
Abstract
BACKGROUND:
This scoping review aimed to identify the barriers, facilitators and benefits of returning to work following burn injury, outcome measures used, management strategies, and models of care.
OBJECTIVE:
To provide a comprehensive overview about working-aged adults returning to their preinjury employment after burn injury
METHODS:
We followed a pre-determined scoping review protocol to search MEDLINE, CINAHL, Embase, PsycINFO, PubMed, Scopus, CCRCT and CDSR databases between 2000 to December 2023. Papers reporting primary data from previously employed adults with cutaneous burn injuries were included.
RESULTS:
In all, 90 articles met the review criteria. Return-to-work was both an outcome goal and process of recovery from burn injury. Physical and psychological impairments were identified barriers. Job accommodations and modifications were important for supporting the transition from hospital to workplace. Employment status and quality of life sub-scales were used to measure return-to-work.
CONCLUSIONS:
Consistent definitions of work and measurements of return-to-employment after burn injury are priorities for future research. Longitudinal studies are more likely to capture the complexity of the return-to-employment process, its impact on work participation and changes in employment over time. The social context of work may assist or hinder return-to-work more than physical environmental constraints. Equitable vocational support systems would help address disparities in vocational rehabilitation services available after burn injury.
Keywords
Introduction
Background
Employment is a major life activity, highlighting personal identities, and providing financial resources and social interaction opportunities to participate within the community where a person lives and works. The adverse biopsychological sequelae of burn injury can delay return-to-work, a primary indicator of successful rehabilitation [1, 2], which further restricts maintenance of livelihood and opportunities to seek and secure alternative employment. [3]. Unfortunately, burn hazard exposures are disproportionately high for workforces in lower socioeconomic regions where adequate resources and access to appropriate care are limited. [4–6]. Such challenges can make it difficult to resume work, reintegrate into society, and restore contribution to the economic wellbeing of the families and communities of those injured [1, 7–9].
Support services for return-to-work after burn injury vary from country to country. Across Australia’s major cities, for example, emergency and acute burn care is universally accessible via the specialist burn units located in the public health sector. However, accessibility is limited for those living in non-metropolitan areas while those from rural regions must travel great distances for care. While all individuals with work-related burn injuries are eligible for work rehabilitation services, the same cannot be said for the 80% of Australian adults of working age who sustained their burn injuries outside the workplace [10]. These individuals are more likely to sustain an inhalation burn injury with more than 50% total body surface area (TBSA) impacted [10]. The severity of their injuries is compounded by the fact they are not able to access the same vocational rehabilitation services as those with a work-related burn injury. Therefore, current burn rehabilitation services are underdeveloped and inequitable, forcing individuals with outside-of-work burn injury to navigate complex health and return-to-work systems.
Research and gaps in literature
Barriers to return-to-work are not only associated with physical factors such as scarring, wounds, limited mobility, pain and neurologic deficits (e.g., pruritus, neuropathies), and physical job requirements [11]. Social and environmental factors around where the person lives and engages with their community [12, 13] also act as significant barriers. These factors include the individual’s cognitive abilities, inter and intrapersonal social abilities, their working conditions, access to transport, and psychiatric distress (e.g. anxiety, depression, post-traumatic stress) [11, 15]. Whilst specialist vocational programs such as “In-Voc”, are available for patients with spinal cord injuries [16], the same does not currently exist for patients with non-work-related burn injuries. Further, burn survivors have reported the lack of vocational services during their burn rehabilitation as a barrier to return-to-work [17, 18], indicating potential differences between burn survivors’ lived experience and how or whether burn rehabilitation services overcome individual factors relating to return-to-work barriers.
Current research into return-to-work after burn injury has focused on non-modifiable predictive factors such as burn severity and adverse sequelae [1, 19–21], limiting the ability to adequately address modifiable factors (such as pain, mood disorders or work conditions) to improve burn recovery outcomes [11, 23]. Furthermore, to our knowledge, there are no agreed definitions of what constitutes work, paid versus unpaid work, the types of work, levels of injury, and considerations of the legal ramifications of work-related and non-work-related burn injuries. The lived experience and perceptions of people with burn injury towards returning to work and what is required to facilitate this aspect of burn recovery is unknown [18, 23]. Thus there is an urgent need to investigate how these factors impact return-to-work.
A scoping review of return-to-work after burn injury was chosen to provide a comprehensive overview to map what is known and not known about working-aged adults returning to their preinjury or alternative employment following a burn injury, including work outcomes, barriers, facilitators and benefits to returning to work after burn injury; outcome measures used to quantify/qualify return-to-employment; management strategies and interventions used; and models of care reported to assist with return-to-employment.
Methods
We developed an a priori scoping review protocol [24] using the updated Joanna Briggs Institute (JBI) scoping review methodology [25] based on the first five stages of Arksey and O’Malley’s [26] scoping review framework. The details of the methods for our scoping review protocol have been previously published [24]. Reporting followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) checklist [27] (Appendix A). Iterations to the study criteria were made, as we examined the content and parameters of the evidence base in the context of our research objectives, aligned with updated JBI scoping review methodology [25]. These iterations are reported in the sections that follow.
Information sources
To ensure a comprehensive search as required for a scoping review, we selected MEDLINE, CINAHL, Embase, PsycINFO, PubMed, Scopus, Cochrane Central Register of Controlled Trials and Cochrane Database of Systematic Reviews databases. Identification of existing review papers was undertaken with a preliminary search of Medline and Cochrane Database of Systematic Reviews (CDSR) databases. Three papers [2, 28] were selected to analyse the text words and index terms used in their descriptions and search strategies. The search strategy was designed and tested by the lead author (AK) with the assistance of two research librarians and further refined after discussion with the research team which clarified key concepts relevant to the review question. We compared subject headings in each database’s thesaurus to our key concepts for consistency. The full search strategy is detailed in Supplementary Table S1. The search was conducted on March 17, 2019 and updated August 2021 and December 2023.
