
Abstract
BACKGROUND:
Hands execute intricate tasks vital for everyday life and professions such as cooking, tailoring, and craftsmanship.
OBJECTIVE:
This study aimed to establish reference data for hand grip and palmar pinch force sense in young adults, accounting for gender differences, and to determine the correlation between these data and school-entry ages.
METHODS:
The cross-sectional observational study comprised 284 participants (156 females and 128 males). Demographic details, including age, gender, weight, and height, were recorded. Participant ages ranged from 18 to 29, representing the youth workforce population as defined by the International Labour Organization. Factors like hand dominance and school-entry age were ascertained based on participants’ self-reports. Hand grip and palmar pinch force senses were separately assessed in the dominant and non-dominant hands of 130 randomly chosen participants to evaluate test-retest reliability.
RESULTS:
Hand grip (dominant: p < 0.001, non-dominant: p = 0.002) and palmar pinch force sense errors were significantly lower in male participants compared to females. Palmar pinch force sense error for the dominant hand was reduced in males (p = 0.002), but no significant disparity existed between genders for the non-dominant hand (p = 0.222). Healthy adults who began school at age five or earlier exhibited a decreased force sense error rate (p < 0.05).
CONCLUSIONS:
Force sense error reference values vary based on gender and school-entry age. This reference data will aid rehabilitation specialists working with young adults in physiotherapy and occupational therapy fields in identifying potential impairments.
Keywords
Introduction
Proprioception is a fundamental sensory system that enables the peripheral and central nervous systems to communicate, forming the basis of joint position awareness, postural orientation, and spatial positioning. It encompasses kinesthesia, joint position sense, and force sense, each contributing to the execution of precise movements [1]. The development of proprioception is particularly crucial during youth, a period characterized by significant growth and learning. As children progress through developmental milestones, their proprioceptive abilities underpin the acquisition of fine motor skills, such as those required for hand grip and pinching techniques [2].
Research on proprioception has traditionally concentrated on populations at specific time points, predominantly adults or those in early childhood, yet it has neglected to adequately address the continuum of pediatric developmental processes. Youth’s unique developmental trajectory is critical to their educational and social needs [3, 4]. The absence of specialized reference data for youth obstructs the precision of assessments and the crafting of interventions tailored to their needs. Studies have underscored that proprioceptive impairments in youth can markedly interfere with the evolution of motor skills and everyday functionality [5, 6]. Moreover, proprioceptive development has been linked to competencies in coordination and balance, which are pivotal in physical education settings and impact learning and adaptability [7]. Recent findings underscore the potential of proprioceptive training specifically designed for youth to bolster injury prevention and rehabilitation, especially in sports [8]. This situation is further corroborated by evidence suggesting that customized rehabilitation programs, founded on reliable reference data, yield better outcomes for children with developmental coordination disorders [9]. Such evidence underscores the imperative to establish comprehensive reference datasets for proprioceptive development in youth.
Against this backdrop, force sense— the ability to discern and interpret forces within a joint— becomes a salient factor for rehabilitation specialists and occupational therapists to consider. [10]. These professionals apply this knowledge in designing and implementing therapeutic strategies tailored to enhance hand grip and pinching capabilities, which are not only critical for blue-collar occupations but also for daily tasks and leisure activities [11–14]. There is, however, a scarcity of research examining the relationship between hand grip and pinch strengths and various demographic characteristics among children and young adults. This includes the interplay between these strengths and factors such as gender, hand preference, anthropometry, and school-entry age [15, 16]. While therapists possess abundant tools to measure grip and pinch strength, resources to interpret force sense error— a key aspect of proprioceptive evaluation in the hand— are insufficient [17–19]. Studies focusing on enhancing the perception of pinch strength and the immediate effects of interventions like kinesiotape on hand grip force sense have shown promising directions, yet they are limited by small sample sizes and inadequate demographic considerations [20, 21]. Recognizing this gap, our study aims to delineate how school entry age influences proprioceptive abilities in young adults and to formulate gender-specific reference data. Through this research, we intend to enrich the understanding of the developmental implications of early schooling on sensory-motor skills, thereby filling a pivotal void in the existing educational and developmental discourse.
