%) and high (HIC/21.9%) income based on IS-COO. No significant influence of IS-COO on critical thresholds in each burnout domain could be found. Of urologists from LIC, MIC and HIC, 42%, 59% and 57%, respectively, showed rather or extreme JS (p = .446). There was also no significant difference between groups in income satisfaction (p = .838). However, in multivariate-models, duration of stay in Germany (≥7 vs. <7 years) had significant effects on DP (OR: 0.28, p = .038) and RPA (OR: 0.09, p = .014), but not on EE and JS.
CONCLUSION:
IS-COO has no impact on burnout and JS among urologists who immigrated to Germany. Similarly, income satisfaction in the country of residence is not influenced by IS-COO.
Keywords
Introduction
In German hospitals, part of the severe shortage of physicians is currently being compensated by recruitment of foreign doctors. The number of foreign doctors in Germany has increased from 16,818 in 2007 to 52,522 in 2019 [1]. Germany’s urology clinics are also benefiting from the increasing immigration in recent years. In this context, satisfaction with the job and the working environment is key to maintain long-term working capability. In order to create working conditions that promote job satisfaction among foreign urologists, it is essential to identify determinants of job satisfaction as well as groups possibly at risk for reduced job satisfaction. In various studies, higher job satisfaction was associated with lower physician burnout (PBO), a finding that is also evident in previous publications of our current study [2–5].
The term “burnout” was first described by Freudenberger in 1974 [6]. Maslach and Jackson defined burnout in 1981 as emotional exhaustion (EE), depersonalization (DP) and reduction in personal accomplishment (RPA) [7]. Burnout syndrome is associated with a variety of psychological and physical complaints. Burnout among physicians can also be connected with medical errors, reduced work efforts as well as work quality [8, 9]. The Maslach Burnout-Inventory (MBI) is considered a standard instrument for measuring burnout and is used in 90% of all burnout studies [10].
In 2020, Sabitova et al. published a meta-analysis on burnout and job satisfaction among physicians in both human medicine and dentistry in low- and middle-income countries [11]. This meta-analysis found a burnout rate of 32% and job satisfaction among 60% of physicians. Despite some limitations (e.g. high heterogeneity of included studies, limited consideration of studies on participants from countries with low income structure, lack of differentiation between studies among physicians from human medicine and dentistry), this meta-analysis provides a good picture of physician burnout (PBO) and job satisfaction in countries with middle income structure [11].
Other studies focused on differences in PBO between specialties, with urologists reported to have the highest burnout rates of up to 68.2% [12, 13]. In addition to the influence of medical specialty, younger age, female gender and longer working hours are described as significant factors influencing the development of PBO [14, 15]. Stress reduction, mindfulness exercises, discussion in small groups, focusing on hobbies and achieving physical fitness, but also structured continuing education and reading non-medical books were shown to be protective against PBO [3, 16–18]. A recent study pointed out that physicians with migration background working at German hospitals had higher burnout rates compared to native German colleagues (p≤.001) [19]. However, whether IS-COO has an effect on burnout rates and/or job satisfaction of physicians with a migration background working in Germany has not yet been investigated in the field of urology or any other medical specialty.
The survey “Assessment of their urological working environment by foreign clinicians in Germany” (EUTAKD) was conducted among urologists working in German clinics who were born in a country other than Germany and had obtained non-German citizenship there. Thus, the EUTAKD study deals with urologists who migrated to a high-income country (i.e. Germany). Within the framework of this study, a sub-analysis was carried out investigating PBO and job satisfaction according to IS-COO. Also, duration of stay in Germany as well as satisfaction with the income earned in Germany were taken into account. Since satisfaction with income correlates inversely with PBO, an analysis of burnout among doctors with a migration background taking into account the income structure of the country of origin (IS-COO) might shed light on the relationship between income and physician burnout [20, 21]. Thus, the rationale of the present analysis is to investigate the influence of IS-COO on PBO. Various studies have shown that income is a significant factor in emigration [22, 23]. This leads to the expectation and subsequent working hypothesis that among physicians who migrated to a high-income country, a lower IS-COO is associated with higher job satisfaction, higher satisfaction with income earned in the country of residence and lower rates of PBO.
