
Abstract
BACKGROUND:
The COVID-19 pandemic had direct and indirect impacts on public health, also affecting the mental health of the population.
OBJECTIVE:
To analyze symptoms of generalized anxiety disorder (GAD) and associated factors, in primary health care (PHC) professionals.
METHODS:
Cross-sectional and analytical study conducted with professionals who work in the Primary Health Care (PHC) of the Northern health macro-region of the state of Minas Gerais, Brazil. Data collection was carried out through an online, self-administered questionnaire, made available from August 27, 2021, to October 30, 2021 using the Google Forms tool. The questionnaire included sociodemographic questions as well as questions related to the history of anxiety and work during the pandemic. To assess anxiety symptoms, the General Anxiety Disorder-7 (GAD-7) instrument was used. Data treatment consisted of descriptive analysis of the variables, bivariate analysis followed by multivariate Poisson Regression with robust variance.
RESULTS:
702 health professionals participated in the study and the general prevalence of GAD was 32.2%. Current anxiety symptoms were self-reported by 37.6% of the participants. In the final model, the associated factors identified were: female sex (PR = 1.82; 95% CI = 1.17–2.84; p = 0.007), previous symptoms (PR = 1.58; 95% CI = 1.19–2.10; p = 0.002) and (PR = 2.68; 95% CI = 2.00–3.62; p < 0.001) current self-reported anxiety.
CONCLUSION:
The results show the need to implement actions in mental health promotion and anxiety prevention, through the dissemination of information about mental health care, health education activities, encouraging the adoption of healthy habits and professional monitoring when necessary.
Introduction
In Hubei Province, China, an outbreak of pneumonia caused by a new type of coronavirus was reported and associated with the local food market in December 2019 [1]. This disease is caused by SARS-CoV-2, received the name of COVID-19, and was declared a pandemic in March 2020 by the World Health Organization (WHO). It is a contagious disease that can be lethal, depending on the conditions of each infected patient [1, 2].
With the COVID-19 pandemic, health services had to reorganize their work processes due to the increasing number of positive cases of the disease, which require greater attention from health professionals. Additionally, the lack of hospital beds has been observed in countries with insufficient capacity for hospitalizations [3]. However, publications highlight the importance of strengthening Primary Health Care (PHC) in the fight against COVID-19 in the context of the pandemic [4, 5]. With its roles and work processes, PHC has been fundamental in health surveillance within its territories and in the monitoring and management of patients with mild and moderate symptoms. Furthermore, PHC acts as a care coordinator for cases that need to be referred to the tertiary level of care [4, 5].
The work overload of health professionals in response to COVID-19 has had several consequences on their health status. The manifestation of symptoms of physical and, mainly, mental stress is being widely reported to the scientific community [6–10]. Generalized Anxiety Disorder (GAD) is a disorder that can lead to a loss of quality of life and is among the ten leading causes of years lived with disability. Brazil has the highest prevalence of anxiety in the world [11]. In a systematic review, the findings on the prevalence of anxiety in health professionals showed results that ranged from 22.2% to 33.0% [12]. However, the prevalence of this disorder in this population is higher than in the general population [13].
To our knowledge, studies involving the assessment of the prevalence of anxiety symptoms in the different professional categories of PHC in Brazil are unknown, as well as their factors associated with the COVID-19 pandemic. Thus, the objective of this study is to analyze GAD symptoms, as well as their associated factors, in PHC health professionals.
Methods
A quantitative, descriptive, analytical, and cross-sectional study was conducted in the northern health macro-region of Minas Gerais (MG), Brazil. This region is composed of the Regional Health Superintendence (SRS) of Montes Claros, which comprises 54 cities, the Regional Health Management (GRS) of Januária, covering 25 cities, and the GRS of Pirapora, covering seven cities, presenting a total of 86 target municipalities for the present study.
