
Abstract
BACKGROUND:
To carry out their victim rescue and fire-fighting missions, firefighters perform high levels of physical exertion and among them strenuous muscular activity. A specific mental preparation protocol that could induce better strength performance throughout their 24-hour schedule is a major issue for firefighters.
OBJECTIVE:
This case report aims to examine whether a 6-minute Intervention combining mental imagery practices and breathing exercises, specifically designed to be used while travelling between the fire station and the mission site, would be able to promote maximum strength performance.
METHODS:
A series of three Single Case Experimental Designs (SCED) was conducted in single blind design to investigate the effects of repeated challenge-withdrawals between the Intervention and the Baseline on the maximum voluntary isometric contraction (MVIC) strength of the hand-grip.
RESULTS:
Data analyses revealed that 62.5% to 100% of the hand-grip strength values during the Intervention periods were greater than or equal to the maximum data point recorded in the Baseline periods. The effect sizes of these highlighted increases of the hand-grip strength performance revealed by the percentage of non-overlapping data (PND) were 75% i.e., moderately effective on average.
CONCLUSIONS:
Such a “psyching-up” practice before an upcoming muscular activity can promote muscular strength in firefighters. These results have led French firefighter departments to integrate the teaching of these practices into the initial instruction of firefighters, and remains to be confirmed by a randomised control trial.
Keywords
Introduction
Firefighters regularly perform victim rescue and fire-fighting activities which may be carried out in hostile situations and/or environments [1, 2]. To carry out their missions, firefighters perform regular strenuous muscular activity especially in the upper limbs and hand-grip [3] (for example: lift, carry and use heavy protective devices and tools, climb ladders and ropes, grab, lift and transport unconscious victims) in dangerous and unpredictable environments (high temperatures, smoke, fire, restricted areas) in chaotic conditions (cries, noise, low visibility, void) [3]. An elevated level of fitness, muscular endurance and muscular strength have already been correlated with improved professional performance during firefighting activities [4, 5] and with a decreased risk of injury [6]. As such, the capacity of firefighters to be able, almost continuously night and day when on call, to produce an optimum muscular strength performance appears to be important. During their 24 hours on call, several factors induce fatigue and decrease the firefighters’ ability to produce their maximum muscular strength performance. For example, the repetition of interventions involving physical activities with a high level of psychological and physiological stress throughout a 24-hour on call [7], the time of the day [8], the repeated heavy object handling [7], the psychological workload [9] or certain emotional interactions [10] are all known to be able to decrease muscular strength performance.
Without changing the work schedule to have an acceptable interference in firefighters’ duty, two kinds of countermeasure would appear to limit the harmful effects of fatigue encountered throughout a 24-hour on call period and to promote muscular strength: the first way is to put in place efficient intervention protocols to promote recovery during intermittent break periods between two missions. Previous studies, including from our group, have already shown the interest of such a recovery protocol for firefighters [12, 13]. The second way is to develop intervention protocols to energize firefighters and promote their upcoming muscular strength performance by stimulating their neurophysiological system, whatever their current state.
The first objective of this study was thus to create an efficient intervention protocol designed to promote upcoming muscular strength performance and investigate its impact on firefighters throughout a 24-hour period. To do this, several methods are well-known to enhance muscular strength performance due to neural factors. For example, transcranial direct current stimulation [14, 15] or pre-event massage [16] have been reported to improve upcoming muscular strength performance but have not been retained here because of their impracticability in the professional context of firefighters in France. Muscular warm-up improves any upcoming muscular strength performance and is already used as a gold standard preparation for sports training by French firefighters [17]. However, muscle warm-up is made of real muscular contractions which, if they are repeated systematically before each mission throughout a 24-hour period, will lead to muscle fatigue. In itself, that would be the opposite of the effect sought here. On the contrary, and using no real movements, several “psyching-up” techniques have been reported to increase physical and mental activation and reported as beneficial tools for strength improvement among athletes [18] and non-athletes [19, 20]. Currently, motor imagery consists of mental simulation of an action or a muscular contraction but without any concomitant actual movement [21]. From a neuronal viewpoint, motor imagery is well known to activate some of the same brain areas as actual motor execution [22] and to induce greater activation of the corticospinal pathway when compared with rest [23, 24]. From a behavioural viewpoint, mental imagery can elicit, among other actions, a greater level of muscle activation [25], can delay the onset of neuromuscular fatigue [26], and can increase muscular strength performance [27].