Methods
Subjects
This cross-sectional study was conducted in the Occupational Therapy Laboratory at Çankırı Karatekin University Faculty of Health Sciences from September to November 2022. The study population consisted of young adults (n = 284) residing in seven different regions of Türkiye. The study focuses on the transition from adolescence to adulthood, focusing on youth aged 18 to 29, who typically complete formal schooling and enter the workforce [22]. This age range is crucial for assessing proprioceptive development, as the maturation of proprioceptive accuracy stabilizes during late adolescence [23]. The chosen sample is representative of this developmental stage. All participants provided their informed consent by signing a consent form that explained the study’s objectives and procedures. This research adhered to the principles outlined in the Declaration of Helsinki and was designed as an observational study.
The Çankırı Karatekin University Research Ethics Committee determined that no ethical approval was required for this study, as indicated by protocol number e14d9d12b9574b42.
To establish accurate norms, individuals with specific conditions, such as cognitive or neurological disorders, upper extremity pain, functional limitations, or cognitive impairments, were excluded from the study.
Instrumentation and procedures
This study rigorously collected demographic data from participants, including age, gender, body mass index (BMI), height, and other characteristics such as hand dominance and age at school start, using a standardized questionnaire. The BMI was computed by dividing the weight in kilograms by the square of the height in meters, which is a widely accepted measure for determining the relationship between a person’s weight and height.
In order to familiarize participants with the evaluation equipment and minimize the impact of learning effects, a preliminary session was conducted where they practiced using hand dynamometers and pinch gauges. Subsequently, we systematically collected measurements of hand grip and palmar pinch force from both the dominant and non-dominant hands of a selection of 130 people. These participants were randomly selected using a Simple Randomization technique to evaluate the reproducibility of the test-retest. The selection was conducted using a random number generator to ensure the impartiality of our sample. Figure 1 visually illustrates the test setup and procedural details to improve understanding of the testing methodology.
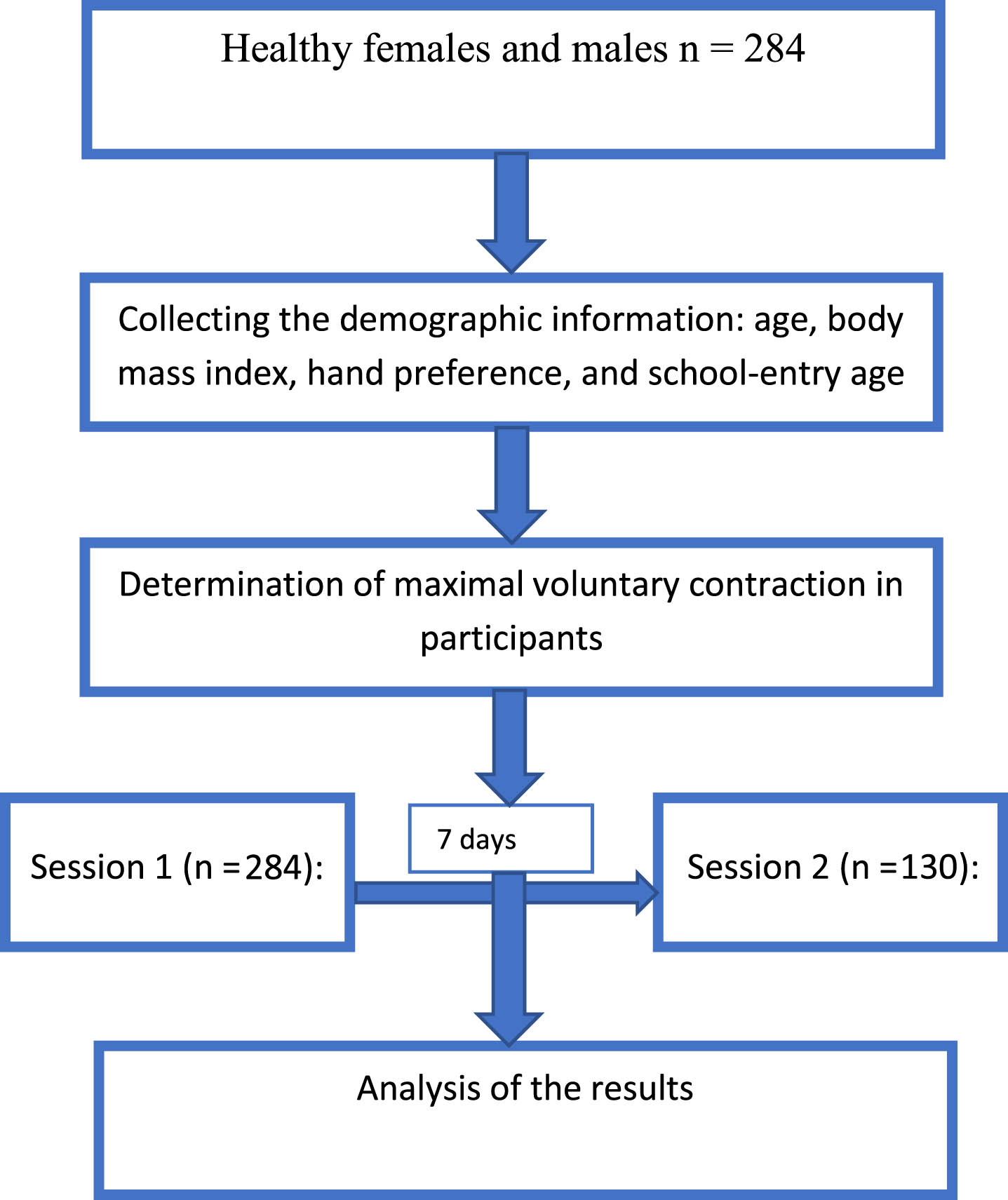