Material and methods
Development and structure of the questionnaire
With the aim of conducting a study on the topic of “Assessment of their urological working environment by foreign clinicians in Germany” (EUTAKD is the German acronym of this study title), an interdisciplinary working group was constituted in January 2020. A survey comprising 101 items was developed based on the questions of a Saxon cross-sectional study, which was subsequently adapted and validated in 12 structured separate interviews with urologists (born in Germany and abroad) to verify the comprehensibility of the questions [2, 25]. The development, structuring and evaluation of the questionnaire was carried out in close consideration of the CHERRIES (Checklist for Reporting Results of Internet E-Surveys) guideline [26].
The EUTAKD questionnaire contains 12 items on the general characteristics of the participants (questions 1-10,39,40), 25 items on medical training and activity (questions 11-31,33-36), three items on immigration to Germany (questions 32,37,38), the complete MBI with a total of 22 items (questions 41.1-41.22) as well as 39 items on private and job satisfaction (42.1-42.39).
The MBI is a robust-validated instrument for quantifying PBO and contains three dimensions: A) emotional exhaustion (EE), B) depersonalization/loss of empathy (DP) and C) reduction in personal accomplishment (RPA) [4–11]. The sum score of the dimensions EE and DP correlates positively with PBO, while the sum score of the dimension RPA correlates negatively with PBO. The three burnout dimensions can be categorized into low, moderate and high risk of burnout: for EE 0–16, 17–26, and≥27, respectively; for DP: 0–6, 7–12, and≥13, respectively; and for RPA: ≥39, 32–38, and 0–31, respectively [4–10, 12–20]. The three burnout dimensions can also be dichotomized into high (critical) vs. low-moderate burnout risk. A high risk of burnout therefore exists at EE≥27, DP≥13 and/or RPA≤31 [4–10, 12–20]. A dual-combined end point was then still formed from the aggregated assessment of the risk constellations in the PBO dimensions EE and DP (EE≥27 and/or DP≥13).
Response options regarding satisfaction with private-life and job comprised a 5-point Likert scale (1-extremely dissatisfied, 2-rather dissatisfied, 3-partly dissatisfied/partly satisfied, 4-rather satisfied, 5-extremely satisfied).
Study implementation
The EUTAKD study was directed at all physicians currently working at a urology clinic in Germany who were born in a country other than Germany and had obtained non-German citizenship there (even if German citizenship had been applied for or obtained in the meantime). All physicians who did not meet these criteria were excluded from the study. An ethics vote has been given by the ethics committee of the University of Regensburg on 22.4.2020 (ZE: 20-1808-101).
The survey was conducted via Survey-Monkey® (SurveyMonkey Inc., San Monte, USA) from August 1, 2020 until October 31, 2020. To raise public awareness for the EUTAKD study, access to the Survey-Monkey® was advertised by means of a QR code in corresponding articles in the journals Uro-Forum and Uro-News (which are freely and widely available for every urologist in Germany), as well as by an information campaign via the Society of Urological Residents (GeSRU) [27]. Furthermore, all presidents of the regional urological societies were contacted twice and asked for their support by forwarding the study invitation to the various clinics of their regional society. Funding was provided by the Hans-Neuffer-Foundation.
Research question and statistical methods
The present analyses address the question of the extent to which IS-COO influences overall job satisfaction, satisfaction with the current income (received in Germany) and the risk of critical PBO during urological professional practice in Germany.
Endpoints of the study were the individual dimensions of burnout, i.e. EE, DP and RPA as well as the dual-combined endpoint of EE and DP, whereby a critical risk of PBO was defined as EE≥27 and/or DP≥13 [28]. In addition, overall job satisfaction and income satisfaction were further study endpoints. All endpoints were evaluated as sum-scores and dichotomized: satisfaction items were categorized as rather/extremely satisfied (Likert-scale 4-5) vs. partly satisfied/partly dissatisfied to extremely dissatisfied (Likert-scale 4-5 vs. 1-3). To evaluate the influence of time already spent in Germany by the study participants on the various endpoints, time was dichotomized in the median (≥7 vs. <7 years).