Moreover, emotional visualisations [28] have also been reported to enhance the cortical excitability and induce enhancement of muscular strength performance. Dealing with perceived emotional contexts, high emotional arousals to avoid unpleasant contexts and to approach pleasant ones [29], or to approach unpleasant contexts in order to carry out a positive action [30] are also reported to enhance the cortical excitability of the primary motor cortex, increase neuromuscular performance [31], while the muscular strength production concomitantly increased.
Another method retained to promote muscular strength performance by dynamization of the Autonomic Nervous System (ANS) is the use of breathing exercises [32], which may be defined as breathing activities consciously controlled by the central nervous system (CNS) and not solely in an automatic and unconscious manner as during everyday life. Depending on the duration and mode of the inspiration and expiration phases, breathing exercises could either slow down or energize the ANS and the body [33]. In this way, enhancing the sympathetic activation prior to an intense physical exercise may induce cardiac preparation and increase muscular performance [34, 35].
However, even if each of the three components (i.e. motor imagery, emotional imagery, and breathing exercises) thus seems able to optimise the maximum muscular strength capacity due to neural mechanisms, it was essential to pay attention to two specific parameters in the present professional context: first, for efficiency reasons, there is the need to create a tool that can be easily implemented by firefighters when travelling between their fire station and the mission site. Consequently, the duration of practice time that was chosen was of 6 minutes in agreement with the firefighters and their operational constraints. To our knowledge, no study on the possible impact of these three methods, or a combination of the three, on muscular strength performance with such short execution times has yet been carried out. Secondly, considerable inter-individual heterogeneity exists and not all subjects systematically respond or respond equally to each of these three components [33, 36]. That is why an innovative and efficient intervention protocol (the Intervention) was specifically designed combining mental imagery practices comprising motor and emotional imagery, breathing exercises, and a short 6-minute duration execution.
The main aim of the present study was thus to investigate, using a series of “N-of-1” study design, the effects of this experimental 6-minute Intervention on the maximum voluntary isometric contraction (MVIC) strength of the hand-grip. We hypothesized that in each Intervention period, the hand-grip MVIC strength could be systematically stronger than the MVIC strength recorded during the Baseline period.
Material and methods
Participants
Participants were required to have a physical check up by the local firefighter’s healthcare institution, and participants received medical clearance to perform firefighting activities. Eligibility criteria were: 1) aged between 22 years and 40 years old with at least three years’ experience as a professional firefighter and be medically fit to work; 2) not having any musculoskeletal disorders or recent musculoskeletal injuries; 3) not suffering from post-traumatic stress disorder; 4) not having a history of neurological disorders; 5) not following acute or chronic drug treatment; 6) having a normal or corrected-to-normal hearing; 7) not undergoing sports training during the 4 days of data measurements; 8) having a minimum of 10 consecutive days off without professional work. The experimental design required 6 days. To ensure that possible fatigue related to firefighting activities did not interfere with the results of the study, we implemented a 2 days’ rest period before the start of the experiment. In the same way, to ensure that possible fatigue related to the experimental protocol did not interfere with the firefighting activities of the participants, we implemented another 2 days’ rest period after the experiment and before that these firefighters go back to work. Exclusion criteria were: 1) consuming neuro-stimulants or energy drinks 24 hours before and during the experiment.