Flowchart of the study.
Prior to conducting force sense measurements, MVC values for each hand were determined by placing the hands in the appropriate test position. Researchers (CT and EK) instructed participants to gradually increase their strength over a 2-second period and then maintain maximum grip and pinch strength for an additional 3 seconds. The MVC value was calculated based on the most stable region of the force recording. For each hand, the larger of the two gripping or pinching efforts was designated as the MVC, and this value was used as the reference point for assessing force sense (20% of MVC for hand grip and 30% of MVC for pinch force sense).
To prevent fatigue, participants alternated between maximum efforts with their hands, followed by 3-minute rest periods.
Assessment of hand grip force sense error
We employed an electronic hand dynamometer (Baseline Smedley Digital Hand Dynamometer; Fabrication Enterprises Inc, Irvington, NY) for the measurements. Prior to conducting force sense error measurements, MVC were recorded for each hand. Participants were instructed to gradually increase their grip strength over a 2-second period and maintain their maximum strength for an additional 3 seconds. This duration of sustained pressure in proprioceptive measurements is chosen due to existing literature indicating it is a critical threshold for activating mechanoreceptors responsible for proprioceptive feedback [24]. After determining the MVC values for both the right and left hands, 20% of the MVC was established as the reference point for measuring hand grip force sense errors.
To prevent fatigue, participants alternated their maximum effort between their hands, with 3-minute rest periods in between. Participants were given a brief practice session to learn how to achieve the 20% MVC reference grip force without relying on visual feedback. They were asked to grasp the handle, apply the required hand grip force within 2 seconds, and sustain that force for an additional 3 seconds, with verbal cues provided during the effort. If the actual hand grip force during the holding phase deviated by more than 5% from the planned force, an additional trial was conducted. However, participants quickly learned to consistently apply the required force level based on their perception within two to three practice trials for each hand. The absolute error (AE) of the hand grip force sense was calculated by averaging the differences between the matched and reference forces, expressed in “MVC% ”.
