
Abstract
BACKGROUND:
It is important to measure the self-efficacy knowledge of the caregiver of Duchenne muscular dystrophy (DMD) patients in order to overcome the problems that arise and carry out the care process in a healthy manner.
OBJECTIVE:
This research was carried out to develop a self-efficacy scale in caregivers of individuals with DMD.
METHODS:
The study was conducted with 99 volunteer DMD caregivers to evaluate the psychometric properties of the developed scale. Exploratory Factor Analysis (EFA) was performed with the SPSS 25 Package Program to determine the factors of the scale. Confirmatory Factor Analysis (CFA) analysis was performed with AMOS 23 to confirm the factors obtained by EFA. Cronbach’s alpha coefficient was used for the internal consistency of the DMD-CSES.
RESULTS:
A valid and reliable scale was obtained to measure the self-efficacy of caregivers of DMD patients.
CONCLUSION:
Although some scales have been developed to evaluate the care burden of family members who care for patient-centered symptoms and functional changes in patients with DMD, there is no single scale that adequately describes the conditions and resources of caregivers on a global scale. The search for a definitive scale is expected to continue until a definitive treatment for the disease is found. Developing a valid and reliable scale to identify the self-efficacy, knowledge, skills and resources of caregivers with a common perspective of physicians and health management team centred on patients with DMD will be effective in practice.
Keywords
Introduction
Duchenne muscular dystrophy (DMD) is caused by a mutation in the dystrophin gene on the X chromosome, resulting in a deficiency in the production of the essential muscle protein dystrophin. It is characterized by progressive loss of muscle, strength and function. The disease is inherited, with a prevalence of 2 out of every 7,000–10,000 men born alive. There are three isoforms of dystrophin, specific to skeletal muscle, heart and brain tissue. Mutations between exons 1–31 have been found to affect these isoforms and comorbid disorders such as epilepsy and autism spectrum disorder have been reported to be seen at a significant rate in these patients [1–3]. There is no definitive cure, and medical rehabilitation still remains the most effective treatment. The loss of vital functions begins at an early age and they often lose walking between the ages of 8–13. With good care, death can be delayed until the age around 40, when death occurs from cardiac or respiratory failure [1].
In the musculoskeletal system, joint contractures, scoliosis, and tendon shortness device for them, physiotherapy for osteoporosis, muscle shortness, atrophy and fall prevention, standing exercises and the gastrointestinal system; the problem of excessive appetite increase and weight gain should be addressed with glucocorticoid therapy due to decrease in physical activity. With more frequent involvement of smooth muscles, swallowing, constipation, dyspeptic problems, motility, and tube feeding are needed in advanced ages [4].
The family’s initial rejection of the diagnosis, then anger, fear of loss, and then efforts to learn about the disease, seek treatment, and communicate with families in similar situations indicate that the family initiated the care process [5]. It has been observed that the problems faced by caregivers, such as feeling guilty about passing the disease on to their children, blaming each other, and uncertainty about how they feel in situations such as divorce, have been studied very little if the mother is a carrier [6, 7].
It is stated that measuring the self-efficacy knowledge of the person who undertakes the care task at every stage of the disease, from diagnosis to death in chronic diseases, is important in terms of overcoming complex multi-problems that arise or that will arise, and in carrying out this process in a healthy way. The family with self-efficacy will manage the process in coordination with the health team. This will enable to learn progressive care rules to improve patients’ quality of life, facilitate the development of correct management rules for good care, and increase the life expectancy of patients [8].
Although many studies have been conducted on family relationships, work life and social life conditions of DMD patients’ relatives, it has been observed that there are very few studies on the self-efficacy of caregivers and caregivers of this patient group. In fact, there is hardly a suitable scale for assessing the self-efficacy information of caregivers of DMD patients [9]. It has been argued that the self-efficacy values of caregivers and patients should be considered and analyzed as a whole. However, a common formula that would accurately describe the relationship between the patient and caregivers, who went through this process, could not be established. This shortcoming reveals the motivation for this study. Because, with this study, the self-efficacy information of the relatives of DMD patients, which is a special and rare disease, will be measured and the competencies of these people will be tried to be revealed [5, 10].
