
Abstract
BACKGROUND:
The Motor Vehicle Accident (MVA) Fund Botswana compensates claimants who lose their incomes due to road traffic accidents. In Botswana, road traffic accidents are becoming more frequent, and the MVA Fund is experiencing escalating claims. We describe the demographic characteristics of loss of income (LOI) claimants of the MVA Fund Botswana. We assess whether demographic characteristics are related to return to work (RTW).
OBJECTIVE:
We retrospectively reviewed records of MVA Fund claimants and extracted demographic information. We investigated the demographic profile and the relationship between demographic information and RTW.
METHODS:
We reviewed 432 LOI claims received by MVA Fund from January 1, 2015 to December 31, 2020. We descriptively analysed the demographic profiles of claimants. We used a univariate analysis and multivariate logistic regression to determine the association between independent demographic variables and the dependent variable, RTW.
RESULTS:
MVA Fund claimants were on average 37-years-old. Claimants were mostly from low-income socio-economic backgrounds. RTW was significantly associated with injury severity, type of injury, and having a RTW plan offer. The final predictors of RTW, using logistic regression, were time away from work and severity of injury.
CONCLUSION:
In Botswana, claimants who had severe injuries and who stayed away from work for longer were less likely to RTW. The MVA Fund Botswana must recognise the demographic profiles of claimants which are likely to influence RTW.
Keywords
Introduction
Road traffic accidents (RTAs) are a leading cause of morbidity and death globally [1, 2]. The World Health Organisation (WHO) estimates that 1.35 million people died in RTAs in 2020, with over 93% of all road fatalities occurring in low-and middle-income countries, such as Botswana [1]. Botswana’s RTA fatality rate is 20.1, which is above the global rate of 17.4 per 100 000 people [3]. In addition to fatal accidents, 20 to 50 million more people suffer non-fatal injuries every year, with close to 800,000 people incurring a disability due to their injury [1]. The WHO attributes many severe injuries or disabilities to approximately 800 000 crashes globally, which results in many people not being able to work [4].
The African region reportedly has the highest RTA death rates, involving mostly people from low socio-economic settings [4]. Studies from many countries have shown increased and extensive economic losses due to RTAs [5–7]. Botswana is no exception, ranking among the countries with the highest incidence of RTAs worldwide [7], with RTAs being the second leading cause of death [8], affecting up to 3% of the economy [9]. In Botswana, the Motor Vehicle Accident (MVA) Fund has been mandated to compensate Botswana citizens who incur loss of income due to RTAs. The burden of RTAs leading to socio-economic challenges arising from disabilities and loss of employment is thus a concern for the MVA Fund Botswana. To limit costs and reduce the burden on taxpayers, the MVA Fund needs to advocate for return to work (RTW).
RTW facilitates re-integration of workers back into work following absence due to sickness or injury [10, 11]. Successful RTW has both societal and individual benefits [12, 13]. Individuals who RTW generally experience better health and emotional outcomes [13, 14]. RTW is more likely if motor vehicle accident fund claimants are younger than 45-years-old, highly educated, and strongly supported by their families [15, 16]. Often people in this group have better access to care and medical insurance [16, 17]. In contrast, Cancelliere, Donovan, Stochkendahl, Biscardi, Ammendolia, Myburgh and Cassidy [18] assert that RTW is less likely in people who are older, female, depressed, experienced higher pain, disability or activity limitations, higher physical work demands [19], or had previous sick leave and unemployment [16, 20–24]. People who receive disability benefits and or compensation may also be reticent to RTW [17]. There is a need for RTW stakeholders to explore the facilitators and barriers to swift RTW using evidence-based and equitable administrative processes [25].
The rehabilitation process may also influence RTW outcomes [18]. Rehabilitation should be multi-disciplinary, involving both the employer and claimant [26, 27]. Emphasis is put on collaborative, aggressive, and early intervention to facilitate RTW through a culturally and contextually relevant case management approach. Moreover, occupations facilitate processes for enabling empowerment and justice for people who are disempowered [12]. Occupational therapists aim to enable people to identify, choose, and engage in meaningful occupations for health and quality of life, in this case, work [10]. RTW affects individuals and society and therefore is often considered an important and final goal in rehabilitation. In Botswana, the MVA Fund coordinates RTW intervention for road accident victims amongst other roles [28]. Understanding the demographic characteristics of their claimants will help the MVA Fund to offer more client centred, holistic, and contextually relevant rehabilitation.