Fourteen French professional firefighters were prospected to take part in the experiment. Nine of them were excluded before being enrolled in the study because they were not eligible for at least one of the inclusion criteria (more precisely: having a recent musculoskeletal injury in the upper limb, n = 4; following acute or chronic drug treatment, n = 2; suffering from post-traumatic stress disorder, n = 1), or because they did not wish to give their consent (n = 2). Five professional firefighters were enrolled in this study but two of them had to stop the experiment: the first due to COVID 19 infection and the second for professional requisition. Finally, three right-handed French professional firefighters volunteered to take part in the study completed the experiment. The flow of participants as recommended by the CONSORT guidance for reporting series of “N-of-1” trials [34] is reported in Fig. 1. The descriptive characteristics of these three participants were specified in Table 1.
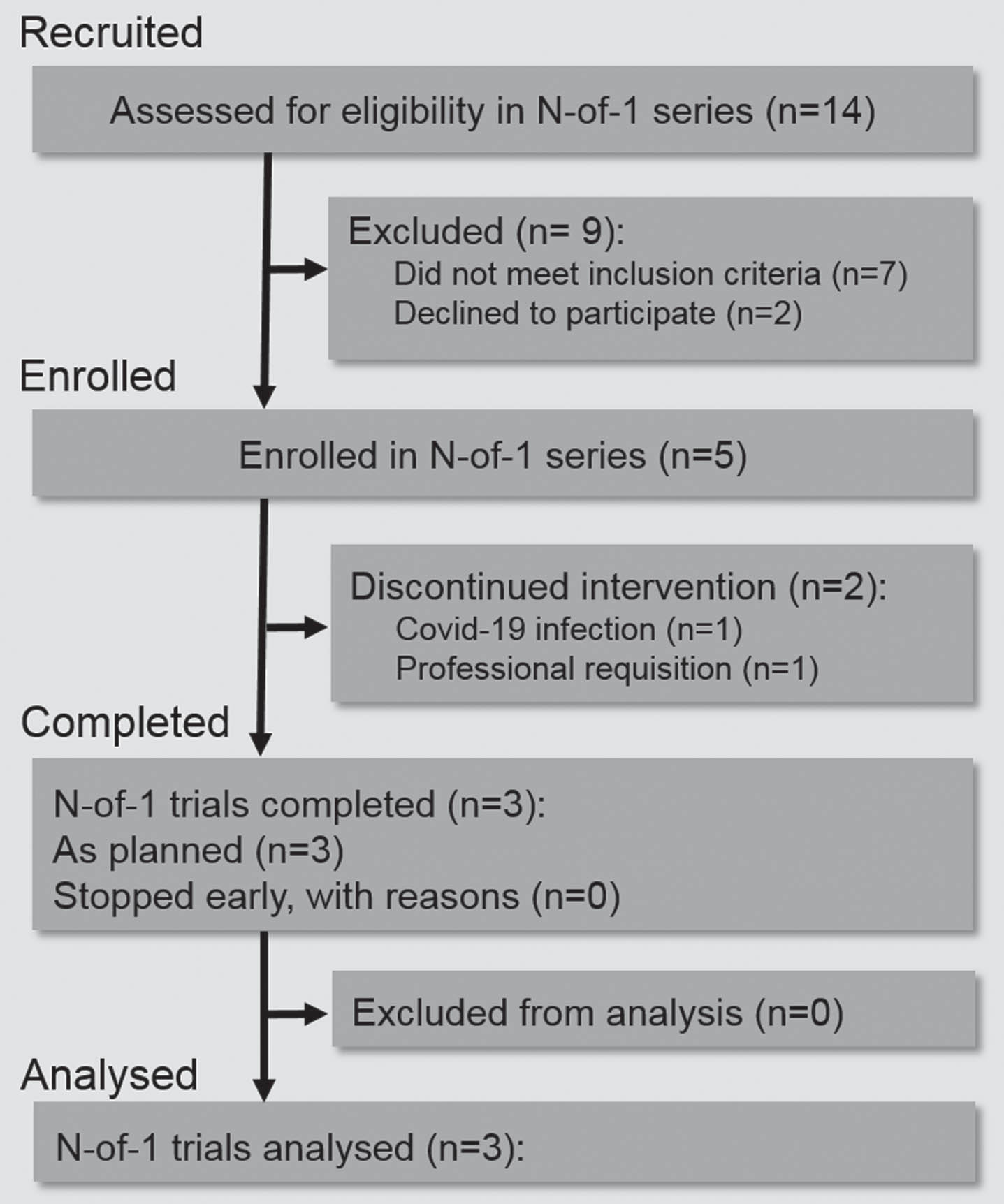
Flow diagram of participant recruitment. Representation of the flow of participants as recommended by the CONSORT guidance for reporting series of “N-of-1” trials (36).
