
Abstract
BACKGROUND:
School servants are professionals involved with cleaning and feeding activities in schools. Exposed to conditions of physical and psychosocial overload at work, they may face situations of morbidity and functional restrictions.
OBJECTIVE:
To evaluate personal and work characteristics and work ability index (WAI) of school servants in Brazil and test the mediating effect of WAI in the duration of sickness absence.
METHODS:
163 Brazilian school servants participated in this cross-sectional study, that including the self-completion of a sociodemographic questionnaire, information about the Work Environment, the Protocol of Psychosocial Risks at Work’s Evaluation, and the Work Ability Index. Also was collected, in a secondary health database, information about sickness absence. A linear regression model was constructed to identify the predictors of the duration of absence, followed by the analysis of mediation with the Path Analysis method.
RESULTS:
The study found that the WAI partially mediates the relation of the personal characteristics and the work conditions with the duration of absence of the school servants. The predictors included the organizational aspects of work, mental exhaustion, physical damage, health self-evaluation, availability of personal protective equipment, and the need to assume inadequate postures at work. These predictors explained 33% of the duration of absence and 53% of the WAI of these workers.
CONCLUSION:
This study indicated that inadequate working conditions and low WAI impact in the sickness absence, increasing by 33% the length of time off work of school servants.
Introduction
The organization and the dynamics of work have been through transformations in recent years, with changes in the ways people work, in the profile of diseases of the worker, and on the prevalence of indicators such as indices of people on leave, with disabilities, and of returning to work [1, 2]. In Brazil, most work leaves are due to lesions, followed by musculoskeletal and mental diseases [3,4, 3,4]. Specific groups of workers with high physical and psychosocial demands at work are exposed to greater risk and vulnerability, with high rates of morbimortality, absenteeism from work activities, and disability retirement [5, 6].
This is the reality of the work of school servants, professionals responsible for cleaning, preparing meals for all students, disciplinary assistance in recreational moments and use of restrooms. In Brazil, school servants do not provide pedagogical and educational services. The Brazilian school servants typically perform work in manual labor (blue collar), and are perceived to be less educated, low-skilled, and of a lower social class. In their daily work, school servants are subjected to occupational segregation, social invisibility, gender inequality, precarious work conditions, and disease, especially due to musculoskeletal disorders [7,8, 7,8]. Investigations in workers who carry out activities that are similar to those of the school servants, describe inadequate work place, posture, overload, physical environment, equipment, and processes [9–11]. Brazilian and international publications related with school environment focus on the general staff of schools, especially teachers [12, 13]. Although it is necessary to intervene in the work conditions of the school servants, studies about these professionals are scarce, especially with regard to the work ability.
Our study is based on the multidimensional Work Ability House Model who been proposed to explain the work ability process. This model considers that the WA depends on the balance between individual resources, work-related factors, and the macrosocial environment [14,15, 14,15]. The model is expressed by a four-floor House and a roof inserted in an encircling environment [15]. The first floor represents the base that supports the building and concerns health status and functional capacity, including physical, mental, and social aspects. The second floor relates to professional competence (knowledge and skills, training and learning at work) and its continuous development used to meet the demands of working life. The third floor represents the internal aspects of the individual, manifested as values, attitudes, and motivation. The last floor represents factors related to work such as work conditions, demands and content, organization and communitarian environment, management and supervision: this is the “heaviest” floor in the building and can affect the other dimensions. The roof of this building is the WA, resulting from the interaction and balance between the previous dimensions [15].
Many studies have investigated factors related to the work ability in different professional categories [16–18], highlighting the sickness absence as associated to a low work ability [19,20, 19,20]. As an indicator of health at work, monitoring the duration of absence of workers generates indicators of the exposure to risks in the varied sectors of work, making it possible to monitor the prevalences and most common diseases, while predicting states of disability and reflecting investments on the health of the worker [21]. Sick leaves also represent a financial expenditure, associated to the loss of productivity, to the hiring and training of new professionals, expenses with benefits or welfare, and extra costs with health services [5].