The MVA Fund Botswana continues to experience escalating healthcare costs due to increasing RTAs resulting in funeral, medical, loss of income (LOI), and loss of support claim payouts [8]. Medical, rehabilitation and LOI claims account for 75.6% of the MVA Fund’s expenses [29], which increased by 5.2% from BWP176.6 million in 2018 to BWP185.9 million in 2019. The MVA Fund is also affected by the escalating cost of private healthcare resulting in tariff increments across the MVA Fund’s service providers [30]. The escalating RTAs, rising medical inflation and negative financial performance challenge the sustainability of the MVA Fund [30]. The MVA Fund has to ensure RTW in the shortest possible time to impact positively on the claimant whilst reducing unnecessary costs and ensuring the future success of the MVA Fund.
Although the effects of RTAs have been extensively documented and acknowledged, little is known about the RTW experiences of people in low-and middle-income countries [26, 31]. The demographic factors that may contribute to delayed recovery and RTW, particularly in low-and middle-income countries such as Botswana have not been described. Most studies have been conducted in high income countries such as the United Kingdom, the United States of America, and Australia [2, 32]. In this paper, we established the demographic factors of MVA Fund’s LOI claimants in Botswana.
Methods
The MVA Fund Botswana
The case management department at the MVA Fund Botswana supports, compensates, and rehabilitates claimants injured in RTAs [28, 29]. Rehabilitation includes restoring claimants to their highest possible level of function, vocational rehabilitation, return to work advocacy, facilitating the process of RTW, and social rehabilitation of claimants [28, 29].
Compensation includes covering incurred past and projected medical expenses. These include assistive devices, incidental expenses, caretaker expenses, and enhancement of quality-of-life needs. The benefits are capped at BWP 1,000,000 ($86,744.26) for non-negligent road users and BWP 300,000.00 ($26,019.38) for negligent road users [33]. Claimants also receive the LOI benefit for either a temporary or permanent period depending on the severity of the injuries defined by the MVA Fund assessment guidelines. The LOI is payable upon assessment and capped at BWP6000 ($520.29) or the prevailing minimum wage rate for the period of incapacitation [33]. The claimants are also supported with a RTW program and advocacy.
Brink et al. consider the best research design to be the one that validates the research findings, fits the research purpose and is compatible with available resources [34]. We used Records Review Methodology (RRM) to determine the demographic profile of the MVA Fund LOI claimants and to establish the relationships between the demographic characteristics and RTW. The MVA Fund Information Technology systems being the System Analysis Program (SAP)-Enterprise Resource Planning (ERP) and Client Relationship Management (CRM) systems, stores all claim information. We included all successful LOI claims received from eight MVA Fund Botswana offices between January 1, 2015, to December 31, 2020.
Population
Loss of income claims are claims received from claimants of MVA Fund Botswana who were involved in RTAs with resultant injuries that prevented them from continuing to work, being employed or to make gainful employment. Therefore, successful beneficiaries of the LOI claim offered by MVA Fund Botswana as a result of losing the capacity to earn an income as a result of injuries sustained in an RTA depending on the nature and severity of the injuries are called LOI claimants. The successful LOI claims received from the 1st January 2015 until the 31st December 2020 were included.
We excluded LOI claims that were received between 1st January 2015 and 31st December 2020 but were rejected or repudiated, meaning the claimants did not benefit from the LOI benefit. We excluded claims for other benefits (medical, loss of support or funeral). The study used purposive sampling of LOI claims received by the Motor Vehicle Accident Fund Botswana during the data collection period. Total sampling was used with a total sample size of 534 claims of which 432 (81%) claims met the inclusion criteria and were included in the analysis.
Variables
Demographic variables
From each file, we recorded the claimant’s age, gender, injury, severity of injury, and date of the accident.
Injury variables
Injuries were classified using the ICD-10 codes. For this study, we were particularly interested in injuries of the nervous system (G); the eye and adnexa, ear and mastoid process (H); digestive system (K); musculoskeletal and connective tissue (M); injuries, poisoning, and other consequences caused by external factors (S, T); and factors influencing health status and contact with health services (Z).
Injuries were classified as minor (A), moderate (B), or severe (C). Minor injuries included lacerations and bruises not requiring admission and likely to recover in 4 weeks. Moderate injuries included single fractures requiring short-term admissions, conservative management surgeries, and likely to recover in 8–12 weeks. Severe injuries included multiple fractures, multiple injuries, amputees, spinal cord injuries, and traumatic brain injuries, requiring multiple surgeries, long term hospital stay and rehabilitation. These were likely to take longer than 8 months to recover.
Employment variables
We recorded the claimant’s occupation, time away from work, presence of an individual rehabilitation plan, and presence of a RTW program.