The participants were instructed to exert the target force, which was set at 20% of their MVC, for a duration of 3 seconds and were asked to remember the level of force applied. Subsequently, they received a verbal cue to relax and were required to close their eyes. After a 3-second interval, participants were tasked with reproducing the previous pinch strength without the benefit of visual feedback. When participants believed they had matched the previous force level, they released the device, and the device recorded the applied force. Following this, participants were instructed to relax once more. To mitigate the risk of fatigue, a 30-second rest period was incorporated at the conclusion of each trial.
To assess the reliability and measurement precision of the test, each participant underwent the protocol under consistent conditions. This involved working with the same experienced tester in the same laboratory at roughly the same time, with a one-week interval between sessions (session 1 and session 2). Participants reported no notable health, clinical, or functional changes between the initial testing and re-testing. Additionally, participants were advised to abstain from engaging in physical activity immediately before the testing session and between the initial testing and re-testing to minimize the potential impact of fatigue on the test results.
Assessment of palmar pinch force sense error
We utilized the Jamar digital pinch gauge (Patterson Medical, Bolingbrook, IL, USA) for measurements. Participants were instructed to use palmar pinching. Prior to testing, they engaged in warm-up activities specific to the type of pinch force to be assessed. Following the warm-up, participants were directed to exert maximum pinch force on the dynamometer. This test was conducted twice for each type of pinch grip, and the highest recorded value was documented as the pinch strength. To mitigate the potential impact of fatigue, participants were granted three-minute rest periods between tests.
Participants were instructed to exert the specified target force, which was set at 30% of their MVC, for a duration of 3 seconds and were tasked with remembering the level of force applied. Following this, they received a verbal cue to relax and were instructed to close their eyes. After a 3-second interval, participants were prompted to replicate their previous pinch strength without any visual feedback. When participants believed they had matched the prior force level, they released the device, allowing it to record the force. Participants were then instructed to relax once more. To mitigate the risk of fatigue, the protocol used in the hand grip force sense error test was also applied in assessing palmar pinch force sense error.
Statistical analysis
All statistical analyses were conducted using the Statistical Package for Social Sciences (SPSS, version 28.0; SPSS Inc, Chicago, IL). Prior to analysis, data normality was assessed using the Kolmogorov-Smirnov and Shapiro-Wilk tests. Continuous variables were described using mean and standard deviation, while categorical variables were presented as frequency and percentage.
To assess test-retest reliability, several statistical methods were employed. These included: the calculation of the mean difference with a 95% confidence interval (CI) [25] and the computation of the intraclass correlation coefficient (ICC) with 95% CI estimates based on 2-way mixed effects, absolute-agreement, and single-measurement models [26]. ICC values were interpreted as follows: poor (0.00 to 0.39), fair (0.40 to 0.74), and good (0.75 to 1.00) [27].
To examine gender-related variations in force sense error levels, the Independent Samples t-test was utilized. For assessing differences in force sense errors among three groups based on school-entry age, a one-way analysis of variance (ANOVA) test was applied. Since the sample distribution among groups was not uniform, pairwise comparisons between groups were conducted using Bonferroni correction as a post-hoc test. A significance level of p < 0.05 was chosen to determine statistical significance.
Results
Physical characteristics of subjects
Table 1 provides an overview of the physical characteristics of the young adult participants in the study. A total of 284 participants completed the test procedures, with 156 (54.9%) females and 128 (45.1%) males. Among these participants, 257 (90.5%) reported right-hand dominance, comprising 141 (48.9%) females and 116 (40.3%) males, while 27 (9.5%) reported left-hand dominance, with 15 (5.3%) females and 12 (4.2%) males falling into this category. None of the participants reported ambidexterity.
Demographic characteristics of participants
Demographic characteristics of participants
Abbreviations: SD: Standart deviation, % : percentage.
Additionally, Table 1 includes information about the participants’ age (mean±standard deviation: 21.2±1.5) and BMI (mean±standard deviation: 22.4±3.7).
The test-retest reliability results for the study sample (n = 130) were analyzed. The participants demonstrated fair to good test-retest reliability for force sense errors in hand grip (0.70≤ICC≤0.74; p = 0.001) and palmar pinch (0.71≤ICC≤0.77; p = 0.001) (Table 2).