There is evidence of associations between personal and work characteristics with work ability and with the duration of absence of the workers, but the processes involved in this interaction are not clear [20, 22]. Recently, the type of occupation was mentioned as an important moderator of work ability and its associated factors [23]. Furthermore, a longitudinal study that followed municipal workers for 15 years indicated specific determinants associated to different trajectories of absence [24]. There are few investigations about the effect of work ability as a mediator of the relation between personal characteristics of the worker, working conditions, and the duration of absence [14, 26]. The study by Kartika and Widhiandono [25] investigated the mediation effect of work ability on the relationship between job training and job performance; von Bonsdorff et al. [26] investigated the personal strategies and high-involvement work practices and the mediation effect of company work ability and company performance. A recent literature review investigated work ability and its affects in work attitudes, performance, and retirement [14]. As can be seen, these studies focus their analysis on workers characteristics or work characteristics, without interrelating them in the mediation between work ability and sick leave, especially in school servants. Identifying these characteristics can be the key for targeted interventions to reduce the expenses with diseases in this group of workers, in addition to promoting them with safer, healthier, and more functional work conditions.
Considering the above mentioned, the aims of this study were to analyze personal characteristics and work conditions of Brazilian school servants, and to verify whether the work ability of these professionals has a mediating effect between their personal characteristics such as work conditions, and their duration of absence.
Methods
Participants
The cross-sectional study carried out with public servants from the Education Secretariat of the city of Nova Lima, Minas Gerais (MG), Brazil.
The study included workers who were active school servants, above 18 years old, who had been working for at least three months in the public schools of the city. Active workers were those who were exercising their functions, who were not away from work and who were not retired. The criterion for inclusion of “minimum of three months” was chosen because with this time the participant would already have contact and experience with work activities in order to respond more reliably to the work evaluation instruments. All servants who, during data collection, were distance workers, carried out administrative functions, or were young apprentice (teenagers aged between 14 and 18) were excluded.
To calculate the sample, a significance level α=0.01; testing power (1-β)=0.95; large conventional effect (f2 = 0.35), and a maximum number of predictors = 15. Therefore, the sample size, for a regression model and for the analysis of the mediating variable, was n = 118, as calculated by the software G*Power 3.1. The population of active school servants in 2019 was 324. Due to protective measures adopted in schools against the coronavirus disease 2019 (COVID-19) pandemic, 193 servants continued working in-person in 2020. All the servants were invited to participate in the study and, from those, 163 school servants agreed to participate. This sample by convenience (163) totals 84.5% of active workers at the time of data collection.
This study was approved the Research Ethics Committee from the Federal University of Triângulo Mineiro on October 27, 2020 (CAAE: 36566420.0.0000.5154, opinion 4.364.500). The STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for reporting observational data was followed in this study [27]. To reduce potential information bias, the evaluator was previously trained in the application of the instruments and the participants were blinded to the objectives related to the analysis of the study data.
Instruments
The first stage took place from October to December 2020. All instruments were self-administered and participants answered the research instruments at their workplace. The data collection protocol was formed by a set of instruments: a sociodemographic, professional, life habit, and health information questionnaire specifically designed for this study; a set of questions about Work Environment; the Protocol of Psychosocial Risks at Work’s Evaluation (PPRWE); and the Work Ability Index (WAI).
The sociodemographic, professional, life habit, and health information questionnaire also included self-rated health. The question “How do you rate your health in the last 30 days?” was used and the response included options ranging from very bad to very good. Subsequently, the responses were dichotomized into positive perception and negative perception [28].
The block of Questions about the Work Environment was adapted from Barbosa et al. [29], including 15 items about three factors (factorial structure with KMO = 0.727; sphericity test Bartlett’s with p = 0.000; accumulated variance = 62.21): environmental conditions (6 items: α=0,81), physical demands (6 items; α=0,73), and personal protective equipment (PPE) (3 items; α=0,83). The items about PPE had two possible responses (yes/no); the score of the others was calculated using four-point Likert-type scales. For the environmental conditions, these varied from inadequate to adequate, while for the frequency of the physical demand, it varied from never to always.
The Protocol of Psychosocial Risks at Work’s Evaluation (PPRWE) is an instrument elaborated by Brazilian researches to map the psychosocial risks at work [30]. The PPRWE has been widely used in Brazil and in studies with workers from other countries with similar socio-economic conditions [30–32]. It includes 92 self-applicable items, distributed in 4 scales: Prescript Organization of Work Scale (POWS); Styles of Management Scale (SMS); Pathogenic Suffering at Work Scale (PSWS); and Psychosocial Damages at Work Scale (PDWS). Each PPRWE scale contains a block of questions about common issues. Thus, POWS has items on organizational aspects of the work context, including 10 items of the division of tasks (α=0,85) and 12 items of the social division of labor (α=0,90) [30]. The SMS points to the characteristic of management used by the organization, with 10 items for the individualist (α=0,85) and 11 items for the collectivist style (α=0,93) [30]. The PSWS includes questions about lack of recognition (11 items; α=0,92), meaninglessness at work (9 items; α=0,90), and mental burnout (8 items; α=0,91) [30]. Finally, the PDWS gathers questions about physical (9 items; α=0,93), psychological (7 items; α=0,94) and social (7 items; α=0,91) problems that workers assess as essentially caused by work [30]. Each scale was subjected to factorial analysis, using the PAF method with oblimim rotation. The literature indicated a satisfactory factorial structure with eigenvalues above 1.00 for all factors; items with a load greater than 0.30, KMO above 0.94, accumulated variance around 51.79 and correlations with values above 0.22 [30]. The score of the items in the PPRWE follows a Likert-type scale, varying from 1 (never) to 5 (always). The score of each scale is calculated with a simple arithmetic mean. Finally, the value of each score is classified as low, medium, or high psychosocial risk, with the exception of the SMS scale, which is classified as a little, moderate or predominant pattern in management styles [30].