Occupations were categorised using the International Standard Classification of Occupations 2008 (ISCO-08) [35]. The ISCO08 provides a system for classifying and aggregating occupational information obtained by means of statistical census and surveys [35]. The ISCO08 classifies occupations in 10 groups as being: Class 0 (Armed Forces), Class 1 (Managers), Class 2 (Professionals), Class 3 (Technicians and Associate Professionals), Class 4 (Clerical Support Workers), Class 5 (Services and Sales Workers), Class 6 (Skilled Agricultural/Forestry/Fishery Workers), Class 7 (Craft Related Trade Workers), Class 8 (Plant and Machine Operators and Assemblers) and Class 9 (Elementary Occupations).
Time away from work was calculated using the incapacitation period as indicated in the sick leave and LOI offer status. RTW was defined as the last day of sick leave, with the employer confirming that the claimant RTW on a certain date as documented in case notes, work visits, or any claim documentation leading to graduation from the LOI benefit.
Presence of a RTW plan or an individual rehabilitation plan, or RTW engagement was confirmed if there was any evidence that the claimant participated in the rehabilitation process to prepare for RTW. This information was gathered from home visit reports, functional capacity evaluation (FCE) assessments, or SAP–Enterprise Resource Planning (ERP) system notes documenting any form of advocacy with the employer. Return to independence claimants is defined as claimants who were rehabilitated back into the job market but whose employment was terminated on grounds of the medical condition. With respect to this study, the definition of RTW involves certification of good health according to medical reports, being certified to resume work responsibilities, FCE confirmation of the ability to return to the job market, the termination of LOI based on successful return to employment, alternative employment or economic gainful activities.
Socio-economic variables
Socio-economic variables include the claimant’s income level, monthly earnings, LOI settlement amount, addendum offers, and graduation year.
The claimant’s income level was classified as low, medium, or high using the Botswana tax threshold of BWP 3000.00 as of December 31st 2020. Low-income (L) claimants earned less than BWP 3000. Medium income (M) claimants earned more than BWP 3000 but less than the MVA Fund’s monthly LOI cap of BWP 6000. High income (H) claimants earned more than BWP 6000. Monthly earnings were extracted from pay slips, or any supporting documentation indicating how much the claimant earned per month. An addendum offer is an extension of the initial LOI offer as supported by sick leave, FCE, or medical reports.
Data collection and organisation
Claims data were extracted from the SAP–ERP system and from the claim documents, including medical forms, pay slips, affidavits confirming income generation activities, employer supporting documentation, sick leave, FCE reports, individual tax returns, bank statements, medical reports, and other supporting LOI claim documents which indicates the person was generating an income. The first author and two research assistants, who were case management officers trained to use ICD 10 codes, ensured consistency and integrity of the data collected through a quality assurance process. Two additional case managers, who did not collect data, also checked the extracted data to enhance accuracy.
Although this phase of the study did not include experiments on human subjects; the data collection was done in accordance with the ethical standards of the Committee on Human Experimentation of the institution in which the experiments were done or in accord with the Declaration of Helsinki of 1964 and its later amendments or comparable ethical standards. Informed consent for the use of data was obtained from the Motor Vehicle Accident Fund Botswana, Chief Executive Officer whilst researchers ensured that all identifying information on the claim records or data, including patients’ names, initials, or hospital numbers, will not be published in written descriptions or any part of the publication. Furthermore, the study was approved by the Ministry of Health Botswana –Health Research and Development Unit Reference (No. HPRD: 6/14/1) and a study permit was granted in February 2021. The study was also approved by the Research Ethics Committee of the University of Pretoria’s Faculty of Health Sciences (255/2021) in May 2021.
Data analysis
The extracted data were imported into IBM Statistical Package for the Social Sciences (SPSS) version 27, 2020 [36]. Data were descriptively analysed using frequency tables for categorical variables, means, medians, and standard deviations for continuous variables. We conducted a univariate analysis to determine if Status (RTW and No RTW) was associated with any demographic variables. The null hypothesis tested is stated as follows: H0: There is no association between Status and demographic variables. Alternative hypothesis H1: There is an association between Status and demographic variables.
If the computed p-value is < 0.05, we reject the null hypothesis, else if the p-value is > 0.05 we fail to reject the null hypothesis i.e. the status (RTW and NRTW) is independent of demographics variables.
We tested for associations using the following tests: Pearson’s chi-square test, Fisher’s exact, and Fisher-Freeman-Halton exact tests. The Fisher exact test is used when there are fewer than five counts per cell and there are two rows and columns. The Fisher-Freeman-Halton test was used when there were more than two rows and columns.
