
Abstract
BACKGROUND:
Smartphones are a technical marvel that rapidly evolved to play an important role in our lives. One downside to smartphone use is that it significantly worsens posture. It is believed that using a smartphone while walking increases the risk of cognitive decline and the loss of dynamic balance needed to perform functional tasks.
OBJECTIVE:
The objective of the study was to determine the impact of smartphone usage on dynamic postural control among South Indian college students.
METHODS:
The study was carried out in a private college with 400 invited students through online social media platforms. The four-square step test and SAS-SV were used to determine the impact of smartphone usage on dynamic postural control. The students were informed about the study process. A total of 250 participants were included based on the inclusion criteria.
RESULTS:
There was a high percentage of agreement on smartphone usage on dynamic postural control measured with SAS-SV, revealing statistical significance with a mean value of 41.532 and SD of 10.010886. The four-square step test with a mean value of 22.5 and SD of 1.8995878 also proved significant impact. A positive correlation was found between smartphone usage and dynamic postural control, which was analysed using Pearson’s correlation coefficient of 0.90130.
CONCLUSION:
A significant correlation was noted between mobile usage and dynamic balance. Smartphones can have a negative impact on dynamic balance by distracting users from their surroundings and increase the risk of falls.
Introduction
Due to numerous advantages, such as information accessibility, social networking, professional applications, portability and handiness, smartphones are a common technological breakthrough that have significantly expanded to play a vital part in our lives. [1]. The smartphone has already ingrained itself into teenagers’ daily lives; while it provides many conveniences, it also has certain drawbacks. Smartphone use affects users both physically and mentally. Extended use of smartphones puts the muscles and ligaments under continuous mechanical strain, which may be harmful to the musculoskeletal system [2].
With the increased usage of mobiles for the purpose of communication, telephones have evolved and have been converted into smartphones in recent years. When it comes to features other than phone communication, including access to social networking applications and business tools, smartphones have supplanted computers. [3]. According to Shetty et al., 79% of those who aged between 18 to 44 years have their cellphones with them practically all of the time, with only 2 hours of their walking day spent without them [4].
Balance is the ability to maintain one’s gravitational line inside the base of support. It is sometimes referred to as the capacity to sustain equilibrium, which is any circumstance in which all of the forces at play are present and neutralise one another to produce a stable, balanced system. While body parts are moving, dynamic balance is the ability to maintain stability of posture and its orientation with the centre of mass over the balance of support. Proprioceptive information from mechanoreceptors in the capsule, ligament, muscle, and tendon, as well as vestibular and visual input to the central nervous system, are all necessary for maintaining balance [5]. Balance does not need intense concentration in most of the environments and is regulated passively [6]. Additionally, it was shown that using a smartphone negatively affected posture, especially in the trunk and neck regions. Both the plantar pressure distribution and the stabilize-graphic factors may be impacted by these changes. [7]. Using a smartphone while walking to do activities such as listen to music, send messages, browse the web, or play games, is considered to reduce cognitive capacity and so damage the dynamic balancing ability required for functional tasks [8]. The amount of time spent texting on mobile devices has skyrocketed in recent years, especially among youngsters worldwide. In Sweden, everyone between the ages of 15 and 24 years has access to a cellphone, and 93% of them text on a daily basis. In the USA, 75% of 12 to 17-year-olds in 2009 had their own mobile phone, and 88% of those were text-messaging devices. One-third of them send more than 100 texts per day, and half of them send more than 50 texts daily. The posture needed to utilize visual display terminals, like those in smartphones, for a longer period of time can result in MS system and posture issues [9]. Multitasking situations, such as using a smartphone while driving, can be bad for your posture, much as reading the newspaper while standing on an unsteady surface [10].
When employing dynamic postural control, some degree of movement around a base of support is required. This could involve actions like jumping or hopping to a new location and then trying to stop moving as soon as you can, or trying to make controlled segment movements (reaching) without compromising the established base of support. Dite and Temple created the four-square step test (FSST), which includes quick steps while changing directions. The FSST was developed to examine dynamic standing balance and mobility to a range of patient populations [11, 12]. The Smartphone Addiction Scale - Short Version (SAS-SV) was also found to be feasible, time-effective, and helps to analyze smartphone addiction quickly and easily [13]. The purpose of the study was to examine how South Indian college students’ use of smartphones affected their ability to maintain dynamic postural control.
