
Abstract
BACKGROUND:
Cell phone usage is highly prevalent among young adults. They are used for multiple purposes including communication, studies, social networking and entertainment. However, its excessive usage has been associated with adverse health outcomes.
OBJECTIVE:
The objective was to find the association of cell phone usage with musculoskeletal discomfort (MSD) and its associated factors.
METHODS:
A cross-sectional study was conducted on young adult students from a low-middle income country over a period of 3 months from December 2018 to February 2019. A structured questionnaire based on the Disabilities of the Arm, Shoulder and Hand (QuickDASH scoring) was used to record the musculoskeletal discomfort.
RESULTS:
Out of 803 questionnaires, data of 754 (94%) were entered and the remaining questionnaires (n = 49) were discarded due to incomplete answers. The mean age was 20.83 (1.62) years. In our study, there were 194 (25.7%) males and 560 (74.3%) female participants. Neck and shoulder were the most frequently affected regions. A significant difference in QuickDASH score was observed between genders (p-value p ≤ 0.001). Left-handed individuals scored significantly higher on QuickDASH score compared to right-handed individuals (p < 0.05). Increased musculoskeletal discomfort was reported by individuals with daily cell phone use of more than four hours (p < 0.05). A positive significant correlation was found between continuous one hour cell-phone use and higher mean QuickDASH scores (correlation coefficient 0.124, p value 0.001). Shorter eye-to-screen distance was significantly associated with MSD (p < 0.05).
CONCLUSION:
Musculoskeletal discomfort is associated with the female gender, duration of cell phone use and a small eye-to-screen distance.
Introduction
Cell phones have become an integral part of every individual’s life these days. The advent of touchscreen smartphones with abundant applications has influenced all factions of the society, and students are no exception. Cell phones are a source of satisfaction for students, be it for studying, communication or fun [1–3].
Evidence suggest that “text messaging” is the most frequently used method of communication among young adults [4, 5]. Mobile phones have found a promising role in the smarter study model amongst students, in addition to their use for communication or entertainment. The highly remarkable use of cellphones among medical students and doctors are not surprising owing to its utility to access online clinical evidence such as Medline [6–8]. For a health professional a cell phone helps to access quick reference in the clinic, as an alarm clock, a real time city map, and a convenient way to make financial transactions. The use of cell phones is ubiquitous and is more than just a communication device. The majority of the world population owns a cell phone and two third has access to the internet [9]. According to the national telecommunications authority of Pakistan, tele-density in the country is exceeding 84% with 185 million cellular subscribers and a 37% growth in tele-density in the last 7 years [10].
Despite a contrary finding [11], there is a growing evidence about the detrimental effects of cell phone use on health [12–24]. The use of cell phones for prolonged periods increases the likelihood of musculoskeletal discomfort (MSD). Hence, it is plausible to depict a dose response relationship between addictive use of cell phones and adverse health outcomes. As most of the individuals keep their neck flexed while using cell phone, this sustained neck flexion can eventually result in chronic neck and shoulder pain. Similarly the lower back, elbow, and small joints in hand are also affected [14, 23]. Multiple risk factors have been proposed including repetitive hand movements, poor posture, and overuse of cell phones for texting, studying, or playing games. Each of these factors alone or in combination can result in injury to nerves, muscles, and tendons in fingers, hands, wrists, arms, neck, or shoulders; which may end up causing persistent damage if not paid heed to [15, 25].
A number of studies indicates that that musculoskeletal discomfort is associated with excessive cell phone use [16, 26–31]. Unsurprisingly, the most painful body regions among smartphone use were found to be the shoulder and neck [13, 32]. Association has also been established between text messaging and musculoskeletal pain in neck, shoulder and arm, and numbness and tingling in hands and fingers. It has also been found that text messaging is mostly associated with short term effects on the musculoskeletal system and to a lesser extent, long term effects [15].
Despite the use of cell phones worldwide, longitudinal and experimental studies on musculoskeletal discomfort and cell phone use are still scarce. Systematic reviews on this topic concluded that limited evidence exists due to inadequate literature, with few cross-sectional and no longitudinal studies [26, 33]. Evidence of musculoskeletal discomfort with cell phone use among medical students is still limited, and to the best of our knowledge, data on this matter is still lacking in Pakistan. Medical students represent the young adult population of any society and are at risk of cell phone associated musculoskeletal discomfort. Hence, any untoward association of cell phone use with their health may be considered as the prelude of chronic consequences. The above statement has important implications for the own health of future physicians and the patient care. Therefore, this study aimed to examine the relationship between the degree of cell phone use and musculoskeletal discomfort among young adults. Our secondary objective was to examine the trend of cell phone use, the different musculoskeletal problems, and the factors which are associated with cell phone use and musculoskeletal problems.