Descriptive characteristics of the participants (n = 3)
Abbreviations: BMI, body mass index.
All participants gave written informed consent to participate in the experiment. All procedures were approved by the Ethics Committee of the Federal University of Toulouse Midi-Pyrénées (No.: 2020-04-21-213) and complied with the Declaration of Helsinki as of 2008.
The recruitment for group trials and retention (6 days in this study) may be difficult without causing some alteration of the organisation of protection of the population in France. The availability of such professionals to participate in a study are limited, and recruiting large numbers of professional firefighters at the same time is very difficult because of obvious operational constraints inherent in the profession. Moreover, it remained some reasonable doubts about the efficacy of the experimental intervention in such timeframes and with these professionals (because of their particular professional activities, firefighters cannot be considered identical to other members of the general population [3]). That is why, according to Shamseer and colleagues [37] “when recruitment for group trials is not always feasible and retention may be difficult”, we chose to design a series of “N-of-1” studies according to the CONSORT extension for “N-of-1” trials guidelines [37, 38]. Introduced as early as 1960 by Sidman [39], single-case study designs are now well-known to allow drawing strong causal inferences [40–42]. Such experimental design has been used in many recent behavioural and clinical research [43]. It is indeed listed as “level 1” evidence by the Oxford Centre for Evidence-Based Medicine 2011 levels of evidence [44]. That is why, according to the Consolidated Standards Of Reporting Trials Statement guidelines [37], this study is thus a series of N-of-1 trials designed to evaluate the same intervention across three individuals, namely a repeated challenge-withdrawal trial for each individual. Here the intervention combined mental imagery practices (motor and emotional imagery) and breathing exercises. In this so-called “ABAB” trial (in the present study, “A” is the Baseline whereas “B” is the Intervention), the period, namely the time during which a single treatment (A or B) is administered, was 24 hours. The sequence for each participant comprised two blocks of two periods with a 48-hour washout period between each block. The timeline of the experimental design is given in Fig. 2. The washout duration was chosen to match the firefighters’ rest period after a 48-hour period on call, and should allow recovery from night-timeactivities.

Timeline of the experimental design. Representation of the two 48-hour blocks made up of two 24-hour periods, the two experimental 48-hour blocks being separated by a 48-hour washout phase.
In order to overcome any possible order and/or fatigue effects in the sequence, the order of the two repeated pairs was pseudo-randomised for each participant (i.e., the outgoing combinations were automatically removed for the draw order for the next participant). Participating firefighter no. 1 followed an “AB BA” sequence, firefighter no. 2 a “BA BA” sequence and firefighter no. 3 an “AB AB”sequence.
Each period began at 4pm. In each 24-hour period, a signal was emitted every 3 hours from a beeper worn on the participant’s belt for a total of 8 measurements in a 24-hour period and a total of 32 measurements per participant in each whole SCED. At this signal, the participant had to go as fast as possible to a locker room to don his firefighting outfit. The participant then sat in a seat with armrests and put on headphones. The experimenter started a 6-minute soundtrack which was broadcast via the participant’s headphones. The broadcast was either the control soundtrack to establish the Baseline, or the Intervention soundtrack (Intervention contents are summarized step by step in Table 2). At the end of the 6 minutes, the participant went to an adjacent room to perform the maximum hand grip force measurement. The entire protocol was conducted in single-blind on the experimental side. The experimenter carrying out the measurements and analyses did not know the sequence (Baseline or Intervention) until the blinding was lifted at the end of dataanalysis.