IS-COO based on income per capita reflecting the entire country population was classified into the three categories low-, middle- and high-income according to the World Bank criteria: Countries with an income of less than 1,045 USD/year are referred to as low-income countries (LIC) and those with a per capita income of more than 12,745 USD/year as high-income countries (HIC) [29]. The range of values in between (>1,045 to < 12,745 USD/year) represents the income per capita of a middle-income country (MIC).
All categorical group comparisons were performed exclusively with the Chi2 test, whereas the comparisons of the sum scores in the individual PBO categories were always performed with the Mann-Whitney test (moreover, it was always specified in the tables exactly which statistical tests were used in the individual group comparison).
Multivariate-logistic regression models (MLRM) were used to test the influence of the following criteria on the various binary study endpoints: (1) IS-COO (categorical), (2) time in Germany (dichotomized in median), (3) gender (male vs. female) and (4) satisfaction with income (dichotomized in rather/extremely satisfied vs. partly/partly to extremely dissatisfied). The influence of the independent variables on the defined endpoints is presented with odds ratio (OR) including the 95% -confidence interval.
Data analysis was performed with SPSS 26.0 (IBM Corp., Armonk, NY, USA). The p-values given are always two-sided, the significance level was considered statistically significant at p≤.05 for all tests.
Results
The composition of the study group in the individual evaluation criteria of this work is shown in the form of a flow chart as Fig. 1. The three most common countries of origin were Syria (34.4%; 33/96), Iraq (4.2%; 4/96) and Russia (4.2%; 4/96). Study participants were predominantly male (90%), of the age range 30–39 years (69%), married (72%) and working full time (94%) (Table 1). Of 96 urologists participating in the study, 81 completed the questionnaire and thus formed the evaluable study group. Of these, 34 (42.0%) were from low-income countries (LIC), 28 (34.6%) from middle-income countries (MIC) and 19 (23.5%) from high-income countries (HIC) (Table 1). The median time spent in Germany was 7 years (interquartile range: 5–11 years).
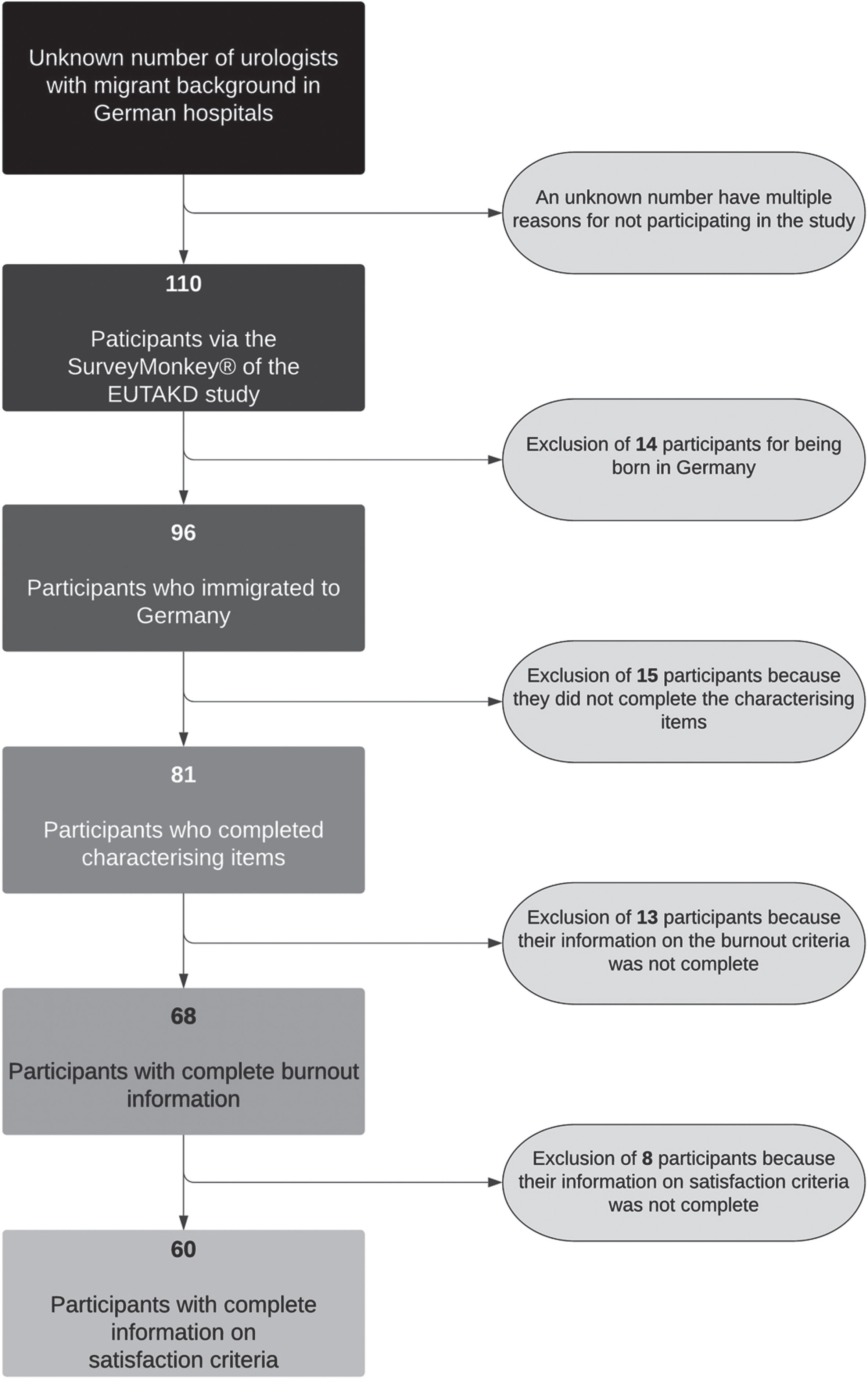
Flow chart of the composition of the study group in the individual evaluation criteria.
Participant characteristics according to median length of stay in Germany
Legend: Statistical comparisons were performed with the chi2 test, significance level was ≤.05.