Methods
Study design
This cross-sectional study was conducted from December 2018 to February 2019 after approval from the Institutional Review Board was obtained (IRB-1147/DUHS/approval/2018).
Study population and sample size
The prevalence of musculoskeletal discomfort in a previously conducted study in Taiwanese Junior College was found to be 52% in the neck region, which was used as the anticipated frequency while calculating the sample size [17]. At 95% confidence interval, and a 4% margin of error, a sample size of 730 was calculated using openepi.com [34]. A 10% additional sample was drawn to account for sample attrition and a better representation of the targeted population [35]. The study population was young adults from a large national medical college in a low middle-income country.
Outcome measure
The mean QuickDASH score was considered as the outcome indicating the musculoskeletal discomfort of the study participants. The QuickDASH instrument measures disability and symptoms related to pain and discomfort along with its severity in the arm, shoulders and hands graded as ‘None, Mild, Moderate, Severe, and Extreme’. In addition, a separate question regarding medical treatment required by the respondent was asked. Those who sought medical treatment were considered as having moderate to severe musculoskeletal discomfort.
Data collection procedure
A total of 803 questionnaires were distributed to students in each of the five professional years. Forty-nine questionnaires were discarded due to incomplete, or improper filling. Before administering the study questionnaire, the students were asked relevant simple questions and their documented medical history, relevant to our study objectives, were assessed. Participants with pre-existing musculoskeletal disorders, recent injuries to the neck, back or upper limb in the past six months were excluded from the study. Verbal screening was conducted at the time of introducing them about the survey and obtaining the consent to participate.
A structured self-administered questionnaire comprising 18 questions was designed for this study following an extensive literature review and evaluation by two medical professionals. It was adapted from a similar study conducted in Korea [21]. The Disabilities of the Arm, Shoulder, and Hand scoring (QuickDASH) questionnaire was also included in the study to evaluate the degree of musculoskeletal discomfort [36]. A pilot study including 20 participants was conducted to check for its clarity. The Cronbach’s alpha value for the QuickDASH scale was calculated to check the reliability of the questionnaire. The reported validity of QuickDASH in the literature is 90%.
All study participants received a description of study’s objective and procedure. Informed consent was obtained at the start of the survey and the participants were briefed in the classrooms about options to either fill in the questionnaire in a Google form or using pen-paper method. Both the forms were similar in structure, easy to answer and were prepared for the purpose of self-administration by the participants to ensure unbiased data collection. All data collectors were trained by the study authors for smooth distribution and collection of the forms and field editing in case of pen-paper based survey. Consecutive sampling was employed for data collection using the social media platforms for university students. Our final dataset comprised of complete 754 questionnaires without missing data and no imputation methods were required.
Data collection instrument
A structured self-administered questionnaire was divided into four sections. The first section included the sociodemographic details such as age in years, gender of the respondent, education level, and dominant hand of the participants. The next section inquired about cell phone usage; the time spent on it, the activities it is used for, eye-to-screen distance and the posture while using cell phone. The third section evaluated the symptoms of musculoskeletal discomfort and the regions affected by it. The severity of MSD was assessed primarily by the QuickDASH score itself. The higher the score the more intense the MSD. We also indirectly assessed the intensity of pain in the last seven days duration by recording the sleep disturbance level and medical treatment sought by the respondents. We also recorded the intensity of participants’ physical activities. Physical activity was labelled as light, moderate and heavy and were elaborated in the questionnaire as: Light (casual walk, cooking food, washing dishes, shopping, walking upstairs, sitting using computer, child care); Moderate (brisk walking, jogging, running, swimming, house cleaning, mowing lawn, playing golf); and Heavy (biking, hiking, jogging, running, swimming, jumping rope, playing basketball/football, lifting heavy objects). A detailed description of physical activity as per the CDC criteria were used [37]. The last section comprised of the QuickDASH questionnaire.
