
Abstract
BACKGROUND:
Smartphone usage has increased rapidly in the last decade due to rapid technological advancements. This extensive usage of smartphones led to physiological problems and musculoskeletal disorders (MSD) due to inappropriate postures.
OBJECTIVE:
Past studies have reported the effects/discomfort of smartphone usage for short periods, ranging from 3–20 min, which does not represent the current era of smartphone dependency (approximately 7-hr/day).
METHODS:
This study was performed on fifty-four participants aged 20–28 with 1-hr smartphone texting in a sitting posture. Flexion angles, both sides (dominant and non-dominant) muscle activity (maximum voluntary contraction %) at sternocleidomastoid (SCM), upper-trapezius (TRP), extensor digitorum (EDM) and abductor pollicis brevis (APB) muscles, and subjective discomfort were analyzed.
RESULTS:
After 1-hr smartphone texting, the muscle activity at eight upper extremities: SCM (24.80%), TRP (29.45%), EDM (14.44%) and APB (19.87%) significantly (p < 0.001) increased by 1.5–1.9 times with 27.4±3.18° and 82.94±7.03° head and lower-arm flexion angles, respectively. The mechanical loads on the cervical spine increased by 4.6 times, and subjective discomfort by 3 times.
CONCLUSION:
Maintaining the same posture for a long duration causes postural stress, muscular imbalances, and discomfort, leading to MSD with increased cervical intervertebral disc pressure.
Keywords
Introduction
Smartphone usage has exponentially increased due to connectivity, affordability, entertainment, and ease of access to information. In 2022, the smartphone adoption rate increased from 3.5 billion in 2019 to 5.4 billion users globally [1] and 647 million in India [2]. Due to the COVID-19 pandemic, global smartphone usage increased by 54% [3] and 31% in India [4], with a 7-hr/day average usage [1]. Excessive smartphone usage leads to fatigue at the neck, shoulder, and thumb; digital eye strain, and addiction [5–10]. Environmental, physical, demographic, and habitual risk factors contribute to fatigue [11, 12]. Muscle fatigue due to smartphones results in muscular imbalances and musculoskeletal disorders (MSD) [13–15]. Maintaining flexed head postures during texting strains the neck muscles causing discomfort, named ‘text-neck’ syndrome [16, 17].
Researchers have utilized various methods to measure head flexion angle (HFA) and lower-arm angle (LAA), using inertial measurement units, accelerometers, and gyroscopes [16–18]. Studies have investigated the correlation between smartphone usage duration and HFA during gaming [19] and web browsing [17], with different postures and natural movements [16–18]. These studies have shown a 3–5 times higher load acting on the neck during smartphone usage than in neutral posture [20, 21]. The kinesiology of the lower arm or elbow with smartphone interaction affects the upper extremities’ muscle activity and HFA [8, 22]. Similarly, a study examined the correlation between joint movements (shoulder, elbow, and wrist) during smartphone gestures [10]. Smartphone-related MSD predominantly involves the shoulder, neck, lower back, elbow, wrist, and thumb muscles [5–14]. Surface electromyography (SEMG) was utilized to record discomfort in the sternocleidomastoid (SCM) [5–7], trapezius pars descendens (TRP) [5, 9], cervical erector spinae (CES) [8], extensor digitorum (EDM) [10, 11], and abductor pollicis brevis (APB) [12–14] muscles.
The correlation between body posture and resultant muscle activity was studied, and the increased muscle activity is associated with increased fatigue levels [10–13]. Several studies assessed the discomfort levels of participants using a subjective evaluation of questionnaire data with their socio-demographic information, smartphone usage pattern, and body posture [16, 23]. The collected questionnaire data were analyzed using various techniques of neck disability index, Likert scale, or Q-factor analysis [24–26] to assign scores based on the subject’s discomfort. Rapid upper limb assessment or RULA is a subjective ergonomic evaluation tool for postural analysis during smartphone usage [27].
The key findings drawn from recent studies are: Prolonged usage of smartphones leads to increased muscle fatigue, which can induce MSD [28, 29]. SCM and TRP muscles are responsible for head stability [30]. EDM and APB muscles significantly affect thumb movements [11, 12]. Various techniques, such as angle measurements and motion sensors, are employed to measure flexion angles and correlate them with muscle activity [17, 18]. Numerous researchers have examined smartphone users’ discomfort levels through questionnaire data of pen-and-paper-based or web-based methods under different scenarios (usage content, age groups, duration, and posture maintained) of smartphone usage [24–26].
The research gap based on the available literature states that past studies [8–11, 29] have reported the effects of smartphone usage for short periods, ranging from 3–20 min (4–10% of MVC on average), which does not represent the current era of smartphone dependency (approximately 7-hr/day). In addition, limited studies have been performed on the second-highest smartphone user country (India). As smartphone usage patterns [31] and anthropometry [32] differ across various countries, flexion angles and muscular activities vary based on their demographic data. Numerous studies have relied solely on subjective assessments [16, 23–27], therefore, an extensive experimental investigation is necessary on prolonged smartphone usage and its effects. Thus, this study elucidates the correlation between dominant and non-dominant upper extremities (SCM, TRP, EDM, and APM) muscle activity, HFA, and LAA with 60-min smartphone texting among young Indian adults. In the current study, three hypotheses are proposed based on, (i) after 1-h smartphone texting, all eight muscle activites reach above 15% of their maximum voluntary contraction (MVC), (ii) the muscle activity is equivalent (non-significant) in both the dominant and non-dominant side while texting and (iii) the head and lower-arm movements have a minimal range of motion during texting.
Methodology
This section explains the selection procedure of participants, experimental methods and tools, data collection procedure, and processing techniques.
Selection of participants
As presented in Table 1, 54 young adults were enrolled in this study after signing an informed consent form. The selected participants had at least 1-year smartphone texting experience and no history of MSD. In addition, participants were requested to avoid intense muscular actions on the assessment day. The Institutional Ethics Committee (Human Studies) has reviewed and approved the study design (approval number: 1980/IEC/2020). The Institutional Ethics Committee follows biomedical research guidelines on human participants as per the direction of the Declaration of Helsinki.
Participants’ demographic information (n = 54)
Participants’ demographic information (n = 54)
M –Mean, SD –Standard Deviation.