In the light of all this data, although some scales have been developed to evaluate the information and care burden of family members who care for patient-centered symptoms and functional changes in DMD patients, and to detect changes, there is only one single instrument that adequately describes the conditions and resources of caregivers in an organized global scale. In this study, DMD aimed to find a solution by developing a question-based scale to determine the self-efficacy skills of caregivers and the problems experienced, with a patient-centered, physician and health management team’s joint perspective.
Methods
This study, the details of which are given in the sections below, was examined in two stages.
The first stage is the pilot application, which includes information about the content validity of the scale draft being developed and the initial reliability of the draft scale.
In the second stage, the main study was conducted in which explanatory factor analysis and concurrent validity tests were conducted to evaluate the psychometric properties of the Self-Efficacy Scale for Caregivers of Duchenne Muscular Dystrophy (DMD) Patients (DMD-CSES) and to reveal the structure of the factors that make up the scale.
Statistical analysis
To carry out Exploratory Factor Analysis (EFA), the required Kaiser-Meyer-Olkin (KMO) value should be 0.60 and above, and the Bartlett’s Test of Sphericity (BTS) value should be statistically significant [11].
Principal Components Analysis and Orthogonal Varimax rotation method were used within the scope of EFA conducted for the DMD-CSES scale.
Four different stages of EFA analysis were followed to reveal a factor structure that was complete, accurate and consistent with the necessary criteria. In the first EFA analysis phase, it was determined that there was one item that loaded on all three factors of the scale. It was observed that the factor loading of this item, which loaded simultaneously on all three factors of the scale, was less than the critical value of 0.45. In addition, as a result of the first EFA analysis, it was determined that one item was loaded on two separate factors, but there was no literature relationship between these factors and the item. In the second EFA analysis stage, the item loaded on three factors at the same time and the factor load lower than the critical value of 0.45 was removed and the analysis was repeated. As a result of the second EFA analysis, the values improved slightly, but in the first stage, the item loaded on two factors at the same time and not related to the factor loaded and literature gave the same result. For this reason, the problem-causing item was removed in the second stage and the third EFA analysis stage was started. The third EFA analysis phase was re-introduced in the second phase of the item removed and the item that caused the problem in the second EFA phase removed. However, it was decided to remove two items that constantly caused problems in the first, second and third EFA analysis stages. The last stage, the fourth EFA analysis stage, was carried out with 18 items and according to this result, a three-factor, coherent structure emerged.
Scale development
A draft scale was prepared with a 20-items question pool based on the opinions of academics who have knowledge about neuromuscular diseases, the information provided by patient relatives and associations, and the literature. This draft scale includes 11 items related to the first factor, 6 items related to the second factor and 3 items related to the third factor.
The scale was prepared with a 5-point Likert type (1 = Strongly Disagree, 2 = Disagree, 3 = Undecided, 4 = Agree, and 5 = Strongly Agree). As the score obtained from the scale increases, the self-efficacy of the caregivers increases.
Four academic experts (a scale development and biostatistics specialist, a neuromuscular diseases and physiotherapy specialist, a researcher working on self-efficacy, and a public health specialist) evaluated the question items of the DMD-CSES scale for relevance and intelligibility.
Content validity was performed on the answers of the experts who evaluated the DMD-CSES scale draft. For this, a form was sent to the experts for each item as “appropriate”, “not applicable”, and “needs correction”. After these forms, the correspondence between the answers given was checked. This concordance was calculated for each item. As a result of this calculation, the lowest agreement was found to be 0.94 and the highest agreement to be 0.98. Especially neuro diseases and physiotherapy specialist suggested major changes in the expressions of some items. Some minor changes were made in line with the recommendations of the other three experts (See Appendix 2). With these corrections, a pilot test was conducted with the 20-items DMD-CSES draft scale.
Ethical considerations
Ethics committee approval (decision numbered 10.06.2021–105) was obtained from Dicle university. Informed consent was obtained from all caregivers of muscle patients who voluntarily participated in the study.
The pilot test
Sample
The pilot test sample consisted of 30 people who care for neuromuscular patients receiving health care from a training and research hospital in the province of Diyarbakır, located in the southern region of Turkey. The inclusion criteria of caregivers are as follows: (1) the caregiver must be the primary caregiver recognized by the patient, (2) the caregiver must live in the same household as the patients, (3) the patients diagnosed with neuromuscular disease, unable to perform self-care and in need of care. must be a family member, (4) be at least 18 years old.