Statistical analyses
Data were entered and analyzed using the Statistical Package for Social Sciences v. 23.0 (IBM Corp., Armonk, NY, USA). Categorical variables were reported as frequencies and percentages, while continuous variables were presented as mean and standard deviation (SD). We compared the study outcome, mean QuickDASH scores, between genders using an independent sample student t-test. For independent variables, where there were more than two categories were present, we used a one-way ANOVA test for comparison of mean scores. Where applicable, the post-hoc Tukey test was used to identify significantly different categories. Based on questions 29–32, we regrouped and dichotomized the severity of pain and MSD, experienced during different activities, into mild and moderate to severe. The prevalence of MSD was compared with three categories that is, durations of cell phone use (light, up to 10 minutes; moderate, 10–30 minutes; and heavy, more than 30 minutes; in one sitting) using the chi square test. Finally, we used a generalized linear model to predict the factors associated with high mean QuickDASH scores. We used the GLIM or GLM, the generalized linear model which expands the general linear model so that the dependent variable is linearly related to the factors and covariates via a specified link function. Moreover, the model allows for the dependent variable to have a non-normal distribution, which is the QuickDASH scores, and to assess both factors and the covariates in the model. P values≤0.05 were considered significant in all comparisons.
Results
Out of 803 questionnaires distributed, the participants correctly filled 754 questionnaires, while the remaining were discarded due to incomplete responses, yielding a response rate of 94%. The following data analysis is based on completed questionnaires.
The majority of participants (511; 67.8%) had symptoms such as pain, numbness, tingling or fatigue in arms and shoulders. More than half of these (283; 55.4%) had bilateral symptoms, 158 (30.9%) had right side symptoms, while 70 (13.7%) had left side symptoms. Half (50.1%) of the 511 participants attributed their musculoskeletal symptoms to their cell phone use habits. A considerable proportion (91; 17.8%) of participants experienced intense symptoms that required medical treatment. Of the total, 107 (14.2%) had mild difficulty in sleeping due to pain while 36 (4.8%) had moderate to extreme pain disturbing their sleep in the last seven days duration. In a multiple response variable, among the 511 participants who reported MSD symptoms, 73.4% had pain in their neck and 65% in their shoulders. Other painful body sites were lower back (54.2%), legs and feet (44.7%), upper back (42.3%), hands/fingers (38.9%), wrists (29.7%), waist (23.3%) and elbows (16%). It can be seen that the neck and shoulders were the most commonly mentioned body regions with musculoskeletal discomfort in our study population.
The mean QuickDASH scores with respect to the socio-demographic and cell phone usage characteristics of the study participants are presented in Table 1. All study participants owned a personal cell phone. The overall age range of the study participants was 17 to 29 years with a mean age of 20.83 (1.62). The sample had 194 (25.7%) males and 560 (74.3%) female participants. Of the total sample, 68 (9%) of the students were left-handed. The study included 151 (20%) students from first year, 156 (20.7%) from second year, 150 (19.9%) from third year, 170 (22.5%) from fourth year, and 127 (16.8%) from the final year of medical school.
Sociodemographic and mobile phone use characteristics of young adults. QuickDASH scores, Mean (SD)
Sociodemographic and mobile phone use characteristics of young adults. QuickDASH scores, Mean (SD)
*No male participant.
Regarding the assessment of QuickDASH, the female participants when compared to males (p-value 0.001) as well as the left-handed participants in comparison to right-handed ones had a higher score (p-value<0.05). Though the prevalence of MSD was higher among the first year students and declines in the subsequent years but there was no statistically significant difference in the prevalence of MSD observed (p > 0.05). Similarly, no significant difference was found in the MSD in relation to the cell phone screen size or the number of years of smartphone use and the posture while using cell phones (p > 0.05; Table 1).
Table 2 presents the results of a one-way ANOVA depicting the relationship of various cell phone use behaviors with mean QuickDASH scores. This table shows that overall prolonged use of cell phones in any manner had a higher QuickDASH score.
Factors associated with high mean QuickDASH scores among healthy young adults (n = 754)
The prevalence of MSD among the light, moderate and heavy cell phone use in one sitting was significantly different (chi square value 54.43, df = 2, p < 0.0001). Figure 1 shows the prevalence trend of MSD, during various daily activities, due to prolong cell phone use in one sitting. Those using the cell phone for more than 30 minutes in our sample had twice the prevalence of MSD as compared to the 10 minute usage in one sitting.