Methods
Study setting and participant selection
With institutional scientific research board (ISRB) clearance, the study was carried out in a private college in South India. Email invites and social media sites were used to find participants. Students who expressed interest were contacted and given comprehensive details on the study’s approach. Informed consent was obtained from those who agreed to participate. Initially, a total of 400 students were included in the study. 370 of the 400 students fulfilled the requirements for inclusion, while the 120 who did not were eliminated. Thirty students dropped out the study time for personal reasons. Ultimately, the study was conducted with 250 participants, consisting of 133 male and 117 female students.
Inclusion and exclusion criteria
Participants expressing interest in participation underwent a screening process. Students between the ages of 19 and 25, who exhibited high-frequency mobile phone usage and did not have any musculoskeletal, neurological, or sensory disorders, were included in the study. Exclusion criteria encompassed a history of mental, physical, or psychological illnesses, as well as auditory, visual, or perceptual deficiencies. Additionally, individuals with conditions that would affect balance or neuromuscular control were excluded.
Outcome measures
The FSST was employed as an outcome measure to assess balance in healthy populations. The FSST requires four single point sticks and a timer. Participants begin in one square and sequentially move into each of the four squares in one direction, ultimately returning to the starting position to form a cross. The objective is to complete the sequence as quickly as possible without touching the sticks. Each square requires both feet to make contact with the ground, and participants are instructed to face forward throughout the procedure.
A practice trial and two test trials were conducted to make sure participants understand the sequence of events. During the test trials, the fastest time is noted. The trial was redone if a person trips and falls or makes contact with a barrier during the sequence. In cases where participants are unable to maintain forward-facing orientation, they are allowed to step forward and turn into each square. The FSST measures the time (in seconds) required to complete the entire process. In previous research, a time exceeding 15 seconds has been associated with a high risk of falling in individuals over 65 years of age (positive predictive value 86%, negative predictive value 94%).
The Smartphone Addiction Scale (SAS) was utilized as a self-diagnostic measure to assess participants’ addiction to mobile phone usage. The scale was adapted from the K-scale, which evaluates internet addiction in young people. In this study, the SAS-SV consisting of 10 questions was employed. The scale includes six subscales: Daily-Life Disruption, Withdrawal, Cyberspace-Oriented Relationship, Overuse, Tolerance, and Positive Anticipation. However, for the SAS-SV used in our study, only items from five of the six variables were included, omitting the Positive Anticipation scale. Each question is scored on a scale from 0 to 6, resulting in a total score ranging from 0 to 60. For females, a score higher than 33 indicates addiction, while for males, a score higher than 31 indicates addiction. Scores between 22 and 31 indicate a high risk of addiction. The SAS-SV provides a concise assessment of smartphone addiction in teenagers using a 10-question survey and offers cut-off values for each gender, enabling application in both clinical and practical contexts [13].
Results
A total of 400 students were invited to participate in the study, out of which 250 students met the inclusion criteria and were selected to take part. Descriptive statistics were employed to analyze the data obtained from the SAS-SV and the FSST.
The statistical analysis revealed a high prevalence of smartphone addiction among college students (Table 1). The overall mean score for the entire population was 41.532, with a standard deviation (SD) of 10.010. The results were examined by gender, the mean score for males were 41.879 (SD 9.902), while for females it were 41.136 (SD 10.160). These findings indicate a substantial level of smartphone addiction among both male and female students, with a slightly higher mean score observed amongmales.