The Intervention contents step by step. The contents of the 4 : 00–4 : 30 and 5 : 00–5 : 30 steps are emergency rescue procedures in degraded conditions known to each participating firefighter
The Intervention contents step by step. The contents of the 4 : 00–4 : 30 and 5 : 00–5 : 30 steps are emergency rescue procedures in degraded conditions known to each participating firefighter
The outcome measurement: hand-grip MVIC recordings
The outcome investigated was the maximum voluntary isometric contraction of the hand grip using a Hydraulic Hand Dynamometer (200 lbs/90 kg 5030J1, Jamar, Sammons Preston Rolyan, Nottinghamshire, United Kingdom). Since posture and handle position of the dynamometer can modulate the measured maximum grip strength, however, there is no consensus concerning measurement protocols for hand grip strength [45]. Therefore, this study assessed grip strength by the American Society of Hand Therapists protocol [46–48]: the participants in a seated position with the elbow flexed at 90° resting on a height-adjustable armrest. Their shoulders were adducted and their forearms in a neutral position. The wrist and the dynamometer were in the prolongation of the forearms and strictly over the void, i.e. not resting on the armrest. As recommended by Bechtol [49], a dynamometer with adjustable handle spacing with a verified and current calibration [50] was used to measure hand grip MVIC. Each maximum hand grip force measurement was done with the right hand less than 3 minutes after the end of the Baseline or Intervention period.
Analysis
In this series of “N-of-1” trials, in order to investigate the impact of a combination of breathing exercises and mental imagery on the maximum strength of the hand grip for each participant, we used the percentage of non-overlapping data (PND) method [50]. This method is specifically designed and validated for quantitative synthesis of SCEDs or series of “N-of-1” [43, 53]. In this method, the percentage of data points during the Intervention period which is greater than or equal to the maximum performance data during the Baseline period is calculated as the index of effectiveness of the Intervention. The effect-size is defined by the value of the PND between the Baseline and the Intervention periods within each single-case block, and defined as follows: highly effective ≥90%, moderately effective [70–90]%, minimally effective [50–70]%, ineffective <50% [54].
Results
All results of the hand-grip MVIC strength recorded either just after a passive listening session simulating a 6-minute emergency vehicle journey (the Baseline), or just after the same listening superposed with the 6-minute experimental Intervention were presented and contrasted for each of the three participating firefighters.
Firefighter no. 1
For firefighter no. 1, the order of the sequence conditions was “AB BA”. In the Baseline sequences, the (mean±standard deviation) hand grip MVIC was 43.5±1.3 kg on average in Block 1 and 43.0±1.4 kg in Block 2. In the Intervention sequences, the hand grip MVIC was 46.0 (±1.0) on average in Block 1 and 45.8 (±1.1) on average in Block 2. PND analyses showed an average effect size of 81.3% (75% in Block 1 and 87.5% in Block 2). In other words, this means that in Blocks 1 and 2, 75% and 87.5% respectively of the data points recorded in the Intervention period were greater than or equal to the maximum data point recorded in the Baseline period (see Table 3 and Fig. 3, top graph).
Main results of the hand grip MVIC strength performance for each participant and within each block
Main results of the hand grip MVIC strength performance for each participant and within each block
Abbreviations: SD, standard deviation; Max, maximum value; PND, percentage of non-overlapping data.

Hand-grip MVIC strength. Scatter chart with lines carrying over the values of the hand-grip MVIC strength in kilograms (y-axis) depending on the experimental period (Baseline or Intervention), the day and the time of day (x-axis), in Block 1 (to the left of the double vertical grey full line) and in Block 2 (to the right of the double vertical grey full line). The double vertical grey full line represents the 48-hour washout period. From the top to the bottom, each line corresponds to a participating firefighter. In each block and for each participating firefighter, the horizontal solid grey lines represent the highest value in the Baseline period taken into account for the PND analyses, and the horizontal dashed grey lines show the mean value in the Baseline period.
