
Abstract
BACKGROUND:
Operating room nurses (ORNs) who directly deal with the treatment and care of COVID-19 patients during the pandemic are at risk in terms of psychological stress and other mental health problems.
OBJECTIVE:
The aim of the study was to compare the anxiety and depression levels of ORNs working in different countries in the COVID-19 outbreak, and to determine the predictors and the difference between countries.
METHODS:
This was a descriptive and cross-sectional study. Data were collected online using a google form between February 2021-February 2022. The universe of the research is nurses who are members of national Perioperative Nurses Association (USA, Türkiye, Australia, England, India, Israel) and 1127 ORNs participated the study. In multivariate analysis, independent predictors of anxiety and depression status were examined by binary logistic regression analysis.
RESULTS:
The rate of anxiety is 5.46 times higher in nurses in the USA, 5.07 times higher among nurses in Australia, and 4.49 times higher for nurses in England. It was determined that the rate of depression in ORNs working in Türkiye was 5.97 times higher. It was found that the rate of depression is 1.59 times higher in ORNs living away from the family after care of COVID-19 patient.
CONCLUSION:
Despite some differences between countries in terms of health system, patient potential, economic and the opportunities offered, generally high levels of anxiety and/or depression indicate that all ORNs need urgent support. Identifying risk factors will help recognize anxiety and depression in ORNs and take measures to protect their mental health during the pandemic.
Introduction
COVID-19 first appeared in Wuhan, China, in late 2019 and it soon spread throughout the world. On March 11, 2020, the day the World Health Organization (WHO) designated it a pandemic and the first case in Türkiye was reported [1, 2]. As of February 14, 2023, it was reported that 17,042,722 COVID-19 cases were seen in Türkiye and 101,492 people lost their lives [3]. Healthcare workers who directly deal with the treatment and care of COVID-19 patients during the pandemic are at risk in terms of psychological stress and other mental health problems. The ever-increasing number of cases, increasing workload, lack of personal protective equipment, lack of medications and insufficient support contribute to the increased mental burden of healthcare workers. Previous studies indicate that the psychology of healthcare workers was negatively affected in the 2003 SARS epidemic [4–6]. Studies have indicated that nurses fear infection to themselves, their families, friends, and colleagues, feel uncertainty and stigma, are unwilling to work and even consider resigning, and in addition, experience high levels of stress, anxiety, and depression, which may have long-term psychological consequences [4–6]. Similar problems arise with the mental health, psychological adjustment and recovery of healthcare professionals treating and caring for COVID-19 patients.
Operating rooms are areas where confirmed and potential COVID-19 patients are operated on, and also involve the use of high-risk equipment (surgical instruments, gases, etc.) [7, 8]. The risk of transmission is increased due to the closed and narrow working area [9, 10]. It has also been shown that COVID-19 can lead to severe hospital infections, threatening the surgical staff [7]. Health professionals experience anxiety due to the sudden outbreak of the pandemic, its rapid spread and lack of information about exposure to and treatment for the disease. The increase in time spent for patients, the lack of materials and personal protective equipment, the shortage of human resources, equipment preparation, increased work intensity with additional precautions, and the obligation to distance themselves from loved ones negatively affect the emotional state of surgical nurses who work intensively [11]. With the increase in the number of patients diagnosed with COVID-19 in Türkiye, it has been decided by the Ministry of Health to postpone emergency surgeries and to convert many operating rooms to intensive care units. In this context, some of the nurses working in the operating room started to work in the intensive care unit [12]. Each country has taken different importance in accordance with its own conditions. Due to all these changes, increased patient load and operating room-specific conditions, operating room nurses are considered to be a risky group in terms of psychological symptoms in the pandemic. Since the precautions, conditions, and rules taken due to the pandemic in each country are different, it is crucial to determine the anxiety and depression experienced by the operating room nurses working in different countries during the pandemic and the factors affecting it. With this study, it is aimed to reveal the differences between countries and to determine the predictor factors that affect the anxiety and depression levels of operating room nurses. In the literature, no study has focused on the psychological effects on operating room nurses, such as anxiety and depression during the long COVID-19 pandemic process. In this study, it was aimed to compare the anxiety and depression levels of operating room nurses working in different countries in the COVID-19 outbreak, and determine the predictors, and find the difference between countries.