The Work Ability Index (WAI) was used to measure the work ability. This is an instrument validated in Brazil with good psychometric properties, as Cronbach’s alpha α=0.72, construct validity p < 0.001 and criterion validity p < 0.001 [33]. The WAI evaluates the perception of the worker about their ability to perform their jobs in the present and in the future, considering the demands, their state of health and physical and mental abilities. The WAI has 7 items, who evaluate current work ability compared to lifetime best; work ability in relation to the mental and physical demands of the job; current number of illnesses diagnosed by the physician; estimated loss to work due to illness; absences from work due to illness in the last 12 months; and enjoyment of daily activities, feeling active, alert, and hopeful about the future [15]. The final score varies from 7 to 49 points and higher values indicate better work ability [15]. The index also can be divided in four classes: poor (7–27 points), moderate (28–36 points), good (37–43 points), and excellent (44–49 points) [15].
In the second stage, electronic data on sick leaves were collected from the Integrated Service for the Health Care of Servants (SIASS). This stage was the extraction of electronic data on sickness absence in the database of clinical and epidemiological surveillance at the SIASS. The objective of SIASS is to coordinate and integrate public servants’ health care actions and programs, official expertise, and the promotion and prevention of occupational health [34]. The data used in the study are already part of the routine of health services for public servants in Nova Lima. These data had the causes and the total duration of absence, per disease of each participant, from January 2017 to December 2020. The collection of absenteeism data was carried out up to the date of application of the questionnaires on participants. These data included the sum of all days of sick leaves certified by medical or odontological documents, with a maximum period of 15 days for each certificate. According to Brazilian labor laws [35], workers who are on leave since 15 days are sent for external expert evaluations. The link between the information in the questionnaires and the leave data was established by the full name of the participants. After this connection, the names of the participants were encoded in numbers to guarantee secrecy.
Data analysis
Data was entered in Microsoft Office Excel 2007 and analyzed using SPSS version 26.0 and R version 4.0.3. The duration of absence was considered to be the depending variable and the WAI was evaluated as a mediating variable of the relation between personal characteristics, work conditions, and duration of absence. The categoric variables were submitted to a descriptive analysis, with frequency and proportion measures. For the numerical variables, the median and quartiles were calculated, except for the PPRWE, which were analyzed using mean and standard deviation, according to application criteria of the instrument itself [30].
The means of WAI and duration of absence did not have a normal distribution, and, for the bivariate inferential analysis, Spearman’s correlation was used for numerical values; Mann-Whitney U test for categorical values with up to two independent groups; and Kruskal-Wallis, followed by Bonferroni, for the categorical co-variables with three or more independent groups. For the bivariate analysis, a significance level of α=0.20 was considered.
The multivariate analysis carried out using a “best subsets regression” (ols_step_best_subset), attempted to identify a model that worked better to explain the duration of absence, using the adjusted highest R2 value as a criteria for choice. As candidates for predictors of this model, we considered the co-variables that were simultaneously correlated with WAI and with the duration of absence in the bivariate analysis. The normality for the residues and the homoscedasticity of the model selected were estimated (ols_test_normality e ols_test_f), with a result of p > 0.05.