Study criteria
The review question was formulated using the “Population, Concept and Context” method. In this review, people with burn injuries were defined as patients who required specialist burn care for a cutaneous burn injury, regardless of injury mechanism or location where injury occurred; at least 18 years old; and in paid work activities for a source of income and not working in a voluntary or home carer capacity (Table 1). While study participants must have had time off work because of their burn injury, no limits were placed on the commencement of time off work, duration of work absence, or intensity, frequency, type, or location of work. This was to allow all considerations of what return-to-work entails to be included as there are no established definitions for return-to-work after burn injury [5]. All types of interventions across all settings and all types of outcome measures were included.
Inclusion and exclusion criteria for scoping review
Inclusion and exclusion criteria for scoping review
aReview papers were not included but the primary research studies reported in them were individually assessed for eligibility. bThese papers were deemed unrelated to return to employment after burn injury. #Further exclusions were applied to refine the study criteria from its first iteration to focus on the research objectives as the initial search yielded greater than 30,000 records after duplicates were removed.
In the absence of clarification in the papers, we assumed papers reporting on return-to-employment after burn injury included participants who were previously employed. We defined employment data as any measurement of rate, proportion or counts of participants in employment or time to return-to-employment. In qualitative studies, such data were often not provided. Instead, thematic, metaphoric, analytic interpretive data with quotable illustrations from participants and fieldwork observations relating to return-to-work after burn injury were featured [29]. We excluded records prior to 2000 as it became evident during screening that return-to-work was not well-established as a concept of recovery from burn injury prior to this time and due to the scarcity of records prior to 2000 on this topic reported by previous reviews [1, 30]. Reference lists of all identified reports and articles were hand-searched for eligible papers. Authors were contacted for further information where required for recent publications (i.e. the last five years).
A reference manager software (Endnote X9, Clarivate Analytics) was used to consolidate and manage duplicates in the results obtained from the different databases. Article selection was based on the PRISMA guidelines [31]. Due to the volume of records, the initial title and abstract screening was conducted by AK and LM with the assistance of two physiotherapy students. Calibration exercises with ten, then another hundred randomly selected records were used to ensure congruency during screening and to ensure the inclusion and exclusion criteria were clear. During the title and abstract screening stage, papers were selected as relevant if they were focused on interventions or outcomes or barriers addressing returning to work after burn injury. Selected articles were retrieved for full-text review. A predefined charting form was used to extract data from the selected papers. Key information charted included citation details (first author’s profession, publication year), study details (study objectives, type of study design, study location, participant settings, demographics, interventions, assessment, and outcome measures used, methods of analysis, study limitations) and conceptual details (definitions of work, quantification of return-to-work, classifications of work). Two researchers (AK, LM) trailed the charting form with a random sample of ten results to ensure reliability and accuracy for recording key information. Where available, discharge destination, length of inpatient rehabilitation stays, pre-existing conditions and post-burn complications were added as additional key information for extraction based on trailing the charting form. Supplementary Table S2 provides definitions used in the scoping review for the charting form. A third researcher (ZT) resolved conflicts when these arose. Full-text papers were retrieved for further review when the ambiguity existed. Data extraction was completed by AK.
Synthesis
Papers were grouped according to study design. Key findings and themes, methods of assessing outcomes, intervention types, and care settings were identified and reported using a descriptive narrative. No critical appraisal was conducted as is typical for scoping reviews [25] as this review’s purpose was to map the evidence base. The International Classification of Disability, Functioning and Health (ICF) framework [32] was used to understand work-related activity and participation limitations from burn injury because of its biopsychosocial focus on health-related disability.