A portable-wireless AT-04-001 Myoware [15] sEMG setup [19] was used. The sensor received approval from applicable derivatives and Conformité Européenne to comply with safety and signal quality standards [15]. A medico (Msglt-8 G) with Ag-AgCl polymer gel-coated electrodes of 1 mm thickness and 42 mm diameter was used. The HFA and LAA were measured using a gyroscope setup. This study used a smartphone of 170 g of 5.9′′ screen size with a 720×1440-pixel ratio, and a non-adjustable office chair supported with a backrest and armrest.
Subjective analysis
Pre- and post-subjective discomfort analysis was assessed to analyze the participants’ discomfort after 1-hour smartphone texting. The pre-subjective questionnaire was developed with 32 standard questionnaires [16] consisting of participants’ demographic information, smartphone usage (posture, pattern, and duration), consequences associated with excessive smartphone usage, and discomfort faced before smartphone usage. In total, 1659 responses were received in pre-subjective analysis. During the post-subjective analysis, participants were asked to fill out another questionnaire to indicate their level of discomfort at the neck, shoulder, back, elbow, wrist, and fingers every 15-min during smartphone texting. The analysis scale ranges from 1 (very comfortable) to 5 (very uncomfortable) [26].
Experimental study design
During the experimentation, the subjects were instructed to text on the provided smartphone for 60-min while sitting in a non-adjustable office chair (Fig. 1). From the 1659 responses, 59% of the participants selected sitting as their preferred body posture, and 86% selected texting as their primary smartphone task with > 100 messages/day. During texting, participants are required to hold their smartphone in portrait mode using both hands and text the words recited by an experimenter. The audio-text includes 3–7 English letter words often used in daily routine [10]. Participants were allowed to correct any errors while typing and were not permitted to terminate typing during the task. The participants typed an average of 161 characters/minute with 89% accuracy. The participants are allowed to maintain a comfortable posture with a 30–40 cm eye-to-screen distance [10, 22]. They were instructed to rest their hands and back on the chair supports. The experimental location was kept at a 75–80 lux brightness level.
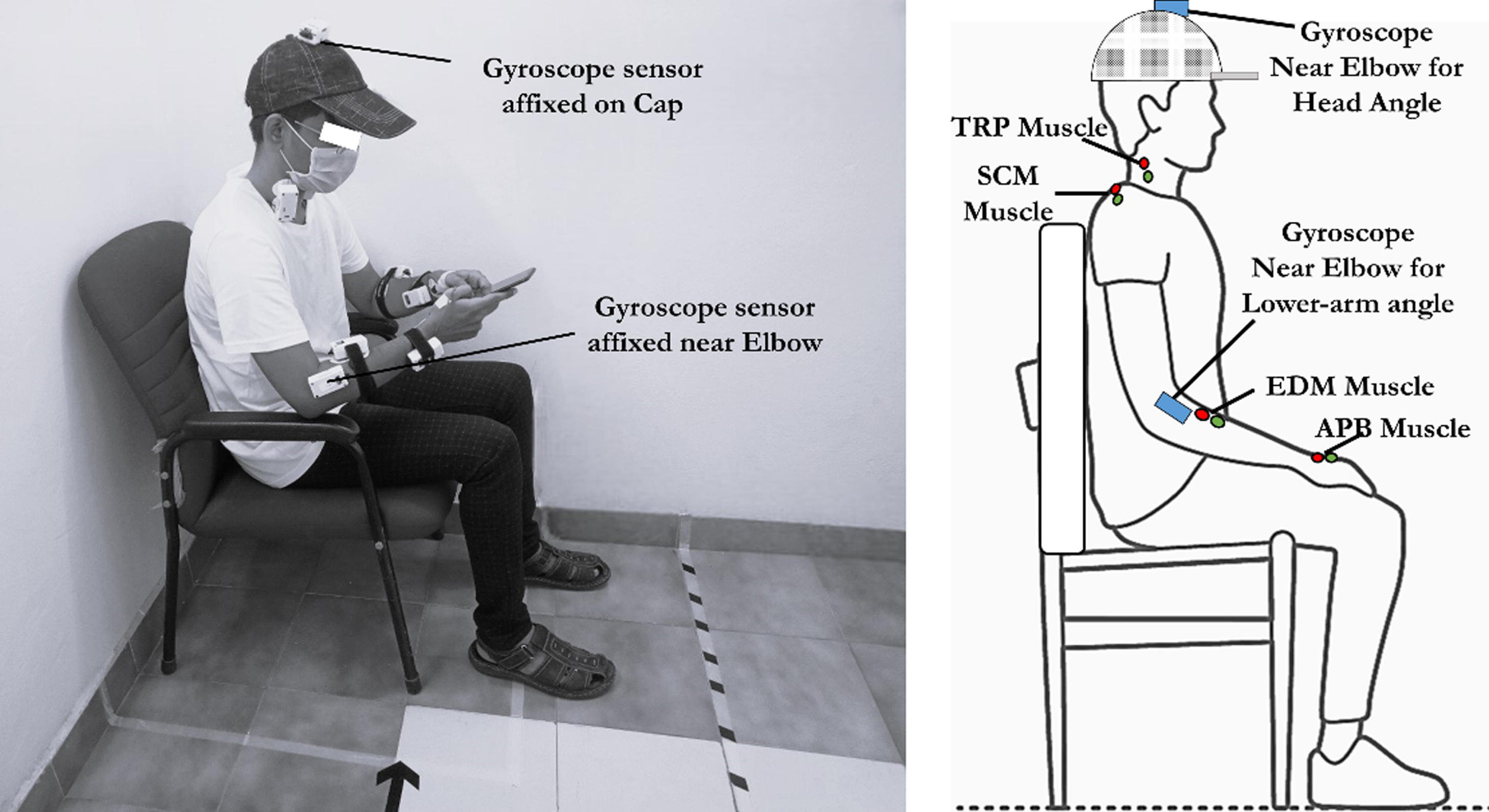
Participant’s posture with sensor attachment at each location during smartphone texting.