Analysis of the mediating effect
The mediation is observed when, in a relation between predictors (X) and response (Y), a third variable (Med) can intervene in the strength of this relation, entirely or partially reducing it [36]. The path analysis is the statistical method traditionally used to test the mediating effect [36, 37]. According to Fig. 1, for this effect to be proved in the regression equation, the relation must be significant in each stage of the path analysis: when estimating the relation between predictive variables and the outcome (step 1, path c), of the predictive variables with the mediator (step 2, path a), and of the mediator with the outcome (step 3, path b). Furthermore, when the mediator variable is inserted in the relation between predictive variables and outcome (step 4, path c’), it should be able to reduce or nullify the strength of this relation. If the coefficient estimated for Med is significantly different from zero, it shows an effect of total mediation, in which the entire magnitude of the relation of X with Y is nullified by the insertion of Med. However, in both cases of mediation, there is a reduction in the determination coefficient (R2) from the path c to the path c’. This study adopted a significance level of α=0.05. For each step of the path analysis, post hoc tests were performed in the G*power software, to check the power of each regression model considering the missing data, and maintaining the analysis only for a power greater than 80%.
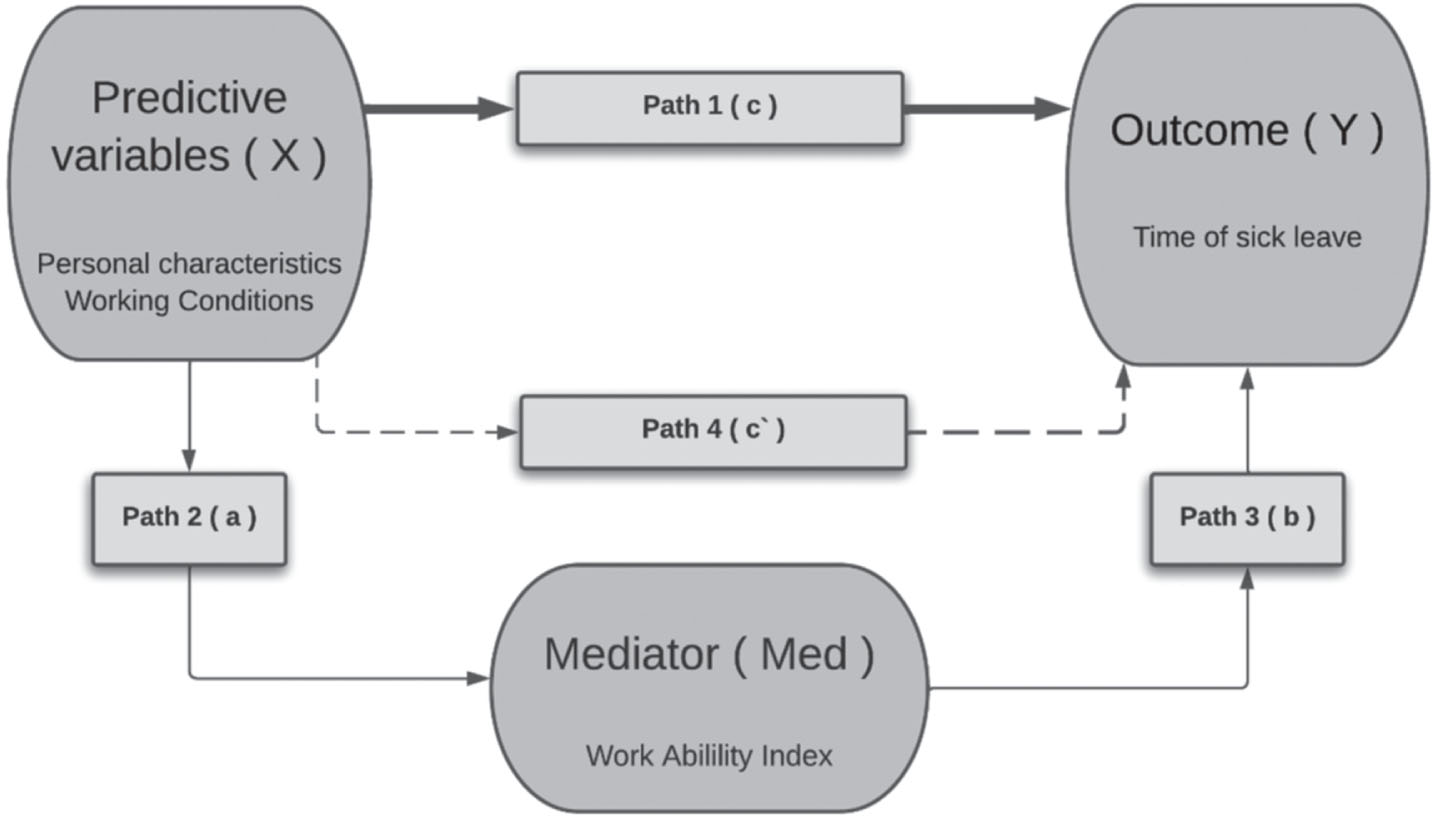
Analysis diagram of the path analysis to test the mediating effect.