For firefighter no. 2, the order of the sequence conditions was “BA BA”. In the Baseline sequences, the hand grip MVIC was 58.3±1.9 kg on average in Block 1 and 59.9±1.0 kg in Block 2. In the Intervention sequences, the hand grip MVIC was 61.8±2.2 on average in Block 1 and 63.2±1.2 in Block 2. PND analyses showed an average effect size of 75% (62.5% in Block 1 and 87.5% in Block 2) (see Table 3 and Fig. 3, middle graph).
Firefighter no. 3
For firefighter no. 3, the order of the sequence conditions was “AB AB”. In the Baseline sequences, the hand grip MVIC was 63.5±1.5 kg on average in Block 1 and 62.9±1.5 kg in Block 2. In the Intervention sequences, the hand grip MVIC was 66.6±1.9 on average in Block 1 and 66.7±2.2 in Block 2. PND analyses showed an average effect size of 87.5% (100% in Block 1 and 75% in Block 2) (see Table 3 and Fig. 3, bottom graph).
Discussion
The first objective of this project was to create an efficient “psyching-up” tool with the aim to promote muscular strength performance throughout a 24-hour on-call period in firefighters. For a good acceptance rate in firefighters’ duty, the execution of this mental intervention should not have modified the schedule of the firefighters’ work and needed to be easily implemented by firefighters when travelling between their fire station and the mission site. For this, a 6-minute Intervention was created by combining mental imagery practices (namely motor imagery and emotional imagery) and breathing exercises. Then the aim of the present study was to investigate whether this 6-minute intervention executed before an upcoming exercise of hand grip MVIC strength during a 24-hour period could induce better strength performance in firefighters over a 24-hour period. Hand grip MVIC performance was compared within three SCEDs in which multiple Baseline and Interventional data were recorded allowing investigating a hypothetical causal relationship between the data values recorded and the execution of the “psyching-up” Intervention.
The 6-minute Intervention in a 24-hour period promotes hand-grip strength performance in firefighters over a 24-hour period.
The results of this study demonstrated that in each of the three SCEDs, the sixteen hand-grip MVIC strength performance values recorded during the Intervention condition were strictly greater than the average of the sixteen MVIC strength performance values recorded during the Baseline condition (see Table 3 for more details). In addition, the effect sizes of these highlighted increases of the hand-grip strength performance were moderately effective on average (see Table 3). Overall, these results showed that the three firefighters included in this series of “N-of-1” studies had a positive response to the Intervention, and thus validate the initial hypothesis.
These results are in accordance with the neurophysiological literature concerning methods used during the intervention phases of this study, which could lead to hypothesize about the theoretical neurophysiological mechanisms underlying these results: Indeed, motor imagery [24], emotional imagery [28], and breathing exercises [33] are reported in the literature to be able, under certain conditions, to increase neuron responsiveness associated with an increased muscular strength performance for the same motor action. For example, Paravlic and colleagues [55] reported in their systematic review and meta-analysis that the favourable effect of motor imagery on the upper extremity muscles when compared with no-exercise controls was moderately beneficial on average, whatever the numerous designs and training protocols of the motor imagery which were used. In the same vein, similar results with similar effect size are also reported for modulation of the emotional context [28] and breathing exercises [32, 34]. So, to conclude, we could hypothesize that one or more of these mechanisms, or interactions between them, may potentially be an underlying cause of the increase in the MVIC strength highlighted in this study.
When combined with emotional imagery and breathing exercises, just a few imagined muscular contractions were enough to promote the upcoming hand grip strength performance.