Results
Review sources
Following the initial search, 66 papers met the study criteria. Another 24 papers were included following the updated searches (Fig. 1).
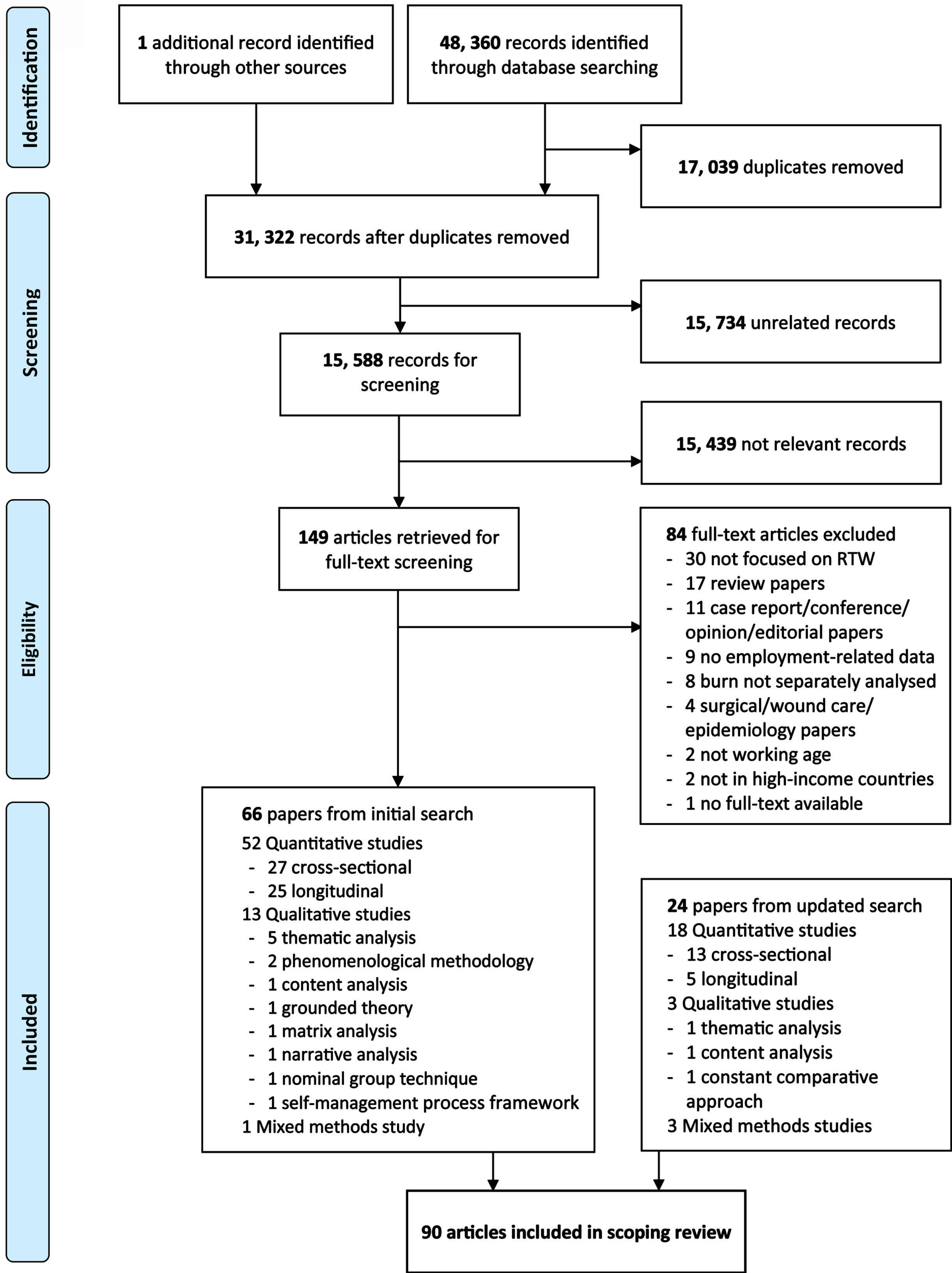
PRISMA study flow chart.
A summary of study characteristics is provided in Table 2. The majority of the 90 included papers had a quantitative design (78%, n = 70), with 18% (n = 16) having a qualitative design and 4% (n = 4) a mixed methods design. The number of published peer-reviewed papers related to return-to-work after burn injury more than doubled between 2000–2009 and 2010–2023 (Fig. 2). While qualitative papers were still less frequently published, their numbers increased in the 2010–2023 period compared to the preceding decade. Most studies (56%) recruited participants from a burn center after they had treatment there. Less than 1% of the participants (i.e. 271 participants) were recruited from a rehabilitation setting. Of the studies reporting mean time from burn to time of the study, this ranged from 1 to 3 weeks [33] to 16.2 years [34]. Of the 43% (n = 30) of longitudinal studies, three time points were the most common for measurement of outcomes (n = 11, 37%), where 6 months (53% n = 16), 12 months (53% n = 16), and 24 months post-burn (27% n = 8). A detailed table of study characteristics for the 90 papers is provided in Supplementary Table S3.
Overall summary of included papers
Overall summary of included papers
Country (where study was undertaken); asome papers used more than one type of data collection method; italicized font refers to number of participants; regular font refers to number of included papers.

Types of published empirical papers regarding return-to-work after burn injury.
A summary of participant characteristics across the study types is listed in Table 3. There were fewer female participants than males across all study types and males were greatly over-represented in working aged adults with burn injuries. Some papers reported on ethnicity, marital status, education and income but few papers reported on income (e.g. yearly wage [4, 35], level of socioeconomic disadvantage [36–38], expenditure over income [39]). Pre-existing mental health problems were reported more frequently (24%, n = 17) than pre-existing physical health problems (21%, n = 15), while six papers (7%) reported co-morbidities but did not define them [11, 40–43]. More studies since 2010 reported on psychological or psychiatric conditions including alcohol and/or substance misuse disorders [37, 44–50] than in or prior to 2010. Pre-existing mental health conditions or disorders were reported to be present in as few as 3% of the study participants (psychiatric history [7]) to as many as 59% [47]. Self-reported alcohol misuse ranged between 11% [51] to 23% [12], self-reported drug misuse in the 12 months preceding burn injury from 5% [50] to 15% [12, 46]; and substance use between 2% [45] and 30% [48, 49].
Summary of reported participant characteristics
Summary of reported participant characteristics
Notes: mean (average of available means reported); range (range of available means reported); no. of papers that reported data (number of papers with data reported for whole study sample and comparable to other papers); adata not aggregated due to large variety of descriptors between papers; bmental health-related conditions (papers reporting at least one of the following conditions: any lifetime psychiatric disorder, previous psychiatric treatment/history; previous psychological treatment); cphysical health-related &/or medical comorbidities (papers reporting at least one of the following: pre-existing health concerns, co-morbidities, co-existing conditions, chronic diseases (obesity, cardiac disease, diabetes mellitus, hypertension), smoking, chronic pain, non-burn illness, neurological impairments, acquired brain impairments/stroke, other medical problems); dPsychiatric diagnosis (papers reporting at least one of the following conditions: psychological symptoms, post-traumatic stress disorder, anxiety, major depression and other mood disorders); eother complications (papers reporting at least one of the following conditions: visual impairments, musculoskeletal symptoms, pain, physical and mental trauma, impaired mobility, AROM deficits, open wounds, other medical problems, heterotopic ossification, complex/multiple trauma, concomitant/associated trauma, compartment syndrome, involved in litigation); f[85] reported mean and [70] reported median; % TBSA (percentage of total body surface area); % TBSA-FTB (percentage of total body surface area with full-thickness burn); LOS-H (length of stay in acute hospital); LOS-R (length of stay in rehabilitation hospital).Italicized font refers to number of participants; regular font refers to number of included papers.
