
Abstract
BACKGROUND:
During the COVID-19 pandemic, physical inactivity and inactivity-related health problems have deepened in many individuals, including office workers. It is not yet known whether there are exercise programs through telerehabilitation that will provide rapid relief in a short time in office workers who apply part or full-time teleworking system.
OBJECTIVE:
To comparatively investigate influences of short-term upper extremity exercise trainings (UEET) on pain, musculoskeletal discomforts (MSD), physical activity (PA), mood, and quality of life (QOL) in office workers during COVID-19 restrictions.
METHODS:
Thirty office workers were divided into exercise (EG) (UEET and walking advice) and control (CG) (walking advice) groups. The UEET was applied for at least 20–40 minutes/day, 5–7 days/week for a one week between February 2022 and June 2022. Office workers’ pain, MSD, PA level, mood and QOL were measured.
RESULTS:
Baseline characteristics of groups (EG: 37.8±7.04 years, CG: 41.6±7.97 years) were similar (p > 0.05). Following UEET, scores of office workers in EG on total step count, vigorous PA, moderate-intensity PA, walking, total PA, physical functioning, and body pain subscales of QOL significantly increased compared to scores of office workers in CG, while scores on neck, back and hip discomforts and anxiety and depression significantly decreased (p < 0.05).
CONCLUSIONS:
One-week UEET and walking advice can improve office workers’ daily step counts, MSD, PA levels, mood, and QOL. Office workers who have a busy work schedule may do these UEET and walking exercises in break times to relieve perception of discomfort.
Introduction
Musculoskeletal system discomforts (MSD) are common in office workers. MSD can develop in the upper extremities of office workers due to various reasons, such as age, gender, poor posture, work stress, heavy workload, making repetitive movements in office environment, unsuitable keyboard/table/screen features, and incorrect sitting posture [1]. In recent years, in parallel with developments in technology, making repetitive wrist movements in front of a computer every day and using computers for a long time in non-ergonomic working positions have been added to these reasons. Office workers may even experience carpal tunnel syndrome, lateral epicondylitis, neck/shoulder/low back pain, and posture disorders [2]. On the other hand, sitting at a desk for a long time can also lead to MSD due to physical inactivity. Sitting in a fixed position for more than two hours increases discomfort in the low back, hips, and thigh regions [3].
Regardless of the presence of pain in office workers, many positive effects of various exercise training programs have been revealed to date [4–21]. Among these positive effects, the first place is shared by reduction of pain and improvement of quality of life (QOL). This is followed by decreases in fatigue, anxiety, depression, and postural overload and increases in muscle strength, balance, body functions, and occupational satisfaction [4–21]. It has been reported that working skills improve in office workers after three months of neck/shoulder strengthening exercise training and ergonomic arrangements. This is also maintained for about nine months [22, 23].
The occurrence of pain in certain body parts including low back, neck, and shoulders due to prolonged sitting and physical inactivity is the most common MSD worldwide. This situation has both socio-economic and individual consequences. One of the effective ways to reduce MSD in office workers is exercise training, which focuses specifically on the upper extremities and spine [22–24]. Upper extremity exercise trainings (UEET) can be applied easily in the office environment and do not cause space problems. These neck and upper extremity specific exercises are based on the stretching, strengthening, doing regular physical activity/fitness program/yoga/Tai Chi and/or Proprioceptive Neuromuscular Facilitation technique [4–24]. These exercises performed for periods ranging from approximately 1 month to 12 months are very effective in reducing the upper extremity and spine problems that are frequently seen in office workers [4–24]. Exercise training has been already recommended to be done for at least 6 weeks to show its effect. However, this period may seem too long for individuals working in an office environment to be sustained in parallel with office work. In the literature, the UEET that will show the effect quickly in a short time in office workers are still unknown. Therefore, studies are needed to determine practically, and optimally valid short-term exercises designed to prevent or treat musculoskeletal pain in office workers without disrupting working hours in the workplace.
In the current period, while the COVID-19 pandemic continues to have a negative impact on the health of all people who are in contact with the virus or not, remote telerehabilitation practices have gained momentum in all parts of society and consolidated their positions in the health healing applications. However, the effects of short-term UEET through telerehabilitation in the workplace of office workers who apply part or full-time teleworking system within the scope of restrictions and precautions during the COVID-19 pandemic are not yet known. Therefore, the present study was conducted to investigate the effectiveness of UEET on pain, MSD, physical activity, depression, anxiety, stress, and QOL in office workers.