The study participants were health professionals who work in PHC in the North health macro-region of Minas Gerais. The study universe, verified in August 2021 using TABNET system [14] developed by DATASUS to generate information from the Unified Health System databases, was composed of 8,968 professionals. The inclusion criteria adopted were: being a health professional in APS and working in one of the cities that compose the macro-region studied. Individuals who were on vacation or on service leave for any reason during the data collection period were excluded.
The sample size calculation was performed using the following statistical criteria: population size of 8,968, a confidence level of 95%, an estimated prevalence of 32% [15], a margin of error of 5%, and a correction for design effect (DEFF = 2). Based on these parameters, a minimum of 645 health professionals was required for the study.
Sampling was done using a convenience method, obtained through the snowball technique [16]. The responsible researcher contacted the SRS of Montes Claros and the other two GRS of the North macro-region to obtain the contacts of the respective PHC coordinators of the cities included in the research. Invitations were sent to the coordinators via email and social networks (WhatsApp and Instagram), and they sent the invitations with the link to access the questionnaire to health professionals in their respective cities for online data collection. The data collection took place from August 27, 2021, to October 30, 2021. The data collection process is described in Fig. 1.
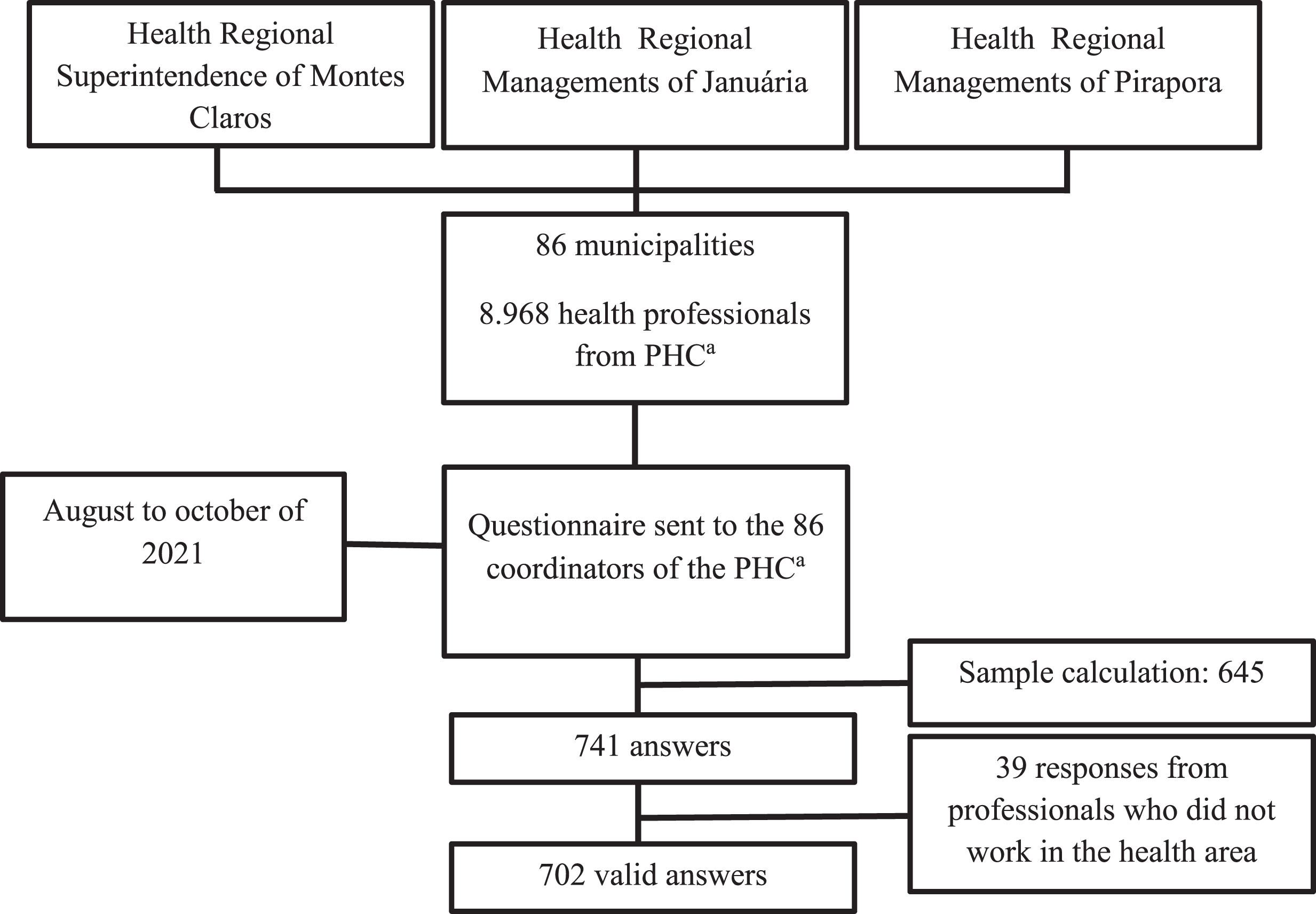
Flowchart of the data collection process. aPrimary health care.
The variables were measured using an online, self-administered questionnaire made available through the Google Forms® tool. The variables used for the characterization of study participants included sex, age group, marital status, income, performance level, professional category, region of activity, and whether they worked on the front line of COVID-19. The contagion of COVID-19 was measured by the question “Have you had COVID-19?". For the history of anxiety symptoms, the variables included previous and current anxiety symptoms, previous and current psychological and/or psychiatric follow-up, and previous and current use of anxiolytic medication. Work overload during the COVID-19 pandemic was measured using the response options “I worked less than usual”, “I worked the same way I used to”, “I worked more than usual and felt overwhelmed”.