Test-retest reliability results of the hand grip and palmar pinch force sense error tests
Test-retest reliability results of the hand grip and palmar pinch force sense error tests
Abbreviations: MVC% : Percentage of maximum voluntary contraction.
Table 3 presents the reference values for hand grip force sense errors categorized by gender and school-entry age. It was observed that hand grip force sense errors were significantly lower in males compared to females (dominant: p < 0.001, Cohen’s d = 0.15; non-dominant: p = 0.002, Cohen’s d = 0.40). When the hand grip force sense errors were compared based on the participants’ school-entry age, it was found that the dominant hand grip force sense errors of participants who were five years old or younger than the school-entry age were lower than those of participants who reached school-entry age at seven years (p = 0.006, Cohen’s d = 0.36). However, on the non-dominant side, there was no significant difference between participants with different school-entry ages (p = 0.077, Cohen’s d = 0.18). Figures 2A and 2B also illustrate the variations in hand grip force sense error values based on both school-entry age and gender.
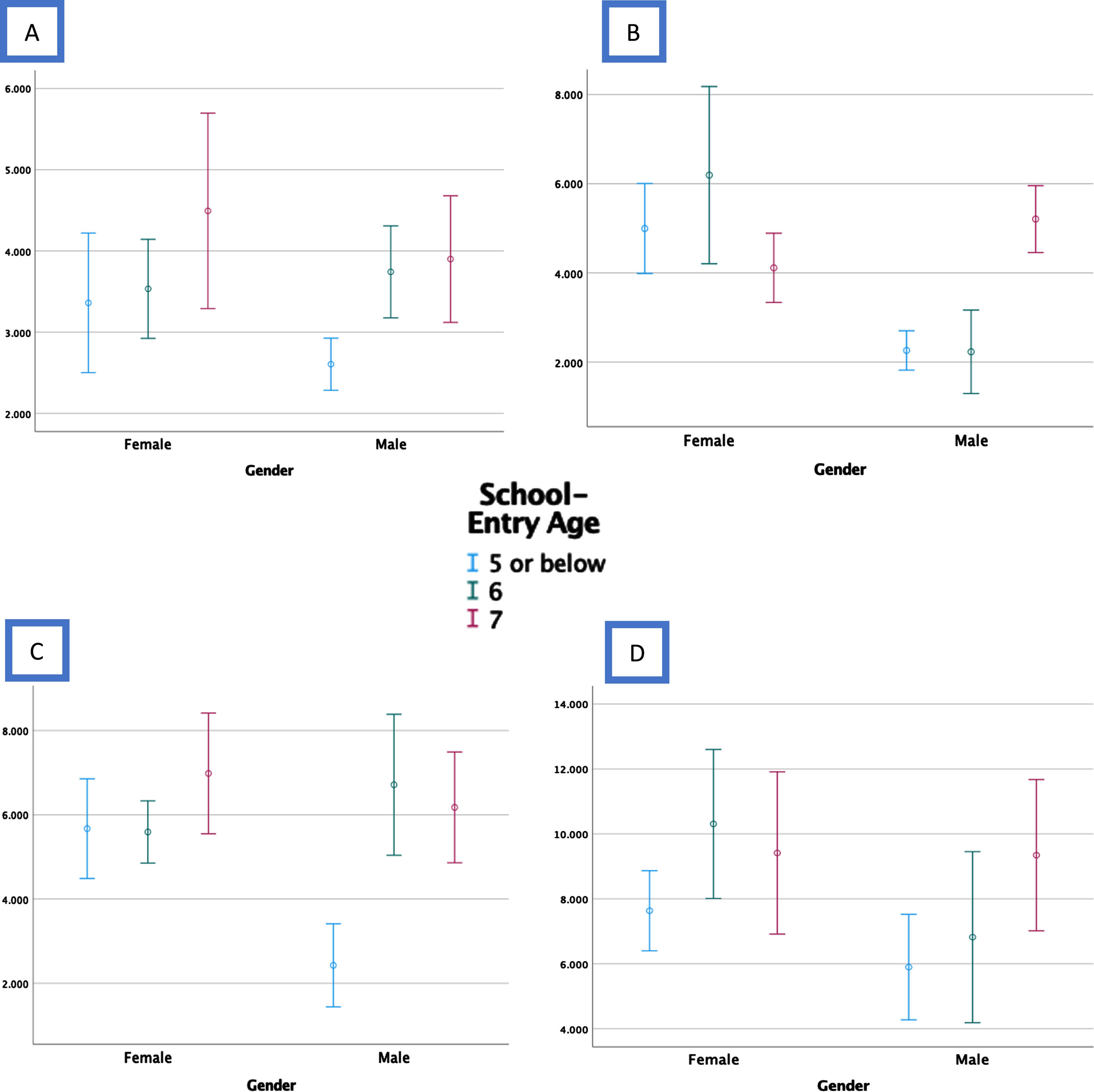
Force sense error bars separated by both gender and school-entry age of the participants. A. Dominant hand grip, B. Non-dominant hand grip, C. Dominant palmar pinch, D. Non-dominant palmar pinch.