Flame burns were more common amongst all participants and the range of burn size was 4–61% TBSA (Table 3). There was a high proportion of participants with visible (face and hand) burns. Two papers on hand burns used alternative measurement systems –mean total surface area in cm2 [52] and median Modified Hand Injury Severity Score [53]. Only four (all quantitative) papers reported mean length of stay (LOS) in inpatient rehabilitation [12, 54–56], which ranged from one day [12] to 184 days [55]. Where relevant discharge destination was only reported in 13% of papers (n = 12) [14, 57–63]. Mean time since burn injury was just over 6 years with maximum of 17 years but the minimum time since burn injury ranged from 1–3 weeks [33] to less than four months [64].
Using the ICF [32] framework, most burn-related complications (for example, pain, post-traumatic stress disorder and itch) mapped to the body structure and functions component (Table 4). Some activity and participation limitations were also reported, such as problems with hand function [65, 66], no enjoyment engaging with others [67] and socialization problems at work [11, 68]; and environmental factors such as employers’ and health professionals’ knowledge gaps [17, 68–70] and financial difficulties caused by burn injury [68, 72]. Post-traumatic stress disorder was the most commonly reported mental health condition post-burn [14, 73–76]; followed by depressive disorders [11, 76], including major depressive disorder [48–50, 75]; and anxiety disorders [14, 74–76].The prevalence of post-traumatic stress disorder reported ranged from 2% [58] to 55% [76]. Psychiatric diagnoses occurred in 19% of work-related burn injuries [4], and neuropsychiatric sequelae were reported by over 80% of individuals with electrical burn injuries [61]. Psychiatric problems such as insomnia, depression, post-traumatic stress, anxiety, body image/deformity, and drug and alcohol dependence affected participants’ return-to-work post-burn [14]. Everyday pain was reported by 30% of individuals with burn injuries 4.6 years post-burn [48, 77], which was similar to 32% of individuals with chronic pain [76] and 38% neuropathic pain [74] in individuals with electrical burn injuries (time since burn not reported in these electrical injuries papers). Burn-related cognitive impairments such as memory loss, poor concentration, and problem-solving difficulties [11, 78] were rarely reported and almost exclusively by papers on electrical burns involving the skin.
Burn-related complications reported using ICF framework
ICF: International Classification of Functioning, Disability and Health; RTW: return-to-work.
Pre-burn employment was reported in 67% (n = 58) of papers, ranging from 37 to 100% of participants (Table 5). Amongst the 15 papers (17%) on work-related burn injury [4, 79–87], one third (n = 5, 33%) focused on electrical injuries [73, 87] and one third (n = 5, 33%) investigated return to duty outcomes for military service members with combat-related burn injuries [59, 85]. The percentage of participants with work-related burns ranged from 13 to 64%, which were more common in those with electrical injuries [35, 74] and hot press hand burn mechanisms [52]; and amongst firefighters [69], ranged from 74–96%. Only 20% of papers (n = 18) described participants’ jobs/occupation type and/or industry, mainly using non-standardized occupation classifications [17, 86–93]. Work hours, job type, industry type, time on job pre-burn, employer size, satisfaction with work/employer before burn, time on job and reasons for not working before burn were rarely reported.
Overview of employment-related data reported
aData not aggregated due to large variety of descriptors between papers; italicized font refers to number of participants; regular font refers to number of included papers.
Most papers (n = 71, 79%) reported post-burn employment rates. There was a large variety of descriptors of post-burn employment tenure amongst included papers, which demonstrated attempts to capture changes to work capacity and job situation. Papers most frequently reported participants returned to the same job as before burn injury (n = 17, 20%) [13, 95], or returned to their job with modifications (n = 18, 21%) [11, 95], for example, modified work tasks and flexible work schedules. Change to work capacity was demonstrated by measuring the proportion of participants who returned to work part/full-time [47, 95], without specific limitations [59], or full duty/less than full duty [79]. Burn survivors reported changes to their employment situations post-burn that included changing jobs, employers, or industries [11, 94]. Some changed to “better jobs” than pre-burn [34, 96], or “worse or less skilled jobs” than pre-burn [13, 82]. Others received re-education [34, 85] or new jobs after retraining [71], had job changes/difficulties because of burn [42, 90], or retirement because of burn [52, 80]. Job accommodations/modifications, sick leave, significant person’s employment or time off work, presence of job difficulties, satisfaction with return-to-work, reasons for not returning to work, employer/co-worker contact during hospitalization, job or employer changes, and income reduction were all rarely reported.
Rate of return-to-employment
Between 13% [39] and 81% [53] of participants returned to their same pre-burn job. This rate was high (60%) even after work-related electrical burn injuries [61]. Post-burn employment ranged from 26% [55] to 92% [37] in the longitudinal follow-up studies. Employment status was most frequently reported at 12 months post-burn [11, 97]. Among the papers reporting post-burn employment rates across time, cumulative rates of return-to-employment increased over time when measured at least twice at any time point during the study period (Table 6) [7, 98]. More participants returned to work in the first six months post-burn and longitudinal studies showed a declining proportion of participants who returned to work after 6 to 12 months and 1 to 2 years post-burn [11, 72]. Regarding this decline, no further details were reported on work participation, which made it difficult to understand if this decline was because the people had returned to work early post-burn but then did not continue that work.
Comparison of pre-burn and post-burn employment rates reported
Comparison of pre-burn and post-burn employment rates reported
Only papers which reported both pre and post-burn employment rates included in this table. SSG: split-thickness skin graft; BiobraneTM: artificial skin substitute; conservative: conservative treatment without surgical intervention; BI: burn injury; post-burn employment rates expressed using the paper’s reported % employed pre-burn as denominator; aChapman 2008a [80] and Chapman 2008b [81] are the same study; bÖster 2011 [48] and Öster 2013 [49] are the same study; cKlein 2007 [60] included N = 2880 enrolled but only n = 828 with follow-up data available; dStergiou-Kita 2014a [86], Stergiou-Kita 2014b [87] and Mansfield 2014 [84] are the same study; epre-burn employment rates included attending school or work; fat >12 months.