The earnings data was continuous data and was not normally distributed. We used the non-parametric test Mann-Whitney U test to test if Status (RTW/NRTW) varied by earnings. Using the results from the univariate analysis, we then used multivariate logistic regression using backward elimination to determine the predictors of RTW.
Results
Demographic characteristics
We included 432 LOI claims, of these 245 (57%) were male claimants who were on average 37-years-old. Most of the claimants were younger than 40-years-old (64%) and 67% of these were male claimants (n = 166) as depicted in Table 1 and Table 2.
Descriptive data of the bio-demographics of LOI claimants
Descriptive data of the bio-demographics of LOI claimants
Descriptive data for the gender and age groups of LOI claimants
In this study, 58.8% (n = 254) of the LOI claimants sustained severe injuries followed by moderate (37.3% [n = 161]) and minor (3.9% [n = 17]) injuries. The most prevalent injuries were fractures involving multiple parts of the body (47.7% [n = 206]). These were followed by injuries to the head, face, and upper body (39.8% [n = 172]) as per Table 3 and Figure 1.
Descriptive data for injuries and occupational classes of LOI claimants
Descriptive data for injuries and occupational classes of LOI claimants
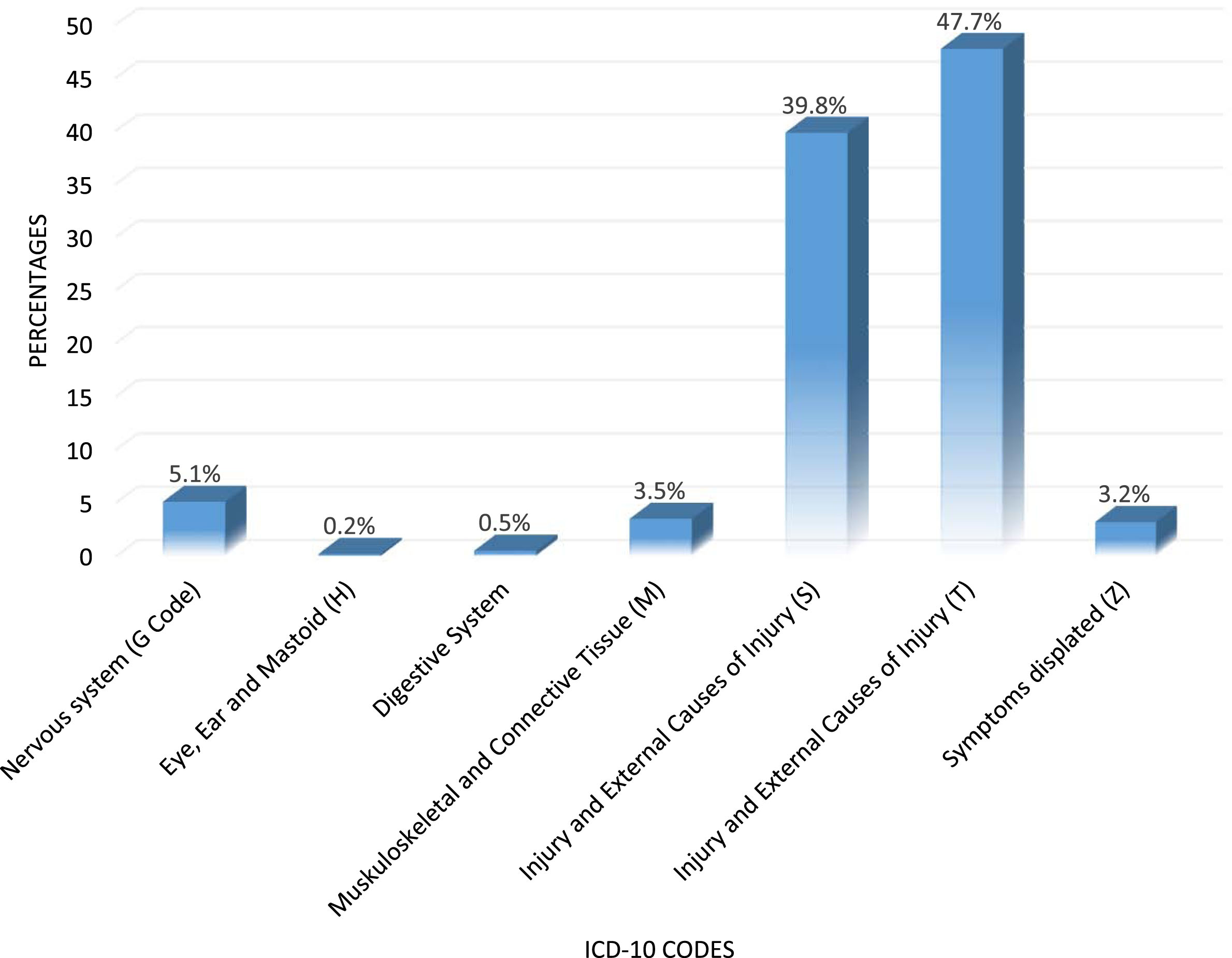
International classification of diseases 10th revision classification of injuries of LOI claimants of the Motor Vehicle Accident Fund Botswana, January 1, 2015 to December 31, 2020.