The experimental procedure involves two stages. In stage-1 of testing preparation, where the participants are fitted with eight sEMG sensors at SCM, TRP, EDM, and APB muscles on both sides as illustrated in Fig. 1. This study adhered to ISEK [33] and SENIAM [34] standards for electrode placement and sEMG data retrieval procedures. After cleaning the skin with alcohol [33], two bipolar electrodes were placed on the dry skin at 20–30 mm, and the reference electrode was positioned away from the selected muscle [34]. The SCM electrodes were placed in line with the sternal portion, at one-third of the distance from the mastoid process, and the reference electrode is on the right acromion process [5–7]. The electrodes were placed at 50% of the spine-acromion line for the TRP muscle, and the reference was at the C7 vertebra [8, 9]. The bipolar electrodes of EDM were placed at one-third from the lateral epicondyle along the styloid process of radius and the reference at the lateral epicondyle at the elbow joint [10, 11]. Similarly, for the APB muscle, the electrodes were placed parallel at one-fourth of the first ossa metacarpal and the reference around the wrist [12–14]. Two gyroscope setups (one over the head and the other near the elbow) were placed to assess the head and lower arm posture, as shown in Fig. 1.
In stage-2, three sEMG signals (rest, MVC, and task) were retrieved. Initially, the participants were instructed to maintain a comfortable sitting posture, and the EMG signals were collected for 90 s, referred to as RestEMG. After this, the MVC measurements for each muscle were performed for 10 s, as illustrated in Fig. 2 [5, 12] referred to as MVCEMG. For MVC measurement, the subjects were directed to gradually apply maximal force for 3 s, maintain the same force for 3–5 s, and then gradually release the force over 3 s [33]. Following the MVC trials, subjects were given a 20-min rest period before performing a 60-min texting experiment (TaskEMG). After the experimentation, each participant filled out a post-subjective analysis form.
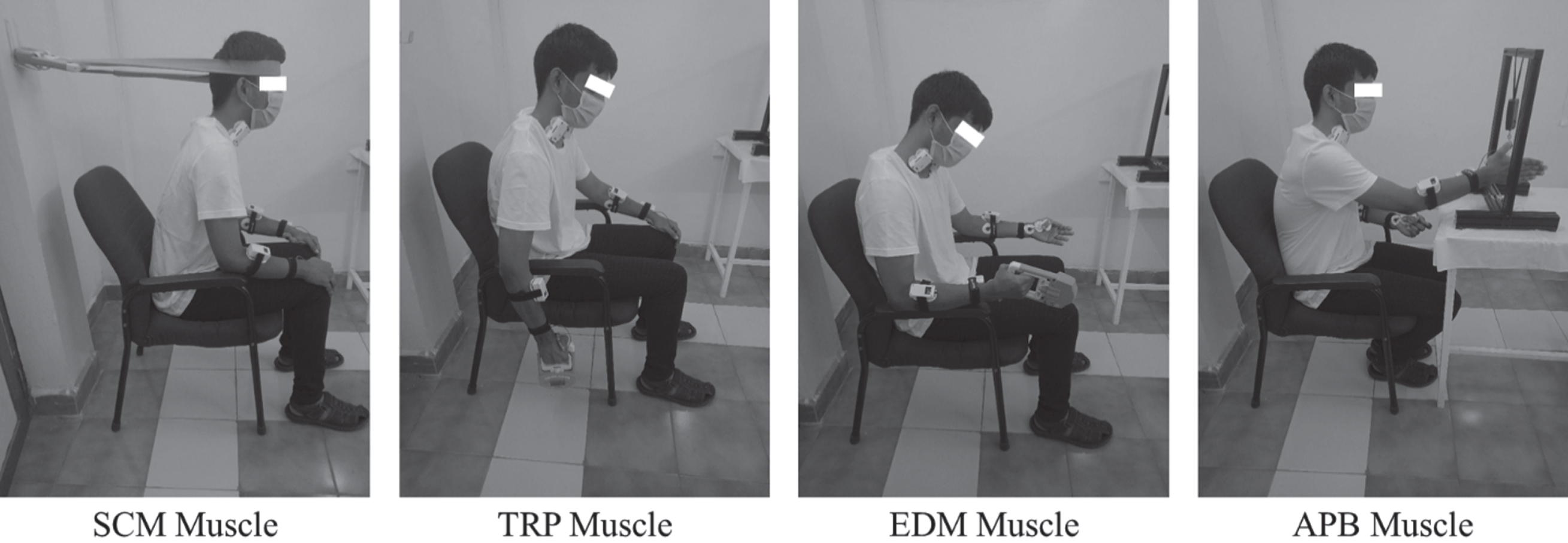
MVC measurement technique for each muscle.
The sEMG and gyroscope were interfaced with a processing unit using a microcontroller, and the retrieved data was exported to an excel sheet. The sEMG signal was recorded with a 1024 Hz sampling rate. The raw sEMG signal was amplified and then filtered to remove any unwanted noise using a common-mode rejection ratio and band-pass (Butterworth second-order) filter with a cut-off frequency of 10–500 Hz [33]. Then the signal was subjected to Fourier analysis to determine the muscle fatigue and frequency potential. Next, the sEMG signal was rectified using full-wave rectification followed by a root mean square (RMS) smoothing process. In the smoothing process, for the identification of reflex actions and fast movements, a 50-ms width time window was used [34], and the RMS feature was extracted. The final step involves normalization using MVC, as shown in equation (a). The normalization method uses RMS value at rest, task, and MVC to compare participants’ fatigue levels [35].
Statistical analysis of average muscle activity, HFA, LAA, and post-subjective analysis was carried out to analyze the significant effect on the duration of smartphone usage using a one-way repeated measure ANOVA (r-ANOVA) [36]. Before the analysis, the normality of the variables was tested. As confirmed by the Shapiro-Wilk test for normality, all the variables followed a normal distribution [36]. Mauchly’s test of sphericity was employed to check the assumption of sphericity [36]. A violation of sphericity was observed with a p-value of < 0.001, which resulted in null hypothesis rejection. The F-value obtained from the Greenhouse-Geisser procedure was corrected using the epsilon (ɛ) parameter to estimate the degree of freedom. The significant effect of body posture and duration was evaluated using a Greenhouse-Geisser correction and a Bonferroni post-hoc analysis with software SPSS 25.0.
RULA postural analysis was carried out on the retrieved HFA and LAA to understand the level of MSD risk [27]. Theoretical calculation of the load acting on cervical vertebra C7 was performed using equation (b) for various HFA ranging from 0° to 60°, at 15° intervals [20]. The load was based on the individual’s head weight at 0°, estimated at approximately 8% of the overall body weight [37]. From Fig. 3, θ represents the HFA.