A total of 163 school servants participated in the study. Table 1 shows information about the personal characteristics of participants, including sociodemographic, occupational, life habits and health data. The characterization of physical and psychosocial work conditions is described in Table 2.
Sociodemographic, occupational, life habit, and health characteristics (N = 163)
Sociodemographic, occupational, life habit, and health characteristics (N = 163)
1 Spearman’s correlation for numerical variables; Mann-Whitney U test for categorical values with up to two independent groups; Kruskal-Wallis, followed by Bonferroni, for the categorical variables with three or more independent groups; *p<0.20; 2DA and WAI were constant in the male sex; 3There was a difference only in the groups with 35 and 40 hours; 4 Other includes employees entitled to reduced working hours due to legal issues in the municipality, such as, for example, having children with disabilities; DA= duration of absence; WAI= work ability index; Q1= 1st quartile; Q3= 3rd quartile.
Physical and psychosocial conditions (N = 163)
1Spearman’s correlation for numerical variables; Mann-Whitney U test for categorical values with up to two independent groups; Kruskal-Wallis, followed by Bonferroni, for the categorical variables with three or more independent groups; *p < 0.20; 2DA and WAI were constant in the group never or rarely; DA = duration of absence; WAI = work ability index; SD = standard deviation; PPE = personal protective equipment.
The PRWE scales presented the following values: 3.34 (SD = 0.64) for POWS; 2.92 (SD = 0.38) for SMS; 2.13 (SD = 0.67) for the PSWS; and 2.39 (SD = 0.68) for the PDWS. These values indicate low risk for experiences of suffering related to work; moderate pattern in management styles, individualistic and collectivist; medium risk for harm at work, especially physical harm; and medium risk for work organization, with a weak point for division of tasks, number of workers, sufficient resources and flexibility in deadlines.
WAI had a median of 34 (Q1 = 30; Q3 = 38), a moderate WAI for the group, with scores varying from 19 to 47 (mean = 34.07; SD = 6.21). The total duration of absence due to sickness was 6.170 days, varying from 2 to 222 days per participant. The median duration of absence throughout the 4 years was 26 days (Q1 = 12; Q3 = 57), with a mean of 37.85 (SD = 36.54) days, per participant, during the 4 years. The three main cause for sick leaves were Musculoskeletal System and Connective Tissue Diseases (19.5% of the total sick leaves), followed by Factors that Influence the Health State and the Contact with Health Services (9.5%) and Respiratory Tract Diseases (9.5%). The order between these three main causes of sick leave was similar between 2017 and 2019, but in 2020, during the COVID-19 pandemic, the Factors that Influence Health State and the Contact with Health Services group represented the first cause and included, mainly, leaves for isolation due to contact with patients contaminated by COVID-19. Among the total of sick leaves, 23.7% did not indicate their cause. Tables 1 2 presented the results of the inferential bivariate analysis of the personal characteristics and work conditions with the WAI and the duration of absence.
The independent variables that showed a simultaneous significant association (p < 0.20) with WAI and duration of absence were: family income, health self-evaluation, Body Mass Index (BMI), PPE availability, assuming postures that can generate pain or discomfort, and the PPRWE scales “organization of work”, “pathogenic suffering”, and “damages at work”. These variables were submitted to multiple linear regression modeling to explain the duration of absence. However, the model found was not significant (p = 0.47). Through the testing of the algorithm “best subsets regression”, the new model included, grouped, six variables predictive of the duration of absence: POWS, PSWS, PDWS, health self-evaluation, availability of PPEs, and assuming postures that can generate pain or discomfort at work.
Figure 2 shows the results of the analysis of the mediating factor (path analysis). The regression model that describes the relation between the predictor variables and the duration of absence (path c, step 1), explained 33% of the duration of absence (R2 =0.3331; p < 0.05). The same set of predictor variables explained 53% (R2 =0.5301; p < 0.05) of the WAI (path a, step 2). Then a simple linear regression model was carried out between the mediator variable (WAI) and the outcome variable (duration of absence) (step 3, path b), indicating that the WAI explained 9% of the duration of absence (R2 =0.093; p < 0.05). In the fourth step (step 4a) of the path analysis (path c’), it was possible to verify that adding WAI to the set of predictor variables weakened the explanatory power for duration of absence. Comparing the adjusted R2, there was a reduction from 24% to 20%, which indicates partial mediation of WAI over duration of absence. To certify the hypothesis of partial mediation of work ability with regard to the duration of absence, the set of variables (POWS, PSWS, PDWS, self-evaluation of health, availability of PPE, assuming postures that can generate pain or discomfort, and WAI) was treated using the algorithm stepwise forward (step 4b). This analysis indicated that the estimated coefficient of WAI, together with the variables availability of PPE and assuming postures that can generate pain or discomfort at work is significantly different from zero (p < 0.01), explaining nearly 18% of the duration of absence (R2 =0.177; p < 0.01).