Methods
Study design
Izmir Democracy University Non-Interventional Clinical Research Ethics Committee (date: November 24, 2021, number: 2021/15-01) approved the study. Informed consent forms were obtained from all office workers who were included in the study. Our study followed the principles of the Declaration of Helsinki between February 2022 and June 2022. This prospective, randomized controlled, parallel, and single-blind study was conducted in the Physiotherapy and Rehabilitation Departments of Izmir Democracy University and Sivas Cumhuriyet University. Simple random sampling numbers were used for allocation concealment via a randomization table automatically generated by a website (computerized sequence generation). An e-mail was sent to all office workers by the personnel departments of these universities, and those who responded positively to this e-mail were included flow list of the study. After, a telephone conversation was held with these office workers in order of e-mail arrival. During this conversation, the workers’ suitability for the study was decided and the office workers were informed about the study. Next, office workers met the inclusion criteria were remotely added to randomization list in order of telephone conversation. Office workers (n = 30) were blind to the study and randomly assigned to exercise (EG) (n = 15) and control (CG) (n = 15) groups. The office workers were blinded first, without being told which group they would exercise in. Considering both conditions related to the COVID-19 pandemic and the demands of office workers, all evaluations and exercise practices were carried out either face to face or via online systems. While an online form prepared on Microsoft Forms was used for distance assessments, an online video conference (Microsoft Teams) or video calls (WhatsApp) was preferred for distance exercise training.
Study population
Inclusion criteria for office workers were I) volunteering to participate in the study, II) being an adult aged between 18 and 65 years, III) having a smartphone/watch on which a pedometer application can be installed, and IV) working actively at a desk for at least three years and at least four hours a day. The exclusion criteria were I) having an infection, musculoskeletal system disease, or psychological, serious cardiac, orthopedic, or neurological disease, all of which may prevent exercise, II) doing regular heavy sports, III) being in quarantine for any reason, and/or IV) being pregnant.
Short-term UEET
The UEET program was applied to office workers under the supervision of experienced physiotherapists once a day for a total of at least 5–7 days for a week. The researchers have experience as physiotherapists for approximately 15 years and in active telerehabilitation interventions for approximately the last 5 years. As shown in Table 1, the UEET program consisted of warm-up and cool-down exercises, stretching, posture (Fig. 1), and resistance exercises with light-medium free weights (Fig. 2). These exercises were adjusted to office workers’ available times during the day. A session of the UEET program was implemented without interruption and lasted an average of 20–40 minutes per a day.
Upper extremity exercise training (UEET) program
Upper extremity exercise training (UEET) program
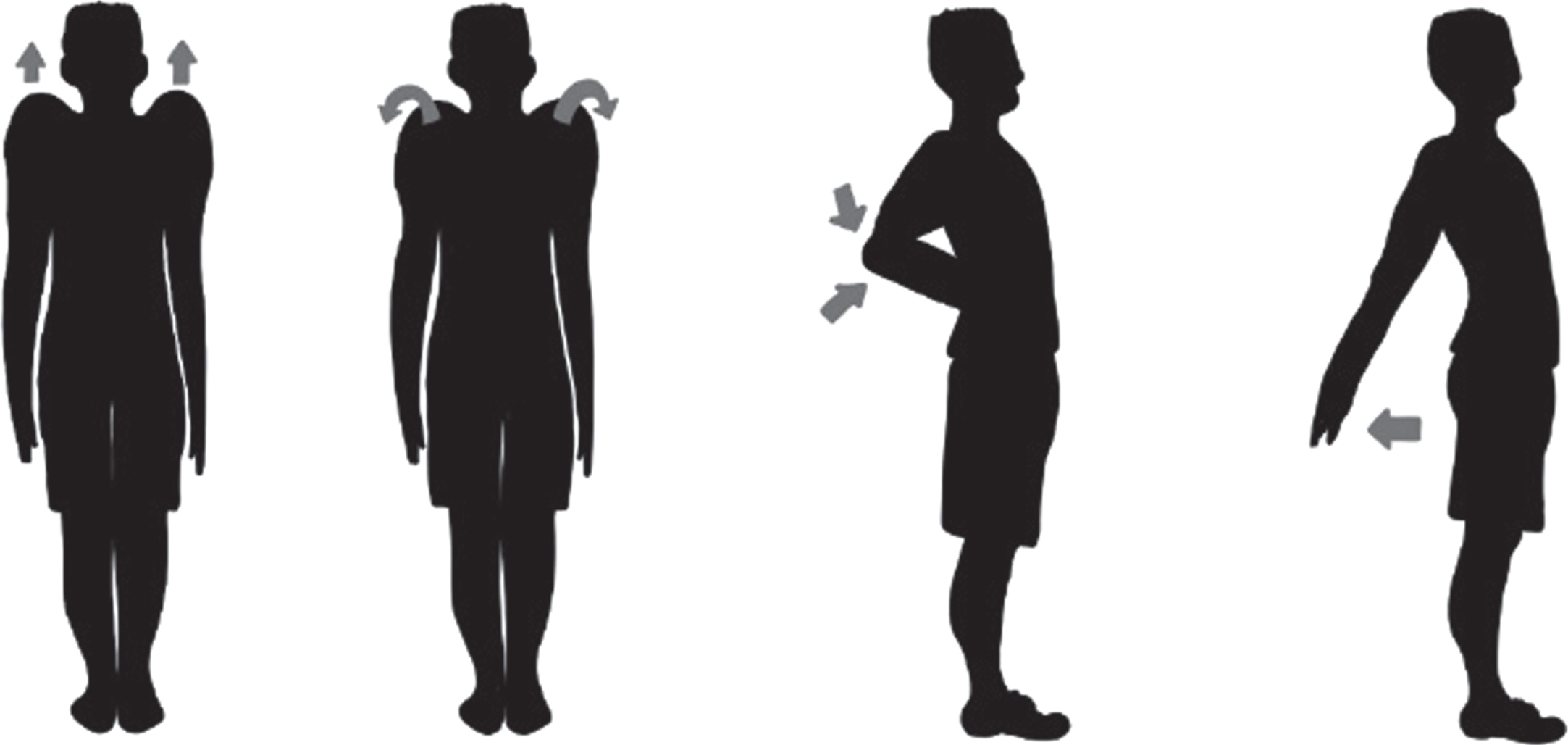
Posture exercises in the upper extremity exercise training program.