In the eleven different protocols reported by the review by Paravlic et al. [55], the motor imagery training durations were from one to twelve weeks, with two to five training sessions per week, from eighty to three thousand the total number of repetitions per study. Their meta-regression analysis revealed that a training period of 4 weeks with a frequency of three times per week with two to three sets of 25 repetitions per set were associated with moderately enhanced improvements in muscle strength following motor imagery practice. Although the above methodology makes it possible to highlight some recommendations for designing protocols in motor imagery for muscular strength improvement, it did not directly allow to favourably respond to the operational objectives and constraints in firefighters that was the main aim of this study. In a novel way, and for professional efficiency reasons, the new experimental Intervention designed and investigated here required to be able to be used during travelling between the fire station and the mission site, i.e. within a maximum of a 6-minute duration as required by the firefighters themselves. In this allotted duration, the intervention protocol was composed of “solely” twelve muscular concentric contractions at medium intensity, and four maximal isometric contractions maintained for thirty seconds each. To conclude, although the present results and their effect-sizes are in the same vein as those reported by Paravlic et al. [55], an important original finding of the present study remains that the muscular strength optimisation of the hand-grip was obtained with a 6-minute Intervention, coupling motor imagery with emotional imagery and breathing exercises. Unlike previous studies [54], the present intervention was carried out systematically before each upcoming performance measurement throughout 24-hour period. The results highlighted during the Baseline periods revealed also that this Intervention carried out for only 6 minutes 8 times a day, for only two days and separated by a minimum of 48 hours of rest without practice (the washout period), did not allow a persistent increase of the hand-grip strength over time. Repetition of this “psyching-up” intervention before each measurement would seem to be necessary here to promote hand-grip strength performance.
Limitations, recommendations and perspectives
The results highlighted in the present study are exploratory in nature. Given the small sample size of three participants, and despite the repetition of 32 measurements in total over 96 hours per participant, a first limitation of the present result is that it should not be generalised beyond the sample without further research. A second limitation is that the 6-minute duration of the Intervention raises the issue of the optimal duration to promote an upcoming performance in firefighters to be even more efficient.
A third limitation concerns the performance of mental imagery tasks itself. Even though the voice commands reflect usual firefighters’ activities, they look like complex commands. In the present study, a simple overall check at the very end of the experiment was carried out with a single question: “were you able to carry out all the exercises in the experimental protocol each time?” All participants answered “yes, absolutely”. However, this does not consist of a self-assessment questionnaire. That is why we recommend in further study to implement any form to better verify if volunteers could effectively follow all the instructions as a self-evaluationfor example.
A fourth limitation is that voluntary hand-grip strength is a reliable measurement, easy to set up, and easily reproducible from a scientific point of view. However, it alone does not guarantee or explain the whole operational performance of firefighters. That is why we recommend to study, in addition to the muscular strength, the impact of such a “psyching-up” tool on other outcome parameters such as muscular endurance, aerobic power, psychological stress or motor skills performance.
Such a “psyching-up” practice is very well received by the firefighters and the French fire service departments. Initiator and Instructor certifications in operational mental preparation for firefighters are being implemented for the very first time in France. Moreover, these results and other works of our group [12] have led French firefighter departments to integrate the teaching of these practices into the initial instruction of firefighters. That is why these promising results have to be confirmed by future research. More precisely, this primary study is leading our team to conduct a randomised control trial including some comments and testimonies from the firefighters in order to make even better the contents of the Interventions and even better evaluate their impact in firefighter operational safety and performance.
Ethical approval
All procedures were approved by the Ethics Committee of the Federal University of Toulouse Midi-Pyrénées (No.: 2020-04-21-213) as also by the Institutional Review Board of the Regional Fire and Rescue Service of Loire (Department n°42) and complied with the Declaration of Helsinki as of 2008.
Informed consent
All participants gave written informed consent to participate in this experiment. No identifying information, including participant’ names, initials, or firefighters’ numbers, are published in written descriptions or photographs in the present study.
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
The authors thank the fire rescue centers and firefighters who participated in this study. They also thank the CS APS2E association for its logistical support.
Funding
The authors report no funding.