The average time to return-to-work ranged from 24 days [79] to 51 weeks [99] with a mean of 143.1 days. When we examined papers reporting time to return-to-employment, % TBSA burn size and hospital length of stay (LOS) [7, 99], the length of time taken to return-to-employment extended with increasing % TBSA and hospital LOS (Fig. 3). Within this small series of papers, studies on electrical burn injuries [35, 61] reported longer time to return-to-employment than the non-electrical burn injury papers [7, 99]. Some papers measured time from hospital discharge to time to return-to-work (e.g. [11, 13]) or time loss from but time to return-to-work was most often measured as the time from injury to time to return-to-employment [37, 99].

Injury-related factors were the most frequently investigated influences on time to return-to-employment. Time to return-to-employment was associated with burn severity (total burn size [7, 47], total full-thickness burn size [47]), hospital LOS [11, 47], bilateral hand burns [13], hand burn severity [53], depth of hand burn [100], burn to trunk [13], personality disorder [47], and work injury [47]. There were mixed findings regarding whether some of these injury-related variables affected time to return-to-employment after burn injury. For example, Öster and Ekselius [47] reported injury-related variables burn size, full-thickness burn size, LOS and work injury were related to a longer time to return-to-work [47] and a longer hospital LOS delayed the timing of return-to-employment [11, 13] where a one-day increment in hospitalization was associated with a 7% decrease in the odds ratio of returning to work within 12 months [13]. In contrast, Esselman [11] reported neither TBSA nor hospital LOS delayed return-to-work after hospital discharge. Time to return-to-employment was not associated with sociodemographic variables [47], work-related variables [47] or employee concerns [11] but was a significant predictor of non-return-to-work post-burn in one study [101].
Absence from work because of burn injury was reported as sick leave [47, 75], time loss from work [4, 42], time off work [35, 62], and absence from work [37]. Sickness absence was also measured by loss of productivity [42], including partners’ productivity losses [37]. Individuals who had returned to work were significantly more likely to have had sick leave shorter than six months while those who had not returned to work were more likely to have longer work absence [75, 101]. Sickness absenteeism, when reported in the included papers, examined the impact of sickness absenteeism and predictors of sickness absenteeism (Table 7).
Summary of sickness absenteeism (SA) reported in included papers
Summary of sickness absenteeism (SA) reported in included papers
aAt 3 months post-burn; TBSA (total body surface area).
Of the 72 outcome measures used (Table 8), half pertained to the Body Structures and Functions component of the ICF. Most outcome measures were not employment-focused or specific to measuring return-to-work ability, capacity or desirability. Most papers used subscales or subdomains within generic outcome measures (e.g. Sickness Impact Profile work and recreation scale [102]) or burn-specific outcome measures (e.g. Burn Specific Health Scale –Brief (BSHS-B) [103], Life Impact Burn Recovery Evaluation Profile [104]). Employment-related data such as employment status (e.g. at time of burn and/or time of study post-burn), work capacity (e.g. return-to-work full-time/part-time), job duties (e.g. same job, changed job), or employer conditions (same, different) were also used to describe study outcomes [13, 76]. While 36 per cent of papers (n = 31) reported on work-related functioning or outcomes following interventions, only three papers directly measured employment [11, 42], with Spronk [42] most recently investigating associations between activity impairment, work status and productivity losses using the Work Productivity and Activity Impairment General Health (WPAI-GH) questionnaire [105] and burn-specific health-related quality of life. Assessments and outcome measures (e.g., Modified Hand Injury Severity Scale [53], Burn Scar Contracture Severity Scale [64], American Medical Association Impairment Rating Scale (5th edition) and the Disabilities of the Arm, Shoulder and Hand [81]) were also used to predict return-to-employment after burn injury.
List of assessment tools and outcome measures reported
List of assessment tools and outcome measures reported
[51, 60] only described what outcome measures were used but did not report results of the outcome measures; ICF: International Classification of Functioning, Disability and Health [32].
None of the five papers reporting on interventions, management strategies, and models of care to assist return-to-employment evaluated their success (or otherwise) using robust study designs such as randomized controlled trials. One intervention study included in the scoping review described an educational tool comprising of digital videos accompanied by discussion with an occupational therapist to answer questions and discuss specific work tasks and potential modifications or adaptations [93]. A graded reintegration treatment approach for the work and social setting was briefly mentioned [71]. Kucan et. al. [83] reported on a systematic case management model designed for workers with work-related catastrophic burn injuries in a compensable setting and compared outcomes against standard care. Björnhagen et. al. [57] described the key components of a general (non-burn specific) medical-vocational rehabilitation program using occupational and physical therapy interventions for patients with burn injury and examined this program’s effect on participants’ direct employment outcomes. Carrougher [79] described the vocational rehabilitation program provided by a burn center as embedded within its outpatient burn service but did not investigate how their program influenced employment outcomes of their participants.
Only a few papers specifically reported on the context of vocational rehabilitation programs, all of which were embedded in healthcare services, not workplaces including: a specialist burn center outpatient clinic for compensable patients [79], a general rehabilitation hospital setting [57], a work-related burn injury treatment in a specialized rehabilitation center [71], and a specialist burn rehabilitation service with a general rehabilitation center [61, 76]. Funding for such services was mostly through workers compensation insurance [76, 83]. Reporting availability of financial assistance benefits for wage replacement either in an injury compensation model [79] or within a non-fault social system [57] was rare and only one paper reported availability of education support for changing jobs through military benefits [85].