The dependent variable of the study was the presence of GAD symptoms, measured by the General Anxiety Disorder-7 (GAD-7) instrument. The GAD-7 is a validated instrument, and widely used in studies. The questionnaire consists of seven questions that assess symptoms experienced by the respondent, including feeling nervous, anxious, or on edge; not being able to stop or control worrying; worrying too much about different things; trouble relaxing; being so restless that it is hard to sit still; becoming easily annoyed or irritable; and feeling afraid as if something awful might happen. The answer options for the questions included “Not at all,” “several days,” “more than half the days,” and “nearly every day” and were answered using a Likert scale with response values ranging from zero to three points [17].
The GAD-7 questionnaire produces scores ranging from 0 to 21 points, with a result of 0–4 classified as minimum anxiety, 5–9 as mild anxiety, 10–14 as moderate anxiety, and 15–21 as severe anxiety. A cut-off point of ≥10 was used in this study to assess the presence of anxiety symptoms. At this cut-off point, the scale has a sensitivity and specificity of 89% and 82%, respectively [17].
It is worth noting that the research team prepared a booklet with information related to mental health care for health professionals. The booklet was organized to provide participants with relevant guidelines on the topic of anxiety and common mental disorders. After completing the questionnaire, participants had access to the material.
The data obtained from the research were entered into the Statistical Package for the Social Sciences for Windows® (SPSS) program. Descriptive analysis of the variables was performed, as well as bivariate analysis (simple Poisson regression) to verify associations between independent variables and the outcome, and multiple analysis (Poisson regression with robust variance). For the multiple analysis, variables associated with a significance level equal to or less than 20% (p≤0.20) were included and the variables that showed an association at a level equal to or less than 5% (p≤0.05) were maintained in the final model. The multicollinearity was evaluated by the variance inflation factor (VIF) values and the goodness of fit of the model was evaluated by the deviance test.