52% of the study participants were satisfied with their overall job situation and 67% with their income. Low or moderate risks for PBO in the EE, DP and RPA categories were shown by 44% and 28%, 31% and 34%, and 3% and 24% of study participants, respectively. A high-risk category for PBO in the dimensions EE, DP and RPA was shown by 28%, 35% and 73%, respectively (dual-combined endpoint from EE/DP: 40%). There was no significant difference between participants from LICs, MICs and HICs in terms of job satisfaction (n = 60) and satisfaction with income. There was also no significant difference between participants from LICs, MICs and HICs on the burnout dimensions (n = 68) EE, DP and RPA (Table 2). The analysis of the endpoints PBO, job satisfaction and satisfaction with income (taking into account the length of stay in Germany) also showed no significant difference between participants from LICs, MICs and HICs (Table 2).
Burnout categories and satisfaction with work and income according to the income structure of the country of origin.
Note: Data are provided for the entire study group and according to the length of stay in Germany; p-values refer to comparisons between different income structures of the countries of origin. Legend: Statistical comparisons were performed with the chi2 test, significance level was ≤.05.
Based on multivariate analyses, IS-COO did not impact job satisfaction or dimensions of PBO (Table 3). However, a length of stay≥7 years was associated with a lower probability of a high risk of burnout in the dimensions DP and PRA (Table 3). Satisfaction with income, on the other hand, only had a significant inverse influence on the PBO dimension RPA.
Multivariate logistic regression models assessing the influence of four independent variables on different study endpoints
Legend: Multivariate logistic regression was performed to test the influence of independent predictors on five endpoints, significance level was ≤.05.
In binary analyses (high-risk category vs. other category), a significantly lower percentage of participants with a length of stay in Germany of≥7 years had a high PBO category in the dimensions DP and RPA compared to those study participants who had been in Germany for < 7 years (Table 4). These results were confirmed in the analyses of the absolute scores of the PBO dimensions (Table 4). When considering the combined endpoint of whether participants intend to leave Germany and/or urology (the so-called “loss score”), 41.3% (19/46) of participants who had been in Germany for≥7 years indicated their intention to leave urology and/or Germany as opposed to 60% (14/35) among those being in Germany for < 7 years (p = .119).