Barriers and facilitators of return-to-employment after burn injury
Barriers and facilitators of returning to work were identified through means of study-specific questionnaires [11, 69], selected demographic or injury characteristics based on previous literature findings [12, 101], clinical record audits [14], hypothesis-testing [13, 44], and qualitative interview or free-text data [18, 106]. Using the ICF framework, factors influencing return-to-employment are listed in detail in Supplementary Table S4. Barriers commonly reported related to the body structure and function component included pre-burn mental health conditions [7, 75] and post-burn psychological [4, 94] or physical impairments [11, 95]. Scarring, pain, heat intolerance in the work environment, loss of muscle endurance, wounds/infection, and decreased mobility due to pain or scar formation affected ability to return-to-work [18, 91]. In addition to the negative impact of burn-related impairments on work performance [17, 107] and re-integration back to the workplace [18, 94], burn survivors also reported the impact of the burn injury itself affected their work identity [17, 107]. Environmental factors such as attitudes or assistance from employers and co-workers [18, 93] could be a barrier when they were negative towards the burn survivor [66, 93], but positive when they were perceived as supportive towards burn survivors returning to previous employment [18, 94]. Burn survivors also reported rehabilitation services did not adequately address employment-related needs [17, 91] and the lack of experience or knowledge of burn-specific recovery needs amongst healthcare providers as barriers to their return-to-employment [65, 86]. Distance from burn treatment centre did not influence employment post-burn or time to return-to-work [97].
A key facilitator of return-to-work was the availability of work accommodations such as progressive return-to-work programs, task modifications, and flexible work schedules [33, 93]. Practical assistance and psychological support from family helped burn survivors’ return-to-work [18, 107]. Peer support helped burn survivors reframe their work expectations which in turn facilitated their return-to-employment [18, 93]. Additionally, burn survivors from countries with social welfare benefits, compensation or insurance schemes reported assistance in the form of financial support, healthcare services or vocational assistance aided their return-to-work [57, 93]. Personal factors such as adaptability [18, 107], being motivated [17, 91], positive thinking [18, 94], and being persistent and proactive [17, 91] were reported to be helpful in facilitating return-to-employment. However, the long period of recovery [18, 108] and older age at time of burn injury [44, 82] were barriers to return-to-employment.
Benefits of returning to employment post-burn
Return-to-work was seen as a marker of normality [33] and regarded by both burn survivors and burn care professionals as an indicator of overall recovery [33, 106]. Being able to work again was acknowledged as important for self-esteem [18], self-worth [93], and regarded as a “real” measure of progress in recovery by both burn survivors and healthcare professionals [70, 106]. Furthermore, working provided distraction from pain [18, 91] and an opportunity to use physically demanding tasks for therapeutic benefit [91]. As burn survivors regained their capacity to resume daily routines [91], they valued being back at work more than staying at home as working enabled them to re-engage with society and feel useful [93]. Employers reported cost containment, improved worker recovery, re-establishment of productivity and prevention of secondary disabilities as the benefits of early return-to-work for electrical workers [92].
Burn survivors who returned to work after burn injury reported better injury-related physical and psychological health, as well as overall quality of life than those who had not returned to work post-burn [82, 101]. Burn survivors who returned-to-work also reported higher scores in work-related domains of burn-specific quality of life outcome measures [34, 101], higher social participation [109], and less activity impairment and work productivity loss [42].
Participation in work after burn injury was reported by participants as providing meaning and structure to daily life [91], financial benefits for the individual as well as their families [91, 94], and opportunities for social interaction and support [91]. Burn survivors valued work which utilized previous skills and work experience as it provided greater meaning to their progressive return-to-work programs [85, 93]. The desire to return-to-work, even in a limited capacity or in alternate ways, provided them with opportunities for post-traumatic growth and exploring ways to continue living a fulfilling life [85, 107]. Burn survivors used reframing the meaning and value of work to come to terms with how they lived with burn injury [18, 107]. This was reported to facilitate greater understanding of their bodies, abilities and personal values [33, 107].
Discussion
This review incorporated all study designs and sought to understand return-to-employment after burn injury broadly compared to prior reviews. Return-to-employment was valued by both burn survivors and healthcare professionals as an indicator of recovery and regarded as both a measure of burn injury outcome as well as a recovery process. This is similar to how patients with other types of physical trauma, their families and clinicians view return-to-work after injury [110]. Previous reviews have primarily focused on burn injury factors, treatment variables, and barriers to return-to-employment [1, 7]. These reviews were largely limited to cross-sectional studies investigating burn injury and treatment variables where the focus has been on quality of life with work as a sub-domain of quality of life rather than return-to-employment itself as an outcome of burn recovery [1, 5].
Personal attributes are recognized in the broader return-to-work literature for how they affect post-injury employment outcomes [111–113]. The influence of personal attributes such as age, gender, income and education on return-to-employment after burn injury is only beginning to be explored [44]. Although females reported more fatigue [36], greater work disability [50] and work interference [89] post-burn than males, there was limited investigation regarding how these outcomes accentuate the precarious working conditions and types of employment females typically undertake [114]. We found insufficient information from the included papers to determine the influence of gender on return-to-employment outcomes within our study’s research objectives. Gender was excluded as a predictor of employment outcomes or barrier to return-to-work in some papers (e.g. [14, 101]) whereas other papers report females as having higher odds of unemployment post-burn (e.g. [42, 54]). Interestingly, Levi et al [115] reported that despite higher rates of burns to “critical” areas (face, hands and genitalia) in males, it was females in their study population who reported significantly lower scores in the areas of in work and employment, and social interactions with others. They found no gender differences in social activities or relationships with family and friends, both of which measure perceptions of ability to accomplish activities and ability to participate with others in these activities. Thus, while gender differences in employment may be similar to the general population, females may have different employment outcomes compared to males because of how visible burn injuries affect them differently to males [115].