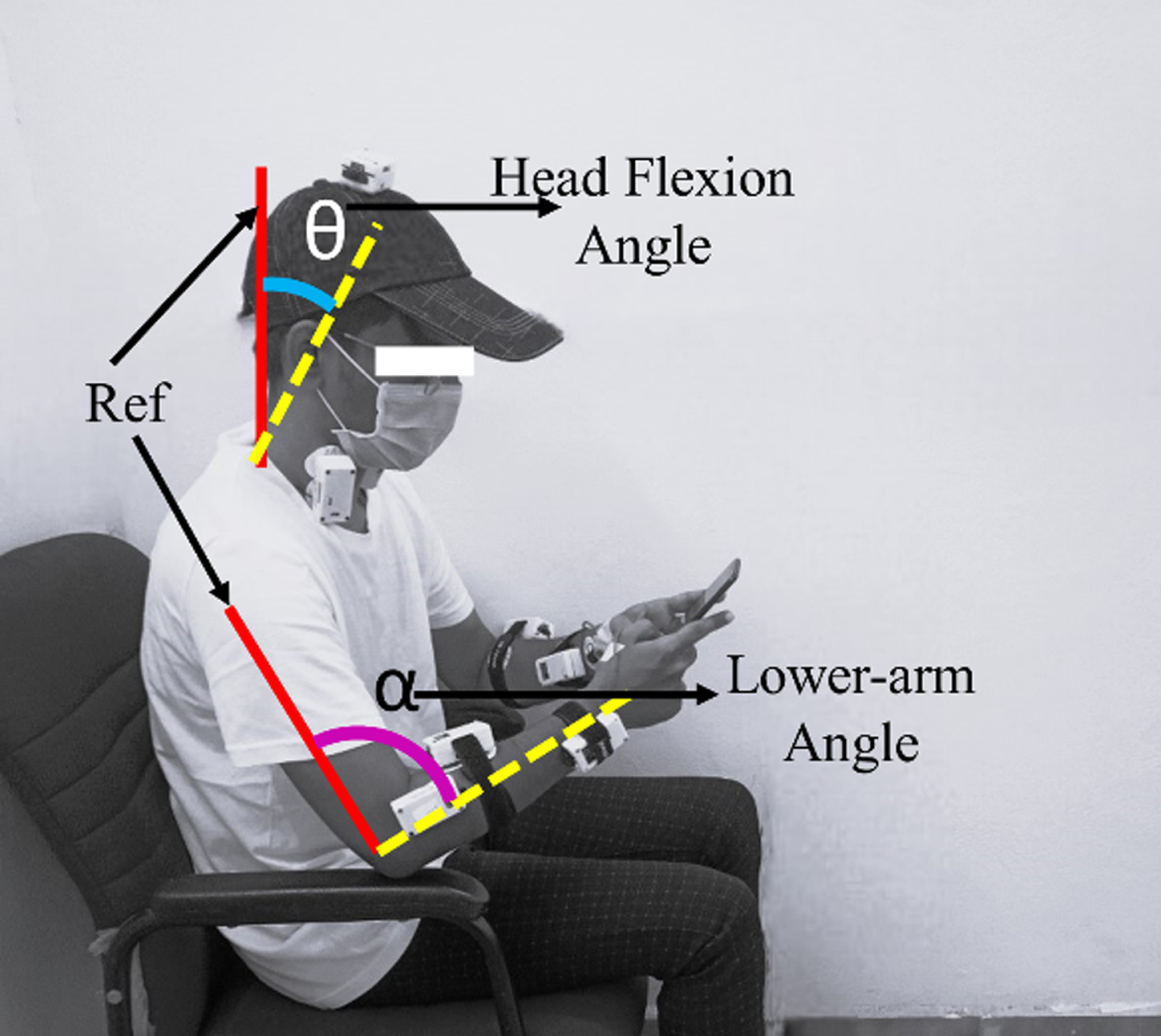
Head and lower-arm flexion angle tracking using gyroscope.
Based on the pre-subjective assessment, the majority (94.7%) of the participants use smartphones as part of their daily routines from a moderate to a very high extent. Figures 4 and 5 illustrates the participants’ average HFA and LAA during different durations, respectively. No significant difference was observed in HFA and LAA with the change in time. The muscle activity (MVC%) of participants at SCM, TRP, EDM and APB muscles during different time ranges are illustrated in Figs. 6–9. Similarly, the overall muscle activity at the upper extremities on both sides after 60-min smartphone texting is presented Table 2. It is observed that muscle activity at eight muscles significantly differed (p < 0.001) with the change in smartphone usage duration; likewise, the muscle activity at SCM, TRP, and APB significantly differed (p < 0.05) with the dominant and non-dominant side. The discomfort level of participants after smartphone texting at the neck, lower back, shoulder, elbow, wrist, and thumb finger are presented in Fig. 10. Although the post-subjective discomfort level in Fig. 10 shows a significant difference (p < 0.05), it is not presented due to legibility. Furthermore, a one-way r-ANOVA with Greenhouse-Geisser correction and Bonferroni post-hoc test analysis with pairwise comparison is conducted, and the results are elaborated in Table 3.