Methods
Design, setting and sample
This study employed descriptive and cross-sectional study and the STROBE checklist. Data was collected with a google form between February 2021-February 2022. The data were collected from members of the Perioperative Nurses Association of each country willing to participate in the study. The criteria for including operating room nurses in the research sample included the following: being at least 18 years of age, and working in the operating room (USA, Türkiye, Australia, England, India, and Israel).
The universe of the research is members of national Perioperative Nurses Association for USA (n = 40,000), England (8,000), Australia (n = 5,000), Türkiye (n = 1,683), Israel (n = 1,000) and India (n = 250). In these six countries, there are a total of 55,933 nurses who are members of perioperative nursing associations. The number of samples was calculated using the G-power (http://www.gpower.hhu.de/) program. In the calculation made with a power of 0.80 and a p value of 0.05, the required sample number was determined as n = 1,044. Stratified random sampling method was used to determine how many nurses will be recruited from each country. The research sample was planned to consist of at least 18 nurses from Israel, 31 from Türkiye, 93 from Australia, 7 from India, 746 from the United States, and 150 from England, according to the calculations. Although the number of samples to be included from India was calculated as 7 and from Israel as 18, it was planned to include at least 30 nurses in the sample in order to provide the parametric criteria. A total of 1127 operating room nurses participated in the study, 462 from the USA, 255 from Türkiye, 230 from Australia, 79 from England, 53 from India and 30 from Israel. Since the USA and England were below the planned number, post hoc power analysis was performed and data collection was not continued as the power of the study increased to 0.96 and this study examined the situation during the pandemic.
Data collection
The questionnaire was sent online to the association members.
The personal information form
This form was created by the researchers by examining the literature on the subject. It consists of 9 personal questions, including age, profession, education level, working time, and number of children.
The practice and attitude survey of operating room nurses towards the COVID-19 outbreak
This was created by the researchers by examining the literature on the subject, and it contains a total of 16 questions. Questions include whether operating room nurses were involved in primary care in the COVID-19 outbreak, number of hours worked, and whether they had contracted COVID-19.
Hospital anxiety and depression scale (HADS)
This was developed in England in 1983 by Zigmond and Snaith [13]. The scale consists of 14 items, 7 of which investigate depression and the remaining 7 focused on anxiety symptoms. The aim of the scale is not to make a diagnosis, but to determine the risk group via a brief screening anxiety and depression. The cut-off score of the depression and anxiety subscales of the scale is≥8. Despite the word ‘hospital’ in its title, this scale can also be used in research in the field or in primary care. HADS has also been proven to be a useful assessment tool and gives the score ranges in a way that minimizes false positive and false negative results. HADS version for Türkiye was developed by Aydemir et al. The validity of the scale was tested for language, content, structure, and co-validity methods. Factor analysis was applied for construct validity, and two factors similar to the original scale were obtained. The first factor relates to anxiety symptoms, and the second, to depression symptoms. In the co-validity method, the correlation coefficient between the anxiety subscale and the Trait Anxiety Scale was 0.75, and the correlation coefficient between the depression subscale and the Beck Depression Scale was 0.72. In the reliability study, it was found that the internal consistency Cronbach Alpha coefficient varied between 0.85 for the anxiety subscale, 0.77 for the depression subscale, item total score correlation coefficients between 0.81 and 0.85 for the anxiety subscale, and 0.73 and 0.77 for the depression subscale. At the split half reliability, r = 0.85 for the anxiety subscale and r = 0.80 for the depression subscale. As a result, the reliability and validity of Turkish form of HADS was established [14].
The form was developed in English and is used in USA and Australia. The validity and reliability study of the Hospital Anxiety and Depression Scale in India was conducted by Thomas et al. In this study, internal consistency Cronbach Alpha coefficient was determined as 0.81 for the anxiety subscale, 0.71 for the depression subscale, and 0.85 for the whole scale. The validity and reliability study of the scale in Israel was conducted by Buria et al., who found an internal consistency Cronbach Alpha coefficient of 0.86 for the anxiety subscale and of 0.89 for the depression subscale.