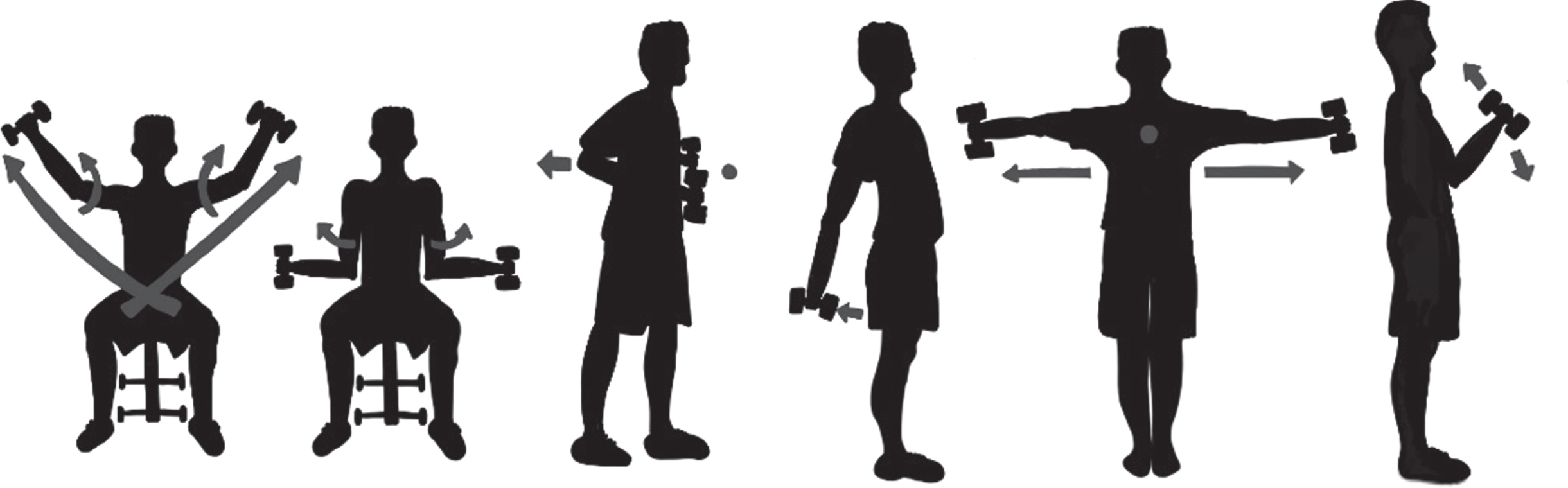
Resistance exercises with light-medium free weights in the upper extremity exercise training program.
After evaluations, EG both performed one-week UEET and followed walking advice while CG followed walking advice only for one week. Office workers in both groups were advised to walk for at least 4–5 days (taking at least 7500 steps/day or 8–10 rounds of at least 10 minutes/day) during the follow-up period. The UEET was similarly applied to office workers in CG after a one-week follow-up.
Measurements
Demographic characteristics (age, sex, height, weight, total working time in the profession, total working days per a week, daily working time at a desk, total rest time during working day, daily sleep duration, job, presence of exercise habits and chronic illness and COVID-19 history) of office workers were recorded. The pain, MSD, physical activity, depression, anxiety, stress, and QOL in the office workers were evaluated only twice, before, and immediately after the 1-week follow-up. It was also questioned whether there was any problem/adverse event during and after the exercises.
Assessment of daily step counts
Pedometer applications on mobile phones or watches of office workers were used to track their daily walks. Office workers were asked to report the total daily step counts to the researchers at the end of the day. Total daily step counts of office workers were recorded in their diaries.
Assessment of pain
The Numeric Rating Scale was used to measure pain severity at rest and during activity. The scores on this scale vary from 0 (no pain) to 10 (maximum pain) [25].