Mean and SD values obtained after statistical analysis using SAS-SV
Mean and SD values obtained after statistical analysis using SAS-SV
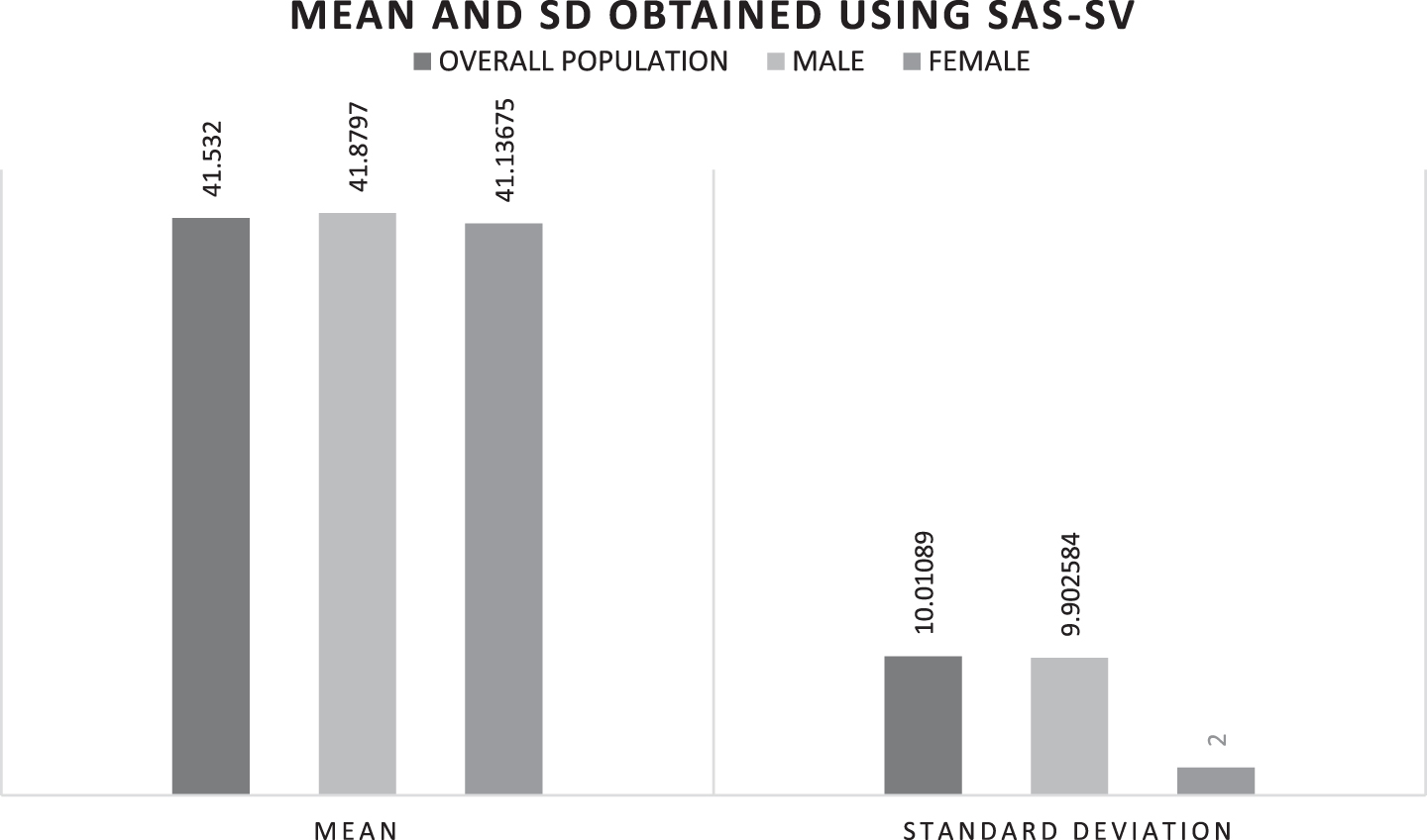
Mean and SD obtained using SAS-SV.
Furthermore, the results indicated a significant decline in dynamic postural control among South Indian students as a result of frequent mobile phone use (Table 2). The overall mean score for dynamic postural control was 22.5 (SD 1.899). Specifically, males had a mean score of 22.017 (SD 1.899), whereas females had a mean score of 22.55 (SD 1.904). Notably, females exhibited a slightly greater loss of dynamic postural control compared to males.
Mean and SD values obtained after statistical analysis using FSST

Mean and SD obtained using FSST.