Results of the hand grip and palmar pinch force sense error tests
Abbreviations: MVC% : Percentage of maximum voluntary contraction. SD: standard deviation, *Independent Samples t-Test; One-Way ANOVA; l: lower than the higher value group or groups according to the Bonferroni correction. h: higher than the lower value group or groups according to the Bonferroni correction.
Table 3 displays the reference values for palmar pinch force sense errors. On the dominant side, it was found that palmar pinch force sense errors were lower in males (p = 0.002, Cohen’s d = 0.19), while there was no significant difference between genders on the non-dominant side (p = 0.222, Cohen’s d = 0.07).
When comparing the palmar pinch force sense errors based on participants’ school-entry age, it was observed that the dominant palmar pinch force sense errors of participants aged five and younger were lower than those of individuals who entered school at the age of six or seven (p = 0.010, Cohen’s d = 0.32). Similarly, on the non-dominant side, participants who entered school at the age of five or younger exhibited lower palmar pinch force sense errors than those who entered school at the age of seven (p = 0.021, Cohen’s d = 0.27). Figures 2C and 2D further illustrate the variations in palmar pinch force sense error values based on both school-entry age and gender.
Discussion
The findings from this study have elucidated vital reference data for hand grip and palmar pinch force sense among young adults, distinguishing differences across gender lines and establishing a correlation with school-entry age. The analysis revealed a statistically significant lower force sense error in male participants for both hand grip and palmar pinch for the dominant hand. In contrast, gender differences for palmar pinch force sense in the non-dominant hand did not reach statistical significance. Furthermore, an intriguing aspect of the findings is the association between early school-entry age and decreased force sense error rates, suggesting that educational environment and developmental milestones may play a role in sensory-motor proficiency.
These results carry significant implications for clinical practice, particularly for rehabilitation specialists in physiotherapy and occupational therapy who work with young adults. The reference values provided can serve as benchmarks for identifying potential impairments and customizing therapeutic interventions. By integrating these results with the broader spectrum of somatosensory research, this study contributes to a more nuanced understanding of the interplay between sensory capacity and demographic factors such as gender and early education.
In this study, a hand dynamometer and pinch gauge were employed to assess hand grip and palmar pinch force sensation, revealing a reasonable-to-good level of test-retest reliability. However, it is noteworthy that the reliability of force sensation measurements using these devices, while still deemed acceptable, falls below the reliability levels achieved in strength measurements conducted with similar devices [16, 29]. This disparity may arise from the fact that the force sensation measurement protocol demands greater concentration and a more intensive cognitive process compared to the MVC measurement protocol.