Assessment of MSD
Cornell Musculoskeletal Discomfort Questionnaire (CMDQ) was used to evaluate MSD felt in the last 1-week in office workers which is valid and reliable questionnaire [26, 27]. It measures the perception of discomfort/pain in 12 body regions, which include the shoulder, neck, back, low back, upper arm, forearm, wrist, hip, knee, foot, and upper and lower legs. The pain in each region is evaluated in three main sections: frequency, severity, and barriers to the ability to work. The responses of individuals to each section are scored using percentages or weighted scores [27]. The weighted scores were used in current study. The frequency of the pain was evaluated on a 5-point Likert scale (never, 1–2 times last week, 3–4 times last week, once every day, several times every day) with the weights of 0, 1.5, 3.5, 5, and 10, respectively. The severity of the pain was evaluated with a 3-point Likert scale (slightly uncomfortable, moderately uncomfortable, very uncomfortable) with the weights of 1, 2, and 3, respectively. Whether the pain interferes with working in the workplace is also evaluated with a 3-point Likert scale (not at all, slightly interfered, substantially interfered) with the weights of 1, 2, and 3, respectively [26, 27]. Finally, the score is obtained by multiplying the weighted scores corresponding to the individual’s answer to each section. The scores obtained for each region range between 0 and 90, and higher scores indicate higher levels of MSD [26].
Assessment of physical activity level
Walking (3.3 metabolic equivalents (METs)), moderate-intensity (4 METs), and vigorous (8 METs) physical activities in the last week were evaluated using a valid and reliable questionnaire, the International Physical Activity Questionnaire Short Form [28, 29]. “MET-min/week” scores were obtained by multiplying the minutes, days, and MET (which is set by convention at 3.5 milliliter of oxygen per kilogram per minute) values of each activity. According to these scores, office workers were classified as inactive, minimally active, and sufficiently active. The inactive office workers did not meet the requirements for being minimally or sufficiently active. Minimally active office workers met at least one of three criteria that are i) doing vigorous activity during ≥3 days/week and minimum of 20 minutes/day, ii) doing moderate-intensity activity during ≥5 days/week or minimum of 30 minutes/day walk and iii) doing combination of walking, moderate-intensity, or vigorous intensity activities for minimum of 600 MET-min/week during ≥5 days/week. Sufficiently active office workers met at least one of three criteria that are i) doing vigorous-intensity activity during minimum of 3 days/week for minimum of 1500 MET-min/week and ii) doing combination of walking, moderate-intensity, or vigorous activities during 7 days for minimum of 3000 MET-min/week [28, 29].
Assessments of depression, anxiety, and stress levels
The Depression Anxiety Stress Scale-21, which consists of stress, anxiety, and depression subscales, was used to evaluate the stress, anxiety, and depression levels of office workers [30]. This scale is valid and reliable [30]. A minimum of ‘0’ and a maximum of ‘21’ points can be obtained from each subscale. A score of ≥5 on the depression subscale, ≥4 on the anxiety subscale, or ≥8 on the stress subscale indicates that the individual has a related problem [30].
Assessment of QOL
QOL was evaluated with the Short Form-36, which consists of eight subscales (physical function, role limitations due to physical health and emotional problems, vitality, emotional well-being, social function, bodily pain, and general health) [31, 32]. This form is valid and reliable [32]. Each subscale is scored between 0 (poorer health) and 100 (better health) [31, 32].
Statistical analyses
The SPSS 15.0 software package was used in all analyses. To determine mean difference in psychological health scores between two independent groups [8] for an α value of 0.05 and a power of 95%, at least 7 office workers in EG and 9 office workers in CG were calculated through GPower program (G*Power 3.0.10 system, Franz Faul, Universität Kiel, Germany). However, considering the possibility of loss, it was planned to include at least 15 office workers for each group. The conformity of variables to normal distribution was determined by visual (histogram and probability graphs) and analytical methods (Kolmogorov-Smirnov/Shapiro-Wilk tests). Descriptive analyses were presented as i) frequency (n) and percent (%) values for the categorical variables, ii) median, interquartile range (IQR), and U values for the non-normally distributed variables, and iii) mean (x) and standard deviation (sd) values for the normally distributed variables. Student’s t test, Mann-Whitney U test, and Chi-square & Fisher tests were used to compare baseline normally distributed, non-normally distributed and categorical variables of the groups, respectively. The intra-group comparisons of pre- and post-exercise training non-normally distributed and normally distributed variables were made using the Wilcoxon test and Dependent samples t-test, respectively. The inter-group comparisons of pre- and post-exercise training non-normally distributed variables, which are delta changes, were made using the Mann-Whitney U test. Effect size d and post-hoc statistical powers were calculated for the outcomes and presented as 1-β. The effect size d values were calculated and interpreted as small (0.20), moderate (0.50) and large (>0.80) effect sizes. The probability of error was accepted as p < 0.05.
Results
Among the 37 office workers, 15 office workers in EG and 15 in CG completed interventions and follow-up (Fig. 3). The evaluation of 4 (26.67%) office workers in EG and 6 (40%) office workers in CG were done via the online form. The evaluation of 11 (73.33%) office workers in EG and 9 (60%) in CG was done face to face. Distance exercise practices of 3 (20%) office workers in EG and 6 (40%) office workers in CG were performed while face to face exercise practices of 12 (80%) in EG and 9 (60%) in CG was performed.