Considerations of how personal attributes and socioeconomic factors influence return-to-employment is important as burn survivors will vary in their motivation and personal resilience, which will affect their ability to participate in the return-to-work process, as with other major trauma and injury groups [116, 117]. The few vocational rehabilitation services reported were primarily funded by workers compensation insurance, which makes these services available only for those injured at work. This raises the question of how previously employed adults with non-compensable burn injuries access vocational rehabilitation services to assist their return-to-work.
A biopsychosocial approach to burn recovery has developed over time with the evidence base moving away from a biomedical model focused on burn injury sequelae. Pre-existing and burn-related physical and psychological impairments are generally understood to be barriers to return-to-employment [4, 101]. Personal, workplace and environmental factors are also of importance, but it is less clear how they influence the different stages of the return-to-employment process [1, 118]. It may be difficult to understand the associations and potential interactions between these factors and return-to-employment after burn injury without a clear framework to guide analysis. Incorporating the ICF (a biopsychosocial framework) to structure the findings from this scoping review, has extended our understanding of: factors influencing return-to-employment in the context of the individual’s personal and environmental circumstances; gaps in knowledge; and future research priorities for interventions [113]. Not being able to participate in employment is considered a limitation to a major life activity in the ICF [32]. However, the ability to participate in employment activities was not critically considered in the included papers. Only one instance of fitness to work was discussed [73], which highlighted how ability to participate in employment activities may be regarded differently by clinicians and burn survivors. The few employment-specific outcome measures used in the included papers demonstrated the heavy reliance on proxy measures (i.e., work-related sub-scales within burn-related quality of life measures) in the current literature.
How employment was measured
Similar with a previous review, the difficulty of synthesizing results from the included papers was largely due to the wide range of descriptors used to report employment outcomes [1]. Clear definitions of work were often missing and it was necessary to include all variations of return-to-employment regardless of employment tenure, work capacity or employer to examine the breadth of the evidence base comprehensively. It was difficult to compare results of the work-related subscales within different outcome measures assessing quality of life, social integration or hand function (e.g. BSHS-B, LIBRE, SIP) because they differ in their content and psychometric properties [103, 119].
Employment rates after injury reported in the longitudinal studies included in this scoping review were highest in the first six months post-burn and were similar to employment trends after other major trauma where most people return-to-employment in the first 6–12 months post-injury [116]. However, both burn and non-burn trauma literature highlight the issue of sustainable return-to-employment, that is, staying employed in the long term [5, 116]. Work participation rates can fall in the long-term even if rates of return-to-work increase over time [116]. Such changes were not found in our review but this is likely related to the shorter periods of study follow-up and also because even longitudinal studies that had surveyed participants more than five years after burn injury did not measure changes in employment rates over time in their study cohorts. Collectively, the above-mentioned methods of defining and measuring employment often miss the nuances of the return-to-employment process. Establishing shared understanding of key terms in describing and measuring return-to-employment is essential for future research and practice [120]. Quantification of employment (e.g. number of people who returned to full/part-time employment, retired because of burn, retrained to other job) and qualification (e.g. working conditions, job duties, modifications/accommodations required) of work participation after burn injury is required so that employment needs and vocational assistance can be clearly assessed for interventions to be appropriately provided.
Impact of the complexity of recovery from burn injury on work participation
Recovery from burn injury is long and complex. The papers reviewed had outlined a range of barriers to returning to employment after burn injury –namely pain, itch, mood disorders, need for work accommodations, practical and social support during return-to-work while still requiring treatment. These barriers are all modifiable and require a coordinated approach to facilitate returning to work after burn injury. The time lag between burn injury and the onset, recognition and diagnosis of psychological symptoms and physical impairments requires burn injury management to extend beyond the acute and initial post-acute hospital setting. Identifying the more severe burn injuries and scarring as chronic conditions with complex multi-system secondary complications instead of an acute injury could aid in understanding long-term management requirements [121]. Recovery from burn injury requires long-term adjustment and the temporal effect on the return-to-employment process bears similarities with those of spinal cord injury [122].
It was clear from our findings that environmental factors such as attitudes towards visible and non-visible burn injury, personal and employer/co-worker expectations of work capacity post-burn, availability of financial supports; also influence return-to-employment. Other groups with traumatic injuries also face similar challenges to returning to work after injury [111]. Understanding the interaction between injury and employment is part of the complexity of recovery from burn injury influencing return-to-employment. For example, return-to-work was impaired and worsened burn-related psychological trauma when burn specialist healthcare professionals did not provide psychological support or information on care plans, or were perceived to lack an understanding of pain or were inflexible with care needs [18, 91]. Furthermore, non-burn specialist healthcare professionals in primary care, outpatient and rehabilitation settings; insurance providers and employers/co-workers need greater understanding of the impact of the gap in psychological care post-burn as an important barrier to recovery affecting work participation after burn injury. To address this key issue, a recovery-focused approach to return-to-work may be beneficial as service providers (healthcare professionals, insurance providers or employers), can incorporate what burn survivors and their families regard as important recovery needs into their provision of services and interventions. Recovery-focused approaches are well-established in mental health care [123] and to a lesser extent in physical trauma care [110] and aim to meet the needs of the individual to participate in meaningful life activities and beyond symptom reduction and focus on impairments.
If, as we found, burn survivors from different high-income countries indicated their need for vocationally-focused rehabilitation services and supports to accommodate their transition from rehabilitation to the workplace, then it would seem such services and supports to assist return-to-work are universally required for working-aged adults who plan to return-to-work after their burn injury, regardless of whether their injury was work-related or not. Additionally, we also found even within high-income countries, cultural differences between healthcare services, social welfare benefits, injury compensation and work legislation affected return-to-employment after burn. This raises another important consideration regarding the differences between work-related and non-work-related burn injury. A comprehensive vocational evaluation is necessary to facilitate return-to-employment and evidence-based guidelines for this has been published [118]. However, such recommendations need the support of an equitable vocational support system, especially for those who were not injured at work or lack access to compensation or benefits. This would require considerable investment for funding but has the potential to increase economic productivity in those who would otherwise remain in need of long-term financial support.