Most of the LOI claimants were Class 9 (Elementary) occupations) (32.9% [n = 142]), followed by Class 5 (Services and salespersons) (27.5% [n = 119]). Class 9 occupations include labourers, cleaners, freight handlers and kitchen assistants whilst Class 5 include housekeeping, preparing and serving food and beverages, caring for children, providing personal and basic healthcare at homes, hair dressing, beauty treatments, security services, selling goods retail, stalls at markets, or supervision of other workers. The fewest claimants were Class 1 (Professionals) as per the distribution on Table 3 and Figures 2 3.
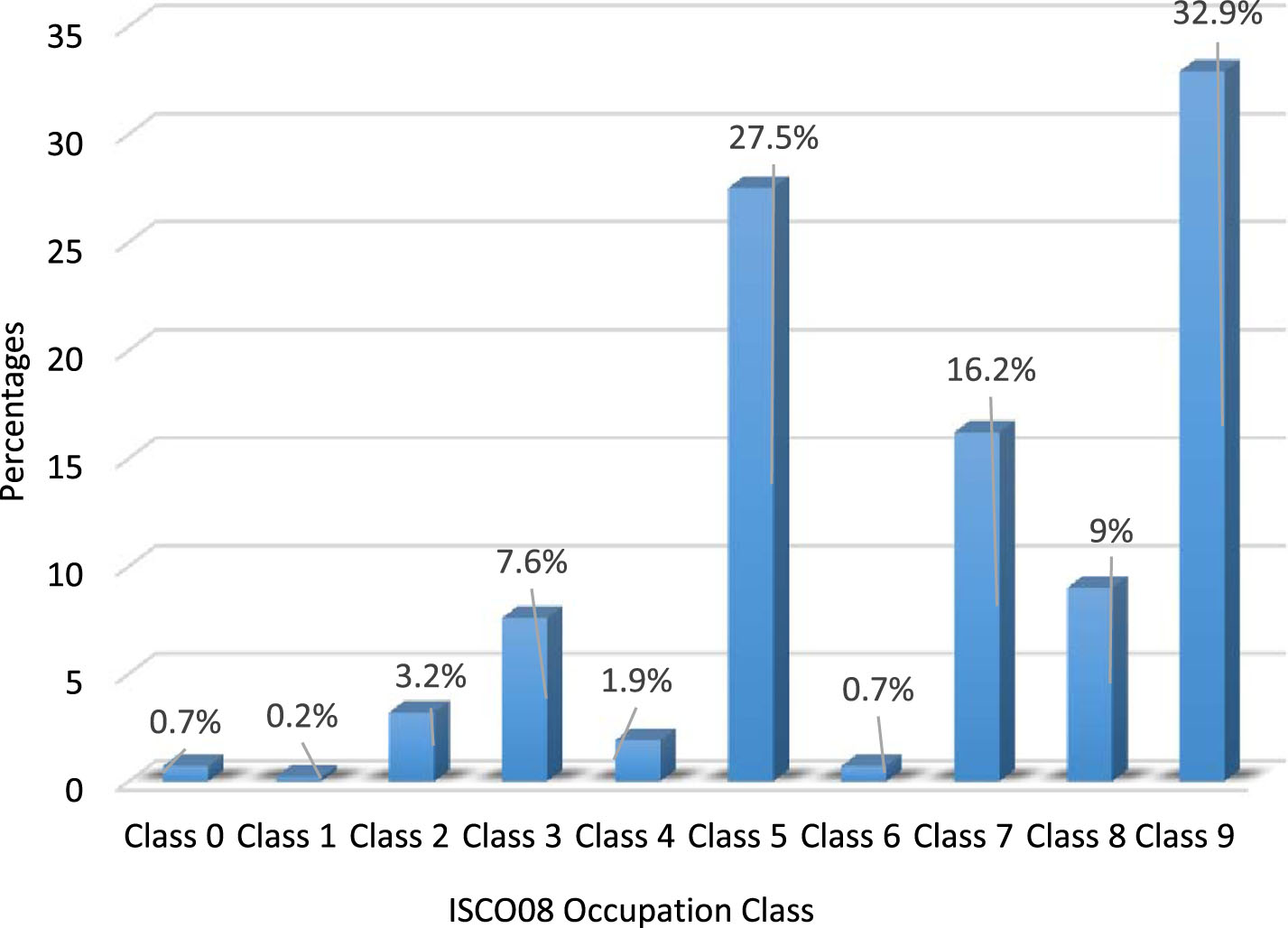
ISCO08 Occupations across number of LOI claimants.