Correlation analysis revealed a significant relationship between the high impact of mobile phone use and dynamic postural control, with a correlation coefficient of 0.901 for the entire population (Table 3) at a significance level of p > 0.05. The analysis employed Pearson’s correlation test. When comparing the correlation rates between genders, females demonstrated a higher correlation coefficient of 0.9029035, while males showed a correlation coefficient of 0.881612 at a significance level of p > 0.05. These results indicate a strong association between smartphone use and its detrimental effects on dynamic postural control, with females exhibiting a slightly stronger correlation.
Correlation between mobile phone usage and dynamic postural control
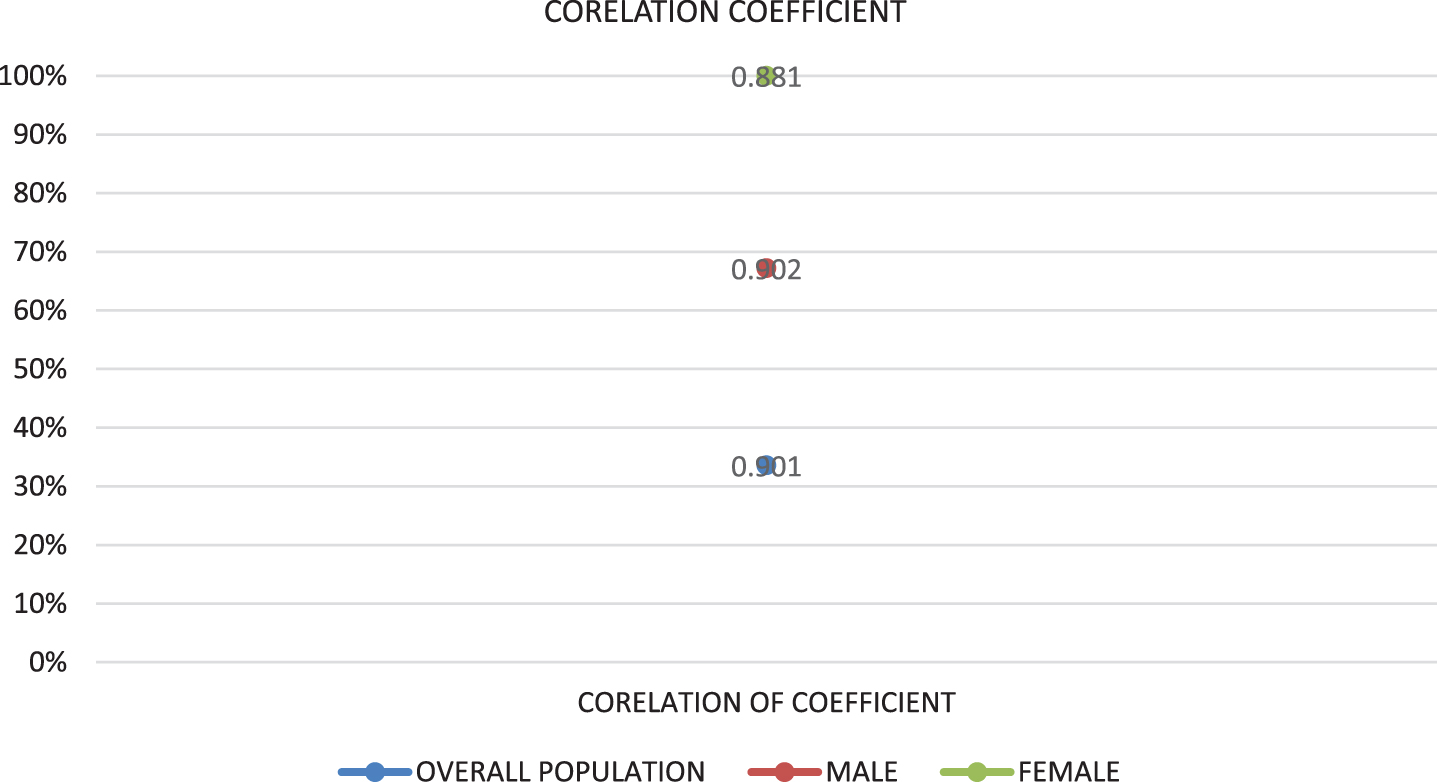
Corelation between mobile phone usage and dynamic postural control.