Data were collected online with Google form between February 2021-February 2022. Researchers from 6 countries contacted the participants from the official social media account of their perioperative nurses association and by e-mail, made announcements, provided information about the research, and collected data from volunteers through data collection tools and forms.
Data analysis
The data was evaluated using the SPSS 23.0 package program. Independent group t-test and chi-square tests were used to determine whether there was a statistically significant difference between operating room nurses’ sociodemographic and application towards COVID-19, their attitudes and anxiety and depression. In multivariate analysis, independent predictors of anxiety and depression status were examined using binary logistic regression analysis with variables determined to be statistically significant in previous analyses.
The predictive role of nurses’ sociodemographic and COVID-19-related characteristics on anxiety was examined by a logistic regression model. This model includes the following: country, age, years of work in the profession, years of work in the operating room, number of children, presence of incentive system for nurses during COVID-19, COVID-19 infection status, compulsory vaccination, difficulty in accessing personal protective equipment, views on how effective personal protective equipment is in preventing the virus, level of anxiety about getting sick with COVID-19, level of anxiety about infecting loved ones with COVID-19, losing a loved one due to COVID-19, working hours, opportunities for rest, the degree of feeling valued in the institution, and the trust in the workplace (Fig. 1). The model fit was checked by the Hosmer-Lemeshow test. If the p-value in the model is greater than 0.05, the predictive value of the model is considered high. In this research, the Hosmer-Lemeshow test p-value was determined as 0.224. Therefore, it is seen that the predictive value of the model is high. The significance level was accepted as p < 0.05.
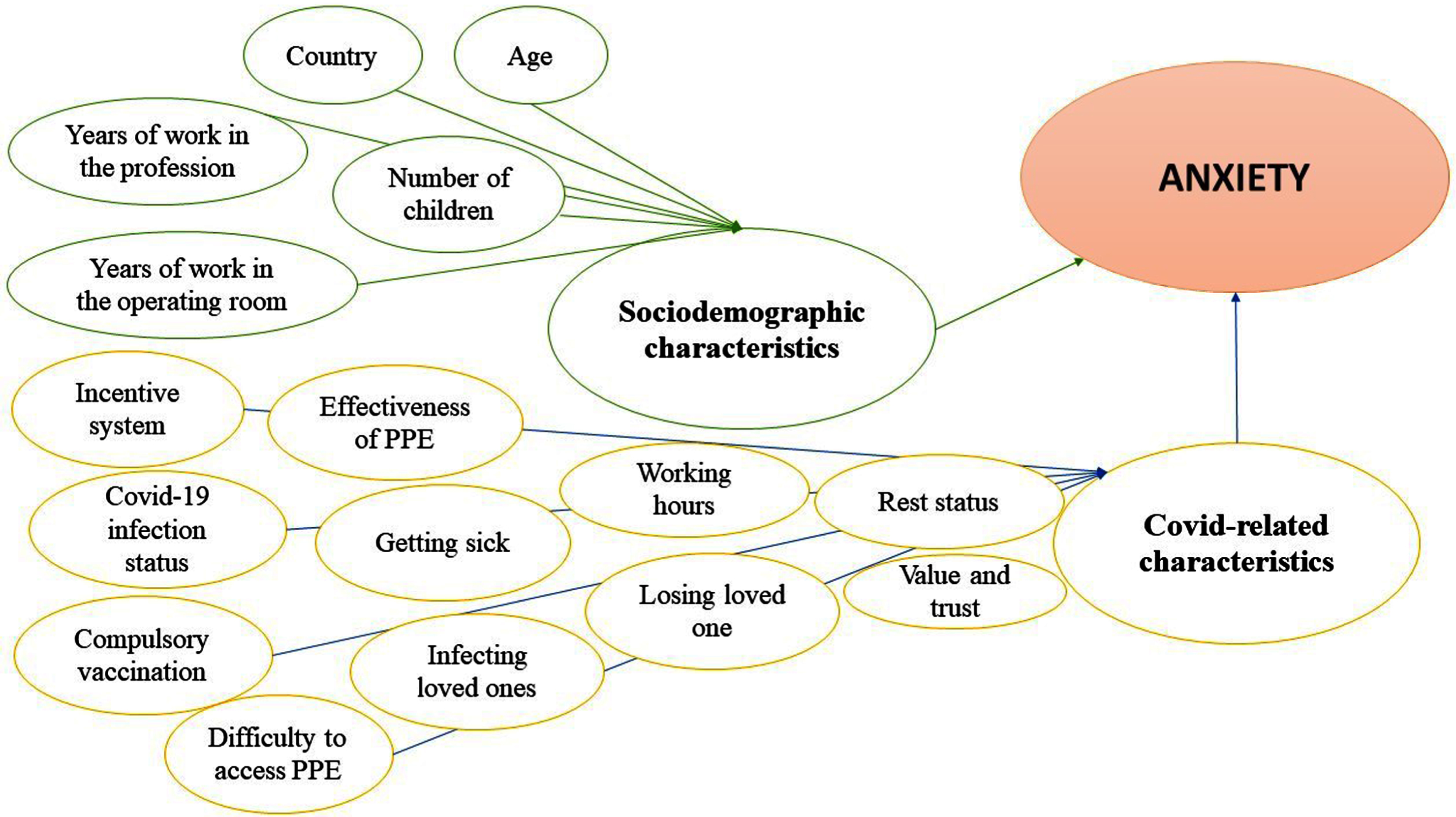