Income Level distribution against number of LOI claimants.
From the 432 claims that met the inclusion criteria, we excluded 68 LOI claims as they did not meet the criteria for RTW. These claimants were mostly unable to RTW because they were permanently disabled or near retirement age. Of these 84% (n = 304) claimants RTW and 16% (n = 60) did not RTW. The average time away from work for LOI claimants was 362 days (Table 4).
Statistical outcomes for initial settlement, amount earned per month and time away from work
Statistical outcomes for initial settlement, amount earned per month and time away from work
Of the 432 claim sample, 72% (n = 312) of the claimants had no evidence of a RTW plan, individual rehabilitation plan, or RTW engagement with the employer. This may be because most claimants were either self-employed or working elementary jobs. Most claimants were not formally employed and therefore the MVA Fund potentially could not engage with any employer in their RTW advocacy.
Most of the claimants from the 432 sample were in the low-income group (79.6% [n = 344]) (Table 1). The middle-income group made up 13.2% (n = 57) of claimants, and the high-income group made up 7.2% (n = 31) of claimants. Claimants earned on average BWP 2448.21 per month (Table 4). In our study, 24.8% (n = 107) of claimants extended their initial sick leave or incapacitation period and increased their LOI benefit period.
Association between demographic variables and RTW
Only 364 claims were analysed for RTW correlations. From the 364 sample, 84% (n = 304) claimants RTW whilst 16% (n = 60) of the claimants did NRTW. The Fisher Hamilton test was significant with p-value<0.000. We rejected the null hypothesis and concluded that the status (RTW and NRTW) is associated with the type of injury sustained.
For moderate injuries it is observed that more people (134) returned to work than expected (119). For severe injuries less people (158) returned to work than expected (172), 80% of the claimants who did NRTW had severe injuries whereas 52% of those who RTW had severe injuries and 44% had moderate injuries. RTW was also compared with injury severity. The Pearson’s chi-square test for the comparison had a p-value of 0.000 (Table 5) which was significant. We rejected the null hypothesis and concluded that the status (RTW and NRTW) is associated with the injury severity.
The association between demographic characteristics and return to work among claimants of the Motor Vehicle Accident Fund Botswana, January 1, 2015 to December 31, 2020
The association between demographic characteristics and return to work among claimants of the Motor Vehicle Accident Fund Botswana, January 1, 2015 to December 31, 2020
Claimants with minor injuries took a shorter time (210 days) to RTW to work compared to moderate and severe injuries (244 days and 323 days respectively). RTW seemed to take longer the more the injury severity increased from minor to severe. For those who did not RTW the same was also observed with time away from work being 73 days for minor injuries, 474 for moderate injuries and 708 days for severe injuries claimants (Table 6). There was no significant relationship between the RTW and gender nor age with a Pearson’s chi-square test score of 0.412* and 0.055* respectively.
Mean time away from work (days) against injury severity
In our study, RTW was associated with the presence of any form of RTW intervention such as individual rehabilitation plan or RTW plan or RTW engagement with a Pearson’s chi-square test of 0.032 (Table 7) which was significant. We rejected the null hypothesis and concluded that the status (RTW and NRTW) is associated with the presence or absence of a RTW Plan.
The association between employment characteristics and return to work) among claimants of the Motor Vehicle Accident Fund Botswana, January 1, 2015 to December 31, 2020
The association between employment characteristics and return to work) among claimants of the Motor Vehicle Accident Fund Botswana, January 1, 2015 to December 31, 2020
Status was not significantly associated with income level or monthly earnings (Table 8). Status (RTW/NRTW) was however associated with the presence or absence of an addendum offer, with claimants Fisher exact test p-value of 0.003* which was significant. We rejected the null hypothesis and concluded that the status (RTW and NRTW) is associated with the presence of absence of addendum offers. When considering those who RTW, those with no addendum offers RTW in a shorter time (average of 235 days’ time away from work) compared to those with addendum offers whose time was longer (average of 458 days’ time away from work) as depicted in Table 8 and Table 9. RTW was however not associated with income level at a p value of 0.514 which we accepted the null hypothesis that there was no association between status and the income level.