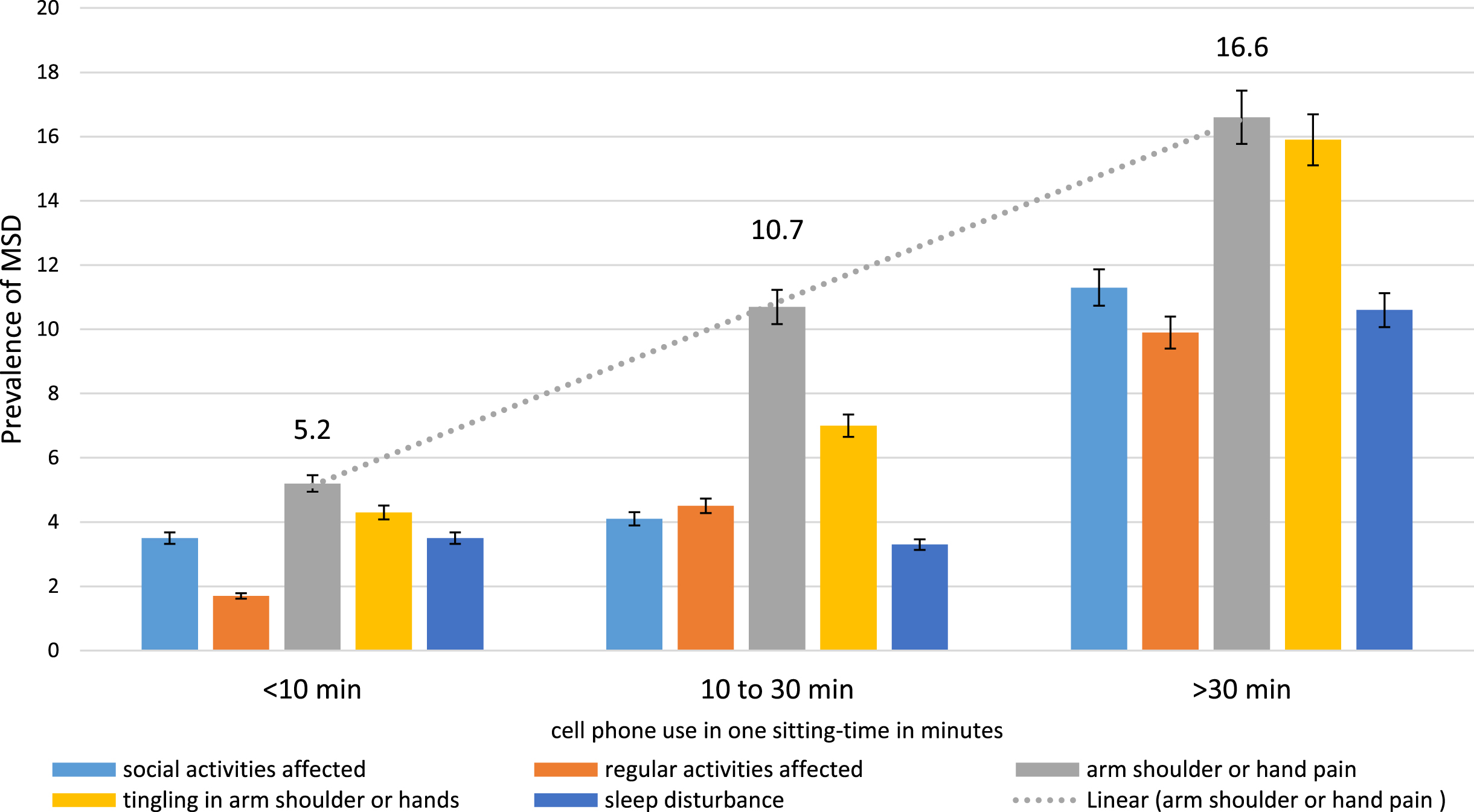
Prevalence trend of MSD in relation to cell phone use in one sitting.
The final GLM model (Table 3) shows that being a female participant (p < 0.001), keeping cell phone close to eyes (p = 0.042), and using cell phone for greater than one hour (p < 0.001) are associated with high mean QuickDASH scores.