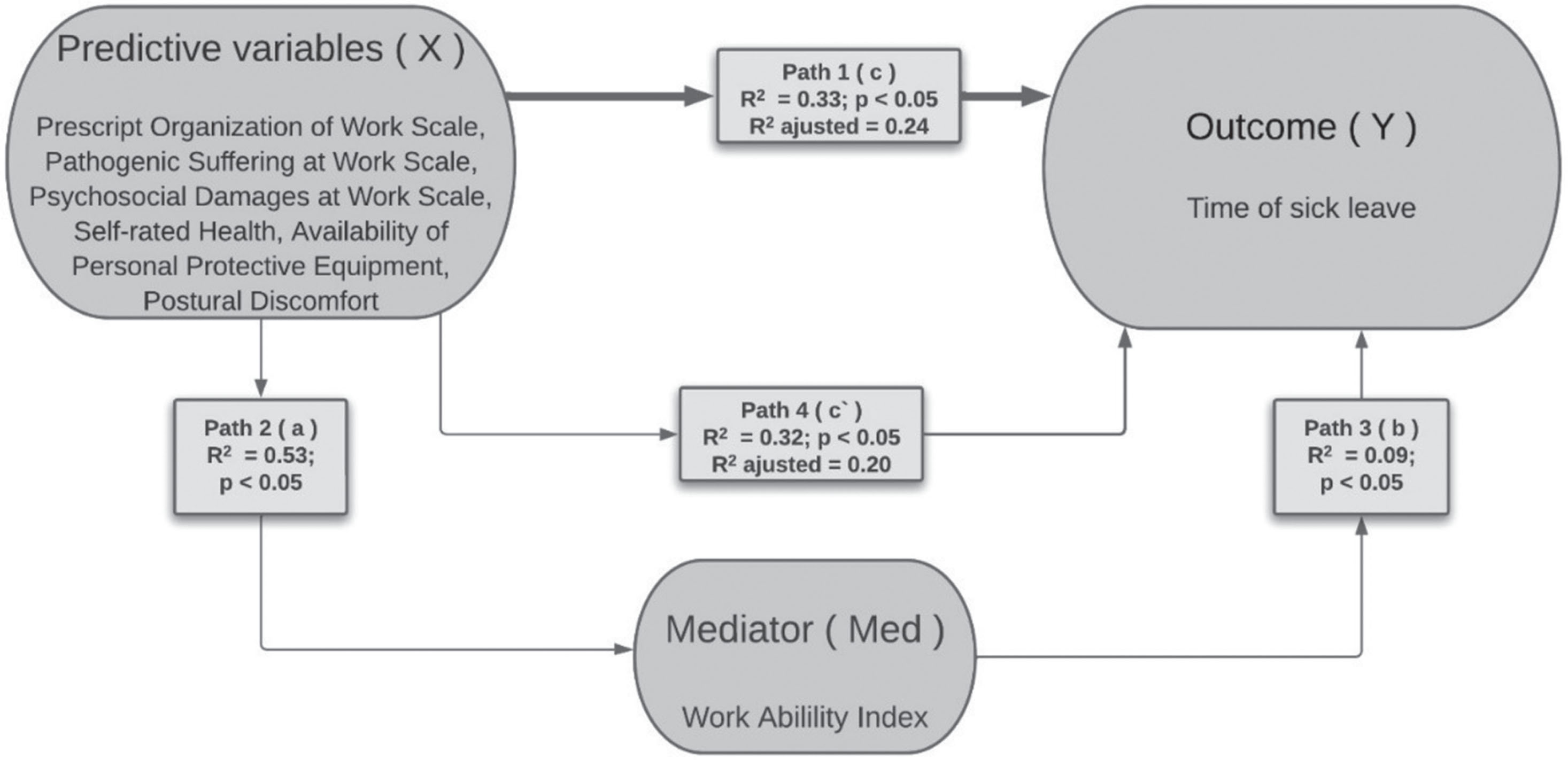
Model of the mediating effect of work ability in the relation between personal and work variables with the duration of sickness absence from work.