Implications for burn care and rehabilitation services
Rehabilitation services need to develop programs to specifically address work participation after burn injury early in the recovery journey [90]. These programs should be based on understanding burn-related complications, barriers, and facilitators of return-to-employment. Identification of individualized work accommodations, key stakeholders, education needs, communication pathways, and support requirements were clearly identified as facilitating the return-to-work process and should form the basis of such programs. Return-to-employment most likely needs to be staged or graduated, which may initially be at lower capacity than preinjury, with several attempts at returning to employment. Services need to provide individualized interventions to address information and communication needs for both the burn survivor and their employer, including adjustments to feelings of vulnerability and new body identity because of bodily sensations arising from burn scarring interfering with work. Burn survivors highly valued peer support as a key resource to help them reframe and explore new meanings to work participation, understand readiness for work, and advocate for support but there are no burn-specific programs utilizing this valuable resource in the workplace setting to the authors’ knowledge. Additionally, there are multiple other strategies healthcare professionals can provide to support the return-to-work process –offering timely re-evaluations of work capacity as burn survivors adjust to changes caused by burn-related impairments; providing assistance to navigate health, employment or insurance systems; and facilitating consistency of psychological care throughout the continuum of care especially when there are signs of post-traumatic stress, anxiety and depression. Lastly, burn rehabilitation services can also address limitations in the activities of employment, driving or social interaction so as to improve burn injury recovery outcomes in a more comprehensive and occupationally fulfilling manner.
Directions for future research
Consensus on measurement of return-to-employment is required. Without this, future research will continue to lack consistency in the qualification and quantification of return-to-employment. We suggest future research using biopsychosocial or recovery-focused approaches to provide a more in-depth understanding of factors influencing the return-to-employment process after burn injury as they are presently not well-understood including: motivation to return-to-employment; volitional factors and interpersonal stressors related to burn survivors, family, co-workers, employers, and healthcare professional perspectives; the timing and type of vocational assistance and supports; and cognitive impairments especially in non-electrical burn injuries; and personal attributes and socioeconomic factors. A biopsychosocial model provides a better means of understanding gaps in knowledge in the field than a biomedical model to improve work ability and reduce work disability [124]. A recovery-focused approach would further advance burn care in a manner that is inclusive and enabling participation in meaningful life activities.
Given the complexity of navigating the return-to-work process raised in the qualitative studies in this review, the need for case management, care coordination or navigation may not be appreciated and is something burn survivors have raised as a key concern in managing the transition from hospital to the workplace. It is likely the return-to-work process is non-linear and perhaps even cyclical, as burn survivors who require further treatment for long-term complications such as burn scarring or contractures may have interruptions to their work after initially returning to employment after injury. Future qualitative studies could investigate how pre-burn employment facilitates post-burn employment; as well as investigating how different occupations may also present unique challenges in of themselves, for example, whether because they are inherently more hazardous or psychologically more demanding. While this scoping review focused on return-to-employment in high income countries, future return-to-employment research is also needed in low to middle income countries where there is a higher burden of burn injury globally [125]. Lastly, exploration of personal attributes influencing employment, power dynamics, and occupational transitions and grieving such as gender differences and lifestyle changes; could inform the development of appropriate services and policies to support resuming employment after burn injury.
Limitations of this review
While this scoping review was comprehensive and followed the recommended PRISMA guidelines, employment per se is a difficult to summarize, multi-faceted concept, which meant making specific recommendations for future practice difficult. In the absence of a consensus definition of return-to-work within the reviewed papers, we developed our own definition. We only included papers that reported primary employment data which would have omitted papers that examined return-to-work but did not report employment data in its findings (for example, [126]). Few papers addressed vocationally-focused rehabilitation programs, interventions and management strategies despite being included in the review’s search strategy. Health consumers, who may have a different interpretation of the findings were not involved in this scoping review. Despite these methodological limitations, all the investigators had a health background with two investigators (AK, ZT) having specialist clinical and research burn experience and others (LM, MM) having expertise in return-to-employment in rehabilitation populations that likely enhanced the quality and rigor of this scoping review.
Conclusion
The large number of papers included in the results of this scoping review underpins the breadth of this topic. The defining of work and return-to-work are priorities for future research. This scoping review identified return-to-employment as not always dependent on the burn injury itself. Environmental and personal factors influencing the individual’s work participation after burn injury need to be considered when providing vocational assistance and support. This aligns with a shift from focusing on symptoms and impairments towards a more biopsychosocial and recovery-focused approach to understand return-to-employment after burn injury.
Ethical considerations
This study, as a scoping review, is exempt from Institutional Review Board approval.
Informed consent
Not applicable.
Conflicts of interest
The authors declare no conflicts of interest.
Footnotes
Acknowledgments
The authors thank Junze Chen and Sin Koon Nink, Harry for their assistance with record screen-ing. The authors acknowledge Elaine Tam and Yulia Ulyannikova, academic liaison librarians at The University of Sydney for their technical assistance with developing the search strategy. AK would like to thank Bonnie Cheng, hospital librarian at the Douglas Piper Library, Royal North Shore Hospital for providing database training.
Funding
This work was partly supported by a joint grant from The University of Sydney and Northern Sydney Local Health District Allied Health Kickstarter Grant. All opinions and conclusions expressed are attributed to the authors only and not the funding bodies. JME is supported by the National Institute of Child Health and Human Development/National Centre for Medical Rehabilitation Research under award number R01HD079076. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Supplementary Table S1: Full search strategy; Supplementary Table S2: Definitions of charting form categories; Supplementary Table S3: Full study characteristics of all 87 included papers; Supplementary Table S4: Barriers and facilitators to return-to-employment after burn injury reported; Appendix A: Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Checklist.