Presentation of endpoints for the entire study group and also according to łength of stay in Germany. In addition, mean scores were calculated for the three PBO dimensions
Note: The figures in brackets correspond to the 95% confidence interval. Legend: Comparisons of percentages were tested with the Chi2 test, comparisons of means were tested with the Mann-Whitney U test. The significance level was ≤.05. SG, study group.
Summary of findings
To the best of the authors’ knowledge, these results of the EUTAKD study are absolutely novel and add data to the international literature on migrant physicians: ad 1) IS-COO has no significant influence on job satisfaction or the probability of burnout after immigration to a high-income country (such as Germany), ad 2) the lack of influence of IS-COO on these two endpoints remains if the duration of stay in Germany is taken into account (in other words, both early and late after immigration to Germany, the subdivision according to income structure of the country of origin has no influence on job satisfaction and burnout probability), ad 3) except for the burnout dimension RPA (which it improves), satisfaction with income earned in Germany shows no significant influence on other endpoints (including overall job satisfaction), ad 4) the time already spent in Germany by the urological colleagues is significantly associated with a lower risk for burnout (in other words, the longer the colleagues with migration background live in Germany, the lower the probability of critical burnout), and ad 5) the achievement of a critical PBO category in the dimensions DP and RPA are lowered by the dichotomized “time in Germany” (the median was 7 years in our study) by 72% and 91%, respectively.
Rationale of the present study and possible explanations for its findings, as well as considerations for future research approaches
With a per capita income averaged over all occupational groups of 57,810 USD/year, Germany is one of the high-income countries [29]. In 2019, 52,522 foreign doctors were employed in Germany [1]. How many foreign physicians work specifically in urology is currently not recorded. Urology is one of the specialties with a higher risk of PBO compared to other specialties. Previous studies described burnout rates of 52% for urologists in Ireland and the United Kingdom and up to 64% for US urologists [4, 12]. In the present study, a combined endpoint of the burnout dimensions EE and DP revealed a burnout high-risk category in 40% of the participants. The fact that the proportion of participants with burnout is comparatively low can possibly be explained by methodological differences, and differences between the characteristics of the study populations. In addition, Dyrbye et al. did not use the complete MBI in the US study to survey PBO [13]. In various studies, an inverse relationship between job satisfaction and burnout was observed [2–5].
Interestingly, in the present study participants with a length of stay in Germany of at least 7 years had a significantly lower risk of burnout as compared to doctors with a shorter length of stay. Length of stay and burnout may be mutually dependent – those who are dissatisfied and suffer from burnout leave the host country more quickly (and vice versa). This assumption is also supported by the observation that a smaller proportion of those who have been in Germany for at least 7 years intends to leave Germany and/or urology (41.3% vs. 60.0%, p = .119). It is likely that a longer period of residence leads to people acquiring resources that can reduce the risk of burnout: such as familiarity with the German healthcare system, recognition of professional qualifications acquired abroad, improved language skills, adaptation to the culture in Germany and the development of social networks. However, the observation that even among colleagues with a long-term stay in Germany, more than 40% would like to leave either the host country and/or the urological specialty raises concerns for the functionality of urology clinics in Germany.
Contrary to the initial working hypothesis, in the present analysis IS-COO had neither a significant influence on job satisfaction nor on satisfaction with the current income. Thus, the initial hypotheses of our study could not be confirmed and subsequent hypotheses presupposing this connection had to be rejected. An association between IS-COO and PBO was also not proven. A significant impact of satisfaction with income on PBO could be shown in the dimension RPA, but not on EE and DP.
In a recent study among intensive care physicians in China, Wang et al. demonstrated that higher income satisfaction was an independent protective factor against severe burnout [30]. A possible explanation for the lack of correlation in our study could be that job satisfaction is possibly multifactorial. Other determinants than IS-COO could have a major influence on job satisfaction. This would be good news for the development and implementation of interventions to improve job satisfaction, since determinants of job satisfaction identified in the EUTAKD and previous studies, such as working hours, stress reduction, small group discussions, mindfulness exercises and structured technical training, can be influenced and modified by the employer and also by the employee [8–10]. A sense of calling and a feeling of being significant is also described as a protection against dissatisfaction [31].