Final model showing the positive association of gender, prolong use in single sitting and short eye to screen distance with high average QuickDASH scores in a multivariate model (n = 754)
The main objective of our study was to determine the association of cell phone usage with musculoskeletal discomfort (MSD) and its associated factors. A large number of study participants had musculoskeletal discomfort of at least one body part such as neck, shoulder, arm or hand. The study found that MSD was significantly higher among the participating females, those who use cell phone for prolong durations and who use cell phone at very close distance to their eyes. Similar to our results, Shan et al. also demonstrated in their study that MSD among students is greatly influenced by the use of digital devices [29]. These findings will help highlighting the poor ergonomic practices among young adults and the acute consequences in the form of MSD.
To the best of our knowledge, this is the first study with a large sample size on young adults using objective assessment of MSD from a low-middle income country. During the last decade, the use of touchscreen handheld devices has tremendously increased. The use of smartphones is become so pervasive that the users has started considering these devices as a basic requirement in their life.
We also found a positive association between MSD and the duration of cell phone use. The participants in our study who used cell phones for greater than four hours a day or more than one hour in one sitting had a higher mean QuickDASH score as compared to those who used their phones for less than 30 minutes in a day. Similar findings have been demonstrated by Al-Hadidi et al. showing a correlation between the duration of usage of digital devices and the degree of MSD [30].
In our study, the neck and shoulders were found to be the most common affected body regions. Of the participants with MSD, the majority mentioned head and neck regions as the most affected site. Most of the time these symptoms were reported bilaterally. Previously, Berolo et al. published similar results showing neck and shoulder to be the most prevalent sites for MSD among cell phone users [38]. Repetitive and sustained muscle load due to prolonged cell phone use and abnormal posture is a risk factor for developing MSD [39–41]. This might explain the highest prevalence of neck and shoulder pain, as muscles in these regions remain in prolong flexion during the cell phone use [41–46].
The participants who reportedly used cell phones at an eye-to-screen distance of less than 10 cm had a greater frequency of MSD as compared to those who used phones at a greater distance. This can be attributed to the fact that, similar to other near-work tasks, cell phone use also puts strain on the muscles of the hands, arms, shoulders, and neck [46–48].
Female gender was associated with higher MSD as depicted from the higher mean QuickDASH scores. However, no difference in mean QuickDASH scores was found among the participants who performed different intensities of physical activity. This could be due to the overall low prevalence of moderate to heavy physical activity among our study participants. Other studies have also reported a limited or no association of level physical activity with MSD [20, 29].
Our study also indicated that participants who use cell phones mostly for calling had the highest frequency of MSD compared to those who spent more time on cell phones for other purposes. Also, calls lasting one to two hours were associated with greater MSD compared to those ending before 30 minutes. A study done by Yang et al. showed a greater degree of upper back discomfort among individuals who spent more time using their cell phone for calling [17]. A clear trend of rising MSD was observed in relation to minutes of cell phone use in one sitting. Supporting findings have been previously reported in the literature [30].
We could not find any association of MSD with posture, LCD screen size, or length of time between consecutive cell phone usages. Our study had a few limitations; first, participants from a single medical college were included in this study. Second, the results are based on the last seven days history provided by our study participants which may be subject to the recall bias. The confounding effect of personal computers and laptops usage on MSD could not be ascertained in this study and may also be considered as a limitation. Future studies on MSD may improve upon by assessing the risk factors more objectively and consider including visual ergonomics assessment in their study objectives. More research focused on changing the poor ergonomic behaviors would be helpful to find suitable preventive strategies [49–51]. We recommend conducting experimental studies having innovative ideas with objective ascertainment of the risk factors and the outcome [52, 53].
Conclusion
We conclude that musculoskeletal discomfort among young adults is associated with the female gender, duration of cell phone use and a small eye-to-screen distance. Using the cell phone for more than 30 minutes in one sitting had twice the prevalence of MSD as compared to the 10 minutes use. It is recommended to conduct educative awareness programs highlighting the relationship of MSD to cell phone usage.
Ethical approval
Ethical approval was obtained from the Institutional Review Board of Dow University of Health Sciences (IRB-1147/DUHS/approval/2018).
Informed consent
Informed consent was obtained from all participants prior to enrollment. Data confidentiality and anonymity were strictly maintained.
Footnotes
Acknowledgments
The authors thank the participants for their time.
Conflict of interest
None to report.
Funding
None to report.