Table 3 shows the steps of the mediating analysis with all standardized coefficients and significance levels. It should be noted that, when WAI is input (step 4a) into the initial model, formed by the set of independent and predictor variables for the duration of absence, there is a reduction in the size of the effect (adjusted R2), provoked by the variables of the model. Consequently, there is a diminution in the significance level of each predictor variable (increased p value), proving that the presence of WAI can weaken this relation.
Standardized coefficients and their significance level (in parenthesis) in the steps of the path analysis
*p < 0.05; IV = independent variable; DV = dependent variable; DA = duration of absence; WAI = work ability index; PPE = personal protective equipment.
Occupational health indicators, such as the WAI and absenteeism due to illness, are associated with individual and contextual factors of school staff. The results of the proposed mediation model showed that personal characteristics associated with worse self-rated health and precarious working conditions can reduce work ability and predict absences from work. Specifically, precarious working conditions were the adoption of uncomfortable postures, unavailability of safety equipment, work organization flaws, mental exhaustion and the occurrence of physical harm. The mediation of the WAI suggests that the proposed methodological course represents an advance in understanding the predictors of sick leave among school servants, especially when working conditions are analyzed.
The demographic and occupational characterization in the results of this study were similar to those found by workers in the fields of cooking, cleaning, and education [7, 39]. Most workers were middle-aged women with low incomes, who had children and lived with a partner. These characteristics are historically and culturally associated with the disqualification of the work of females and to domestic overload, with the insertion of women in less valued economic activities, with lower pay or in poorer conditions [7, 40]. In the field of education, this phenomenon is clear [7, 40]. As opposed to other researches [11, 39], the school servants evaluated had a higher educational level. This could be associated to financial incentives towards the career progression of Brazilian public workers.
Their life habits corroborate national findings from researches on the health of the Brazilian population, with a high percentage of sedentary lifestyles, overweight, and obesity [41]. The BMI values were associated with the WAI and the absenteeism. These results are in accordance with findings about the relation between lifestyle and absenteeism at work, especially related to musculoskeletal causes in women [42]. Interventions aimed at promoting healthy lifestyle habits in school staff are described in the literature [12], mainly strategies focused on improving nutritional knowledge and reducing sedentary lifestyle [43]. However, the current literature focuses primarily on assessment of teachers and have included a small number of schools and staff [12]. In this sense, the promotion of healthy habits becomes necessary and should be structured as a strategy in occupational health programs aimed at all education workers, including school servants.
Regarding work conditions, a recent systematic review indicated that physical factors, such as physical environment, burden and psychosocial factors, like decision making and social support, are important mediators of socioeconomic inequalities in the health of workers [6]. In our study, the physical characteristics of the work of school servants were classified as poor, confirming the association between work conditions and risks for occupational diseases. Furthermore, the participants showed a medium psychosocial risk in dimensions of the organization at work, such as number of workers and resources and flexible deadlines. A recent systematic review and meta-analysis found that persistent precarious employment to be associated with poorer health for a number of outcomes [44]. Our results show that structural and organizational interventions at work aiming the reduction of psychosocial risks and promoting ergonomic improvements can be important actions to restore work ability and avoid absenteeism among school servants. These interventions should focus on minimize physical demands, such as inappropriate postures; adequacy in the number of workers and distribution of tasks; and greater offer of PPE’s. These proposals are expected to avoid, mainly, physical harm, mental exhaustion and sick leave among school servants.
Musculoskeletal disorders were the main cause for sick leaves in school servants. This is similar to the prevalence of diseases in workers with similar activities [5, 45]. Groups with more vulnerability at work tend to present a higher prevalence of these disorders, be it due to individual characteristics or to a greater exposure to excessive physical and psychosocial burdens at work [5, 47]. Similarly, the evaluation of the psychosocial factors indicated the presence of physical damage and mental exhaustion in workers and the evaluation of the physical conditions at work showed that most participants (83.3%) show pain or muscle discomfort. Accordingly, an ergonomic study carried out in a unit for school nutrition indicated that the work activities demand moderate effort, with discomfort and pain in the legs [48].
The mean duration of absence of the school servants was higher than that of public municipal servers from the West of Brazil [49], while lower than the duration of absence in the South [50] and then the mean national data [47]. The WAI is a widely used measure in services of health and occupational safety, since it is related to higher risks for future prolonged, frequent, or permanent absenteeism [19, 51]. In this study, the mean WAI of the group was moderate, explaining 9% of the duration of absence of the servants.