This study was conducted in accordance with the Declaration of Helsinki of 1964 and its later amendments, with Resolution No. 466 of December 12, 2012 of the National Health Council of the Ministry of Health and the Circular Letter No. 1/2021 of the National Research Ethics Commission, which presents guidelines for conducting research in a virtual environment, including data security and privacy issues. The research was approved by the Institutional Research Ethics Committee (#4.838.846/CAAE n° 47795821.7.0000.5146).
A total of 741 responses were recorded from August 27 to October 30, 2021, with 39 responses not meeting the inclusion criteria, as they were answered by professionals who were not in the health area, and, for this reason, were excluded. Thus, there were 702 valid responses of health professionals from 61 cities among the 86 in the macro-region of Minas Gerais, with the majority of participants being female (84.5%). The results also show that the majority were in the age group of 19 to 39 years (71.5%), with a mean of 35.31 years (standard deviation of σ 8.35), married (55.7%) and with income from 1 to 2 minimum salaries (55.4%) (Table 1).
Characterization of health professionals in the northern macro-region of Minas Gerais (n = 702), 2021
Characterization of health professionals in the northern macro-region of Minas Gerais (n = 702), 2021
†Superintendência Regional de Saúde (Regional Health Superintendence). ‡Gerência Regional de Saúde (Regional Health Management).
The overall prevalence of GAD was 32.2%. Table 2 shows the variables related to anxiety and the mental health history of professionals. 37.6% self-reported current anxiety symptoms and according to the GAD-7 34.8% had moderate symptoms. In terms of current follow-up with a mental health professional, 14.8% answered affirmatively, and 21.7% reported using anxiolytics.
Anxiety and mental health history of health professionals in the North macro-region of Minas Gerais (n = 702), 2021
Table 3 presents the prevalence, prevalence ratio (PR) and respective p value of the association between the outcome variable and the independent variables of the study. The following variables had a p-value <0.20 and were included in the multiple analysis: sex, age group, marital status, performance level, professional category, frontline work, presence of previous and current anxiety symptoms, previous and current psychological and/or psychiatric follow-up, previous and current use of anxiolytic, and work load during the pandemic.
Bivariate analysis between anxiety (GAD-7) and independent variables in health professionals from the northern macro-region of Minas Gerais (n = 702), 2021
†Superintendência Regional de Saúde (Regional Health Superintendence). ‡Gerência Regional de Saúde (Regional Health Management).
In the multiple analysis, a statistically significant association was found between the variables of sex, profession, and presence of previous and current anxiety symptoms. The highest prevalence was found in female professionals (p = 0.008) and in those who reported previous or current symptoms of anxiety (p = 0.002 and p = 0.000). The variables included in the multiple analysis did not show multicollinearity, as the VIF values were below 10 and tolerances above 0.20 (Table 4).
Multiple analysis between anxiety (GAD-7) and independent variables in health professionals from the northern macro-region of Minas Gerais (n = 702), 2021
It is noteworthy that the prevalence of anxiety found in this study corroborates the results of a systematic review with meta-analysis that evaluated the impact of the COVID-19 pandemic on the mental health of healthcare professionals and the general public. The review found an overall prevalence of anxiety of 33.0% (28.0% – 38.0%) [18]. A similar study identified a prevalence of 24.0%, and when evaluating only articles that used the GAD-7, the same instrument used in this study, a prevalence of 36.9% in healthcare professionals was observed in subgroup analysis [19].
The findings of research carried out in Brazil with healthcare professionals from medium and high complexity services during the COVID-19 pandemic period identified anxiety ranging from 31.3% to 48.9% [20–23]. Studies analyzed in a systematic review [19] show a wide variation in the prevalence of anxiety among these professionals, ranging from 10.0% to 44.7%. This variation can be explained by the heterogeneity of the studies, the variety of instruments used in the research, and the fact that they were conducted in different places and times during the pandemic.