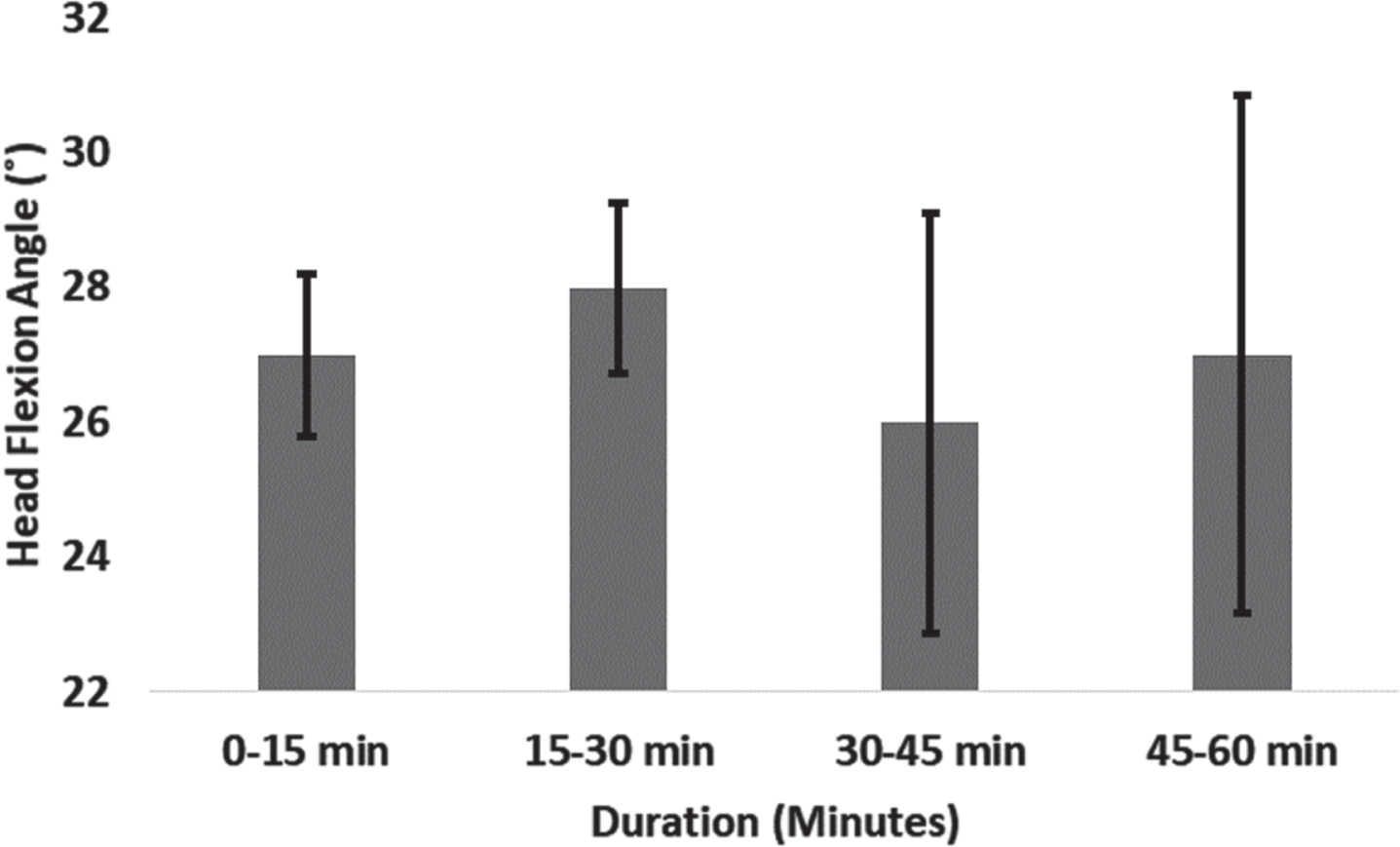
Head flexion angle during smartphone texting within subjects.
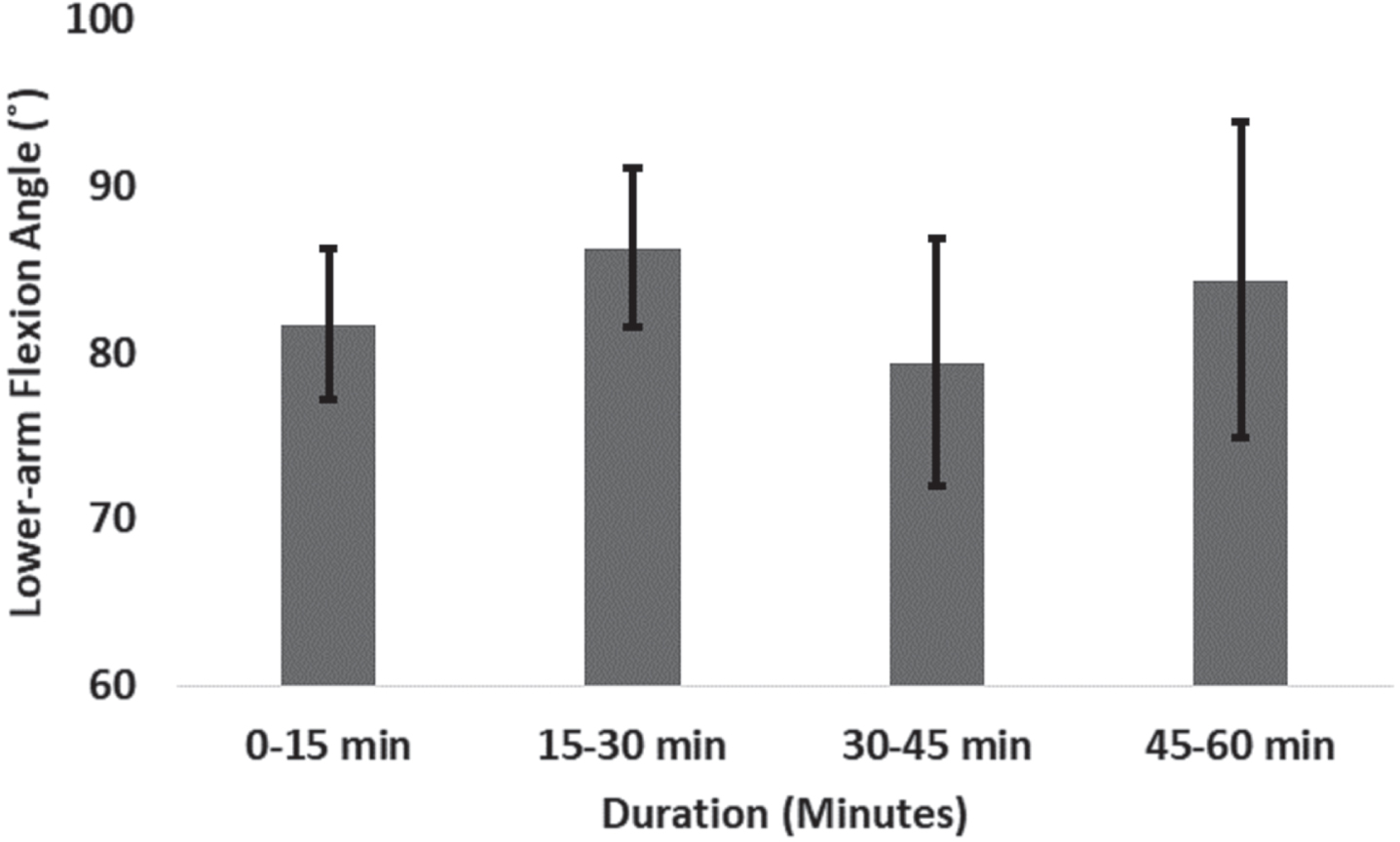
Lower-arm flexion angle during smartphone texting within subjects.