Logistic regression model for anxiety.
The predictive role of nurses’ sociodemographic and COVID-related characteristics on depression was examined by logistic regression model. This model includes the following: country, age, years of work in the profession, years of work in the operating room, the unit assigned after the change, the status of taking part in the surgery of a possible/infected patient with COVID-19, the status of training to prevent COVID-19 transmission when dealing with a COVID-19 positive patient, status of living away from family, daily working hours, weekly working hours, number of shifts per month, presence of incentive system for nurses during COVID-19, views on COVID-19 vaccines, COVID-19 vaccine status, challenges in accessing personal protective equipment, views on how effective the equipment is in preventing the virus, level of anxiety about getting sick with COVID-19, level of anxiety about infecting loved ones with COVID-19, losing a loved one due to COVID-19, working hours, opportunities to rest, the degree of feeling valued in the institution, and the trust in the workplace (Fig. 2). The model fit was checked by the Hosmer-Lemeshow test. If the p-value in the model is greater than 0.05, the predictive value of the model is considered high. In this research, the Hosmer-Lemeshow test p-value was determined as 0.234. Therefore, it is seen that the predictive value of the model is high. The significance level was accepted as p < 0.05.
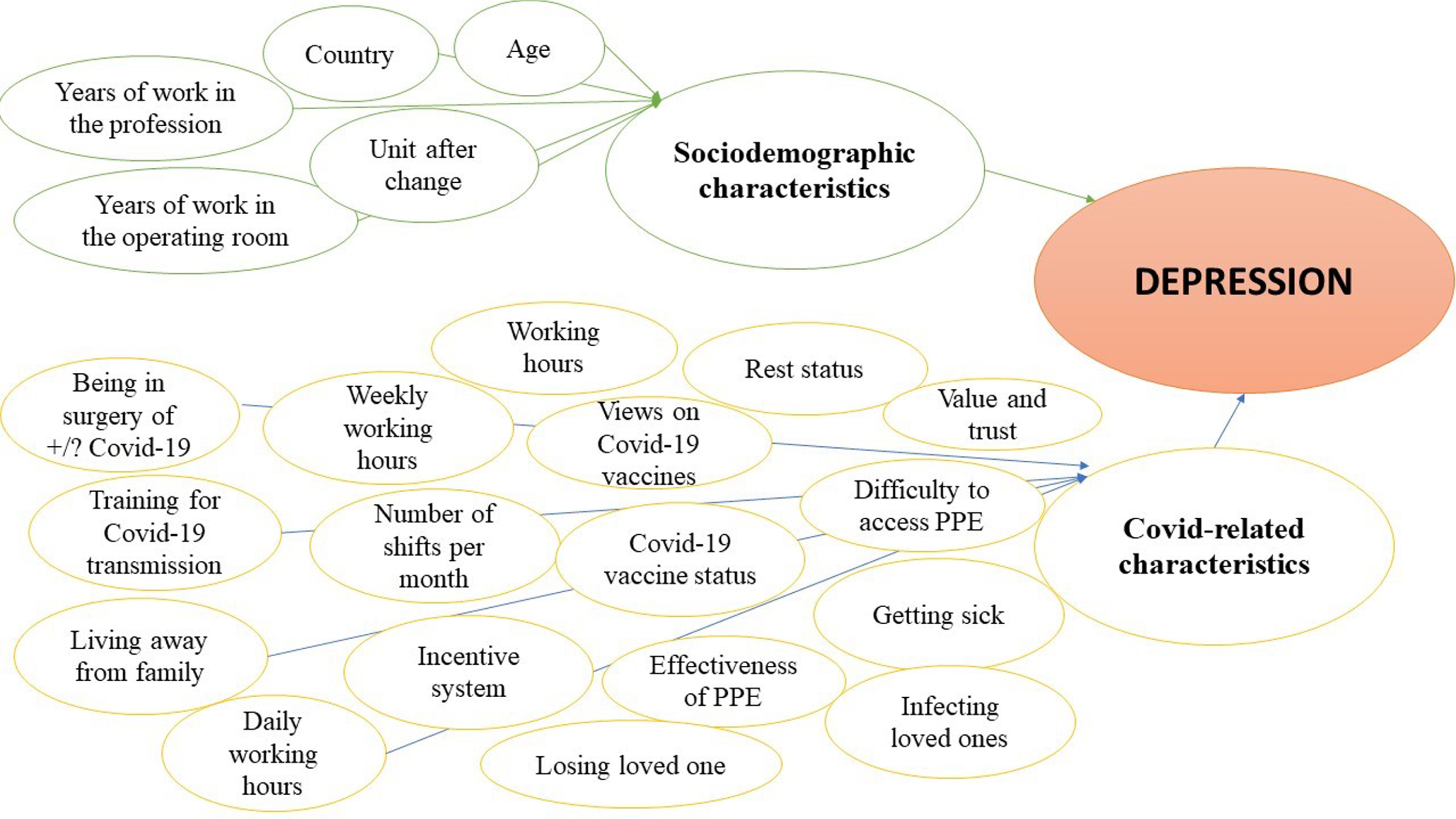
Logistic regression model for depression.
Consent was received from the university ethics committee and written permission was received from the associations. The nurses participated voluntarily in this study and were informed that the data collected would be used for scientific purposes, and that no personal data would be published in any of the scientific reports or articles. The participants were asked to read the informed voluntary consent and click on the checkbox indicating agreement with the statement “I fully agree to participate in this study”.
Results