The lowest age of caregivers is 22 and the highest is 65. The mean age of caregivers is approximately 42±10.1 years. Most of the caregivers were male (56.7%), the majority were married (83.3%), the monthly income of the majority was 4000 Ł or less (76.7%), and the education level of most of them was primary and secondary school (56.7%).
Internal consistency
Cronbach’s alpha coefficient was used for the internal consistency of the DMD-CSES total scale and sub-dimensions used in the pilot test. Accordingly, the DMD-CSES total scale Cronbach’s alpha coefficient was 0.826. The Cronbach’s alpha coefficient of the three sub-dimensions that make up the DMD-CSES scale ranged from 0.756 to 0.819. These values are above the acceptable value of 0.70 [12].
Test-retest reliability
Test-retest reliability was used to reveal whether the DMD-CSES scale was of the same stability. The results of the pilot test application and the main test application were compared. The main test was applied in the second week after the pilot test. The Pearson correlation coefficient was used for the test-retest reliability. According to the test-retest reliability results between these two tests, a statistically significant correlation was found between the pilot test results and the main test results (r = 0.87, p < 0.001). In addition, a statistically significant positive correlation was found between the sub-dimensions of the scale according to the test-retest reliability results. Accordingly, a positive and strong correlation was found between the first factor (r = 0.83, p < 0.01), the second factor (r = 0.90, p < 0.01) and the third factor (r = 1.00, p < 0.01) pilot application scores and the main application scores. In addition, the intraclass correlation coefficient was found to be 0.85 for the total scale and between 0.78 and 1.00 for the subscales (p < 0.01). According to the results obtained, a very strong similarity was found between the results of the pilot application and the main application of the 18-item DMD-CSES scale.
The main test
Sample
The main application sample consisted of 99 people from families of neuromuscular diseases who received health care from a training and research hospital in Diyarbakır, located in the southern region of Turkey. The inclusion criteria of caregivers for the main application were the same as the inclusion criteria in the pilot test. There were 144 patients registered in the training and research hospital where we conducted the study. It was requested to conduct the study with all patient caregivers. For this reason, no sample selection was made. However, 3 of the caregivers were illiterate and 3 people were not included in the study because they were under the age of 18. For this reason, the pilot study was conducted with 30 people and the main study was conducted with 99 people. The data of the study were collected between May 10 and June 10, 2021.