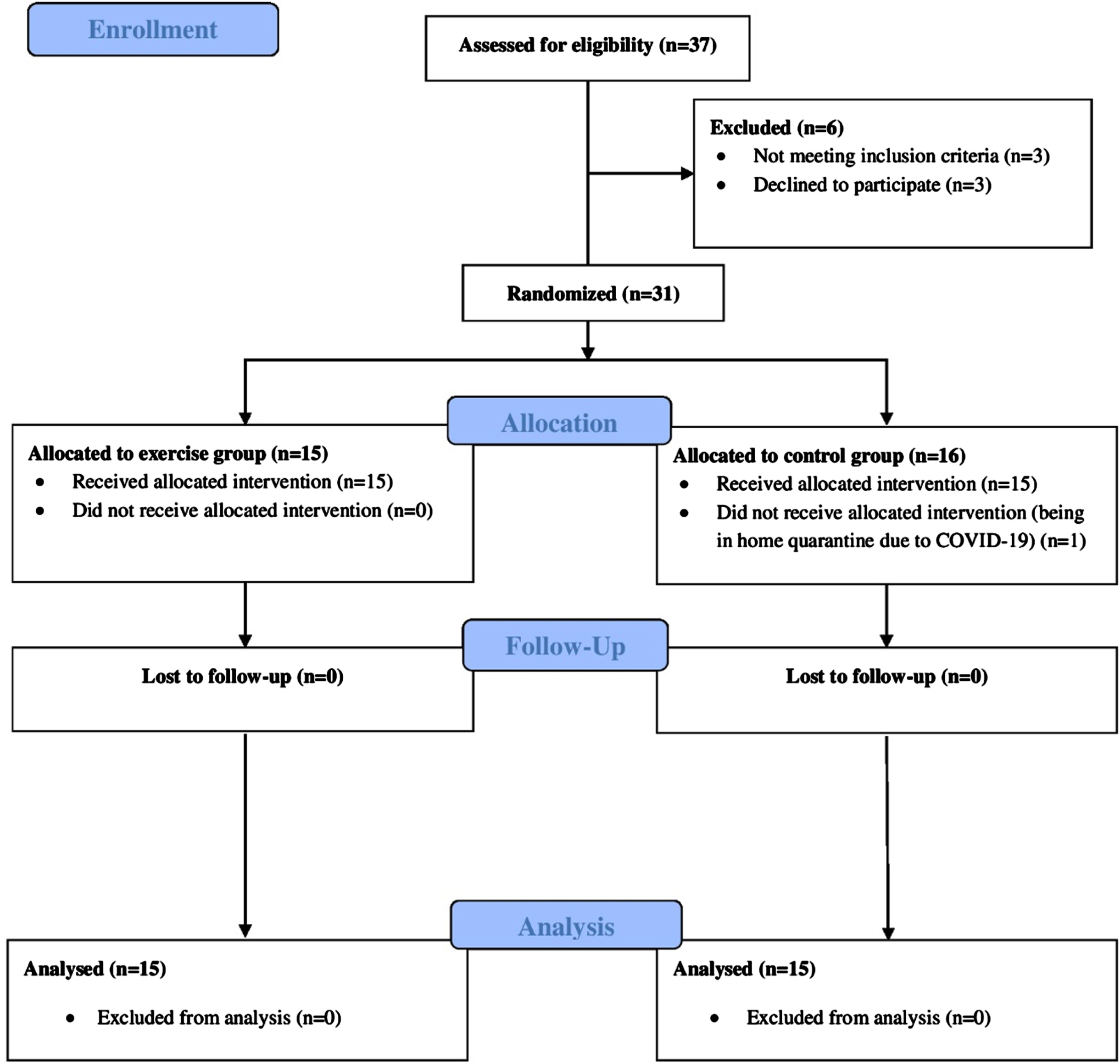
Consort flow diagram of the study.
The demographic characteristics of the groups were similar and presented in Table 2 (p > 0.05). Baseline values for each outcome of the groups before exercise training were also similar (p > 0.05). Baseline measurements also showed that 6 (40%) office workers in EG and 4 (26.7%) in CG had stress, 5 (33.3%) in EG and 1 (6.7%) in CG had anxiety, 4 (26.7%) in EG and 4 (26.7%) in CG had depression (p > 0.05). Moreover, 5 (33.3%) in EG and 6 (40%) in CG were inactive, 10 (66.7%) in EG and 7 (46.7%) in CG were minimally active, and 2 (13.3%) in CG were sufficiently active before follow-up (p > 0.05). Twelve (80%) office workers in EG and 6 (40%) in CG had neck pain (p < 0.05), and 12 (80%) in EG and 10 (66.7%) in CG had musculoskeletal pain (p > 0.05) at baseline.
Demographic characteristics of the groups
kg: kilogram, m: meter, BMI: body mass index, n: frequency, % : percent, COVID-19: Sars-Cov-2, EG: exercise group, CG: control group, x: mean, sd: standard deviation. Student’s t test, *p < 0.05; Chi-square test, #p < 0.05.
Comparison of the values within the groups before and after exercise training were presented in Table 3. In EG, CMDQ scores for neck, back, and low back regions, total CMDQ scores for vertebral column (neck + back + low back) and lower extremities (hip + upper legs + knees + lower legs + feet), and stress, anxiety, and depression scores significantly decreased while moderate-intensity physical activity, walking and total physical activity, physical functioning, vitality, emotional well-being, bodily pain, and general health scores significantly increased after one week (Fig. 4, Table 3, p < 0.05). No significant improvements were found in all parameters in CG after one week (Fig. 4, Table 3, p > 0.05).