The study sample is chosen to represent youth at a critical developmental stage for proprioceptive maturation, a period during which key skills are acquired and refined [30]. This age range coincides with significant neurological and motor developments, making it an optimal window for studying proprioceptive benchmarks [31]. This sample provides broad insights for assessment and intervention strategies. Our data unveiled variations in force sense errors for both handgrip and palmar pinch, which appear to be influenced by gender and the age at which individuals began their schooling. Based on the observed results for hand grip and palmar pinch force sense errors, it appears that males generally exhibit a heightened sensitivity in their grip and pinching abilities compared to females. Additionally, irrespective of gender, individuals who commenced their schooling at the age of five or younger exhibited an increase in both grip strength and pinch sensitivity.
Prior studies investigating force sense errors in relation to gender differences have yielded conflicting results [32, 33]. For instance, Shinohara et al. examined gender differences in sub-maximal force-matching tasks involving the fingers in a cohort of 24 healthy individuals, determining that male exhibited lower levels of force sense errors [32]. In their analysis, the researchers also delved into the “strength-dexterity trade-off” hypothesis as a potentially complicated factor when interpreting their findings. According to this hypothesis, there exists a reciprocal relationship between strength and dexterity, suggesting that an increase in strength may result in a decrease in dexterity [33]. It is worth noting that our research is devoid of this confounding factor. This is attributable to the calculation formula employed in our study, which computes force sense error as a percentage relative to an individual’s maximum strength. Consequently, the force sense error value was not assessed numerically but rather as a percentage specific to each person’s strength.
Supporting our study’s outcomes, which revealed that males exhibited a lower percentage of force sense errors, is the fact that females are more predisposed to upper extremity musculoskeletal injuries compared to males [34–36]. In a related vein, Li et al. devised a formula similar to ours based on MVC and expressed it as a percentage error in their assessment of force sense in a cohort of twenty healthy individuals. Their results closely mirrored our own findings [37].
In light of these analogous studies, it is reasonable to consider hand grip force sense errors within the range of 3 to 5 percent as reference values, aligning with the results of our study, which boasts a larger sample size (3.7% in the dominant hand for females, 5% in the non-dominant hand for males, 3.3% in the dominant hand, and 3.5% in the non-dominant hand for females). Conversely, for palmar pinch force sense, reference error values should be regarded within the range of 5 to 9 percent: specifically, 6% for the dominant hand, 8.8% for the non-dominant hand in females, and 5.7% in the dominant hand, and 7.5% in the non-dominant hand in males.
In this study, we observed both significant and non-significant differences in hand grip and palmar pinch force sense errors between dominant and non-dominant hands across various school-entry ages, irrespective of gender. Remarkably, across nearly all measurement parameters for both hands, students who commenced school at the age of five or younger consistently exhibited lower force sense errors. Notably, there is a dearth of studies that directly corroborate these findings or explore the influence of school-entry age on force sense. However, there is extant research indicating that error values associated with manual dexterity are age-dependent [38–40]. For instance, normative data on manual dexterity in children derived from functional dexterity tests illustrate a linear increase in manual dexterity from the age of three to seventeen [38]. These age-related enhancements in fine dexterity scores can be attributed to the maturation of the brain and corticospinal tract. During childhood and adolescence, there is an increase in white matter and a decrease in gray matter, which may account for heightened motor speed and motor performance [16, 41].
While the optimal age for commencing formal schooling remains uncertain, it is recognized that school activities exert positive biopsychosocial effects on various aspects of human development [42]. Conversely, it has been demonstrated that early school entry, particularly in regions with low socioeconomic status, is associated with a higher prevalence of neurodevelopmental and mental health-related issues. Subsequent years often bring forth conditions like attention deficit hyperactivity disorder and social difficulties in these early school starters [43]. Research by Chandler et al. highlights that nurturing writing skills during the preschool years enhances self-regulation and fine motor skills in children [44]. Likewise, the study by Piek et al. suggests that engaging in motor activities early in life contributes to cognitive development during the school years [45]. Given these considerations, it may be beneficial to introduce hand game tasks for gross motor functions and drawing activities for fine motor skills to children at earlier ages, especially within kindergarten or home settings. This approach can help mitigate musculoskeletal issues that may arise when young children spend prolonged periods at school, sitting at desks for extended durations.