Overall, the findings highlight the high prevalence of smartphone addiction among college students and the adverse impact on dynamic postural control. The results underscore the need for interventions and awareness programs to address smartphone addiction and mitigate its effects on postural control in the student population.
The purpose of this research was to examine how South Indian college students’ use of cellphones affected their ability to maintain dynamic posture. It is critical to comprehend the health risks linked to excessive smartphone usage and how they affect general public health.
Excessive smartphone usage can lead to significant musculoskeletal diseases, resulting in pain and fatigue in various body parts, including the upper limbs, neck, shoulders, arms, wrists, back of the hand, fingers, and waist. Studies, such as the one conducted by Shafeek et al. [2], have highlighted that using a smartphone for prolonged periods can cause a loss of dynamic balance. This finding emphasizes the need for caution to prevent accidents during activities like walking, playing sports, or engaging in daily tasks. However, it is worth noting that the adverse effects on dynamic balance can be reversed after a period of rest.
Zidan et al. [5] discovered a substantial difference between males and females regarding the detrimental effects of extended smartphone use on dynamic balance. These results contribute to increasing public awareness regarding the risks associated with prolonged smartphone usage and the need for initiatives that address the impact on female individuals’ balance abilities.
Research by Kim et al. [6] examined the effects of smartphone use on lower limb joint angles and dynamic balance during gait. While no substantial differences were found in lower limb angular position during walking under smartphone use conditions, there were significant decreases in stability limits during phone conversation and smartphone game conditions compared to not using a smartphone. Therefore, using smartphone while walking require extra attention to maintain the balance.
Additional research has repeatedly demonstrated the detrimental effects of excessive mobile phone usage on dynamic equilibrium, which can cause unsteadiness when walking, playing sports, and performing daily chores. Text messaging while walking, for example, reduces walking speed by 33% and increases lateral deviation by 61%, significantly affecting one’s ability to maintain dynamic balance [10]. To determine the prevalence of the impact of mobile phone usage on dynamic postural control, we selected the FSST as it has been shown to have high reliability and validity in measuring dynamic balance [11, 14].
Based on the significant results from the SAS-SV questionnaire, we found a greater level of mobile phone addiction among students. Significant differences in dynamic balance were observed among mobile phone users during the FSST, indicating a decline in dynamic balance with prolonged mobile phone use. Students’ balancing skills were compromised, resulting in difficulty in adapting to environmental changes and applying vestibular information during task performance. Hence, in order to avoid adverse effects, our study emphasises how crucial it is to refrain from using a smartphone when having poor dynamic postural control [10, 13].
Dynamic balance is impacted by smartphone use, according to a correlation study done by employing Pearson’s correlation coefficient. Generalising the results to people of all ages should be done with caution, as this study exclusively focused on college students. Further research is needed to explore the relationship between mobile phone usage and postural control.
Limitations and suggestions
This study is not without limitations. First, this was a qualitative, not a quantitative, study. Second, no proper follow up of students could be conducted as we aimed to see only the prevalence. We fervently urge the conduct of additional research to examine the impact of additional variables that may have affected dynamic balance. Since we lacked the resources to carry out our research as an experiment, it can be verified more thoroughly by doing so as an experiment with a control group.
Conclusion
By using SAS-SV and the FSST, a significant correlation was found between mobile phone usage and dynamic postural balance. A notable percentage of south Indian college students demonstrated a lack of dynamic postural control associated with the habit of frequent use of their mobile devices. Furthermore by diverting users’ attention from their surroundings and making them less aware of the environment, smartphones can have a detrimental effect on dynamic balance by raising the chance of falls and other mishaps.
Conflict of interest
The authors report no conflict of interest.
Funding
The authors received no specific funding for this work.
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude to the study participants, the authors whose works are referenced and cited in the manuscript, and the creators of the SAS-SV and FSST.
Ethics statement
The study was approved by the local institutional scientific research board (ISRB). Informed consent was obtained from all participants.