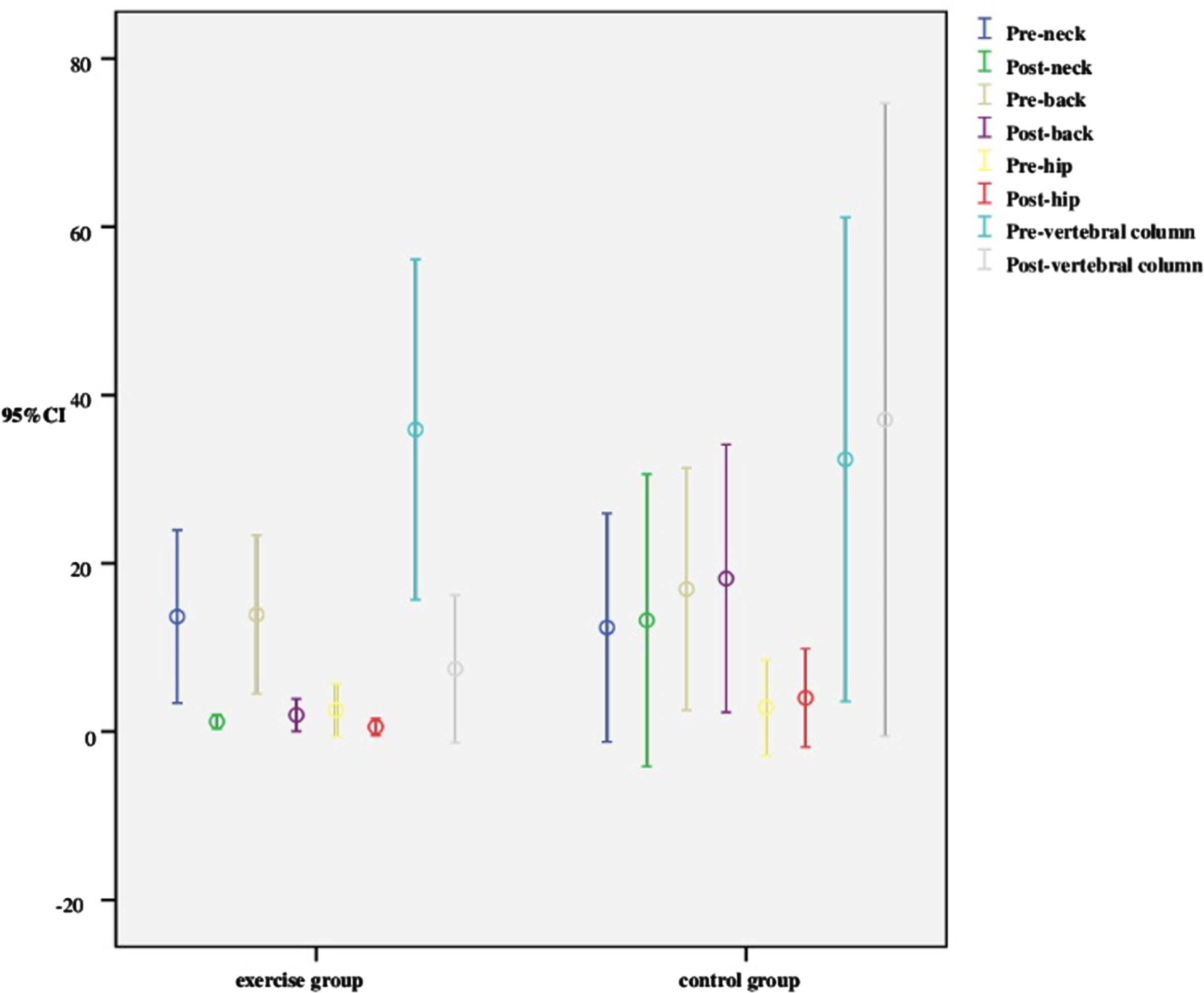
Comparison of the musculoskeletal discomfort scores within the groups before and after exercise training.
Comparison of the values within the groups before and after exercise training
NRS: Numeric Rating Scale, CMDQ: Cornell musculoskeletal discomfort questionnaire, IPAQ: International Physical Activity Questionnaire, MET: metabolic equivalent, min Minute, d: day, wk: week, DASS-21: Depression Anxiety Stress Scale-21, SF-36: Short Form-36, EG: exercise group, CG: control group, x: mean, sd: standard deviation, IQR: interquartile range, U: U value, p: p value. Wilcoxon test, *p < 0.05; Dependent samples t-test, #p < 0.05.