The mean age of 1127 operating room nurses participating in the study was 43.78 + 11.73 (min = 20, max = 77) and 41% (n = 462) of the nurses were in the USA, 22.6% (n = 255) in Türkiye, 20.4% (230) in Australia, 7% in England (n = 79), 4.7% in India (n = 53), and 2.7% in Israel (n = 30). The participants’ average number of working years in the operating room was 15.21 + 11.52, and 30.3% were working in a private hospital and 27.6% in a state hospital. 68.8% of the operating room nurses were married, and 33.3% had 2 children. 12.4% of the nurses had dependent children, 10% had dependents over the age of 65 or with a disability, and 21.5% had received support assistance in the care of their children. 80.3% of the operating room nurses had taken part in the surgery of a suspected or diagnosed patient with COVID-19, and 80.5% had received training on COVID-19 contamination prevention. The average number of working hours of the nurses was 9.33 + 4.04 (min = 6-max = 12) and the average number of weekly working hours was 43.93 + 18.63 (min = 30–max = 60). 28% of the participants stated that COVID-19 is accepted as an occupational disease in their country, 22.8% had caught COVID-19 and 10.9% of these self-isolated for 10 days. 18.3% of the operating room nurses participated in the Phase 3 COVID-19 vaccine study, 87.4% of them were vaccinated (2 doses), and 41.4% of the participants were vaccinated against their will 84.2% of the operating room nurses believed that they could easily access PPE in their institution, 65.1% believed that PPE was adequate protection, while 26.4% believed that sometimes it did not protect adequately. While 50.7% of the nurses were slightly concerned about transmitting COVID-19, 33.5% had high concerns and 34.3% had very high concerns about infecting a loved one. 44.2% of the operating room nurses stated that they had rest periods, 39.6% stated that they had a high level of confidence that their institution could manage the COVID-19 pandemic, while 37.8% stated that they had some confidence. The mean score of feeling valued by the nurses’ institutions was determined as 5.63 + 2.59 (min = 0–max = 10).