There is extensive scientific literature about the need to preserve the WAI of individuals, aiming to guarantee a better functionality of workers, with wellbeing and productivity [23]. An important finding of this research was the fact it understands which characteristics are related with the WAI and with the duration of absences due to disease. The model constructed to predict the duration of absence of the servants included a combination of aspects of work organization, mental exhaustion, physical damage, health self-evaluation, availability of PPE, and postures that can generate pain or discomfort. This result shows that the main contribution to the absenteeism of school servants is due to their working conditions. In agreement with these findings, a study with health professionals showed a greater association of sick leaves with psychosocial factors at work than with personal aspects [22]. Another research with university workers found that the duration of absence is predicted better by a combination of work and personal factors [52].
Since studies about mediation are scarce in this field, the advantage of this research was finding that the WAI has a partial mediating effect on the relation between personal characteristics and work conditions of school servants with the measures of duration of absence due to disease. The planning of actions that seek more balance between work demands and individual factors is needed to promote WAI and potentially reduce sick leaves in school servants. Directive interventions in health and work safety, aimed at minimizing physical damage and mental exhaustion, especially related with work organization, PPE availability, and minimization of situations that provoke pain or discomfort at work, are a potential strategy.
Limitations of this study include its cross-sectional design, which limits causal inferences; the memory bias associated with the use of self-reported measures; and the effect of the healthy worker. Two reasons for this were the maximum duration of each absence period being limited to 15 days in the database on absenteeism, and the fact that the research was carried out during a pandemic, moment in which many school servants with comorbidities were not present for in-person activities. The count of days off work in 2020 also considered the days of preventive isolation related to contact with people contaminated by COVID-19, not representing an illness of the worker. Despite this limitation, this research evaluated 84.5% of the total population of school servants in the municipality, active at work. The sample size of 163 school servants can be considered small when compared to other occupational groups, however, this sample size is high when analyzing the total percentage of the studied population. This fact is even more relevant when considering the precarious working conditions, the invisibility of this worker in society and the scarcity of studies with school servants, an important group of workers who support educational services.
This study gains relevant as it analyzes the mediating effect of WAI on working conditions and the sick leaves in an occupational group that has seldom been addressed by national and international literature. The sample power of the study was above 80% and the robustness of the statistical method used can be attributed both to the use of the best subset found using the regression algorithm and its submission to the recognized path analysis method [36, 37]. This analysis made it possible, thus, to evaluate complex constructs, such as the work ability, and test their association with the duration of absence and predictor variables. Although this study considers the influence of the macrosocial context on work ability and on the duration of absence of school servants, aspects such as the family and sociocultural context, work and welfare legislation were not addressed, and should be explored further in later studies.
Conclusion
The results indicated that the negative health perception, combined with poor work conditions, such as organizational problems, unavailability of PPE, the need to assume postures that generate pain or discomfort, mental exhaustion, and physical damage, responded for 33% of the duration of absence of the school servants analyzed. The WAI was identified as a partial mediating variable in this relation, capable of reducing in 4% the strength of the association between personal characteristics and work conditions with the time on sick leaves.
Sick leave due to illness at work reflects the working and health conditions of the population and brings social and financial losses arising from the loss of productivity, lack of provision of public services and additional overloads on the work team. In a practical way, the proposed model indicates the need to reduce the exposure of school servants to physical and psychosocial risks at work. Thus, we suggest ergonomic adaptations to minimize physical demands, such as inappropriate postures; adequacy in the number of workers, in the distribution of tasks and greater offer of PPE’s. Furthermore, it is suggested the adoption of health promotion programs that focus on disease prevention, especially musculoskeletal disorders and mental exhaustion.
These findings highlight the importance of developing actions to promote WAI and lead to better work conditions. These actions aim to reduce absenteeism and the economic, functional, and social impact of work leaves to workers, organizations, and governments.
Ethics statement
The study was approved by the Research Ethics Committee of the Federal University of Triângulo Mineiro on 27 October 2020 (CAAE: 36566420.0.0000.5154, opinion 4.364.500). The procedures followed were in accordance with the ethical standards of institutional and national bodies and consistent with the revised Declaration of Helsinki. Participants were informed about the goals of the research, the study’s risks and benefits, that their participation was voluntary, and that their identity would not be disclosed. Those who accepted to participate signed the Free and Informed Consent Form. The authors confirm that confidentiality and data security was appropriately handled.
Conflicts of Interest
The authors declare that there are no conflicts of interest. The authors are the sole responsible parties for the content and writing of the article.
Footnotes
Acknowledgments
The authors would like to thank all school servants from Nova Lima, Brazil, who contributed to this study.
Funding
The authors report no funding.