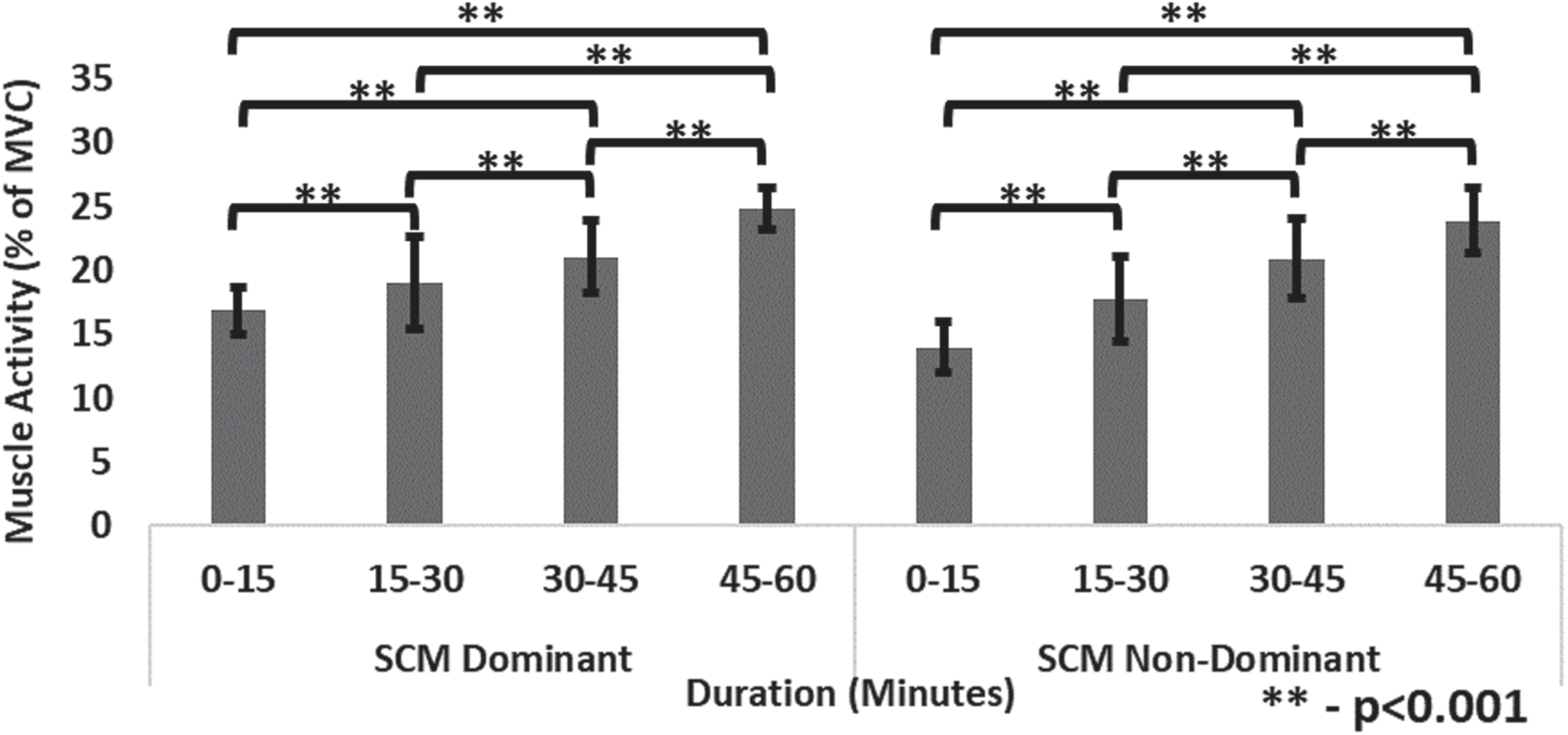
Muscle activity at SCM muscle during smartphone texting at different time ranges.
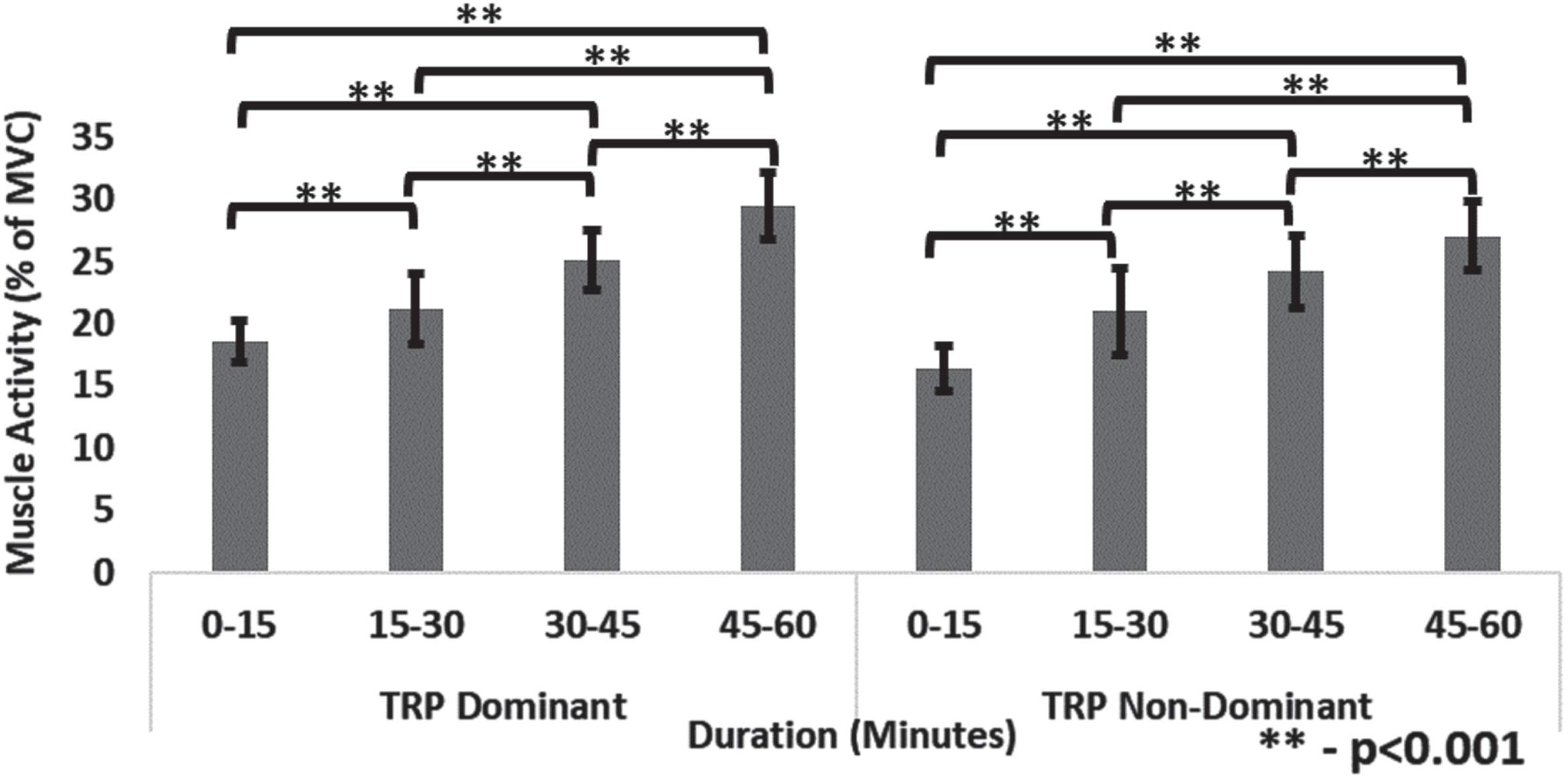