It was determined that 63% (n = 710) of the participating nurses had higher anxiety scores than the cut-off point. Of the operating room nurses experiencing anxiety, 45.2% were in the USA and 23.2%, in Türkiye. It was determined that 42.1% of the nurses had higher depression scores than the cut-off point. Of this group of nurses, 38.1% worked in the USA, 37.9% in Türkiye, and 13.9% in Australia.
It was determined that the anxiety level of the operating room nurses changed statistically significantly according to the following variables: country, age, years of work, years of work in the operating room, the unit assigned after the change, when dealing with a patient with a COVID-19 diagnosis, status of living away from family, daily working hours, weekly working hours, number of shifts per month, presence of incentive system for nurses during COVID-19, COVID-19 vaccine status, challenges in accessing personal protective equipment, views on how effective the equipment is in preventing the virus, level of anxiety about getting sick with COVID-19, level of anxiety about infecting loved ones with COVID-19, losing a loved one due to COVID-19, working hours, opportunities to rest, the degree of feeling valued in the institution, and the trust in the workplace (Table 1).
Anxiety and Depression Status of Nurses by Socio-Demographical and COVID-19-related Characteristics (n = 1.109)
Anxiety and Depression Status of Nurses by Socio-Demographical and COVID-19-related Characteristics (n = 1.109)
*Fisher **Yates.
The risk factors affecting the presence of anxiety in nurses included in the study according to binary logistic regression analysis are shown in Table 2. It was shown that the created anxiety model can predict the state of anxiety with 71.9% accuracy using these variables. The rate of anxiety is 5.46 times higher in USA nurses, 5.07 times higher among Australian nurses, and 4.49 times higher for English nurses. It was determined that the anxiety level was 1.77 times higher in nurses with a little anxiety about getting sick with COVID-19, and 2.36 times more in those with a statistically significant level of anxiety. The anxiety level is 1.75 times higher in those with a statistically significant level of anxiety about infecting loved ones, and 3.44 times higher in those with an excessive level of anxiety. Anxiety was found to be 1.58 times higher in nurses whose working hours partially allowed rest (Table 2).
Distribution of Risk Factors Affecting the Presence of Anxiety in Nurses
Nagelkerke R2:.247, p < 0.001. The rate at which the model correctly predicts the presence of anxiety: 71.9%.
Table 3 shows the risk factors affecting the presence of depression in the nurses included in the study according to binary logistic regression analysis. The depression model created was found to be able to predict the incidence of depression correctly at a rate of 71.5% using these variables. The rate of depression in nurses working in Türkiye was 5.97 times higher. It was found that the rate of depression is 1.59 times higher in nurses living away from the family after care of a COVID-19 patient. It was seen that the risk of depression is 1.70 times higher in nurses who have a statistically significant level of anxiety about getting sick with COVID-19, and 2.35 times higher in those with an excessive level of anxiety. The risk of depression is 2.07 higher in nurses with an excessively high level of anxiety about infecting loved ones (Table 3).
Distribution of Risk Factors Affecting the Presence of Depression in Nurses
Nagelkerke R2: 0.314, p < 0.001. The rate at which the model correctly predicts the presence of depression: 71.5%.
In our study, the anxiety predictors of operating room nurses were found as follows: working in Australia, England, and the USA; worrying about contracting COVID-19 and infecting their loved ones; inadequate time to rest due to intensive working hours; low level of feeling valuable in the institution; and low confidence in their institution for the management of the COVID-19 pandemic. On the other hand, depression predictors were determined as follows: being an operating room nurse in Türkiye; being away from the family (isolation) after providing care for patients with COVID-19; worrying about contracting COVID-19 and infecting their loved ones; a low degree of feeling valuable in the institution.