Interestingly, a study of Polish doctors by Dubas-Jakóbczy et al. showed that one of the main reasons for the intention to emigrate is the higher income in the immigration country [22]. Bazoukis et al. came to almost identical conclusions based on a study of Greek doctors [23]. So while the prospect of a higher income in the immigration country may be a driver of emigration, IS-COO is not necessarily associated with job satisfaction in the immigration country. In this comparison, it should be taken into account that the groups of LICs, MICs and HICs studies may include countries that are not comparable to Poland and Greece. Furthermore, the specific reasons for emigration were not considered in the present analysis.
Nevertheless, in physician migration it certainly plays a role which expectations are actually fulfilled in the immigration country or which aspects actually prove to be relevant. A possible discrepancy between expectation and reality can possibly also have an influence on job satisfaction and burnout risk among doctors.
The relationship between (expected and actual) income and job satisfaction or burnout should be investigated in further studies with prospective study designs. At the very least, further studies should explicitly consider the reasons for migration and the extent to which expectations have been fulfilled. In addition, future studies should address intervention options that can help reduce the relatively high proportion of physician colleagues with a migration background who want to leave Germany and/or the urological specialty again.
Strengths and limitations
To the best of the authors’ knowledge, this study is the first to provide data on the influence of IS-COO on burnout and job satisfaction of migrant physicians. Thus, the present analysis functions as a pioneer study for the urological specialty and probably also beyond.
When interpreting the study results, some limitations of the EUTAKD study should be taken into account: 1.) The response rate cannot be specified, since the number of migrant urologists working in German hospitals is unknown. It is not possible to characterize foreign urologists in Germany who decided not to participate in the study or who were not reached by the extensive and high-profile recruitment measures (see Study Implementation in the Material and Methods section). Thus, statements on the representativeness of the study results cannot be made. 2.) Not all participants who started the survey completed it (Fig. 1). Thus, only 60 complete data sets were available for the 39 satisfaction items, which had a strict implication for the formation of the multivariate models (to avoid overfitting). 3.) Due to the cross-sectional design, no causal or predictive statements can be made. 4.) IS-COO does not necessarily reflect the individual earnings and asset situation of physicians in these countries. 5.) This analysis only considered income structure of the country of origin but not working conditions and employment rights in the country of origin.
Therefore, the EUTAKD study is considered a descriptive and hypothesis generating pilot study [2, 32]. More comprehensive studies on this topic can certainly build on these initial results. Subsequent studies may consider a case-control study: immigrants-nonimmigrants in order to elucidate the influence of migration on job satisfaction and burnout.
Conclusions
To the best of the authors’ knowledge, the EUTAKD study is the first to analyze the relationship of the income structure of the country of origin and burnout and job satisfaction among urologists who have immigrated to Germany. The results provided neither an association between the income structure of the country of origin and job satisfaction, nor satisfaction with income, nor burnout. However, a length of stay in Germany of≥7 years was associated with a lower risk of burnout. Medical colleagues with a background of migration are of great importance for the maintenance of patient care, and this applies in particular to the urological specialty. In order to ensure that these colleagues are available for medical care in Germany in the long term, further, preferably prospective studies should be conducted to identify the key determinants of job satisfaction among foreign doctors in Germany.
Ethical approval
The study was approved by the ethics committee of the University of Regensburg, Germany on 22.4.2020 (ZE: 20-1808-101).
Informed consent
This is an Internet-based study of physician colleagues. Prior to participation in this study, colleagues were informed about the study objectives, that participation in the study was voluntary and that answering the questions constituted informed consent. This methodological procedure was closely coordinated with the ethics committee of the University of Regensburg.
Conflict of interest
The authors have no conflict of interest to declare.
Footnotes
Acknowledgments
The authors would like to thank all medical colleagues with a migration background for participating in this extensive study and hope to contribute to the improvement of their professional integration in the medium term with the publication of the study results.
Funding
This work was supported by the Hans-Neuffer-Foundation.