The lowest age of caregivers is 20 and the highest is 73. The mean age of caregivers is approximately 37±10.2. Most of the caregivers were female (62.6%), the majority were married (71.7%), the monthly income of the majority was 4000 Ł or less (72.7%), and the education level of most of them was high school, primary and secondary school (80.8%).
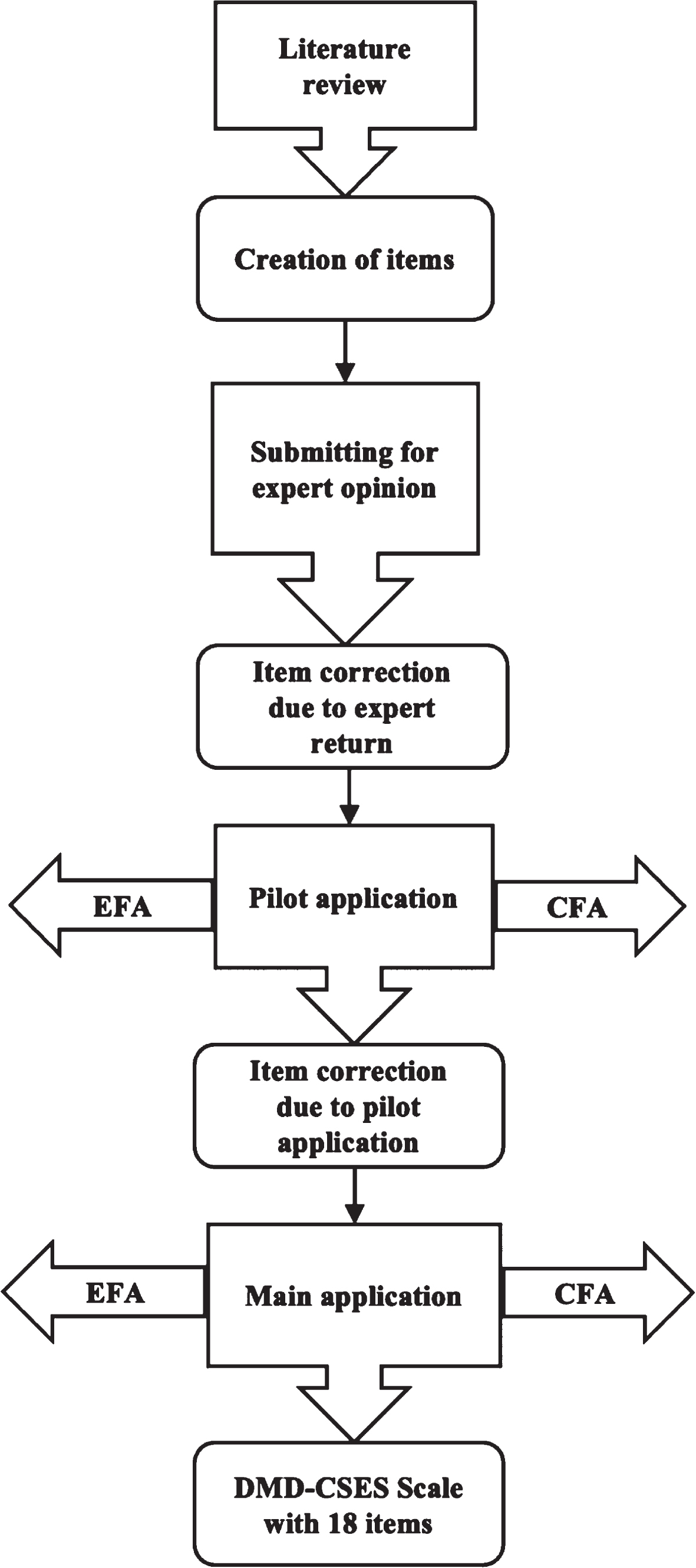
The flow chart of the DMD-CSES scale. The flowchart visualized the process from the beginning to the end of the research. EFA stands for Exploratory Factor Analysis and CFA stands for Confirmatory Factor Analysis.
The item-total correlation coefficient and critical ratio (CR) were used to evaluate the item analysis of the first 20 items of the DMD-CSES scale. An independent t-test was used for the CR analysis of each item. The results of the mean differences ranged from 2.10 to 3.74. The critical ratio was in the range of 6.07 to 17.09 (p < .001). According to the results, there were significant differences between the group with the highest 35% score and the group with the lowest 35% score [13]. Therefore, with this result, the discriminating power of DMD-CSES scale items is seen. Also, item-total correlations vary between 0.63 and 0.89, and the norm for proficiency is over 0.40 [14].
Results
EFA of the DMD-CSES
EFA was conducted using the SPSS 25 package program [15] to determine the factors to which the 18 items in the DMD-CSES scale depend on and the structure of these factors [16]. As a result of the analysis, the Kaiser-Meyer-Olkin Measure of Sampling Adequacy (KMO) value was 0.911 and Bartlett’s Test of Sphericity (BTS) values were also statistically significant, so it was found to be a suitable sample for factor analysis (x2 = 1514.033, df = 190, p < 001).
One of the analyses used to reveal the validity of the measurement tools is EFA. The direction of the relationship and the strength of the relationship between EFA and the items of which the measurement tool is made are revealed.
Considering the relevant results, a variance value above the 40% expected variance was obtained from studies in social sciences.
Since the threshold value for the communities is 0.25 and above, the desired values and better were obtained [17].
According to the EFA results, the DMD-CSES scale exhibited a three-factor structure with 18 items and an eigenvalue above one. The three-factor structure explains 64.82% of the total variance for the DMD-CSES scale. Except for one or two items, all items loaded on at least one factor with a load of.45 and above. Communalities for all items in the scale were over 0.60. For factors with an eigenvalue above one, factor loadings of 0.40 and above are acceptable for social sciences. Therefore, the factor loadings in this study above 0.40 indicate that the study is compatible with the relevant threshold value [13].
It is stated that as many analyses and rotations as possible should be done and developed for the factor analysis to give a fully compatible structure [18]. Thus, two items of the DMD-CSES scale, which originally started with 18 items, were removed and an 18-item, three-factor scale was obtained.