Muscle activity at TRP muscle during smartphone texting at different time ranges.
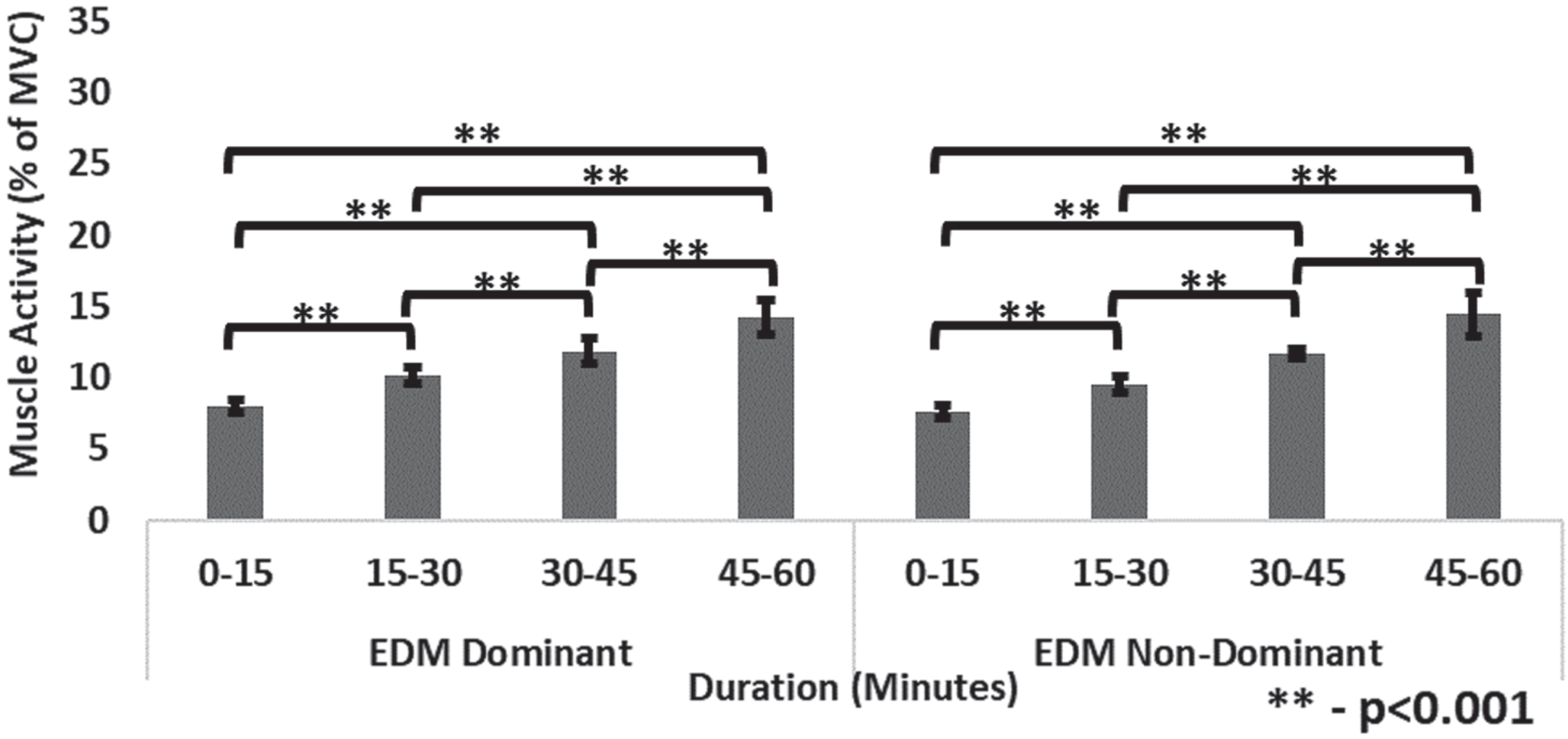
Muscle activity at EDM muscle during smartphone texting at different time ranges.