The association between socio-economic characteristics and return to work among claimants of the Motor Vehicle Accident Fund Botswana, January 1, 2015 to December 31, 2020
The association between socio-economic characteristics and return to work among claimants of the Motor Vehicle Accident Fund Botswana, January 1, 2015 to December 31, 2020
Mean time away from work (days) against addendum offers for LOI claimants
We include all the significant variables identified in the univariate analysis in the final model (Table 10). In the multivariate model, Status (RTW and NRTW) was associated with time away from work and injury severity (Table 10) at a p value of 0.002. This, therefore, meant that those with less time away from work were more likely to RTW as opposed to those with longer time away from work. Furthermore, those with severe injuries were less likely to RTW compared to those with minor injuries.
Multivariate logistic regression of factors associated with return to work among claimants of the Motor Vehicle Accident Fund Botswana, January 1, 2015 to December 31, 2020
Multivariate logistic regression of factors associated with return to work among claimants of the Motor Vehicle Accident Fund Botswana, January 1, 2015 to December 31, 2020
In this study, we described the demographic profiles of LOI claimants of the MVA Fund Botswana over a five-year period, from January 1, 2015 to December 31, 2020. We also investigated if any of these variables were associated with RTW. LOI claimants to the MVA Fund in Botswana were mostly young, unskilled workers, reflecting the dilemma that many low-and middle-income countries face. Few people can afford health insurance and the benefits that compensation funds offer is often more than their basic incomes before being involved in an RTA. For some claimants, there is thus very little incentive to RTW.
In our study, claimants had an average monthly income of BWP 1219, which is about half of the lower tax limit and far less than the BWP 6000 offered by the MVA Fund Botswana. The biggest cluster of LOI claimants in our study were from low income levels and employed in the informal sector, often with limited education and doing physical labour. Officially, the average time away from work was 185 days. Considering that those formally employed may still have paid sick leave before the 185 days are exhausted, for self-employed people and informal sectors this is detrimental as their loss is immediate. Therefore, value is likely to only benefit people who are formally employed. People working in the informal sector are likely not to have had a set time point for RTW and to face systemic barriers where other losses of business may not be covered. For some of the informal sector claimants, their sick leave policy is 20 days as opposed to formally employed employees whose sick leave policy can be between 3–6 months paid leave as per Botswana Employment Act of 2007. It may therefore not reflect here considering the average time away from work was 185 days, and some may not have suffered loss as yet hence no need to lodge an LOI claim. This segment of the employment population needs advocacy for RTW and employers who are willing to support them during the rehabilitation period to avoid being replaced or terminated during the period of recuperation.
The findings highlighted that there was no significant difference between whether one is male or female as a slight difference of 6% was observed across the gender, with the male figure being higher. Therefore the results are indicating a shift in the cultural expectations and maybe a paradigm shift in the modern day women’s roles especially that most households in Botswana are female headed and therefore, necessitating a need to provide for their families [38–40]. However, even in Namibia, young adult drivers were also found to be at risk of RTAs, with over 75% of those sustaining serious injuries being in the ages of between 18 and 45 years old, which makes up 35.8% of the Namibian population [41]. Like our sample the average age of drivers involved in a road traffic accident in Namibia was 37-years old. This is attributed to the fact that younger drivers take more risks. Once again, the studies did not differentiate by gender, in fact mostly indicated that men were more likely to die in a motor vehicle accident [41].
The long period away from work is consistent with the traumatic nature of injuries caused by RTAs and the lack of trauma specialists in Southern Africa which often lead to delays in getting specialist treatment [1, 41]. In our study, almost 60% of claimants suffered severe injuries of which most were fractures (47.7%) and injuries to the head (39.8%). These injuries often require long hospital or ICU stays, and at times, multiple surgical procedures, rehabilitation and timely intervention which at times are not easily available in the Southern African region [41–43]. Given that most of the claimants in our study were employed in the informal sector, severe injuries are more likely to result in a LOI and delayed RTW [43]. Similarly, injuries to the head which formed 39.8% of the severe injuries on the sample may lead to cognitive impairments and delayed RTW as claimants have to undergo intensive cognitive rehabilitation [37]. Although our study did not have a control for the type of road crash but only relied on the type of injuries sustained which head injuries were leading. It may be argued that road crashes in Sub-Saharan Africa has been linked to an increased risk of head injuries due to inadequate and unsafe public transportation systems and the absence of footpaths, sidewalks and safe crossings, as well as, poor maintenance of those pedestrian ways that do exist, and the lack of speed control, and street lighting amongst others. [42] In our study, Status (RTW or NRTW) was associated with the type of injury sustained and the severity of the injury sustained (Table 5), rather than with age and gender as described in previous studies [17, 35]. Studies in Southern Africa do not mention these demographics with regard to RTW [41] however, they do mention that the presence of funders such as MVA Fund does improve the quality of life in comparison to other people of the same injuries who do not have such support as it limits treatment options for trauma management [42].