The fourth EFA analysis, which was the last stage, was carried out with 18 items. A three-factor scale with an eigenvalue above one was obtained. These three factors provided 67.64% of the total variance of the scale (see Table 1). Communalities in factor analysis range from 0.57 and 0.80. It is stated that the threshold value of the Cronbach alpha coefficient used for the internal consistency of the measurement tools is 0.70. According to this value, it is seen that the current research has the desired internal consistency [19].
DMD-CSES components of factors and communalities at scale (N = 99)
DMD-CSES components of factors and communalities at scale (N = 99)
Note: h2 = communalities.
EFA analysis was applied to the revised 18-item DMD-CSES scale. The standardized factor loads of the items loaded on the factors vary between 0.58 and 0.81 for the First FACTOR, between 0.56 and 0.73 for the Second FACTOR, and between 0.72 and 0.83 for the Third FACTOR.
Internal consistency analysis was conducted for the revised DMD-CSES Scale and its subscales (see Table 2). Cronbach’s alpha coefficient was used for the internal consistency of the DMD-CSES total scale and its sub-dimensions. Accordingly, the Cronbach’s alpha coefficient of the DMD-CSES total scale was 0.948, and the Cronbach’s alpha coefficient of the three sub-dimensions that make up the DMD-CSES scale ranged from 0.770 to 0.942. The item-total correlation of the factors and the total scale of the (DMD-CSES) scale is above 0.50. Each item having a scale-total correlation value of 0.30 or above was sufficient and the desired values were obtained [20].
Reliability of the last DMD-CSES scale (N = 99)
Reliability of the last DMD-CSES scale (N = 99)
The correlation coefficient between two parts of the DMD-CSES scale, part 1 and part 2, was examined. A strong and statistically significant positive relationship was found between part 1 and part 2 (see Table 3). Concurrent validity scores usually range between 0 and 1: Less than 0.25: small concurrence. 0.25 to 0.50: moderate. 0.50 to 0.75: good. In the present study, a correlation of 0.86 was obtained between the two parts of the scale. This value is better than the desired best level of 0.75 [21].
DMD-CSES relationship between two forms of the scale: split half method (N = 99)
DMD-CSES relationship between two forms of the scale: split half method (N = 99)