The anxiety levels of 63% of the operating room nurse participants and the depression levels of 42.1% were above the cut-off point. In a meta-analysis, it was stated that anxiety seen in healthcare workers in the COVID-19 pandemic ranged from 8 to 91%, and depression, from 12 to 87% [17]. In a study with results similar to those of our study, 57.3% of the operating room workers were reported to have experienced anxiety and 36.9%, depression [18]. Our study results showed anxiety and depression levels similar to those reported in studies conducted in the early COVID-19 period [17, 18]. In a study conducted by Tamrakar et al. with nurses working in COVID-19 intensive care unit, anxiety and depression levels were 36.5% and 21.2%, respectively, lower than the rate in our study. There are studies with higher rates of anxiety than the rate in our study [19]. Some studies have shown that the prolongation of the pandemic has caused nurses to experience burnout [20] and that anxiety and fears about COVID-19 have increased nurses’ desire to quit [21, 22]. The management of anxiety and depression by nurses can be greatly helped by providing mental health screening, early supportive interventions, access to psychological support services, appropriate working conditions for rest, and adequate personal protective equipment in the institution.
The comparison of anxiety predictors of operating room nurses across countries in our study indicated that anxiety was higher in the US, Australia, and England. Some studies suggest that cross-cultural differences underlie the prevalence of anxiety disorders [23, 24], but the extent of these differences remains unclear. Unlike our study, there have been studies that both associate and do not associate the mental health of health workers with the country’s economic conditions. [25]. In a study conducted in 23 countries during the COVID-19 pandemic, it was found that healthcare professionals in Brazil, Canada, and the USA experienced more anxiety than in other countries. Burkova et al. revealed Canada and Italy as the countries with the highest anxiety levels, and also with higher individualism scores [26]. In addition, it was determined that the countries with the lowest level of anxiety coincided with the lowest level of individualism (Thailand, Indonesia, Malaysia, and Nigeria). In cultures such as the USA, England, and Australia, where individualism is high, personal preferences are prioritized over group needs, and less importance than other countries is given to group harmony and emotional togetherness. However, there are some sources denying any relationship between individualism and anxiety, contrary to this view [27]. In the literature, it is emphasized that less anxiety is experienced in countries with a restrictive society structure, and anxiety levels may be correspondingly higher in free countries [26, 28]. Thus, as well as COVID-19 fluctuations during data collection, the way countries manage the COVID-19 process, and differences in vaccination processes, differences between countries may also be due to cultural reasons.
In our study, it was observed that more anxiety was experienced by the operating room nurses with high levels of worries about contracting COVID-19 and fear of infecting loved ones. In the literature, a relationship was found between the anxiety experienced by nurses and the fear of catching COVID-19 and infecting others, and it was seen that anxiety was more common in front line nurses, especially in the COVID-19 pandemic [21, 29]. Changes in working conditions, routines, job positions, and constant updates of information about the infection during the pandemic are among the factors leading to feelings of unpreparedness and fear. Similarly, many studies reported that nurses experience feelings such as fear and anxiety due to the lack of up-to-date information about the causes, management, and prevention of infectious diseases or the constant update of information [6, 30]. Providing nurses with up-to-date and repetitive education on the management of infectious patients can contribute to reducing fear and anxiety.
In our study, the operating room nurses who were not allowed to rest during working hours had 1.5 times more anxiety than those who were. The longer the weekly working hours, and the fewer the opportunities to rest during working hours, the higher the nurses’ physiological and psychological fatigue [11]. In addition, studies show that nurses working long shifts experience anxiety because they cannot spare time for themselves [32]. Differently from our study results, a study conducted on female nurses found that working time was not significantly associated with depression symptoms [33].The stress and anxiety experienced among operating room workers during the COVID-19 pandemic are also associated with increased workload and the burden of the use of personal protective equipment as a preventive measure, in terms of the extra preparation time needed and the physical discomfort caused (sweating, restricting movements, etc.) [18, 35]. In our study, it was determined that nurses’ dissatisfaction with their institution’s operating room during the pandemic caused more anxiety and depression. Mutual understanding, trust, and respect between nurses and institution managers are important in enabling health professionals to express themselves more openly and to solve their problems more easily [36]. In another study [37], it was stated that supervisors increased nurses’ job satisfaction by solving existing problems in the COVID-19 pandemic. In addition, they emphasized that their satisfaction with the wages received during the pandemic, when the working environment involved more risk and stress, could play an important role in increasing job satisfaction. In our study, operating room nurses not feeling valued in their institution was thought to be a predictor of anxiety, and the anxiety experienced due to COVID-19 may also have caused them to become more sensitive and stressed, and therefore, expect more support from their institutions.