Comparison of the intra-group difference values between the groups before and after exercise training were presented in Table 4. After one-week, total step counts and vigorous physical activity, moderate-intensity physical activity (effect size d = 1.4, 1-β= 0.97), walking (effect size d = 1, 1-β= 0.76), total physical activity, physical functioning, and bodily pain (effect size d = 1.1, 1-β= 0.83) scores significantly increased in EG compared to the scores in CG (Table 4, p < 0.05). On the other hand, CMDQ scores for the neck, back, and hip regions, total CMDQ scores for the vertebral column (neck + back + low back) (effect size d = 1.2, 1-β= 0.91) and lower extremities (hip + upper legs + knees + lower legs + feet), anxiety (effect size d = 0.9, 1-β= 0.74), and depression scores significantly decreased in EG compared to the scores in CG after one week (Table 4, p < 0.05). No adverse event or complication developed in office workers following UEET and walking advice.
Comparison of the intra-group difference values between the groups before and after exercise training
NRS: Numeric Rating Scale, CMDQ: Cornell musculoskeletal discomfort questionnaire, IPAQ: International Physical Activity Questionnaire, MET: Metabolic equivalent, min Minute, d: Day, wk: Week, DASS-21: Depression Anxiety Stress Scale-21, SF-36: Short Form-36, EG: exercise group, CG: control group, x: mean, sd: standard deviation, IQR: interquartile range, U: U value, p: p value. Mann-Whitney U test, *p < 0.05.
Progressive short-term UEET substantially improved step counts, musculoskeletal disorders in neck, back, and hip regions, vertebral column (power: 91%) and lower extremities, physical activity scores (power: 97%), anxiety, depression, physical functioning, and bodily pain (power: 83%) scores in office workers during the prolonged COVID-19 pandemic. These results were demonstrated with moderate-large effect sizes and high-power in the present study.
Various exercise training programs have positive effects on especially pain and QOL in office workers with or without neck pain [4–21]. These programs generally include neck/shoulder resistance exercise, endurance, and general whole-body exercises [4, 23], posture correction, ergonomics arrangements, and stretching exercises for neck and shoulder [5, 10]. Other types of exercise are regular physical activity [8], online aerobic and strength training [9], resistance exercise breaks [12], and multimodal physiotherapy programs [14, 16], Tai Chi [15], and lumbar stabilization [21]. The duration of these exercises also varies from at least 4 weeks to 1 year [4–6, 21–23] in contrast to the short exercise time in our study. As seen, the training programs basically focus on strengthening and stretching exercises. These exercises enable office workers to correct posture and joint positions within biomechanical limits, strengthen the muscles, decrease the intensity of musculoskeletal system complaints in the neck, shoulder, and back regions, and reduce postural overload [9, 21]. Our results with high power showed that even a 1-week exercise program including posture, strengthening, and stretching had more acute curative impacts on pain in the neck, back, and hip regions and QOL compared to controls, which is consistent with the results of previous studies [4–21]. It is a remarkable result that our program reduced pain scores, especially in the hip region. This reduction can be attributed to the fact that having a more upright posture with strengthening the muscles and taking regular steps increases joint mobility, regulates blood circulation, and has positive effects on the other cardiovascular, metabolic, and immune systems [33, 34]. Moreover, it was also shown in the current study that short-term UEET and physical activity recommendations increased weekly step counts and physical activity levels and decreased anxiety and depression of office workers in EG compared to the CG, which was given only physical activity advice. The current study was conducted during the prolonged COVID-19 pandemic and partial restrictions related to the pandemic. The fact that office workers increased their walking time even for one week may have shown some benefits, which is consistent with the results of another study showing improved anxiety, step count, physical activity level, and QOL after 4-week physical activity counseling by increasing daily steps [35]. For these reasons, we recommend office workers who cannot spare time for long exercise and sports activities to take a break for simple exercises including posture, strengthening, and stretching during working hours and to increase their physical activities through ten-minute walks every hour.
Pain in the parts of the body, including the neck, back, low back, and shoulders due to prolonged sitting and physical inactivity, is the most common musculoskeletal disorder worldwide and has both socio-economic and personal consequences [24]. As supported by our results, doing regular exercises and adequate physical activity are effective ways to reduce musculoskeletal pain and disorders among office workers [10, 24]. Until now, the positive effects of exercise training on neck functions [5], general occupational satisfaction [8], mobility, balance, endurance capacity, muscle strength, mood and fatigue [9, 15–17], postural overload [10], mental fatigue [12], and ability to work [22, 23] as well as pain and QOL [4–9, 16–20] have been proven in previous studies, which is compatible with our study. Consistent with our results, it was indicated in a study that office workers who did regular physical activities (running, fitness, yoga, etc.) for at least 3 days/week, 1 hour/day, and a total of 8 weeks had better QOL and general occupational satisfaction than those who did not [8]. Another study demonstrated that resistance exercise breaks which were performed as 15 repetitions/set, 2 sets/session, 5 sessions/day per hour, and a total of 14 days alleviated mental fatigue in office workers and were easily accepted by the workers [12]. These resistance exercise breaks consisted of major lower and upper extremity muscle group exercises [12]. Considering the intense work schedule and often long sitting hours, our study showed that it was a unique opportunity to achieve all these gains regarding pain, step count, mood, physical activity level, and QOL through 20–40-minute exercise breaks at the workplace in only one week. These exercises can be easily performed at the desk or standing in the workplace. Therefore, our exercise program, which was designed to target upper extremity major muscle groups (warm-up exercises, stretching, posture, resistance exercises with light-medium free weights, and cool-down), should be performed as an exercise break at the workplace.