Within the scope of the DMD-CSES construct validity, the CFA analysis was conducted in addition to the EFA. The CFA was carried out using the AMOS 23 Software Package [22] to test the structure obtained by the EFA. According to the CFA results conducted for the construct validity of the DMD-CSES, which consists of 18 items and three sub-factors, the goodness-of-fit values of the the model and the acceptable values are presented in Table 4. Table 4 shows that the chi-square (χ2) value was found to be statistically significant (χ2/df = 1.502; p < 0.001). As a result of the CFA, the factor loadings in the first sub-factor of the DMD-CSES, which has a three-factor structure, ranged between 0.70 and 0.86, and factor loadings of the second sub-factor ranged between 0.65 and 0.82, and factor loadings of the third sub-factor ranged between 0.66 and 0.86 (see Fig. 2). The CFA path diagram and factor loadings regarding the scale are presented in Fig. 2.
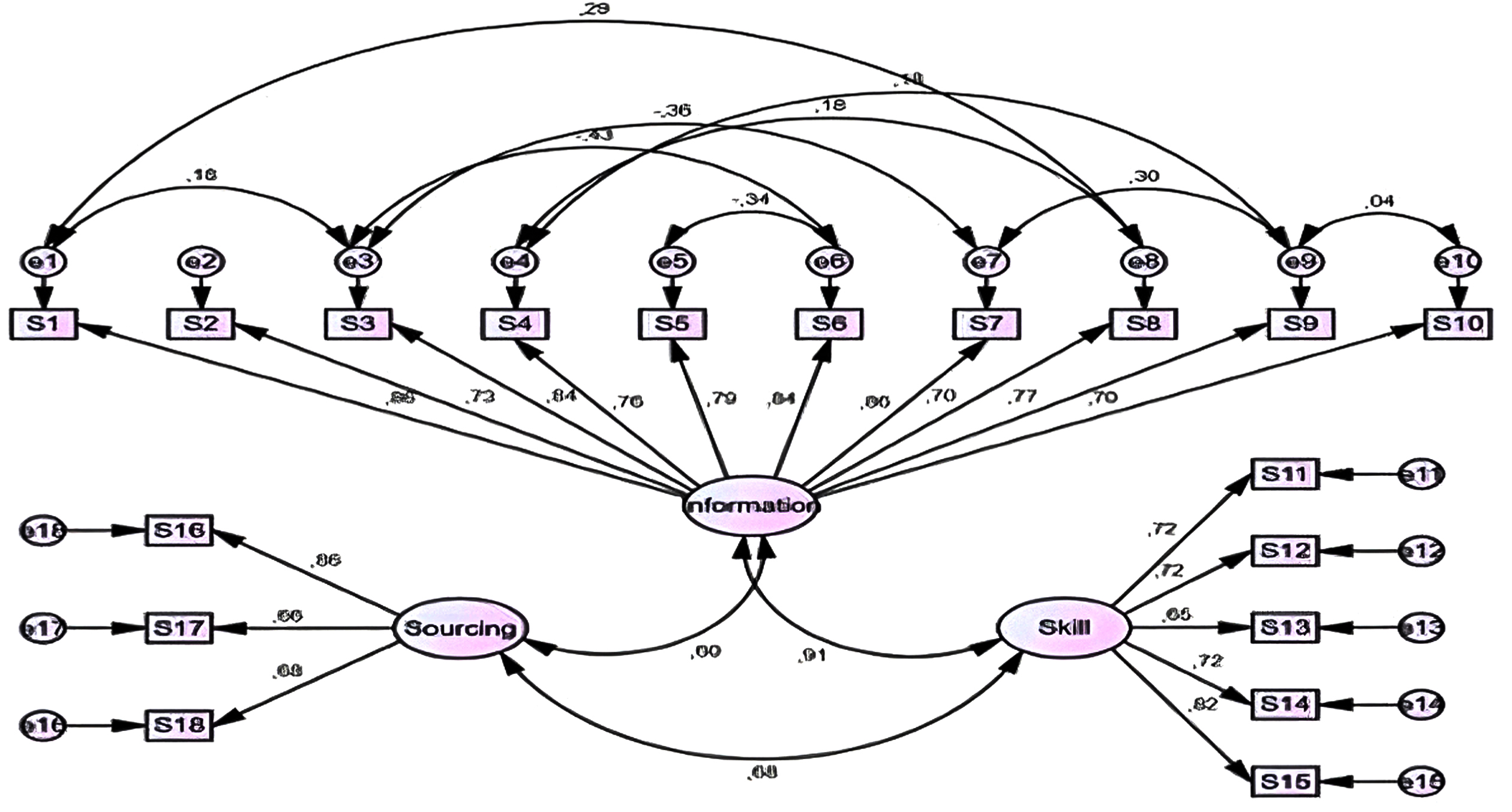
Confirmatory factor analysis path diagram of the DMD-CSES. As a result of the CFA, the factor loadings in the first sub-factor of the DMD-CSES, which has a three-factor structure, ranged between 0.70 and 0.86, factor loadings in the second sub-factor ranged between 0.65 and 0.82, and factor loadings in the third sub-factor ranged between 0.66 and 0.86.
Table 4 shows that the goodness of fit values obtained for the model are above the threshold values except for NFI, GFI and AGFI. The reason why NFI, GFI and AGFI are slightly smaller than the threshold value is due to the small sample size. However, the small population of DMD patients should be seen as a limitation of this study. For this reason, we believe that if some goodness-of-fit values remain below the threshold value, it will not cause a serious problem. Because many authors on CFA analysis state that it is difficult to capture the relevant values in small samples in social sciences, and therefore, an acceptable level of values such as RMSEA, CFI, IFI and TLI is sufficient for model fit [23–27]. The 18-item two-factor DMD-CSES was also confirmed by CFA analysis.
The goodness of fit values obtained as a result of the CFA
RMSEA = Root Mean Square Error of Approximation, GFI = Goodness-of-fit Index, AGFI = Adjusted Goodness-of-fit Index, CFI = Comparative Fit Index, NFI = Normed Fit Index, TLI = Tucker-Lewis Index, IFI = Incremental Fit Index.
Care for DMD patients involves difficult treatment processes. The people who care for these patients also experience wear and tear over time, both physically and mentally. Landfeldt et al. [28] emphasized that caregivers of patients with DMD should be screened for depression. In addition, Reid et al. found that family stress was associated with the patient’s psychosocial adjustment and intellectual function, but not with socio-demographic variables (e.g., age, education, and wheelchair use) [29]. de Moura et al. [11], on the other hand, revealed a lower quality of life and higher burden among people who care for patients with DMD.