A study carried out in Spain [9] compared anxiety symptoms between healthcare professionals working in hospitals and PHC professionals, with prevalences of 35.0% and 37.0%, respectively. Additionally, the risk of developing anxiety was significantly higher in PHC professionals (32.0%) compared to hospital professionals (18.0%). In China, when evaluating anxiety in 33,706 hospital professionals, researchers found a general prevalence of anxiety of 24.4% [24], which is lower than that observed in the present investigation.
Although there is not a high level of evidence for the difference between the prevalence of anxiety in the two groups, Londoño-Ramírez et al. [9] explain the possibility that, as PHC is the first point of contact in the health system, the work overload, uncertainty and fear of being infected by COVID-19 or transmitting it to a family member may have been greater in this group.
Women presented 2.41 times more chances of having anxiety symptoms than men, remaining in the final model of the multiple analysis with an adjusted PR of 1.85. The scientific literature has shown that women are at a greater risk of developing symptoms of anxiety, with a 1.9 times greater risk, which persists even when associated with other variables such as income, ethnicity, and geographic location [25]. A possible explanation for the higher prevalence of anxiety in women is the social conditions in which they live, such as a double burden, social attribution of the female role of care, lack of family support, lack of autonomy, male chauvinism, and being more often victims of domestic violence. The pandemic is a scenario that can aggravate these social factors [23, 26].
The age group from 31 to 39 years old had the highest prevalence of GAD. This result differs from a study carried out in China [27] whose findings, converging with other studies, show that participants younger than 35 years old had a higher prevalence of anxiety symptoms. Another study [28] that assessed the impact of the pandemic on the psychological state of 1653 participants from 63 countries demonstrated a greater vulnerability to the manifestation of stress, depression, and anxiety in the age group of 18 to 35 years. A similar result was found in a systematic review with meta-analysis [29] that identified a higher prevalence of anxiety and depression in the younger population, particularly in the age group of 20–24 years. Due to school closures and broader social restrictions, the physical gathering of young individuals has been hindered, impacting their learning capabilities and limiting peer interaction. Additionally, young people are at a higher risk of unemployment during and after economic crises, such as the one caused by the COVID-19 pandemic, compared to older individuals. These factors are possible explanations for the higher prevalence of anxiety and other mental disorders in this group [30].
In relation to marital status, people who live without a partner may be at a greater risk of developing symptoms of anxiety, as loneliness is a factor that can lead to higher levels of anxiety, as pointed out by Ta et al. [31]. In this study, the category that presented the highest prevalence was divorced, and the other categories did not present a statistically significant difference in the prevalences.
Although no significant difference was found between anxiety symptoms and income, studies analyzed in a review [32] show that people who live with fewer financial resources are at a greater risk of presenting symptoms, as poverty is associated with stressful environmental factors [33], greater exposure to violence and crimes [34], greater difficulty in accessing healthcare services, and greater concern and uncertainty about the future and health crises, such as the COVID-19 pandemic, that can aggravate this situation [32].
Regarding education, the intermediate level of professional education presented a higher prevalence of anxiety compared to the technical and higher levels. However, higher levels of education generally increase access to information related to healthcare and provide more opportunities for making choices, setting goals, and aspirations in life, which can lead to the adoption of healthier habits [35]. It is noteworthy that among the technical professionals, the majority were nursing technicians, professionals who were at the frontline in the fight against COVID-19 with higher exposure to the virus, increased workload, lack of adequate resources, and concerns regarding contagion and transmission of the virus [36, 37]. These factors possibly contributed to the higher prevalence found in this group.
It is observed that higher income and education levels are protective socioeconomic factors regarding mental disorder symptoms in general, including access to treatment, as shown in a study [38] that analyzed 16,753 patients diagnosed with mental disorders in 25 countries. The study identified that few patients have adequate access to treatment, even in high-income countries, with greater inequality in treatment access for individuals with low levels of education and income.