In our study, participants who expressed a low level of confidence in their institution for the management of the COVID-19 pandemic experienced 1.8 times more anxiety than those who expressed more confidence. One of the most important factors associated with the pandemic management of the institution is the provision of personal protective equipment and the improvement of employee working conditions [38]. Anxiety among health care professionals during the COVID-19 pandemic is related to organizational factors, such as the amount and quality of information about COVID-19, competence of hospital managers, preparedness for the pandemic, and ease of access to COVID-19 tests [39]. Assignment of operating room nurses to work in other units due to the postponement of scheduled elective surgeries in the first months of the pandemic process may also be a factor in stress.
In our study, it was determined that working as an operating room nurse in Türkiye caused 5 times more depression. In studies examining the depression levels of nurses during the pandemic in Türkiye, it was shown that nurses experienced depression at rates ranging from 34.9% to 77.6% [40, 41]. These high rates are thought to be related to factors such as working longer than 12 hours, limited psychological support, and changes in the units and working practices [17, 40]. However, unlike our study, Degucgi et al. reported that there was no relationship between workload, job control and social support from their institutions and depressive and anxiety symptoms [42]. The high rates of depression among operating room nurses in Türkiye may be related to the inadequate PPE during the pandemic, the inability of the institution to provide adequate psychological support, and the inadequate wages. In our study, it was found that although there was no statistically significant difference in the anxiety levels of nurses in Türkiye compared to the other countries surveyed, the level of depression was much higher than in other countries in general. According to the OECD, there was an average of 154,004 nurses in a European country in 2019 and 18 nurses for every thousand, but in Türkiye there were only 9 nurses for every thousand. This can cause an increase in the number of patients and workload, burnout, and depression in nurses. The high depression levels of nurses in Türkiye in our study may have been related to the heavy workload already being experienced before the pandemic and the inadequacy of support systems.
In our study, it was found that operating room nurses who were on isolation leave after providing care for COVID-19 patients experienced 1.5 times more depression than those who were not. Quarantine/isolation has been found to be associated with depression in nurses [43]. A higher rate of depression may have been caused by the fact that nurses could not be with their families during the compulsory isolation and could not meet the needs of their families or their dependent children, and the problems they experienced in controlling this situation.
This study has some limitations. The fact that this is a cross-sectional study may limit the determination of the causality of anxiety and depression risk factors. The self-report scales used in the study limit the generalizability of the findings. In addition, it may be difficult to generalise the study’s findings to other demographics or contexts because it only examines operating room nurses in a few selected countries. In this study, gender data was not collected and not considered as an independent variable. It is recommended to carry out further studies that also examine the gender variable. The inclusion of English-speaking nurses from Israel and India in the study sample may introduce bias since it could exclude those who do not speak English proficiently. To mitigate this potential bias in future studies, researchers should strive to collect data in the languages spoken within those countries, which can significantly increase the diversity and statistical power of the sample.
Operating room nurses need health protection including recovery programs aimed at improving psychological well-being. Furthermore, more psychosocial support could be helpful for OR nurses to relieve their perceived psychological stress. In future studies, educational/interventional support studies can be conducted to reduce the stress, anxiety and depression levels of operating room nurses.
Conclusions
This study reveals the difficult struggles of OR nurses during the ongoing COVID-19 outbreak, with long working hours and high anxiety - depression scores. Despite some differences between countries in terms of health system, patient potential, economic and the opportunities offered, generally high levels of anxiety and/or depression indicate that all OR nurses need urgent support. We recommend the provision for timely psychological support and interventions for OR nurses who present with anxiety and/or depression after a mental health assessment.
Ethical approval
The study was approved by the Scientific Research Ethics Committee of Izmir University of Economics (decision no. 34, date 01.02.2021).
Informed consent
Written informed consent was obtained from all participants prior to the study.
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
The authors would like to thank the participants for taking part in the study.
Funding
The authors report no funding.