In this study, a valid and reliable scale will be developed to help determine the cognition levels of caregivers of DMD patients regarding their competencies. For this purpose, a 20-item draft DMD-CSES scale was developed with the help of a researcher who is an expert in scale development and biostatistics, an expert in neuromuscular diseases and physiotherapy, who studies self-efficacy, and a public health expert. This scale was applied to caregivers of neuromuscular patients at a training and research hospital in Diyarbakır.
Care was taken to ensure that the caregivers included in the study were primary caregivers known to the patient. Care was taken to ensure that these caregivers lived in the same house with the patients. Care was taken to ensure that caregivers were 18 years of age or older and were family members of patients diagnosed with neuromuscular disease, unable to perform self-care and in need of care. As a result of the analyses, a final scale consisting of 18 questions and 3 dimensions was obtained. The sub-dimensions of the scale were named as “Knowledge about Care”, “Skill” and “Finding Resources”. As a result, a valid and reliable scale was obtained with this study to measure the self-efficacy of caregivers of DMD patients.
With this developed measurement tool, it is revealed that the self-efficacy of the caregivers of DMD patients is examined, and the changes and developments needed as a result of this examination and to what extent the training will be sufficient. By revealing these requirements and needs, evidence-based data is provided to policy makers. In this way, it will be possible for policy makers to organize more planned and programmed training series for caregivers of DMD patients. On the other hand, it will be possible to make the necessary improvements for the caregivers of DMD patients.
One point more than half of the average score of DMD caregivers from each subscale indicates that the caregivers have sufficient self-efficacy from that subscale. More than half of the total score obtained from the total scale indicates that the DMD caregiver has self-efficacy in all aspects, provided that the total score obtained from each scale is one point higher than the average. A score from the average of the scale grand total score does not by itself indicate that the self-efficacy criterion is met. However, it can be said that DMD caregivers have self-efficacy if they get one point more than the average score from each sub-scale and one point more than the average overall scale score.
As with any research, the current research has some limitations. These limitations can be listed as follows: Since data are collected only from one region of Turkey, similar results may not be obtained in other regions. The socio-economic status of the participants in the study and the socio-economic status of DMD caregivers in other regions may differ. This situation necessitates further studies. Since the data used in the study are short-term and show instant situations, it is necessary to conduct prospective cohort studies in which longer-term data are collected. Statistical methods used should only be considered one-way, as they cannot compare with caregivers of non-DMDs.
The findings obtained from the study should be interpreted within the framework of the constraints listed above.
Suggestions for further studies to eliminate these constraints are as follows: Comparative studies measuring the self-efficacy of DMD caregivers and non-DMD caregivers are recommended. Long-term prospective cohort studies involving DMD patients, and their caregivers are recommended. It is recommended to perform panel data analyses and apply time series, especially with the data obtained after long-term experiences. It is recommended to conduct similar studies with different methods and methods with caregivers with DMD in different regions and countries.
Conclusion
It can be stated that the study is the first of its kind and, when viewed from this aspect, it is original. It is expected that the study will make an important contribution to the literature in terms of determining the self-efficacy of caregivers who are interested in the care of DMD patients, which are rare and require serious effort. In DMD, it is of utmost importance to maintain upper extremity functions in terms of patient independence and quality of life [30]. Thus, the quality of the care service offered can be increased. It is recommended that the study be carried out with confirmatory factor analysis in different cultures with different samples. Developing a valid and reliable scale to identify the self-efficacy, knowledge, skills and resources of caregivers with a common perspective of physicians and health management team centred on patients with DMD will be effective in practice.
Ethical approval
Ethical approval was obtained from the Dicle University Social and Human Sciences Ethics Committee (approval date and number: 10.06.2021–105).
Informed consent
Informed consent was obtained from all participants.
Conflict of interest
The authors declare that there is no conflict of interest.
Footnotes
Acknowledgments
The authors are grateful to all individuals who participated in the study and reviewers for reviewing this article.
Funding
This study did not receive financial support.
Author contributions
All authors contributed to the study’s conception and design, data collection, data analysis and interpretation, drafting of the manuscript, and critical revision of the manuscript. All authors read and approved the final manuscript.