Aside from injury type and injury severity, RTW was also associated with the presence of a rehabilitation or RTW plan. A RTW plan is an immediate advocacy and may be different for someone who is not formally employed. In the insurance industry, RTW plans are dependent on the existence of an employer-employee relationship or where assistance is means tested. [40] In our study, 72% of claimants did not have a RTW plan even though this was expected as part of the MVA Fund Botswana processes. The absence of RTW plans may be due to the fact that most claimants were in the informal sector or were self-employed as previously mentioned, therefore having no employer to advocate to. We suggest that the MVA Fund Botswana should consider RTW advocacy or support for informally employed or self-employed claimants as they are more likely to suffer immediate loss of income. They are also more marginalised due to having no structures in place to support them. Furthermore, MVA Fund Botswana should review the processes of offering minimum wage to the informal sector, since often this group of LOI claimants cannot prove their income, it negatively impacts them as compared to those in formal employment. A RTW plan is an important aspect of case management because it gives a synopsis of all the interventions, risks, and predictors of RTW or RTW prospects. A RTW plan includes engagement with the employer and highlights any support that the employer may need to integrate the employee or enable them to RTW. Literature indicates that early intervention and the presence of a RTW plan can help with effective and successful RTW [15].
Unfortunately, people from low socio-economic backgrounds do not always have access to healthcare interventions or rehabilitation services [38]. Many people from low socio-economic backgrounds cannot afford to take time off work because they can be easily replaced [39]. In our study, Status (RTW/NRTW) was associated with the presence or absence of addendums or extension of their LOI cover.
Cartwright and Roach [32] suggested that claimants who received compensation would be reticent to RTW, since returning to work would result in no further LOI. MacKenzie, Morris, Jurkovich, Yasui, Cushing, Burgess, DeLateur, McAndrew and Swiontkowski [17,44, 17,44] also suggested that claimants from low socio-economic backgrounds, as in our study, would take longer to recover due to lower education levels and being poorer, as these factors are associated with non-compliance to medical treatment owing to health inequalities, rehabilitation access, and general understanding of compliance and processes. Although most of the claimants eventually did RTW, they took longer to RTW.
Fraud may also play a role in delayed RTW. Claimants may feign injuries to extend their LOI claims [32]. Although there is little research investigating insurance fraud in the MVA Fund Botswana, there is evidence of fraud from the Road Accident Fund South Africa [45]. Evidence from the United Kingdom indicates that 40% of personal injury claims following a RTA may be suspicious, involving some degree of malingering [32].
Limitations of the study
We described the demographic characteristics of LOI claimants, who submitted successful claims from 2015–2020, and the relationship between demographics and RTW. Our study excluded LOI claimants from previous years and Acts, some of whom were granted lump sum benefits following their injuries. Furthermore, the study did not explore the causative effects leading to such associations, further studies can explore these variables further to establish the causative relationships between the RTW status (RTW/NRTW) and the demographic variables.
Conclusion
In conclusion, RTW status (RTW/NRTW) is significantly associated with the following: Type of injury sustained, Severity of the injury sustained, Presence/Absence of a RTW plan, and Presence/Absence of an addendum offer.
Furthermore, RTW/NRTW can be predicted using the injury severity and time taken away from work. We predict that LOI claimants who experienced severe injuries would take longer to RTW, and that the more time off work, the less likelihood of RTW, especially when employed in the informal sector. The MVA Fund Botswana needs to understand the demographic profiles of claimants and develop tailored RTW programs to ensure positive RTW outcomes for LOI claimants.
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The study was approved by the Research Ethics Committee of University of Pretoria (Ethical approval number 255/2021) and the Ministry of Health Botswana –Health Research and Development Unit Reference (No. HPRD: 6/14/1).
Informed consent
Informed consent for the use of data was obtained from the Motor Vehicle Accident Fund Botswana, Chief Executive Officer. The researchers ensured that all identifying information on the claim records or data, including patients’ names, initials, or hospital numbers, would not be published in written descriptions or any part of the publication.
Funding
The authors would like to declare a £2000 grant towards the first author from Elizabeth Casson Trust.
Footnotes
Acknowledgments
The authors would like to thank The Motor Vehicle Accident Botswana for the permission to carry out the study within the organisation.