On the other hand, our 1-week exercise program was not enough to decrease overall pain intensity, musculoskeletal disorders in other body regions, and stress and to increase the scores of other subscales of QOL in office workers. Contrary to our findings, it was found by a one-year exercise follow-up study that exercise training decreased the number of other pain regions of office workers with neck pain [4]. This can be attributed to the reduction of pain at the hormonal level through the release of endorphins following long-term exercise training [36]. Therefore, after acute gains are obtained with short-term exercises in the office environment and the employees get accustomed to doing exercise, office workers may be easily directed to longer-term programs such as Pilates, yoga, Tai Chi, aerobic exercises, etc. [8, 15].
The COVID-19 pandemic and the resulting mandatory restrictions were a serious barrier preventing individuals, especially those with chronic diseases from participating in face-to-face rehabilitation in hospitals or other clinics [37]. For this reason, telemonitoring and telerehabilitation applications, and even hybrid modeling, have been rising star in response to the COVID-19 pandemic, which causes rapidly changing dynamic conditions in social life [38]. Consistent with the hybrid application and positive results obtained in our study, Satar et al. has showed that the hybrid model of telerehabilitation enables both a detailed measurement and efficient and safe exercise intervention program even in high workloads in individuals with post-COVID-19 [38]. Another study has similarly demonstrated that telerehabilitation provides improvement in patient satisfaction and physical activity level in cancer survivors. It has become an effective method that can be applied safely during the COVID-19 period [39]. Moreover, Bucki et al has also reported that telehealth evaluation and telerehabilitation interventions may be reliable and effective for some musculoskeletal disorders during and after COVID-19 and mandatory restrictions which is consistent with our findings [37]. Although telerehabilitation appears to be such an effective medical evaluation and treatment method that reflects the digital age, studies showing the effectiveness of various applications with changes in duration and frequency of type and in various populations are still very limited. In this context, our study is very valuable in that it shows the effectiveness of 1-week UEET in office workers and that exercises implemented through a hybrid telerehabilitation adapted to the changing dynamics of COVID-19 are effective, feasible and safe. Moreover, it can be seen that this study is the first in the literature, to our knowledge.
Limitations
A limitation of this study is including the results of office workers from two centers. Another limitation is that more comprehensive telehealth applications could not be provided due to the inadequate facilities of our center. Physical activity levels of the office workers were also evaluated by self-report and therefore this situation is subject to recall bias. In our study, we tried to prevent bias by not informing the participants in which group they would be included. However, instead of single-blind planning (this may be another limitation), 2- or 3-blind study planning may be preferred in future studies.
Conclusion
Under the challenging conditions of the protracted COVID-19 pandemic process, this prospective, single-blind, and randomized controlled trial proved the effectiveness of progressive 1-week UEET and physical activity advice in step counts, musculoskeletal pain in the neck, back, and hip regions, anxiety, depression, and QOL in office workers. Short-term exercise practices and increasing the number of steps provided beneficial gains for office workers. In future studies, there is a need to examine the effectiveness of these exercises that are given as a home program or evaluate the short-term effects of different exercise training programs.
Recommendations
Employers can provide opportunities such as mini exercise stations/room including a treadmill, a stationary bike, and free weights for mini exercise breaks in their workplaces. Thus, office workers who cannot spare time for long exercise may take short breaks during working hours for simple exercises including posture, strengthening, and stretching. In this way, complaints of pain and other discomfort observed in office workers can be reduced or prevented. Employers can offer deals such as gym membership, membership discounts, or promotions to office workers. While this increases office workers’ motivation, productivity, and adherence to exercise in the long-term, it can reduce office workers’ use of reports due to their complaints or hospital visits. Taking ten-minute steps every hour or walking during breaks is an easy way to increase physical activity and the health benefits that come with it. It can be applied anytime and anywhere, during or outside work hours. UEET, which especially targets the upper extremity large muscle groups, should be performed as a whole or in parts as an exercise break at work. At the end of a maximum of 1 hour of desk work, an exercise reminder with artificial intelligence/computer program can be activated which can remind and show the office worker to move and do short exercises.
Ethical approval
Izmir Democracy University Non-Interventional Clinical Research Ethics Committee (date: 24/11/2021, number: 2021/15-01) approved the study.
Informed consent
Informed consent forms were obtained from all office workers who were included in the study.
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
We would like to acknowledge all office workers and families who participated in our study.
Author contributions
GÜLŞAH BARĞI: Conceptualization, Methodology, Data collection, Formal analysis and investigation, Writing –original draft preparation, Writing –review and editing, Funding acquisition, Resources, Supervision.
SİNEM SUNER-KEKLİK: Data collection, Formal analysis and investigation, Writing –original draft preparation, Writing –review and editing, Funding acquisition, Resources.
Funding
The authors report no funding.
Clinical trial registration
Clinical trial ID: ACTRN12622000023752.