Among the professions with the highest number of participants, the prevalence of anxiety in nursing professionals (nurses and nursing technicians) stands out, which was higher than other professional categories. Nursing professionals mostly worked on the frontline in the fight against COVID-19 and studies have shown high levels of anxiety in this professional category [21, 23].
Professionals who worked on the front line in the fight against COVID-19 showed a higher prevalence of anxiety symptoms in the bivariate analysis. This result is consistent with the findings of other studies [13, 39] that compared symptoms between frontline healthcare professionals and other healthcare professionals. Cai et al. [40] identified concerns about personal safety and that of their families, the lack of protective equipment, and increased work overload as variables associated with higher levels of anxiety. Although other studies [41, 42] have shown that patients who have had COVID-19 may have anxiety symptoms during the period of infection and afterward, this study found no significant difference between a previous history of COVID-19 and anxiety symptoms.
Participants who answered “yes” to the variables “previous and current anxiety symptoms,” “previous and current psychological and/or psychiatric follow-up,” and “previous and current use of anxiolytic medication” had a higher prevalence of anxiety symptoms. Having a history of anxiety diagnosis is a risk factor for the manifestation of anxiety symptoms [42].
It is observed that 37.6% of participants reported current symptoms of anxiety; however, the overall prevalence, assessed by the GAD-7, was 32.2%. In both cases, the number of professionals is greater than those who reported being in psychological or psychiatric care and using anxiolytics, which were 14.8% and 21.7%, respectively. This information shows that there is a significant number of healthcare workers who have symptoms of anxiety and have not sought professional help. This situation can lead to a worsening of anxiety.
The professionals who reported working more during the pandemic and feeling overwhelmed had a higher prevalence of anxiety symptoms. This association between work overload and the manifestation of psychological symptoms is well documented by other studies [9, 43].
Regarding the level of anxiety, it was observed that the majority (34.8%) of the participants had a moderate level of anxiety, which can be understood as the presence of mild anxiety symptoms that, even if not currently causing significant impairment in the patient’s life, puts them at risk for the development of more severe symptoms [44].
The limitations of this study should be taken into consideration. The use of a self-administered questionnaire may have led to response and memory biases. Additionally, the convenience sampling method used due to the COVID-19 pandemic may have limited the representativeness of the sample. Moreover, the online delivery of the survey may have excluded professionals who do not have internet access or are not proficient in using the internet.
It is noteworthy that this study is a pioneer in assessing anxiety symptoms among PHC professionals in Brazil. Seeking to understand the mental health conditions of health professionals, especially in PHC, in the context of the COVID-19 pandemic is essential to comprehend the impacts of the new disease on workers’ health. Additionally, efforts must be made to establish strategies that reduce these damages.
Conclusion
The prevalence of GAD was observed in 32.2% of the PHC professionals studied, with the majority experiencing a mild level of anxiety, placing them at risk of developing more severe symptoms. Female gender and self-reported previous and current anxiety symptoms were associated factors identified by the multiple analysis. A significant number of professionals reported experiencing anxiety symptoms but were not receiving professional care, highlighting the need to raise awareness among this population about the importance of mental health care.
Also noteworthy is the importance of developing actions to promote mental health and prevention of anxiety for PHC health professionals. Health education activities on the subject, implementation of listening spaces, encouraging the adoption of healthy habits, psychological and/or psychiatric support and follow-up when necessary are suggested.
Footnotes
Ethical approval
The study was approved by the State University of Montes Claros (#4.838.846/CAAE no 47795821.7.0000.5146).
Informed consent
All participants signed the informed consent form.
Conflict of interest
The authors declare that they have no conflict of interest.
Acknowledgments
The authors thank the Minas Gerais Research Support Foundation (FAPEMIG), the National Council for Scientific and Technological Development (CNPQ), the Coordination for the Improvement of Higher Education Personnel (CAPES), the Health Regional Superintendence of Montes Claros, and the Health Regional Managements of Januária and Pirapora.
Funding
The authors report no funding.