Our foundational results pave the way for the development of practical interventions tailored to enhance proprioceptive function in occupational settings. For example, research indicating gender and age-related variations in force sense error suggests that ergonomic interventions can be customized to accommodate individual differences in proprioceptive abilities. This can include the design of tools and workstations that consider proprioceptive capabilities, thereby reducing the risk of strain and injury in the workplace. Furthermore, our results highlight the importance of early educational interventions in fostering proprioceptive skills, which can have long-term implications for occupational health. By incorporating proprioceptive training into educational curricula, policymakers can contribute to the prevention of workplace-related injuries and promote overall worker well-being.
Some limitations of this study are that although participants from seven different regions were included in it, the majority of the participants were from the interior regions of Türkiye. Participants’ results may not accurately reflect the overall population distribution. In addition, the number of participants who started school at the age of five or younger was lower than the other two groups. These imbalances in the number of participants led us to present the lower age groups as a single group. Another limitation of our study was that the variables possibly can be related to hand functions such as sport history, smartphone usage times, living areas, and socio-economics status of the participants were not evaluated in the study due to the fact that all participants were students. This study fails to fully address the potential effects of various factors on participants’ hand functions and proprioception. Particularly, the unequal distribution of participants across school entry age groups creates some limitations in representing the overall young adult population. Additionally, unexplored variables such as sports history, smartphone usage, living environments, and socioeconomic status are important factors that could affect hand functions and proprioception. The external validity of this study may be limited due to the omission of these factors. The applicability of the results to broader populations or different contexts should be considered under the influence of these and similar variables not covered within the scope of this study. Researchers suggest expanding the methodology in future studies to include these factors and conducting a more detailed examination of their effects on hand functions and proprioception.
In our study, we did not assess the impact of interventions carried out in preschool, kindergarten, or home settings to enhance hand activities in children who did not commence school at an early age. Consequently, there is a pressing need for research endeavors aimed at scrutinizing the outcomes of implementing age-appropriate activities in children, as opposed to early school entry, on their future hand functions. Furthermore, future investigations should delve into other variables that might exert an influence on the hand functions of these children. Based on the normative data presented in this study, we believe there is potential for therapists working with youth to apply these findings in educational, emotional, and social contexts. Further research is needed to fully understand the impact of these data when integrated into treatment protocols for injury rehabilitation in young people.
Conclusion
In summary, this research study provides valuable reference data on hand grip and palmar pinch force sense among healthy young adults while considering gender differences and the age at which individuals begin their schooling. The test-retest reliability of the force sense measurements, which ranges from fair to good, lends support to the validity of our findings.
Our study’s findings indicate a tendency for males to exhibit higher sensitivity in terms of grip and palmar pinch force perception compared to females. Furthermore, we observed that individuals who commence their educational journey at the age of five or earlier demonstrate a reduced occurrence of errors in force sense. To enhance hand function development in these children and mitigate potential musculoskeletal and mental effects of early school entry, we recommend options such as playgroups and kindergarten activities, such as drawing, which can improve hand functions before formal schooling.
These discoveries have the potential to enhance the assessment of force sense errors in clinical and rehabilitative contexts, thereby aiding in the evaluation of proprioceptive function and informing the development of rehabilitation protocols. Additionally, this study underscores the importance of considering demographic variables, such as gender and age at school entry, when assessing hand force perception. Nevertheless, further research with a more diverse and inclusive sample is necessary to validate and expand upon our findings.
In conclusion, a deeper understanding of tactile perception related to hand force and its associated demographic factors can enhance our strategies for mitigating musculoskeletal disorders and optimizing manual dexterity in both daily activities and occupational pursuits.
Ethical approval
The study was approved by the Institutional Review Board of Çankırı Karatekin University (Approval date: 28-09-2022, Application code: e14d9d12b9574b42).
Conflict of interest
The authors declare no conflict of interest.
Footnotes
Acknowledgments
The authors have no acknowledgements.
Informed consent
Informed consent was obtained from all study participants.
Funding
The authors received no funding for this study.