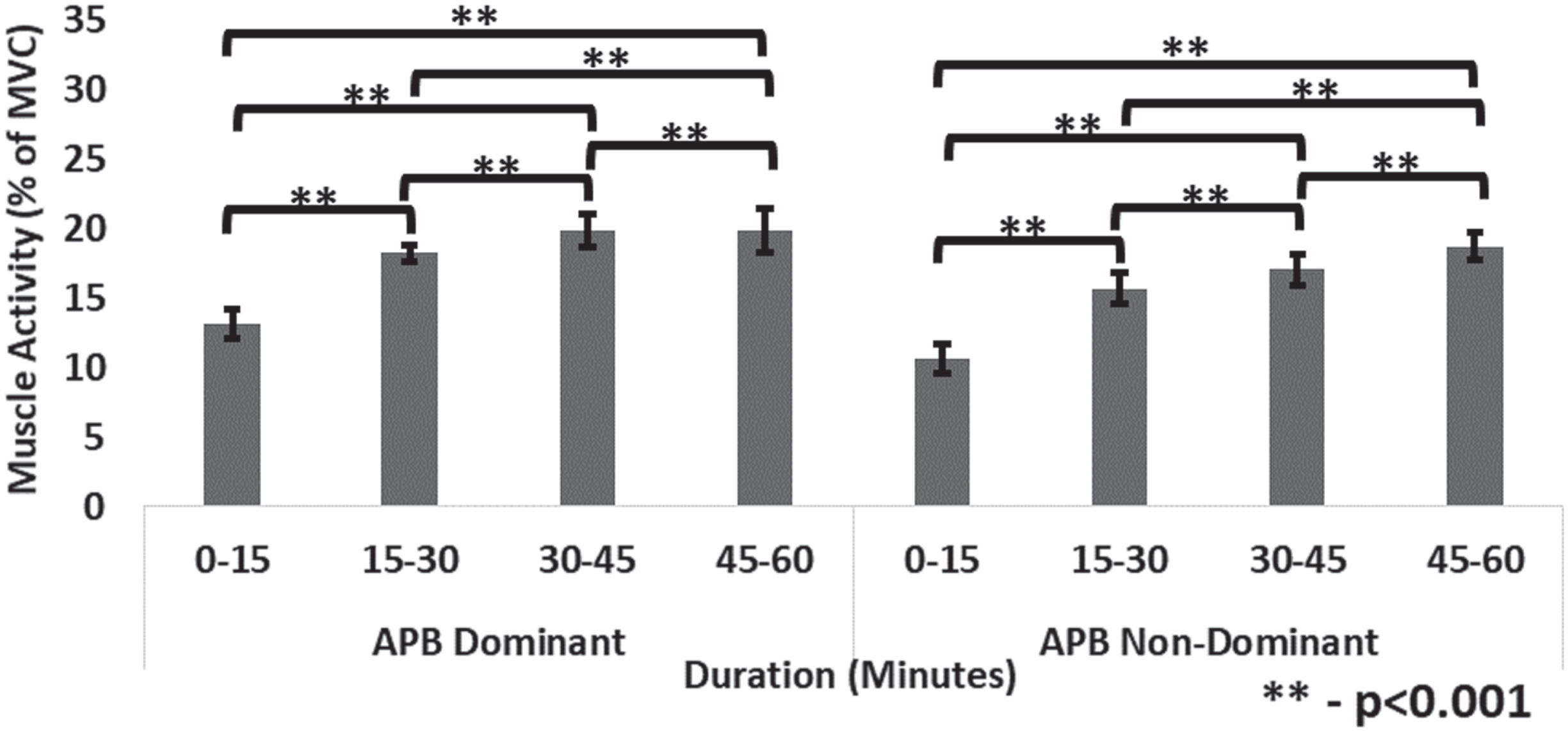
Muscle activity at APB muscle during smartphone texting at different time ranges.
Participants’ muscle activity (MVC%) of different muscles at different time ranges (M±SD)
M –Mean, SD –Standard Deviation.
Pre-subjective assessment
Based on the pre-subjective questionnaire responses (1659), 93% of smartphone users are aged between 18–30 years with a 3-h minimum usage/day. It is indicated that the usage of smartphones is more often during pre-sleep (95%), studying (72%) and eating (45%), with texting (86%), social media (81%) and gaming (80%). From the responses, sitting (99%), lying-down (93%), standing (59%) and walking (37%) postures are maintained during smartphone usage. Participants reported digital eyestrain (75%), neck/shoulder pain (72%), headache (50%) and sleeping disorders (34%) after continuous 1-h smartphone usage. In addition, 80% of participants reported excessive smartphone usage leads to mental and physical problems [23]; and 95% of the respondents reported smartphone usage before sleep leads to insomnia [16], of which only 29% are taking preventive measures. In other studies, 76% of volunteers who participated in a survey confirmed that smartphone usage turned into an addiction, exceeding 4 hours of usage/day [26], and stated that they could not survive without it [21].

Post-subjective analysis –participants’ discomfort level during smartphone texting.
As presented in Table 3, participants maintained various HFA [27.42° (0–15), 27.83° (15–30), 26.80° (30–45), and 27.04° (45–60 min)] in the experimentation cycle and exhibited no significant difference with time ranges. During the experiment, most participants maintained an average HFA of 27.4±3.18° for 47-min (>78% of the duration). Thus, this can be classified as flexed head posture or increased HFA for a prolonged duration. HFA > 20° involves higher risk and is unacceptable according to RULA postural analysis [27]. Therefore, it is recommended to maintain lower HFA [18]. A study reported that one-handed browsing and two-handed texting exhibited an increased HFA from 27.3° to 34.2° and 35.7° to 41° respectively [17]. Based on ergonomic recommendations, HFA is restricted to 13°–15° and 20°–37° during browsing on computers and smartphones, respectively [22].
Statistical analysis of flexion angles, load at C7 and post-subjective discomfort analysis
Statistical analysis of flexion angles, load at C7 and post-subjective discomfort analysis
Similarly, participants maintained different LAA [81.71° (0–15), 86.27° (15–30), 79.42° (30–45), and 84.35° (45–60 min)] during experimentation. The LAA ranges from 110°–120° during the rest position. No significant difference was observed in LAA with different time ranges (0–15, 15–30, 30–45, and 45–60 min). Participants maintained an average of 82.94±7.03° for 35-min (>58% of the duration) during smartphone texting and considered as a higher risk posture as per RULA analysis [27]. The Swedish work environment authority recommended the LAA of 90° and 110° for laptop/desktop and smartphone usage, respectively [22]. A study on two-handed smartphone texting with forearm support observed that LAA varied between 70° and 90° with and without ergonomic recommendations, respectively [10]. Another study observed increased TRP muscle activity at 30° shoulder angle without forearm support during smartphone usage [8].
After 1-hr smartphone texting, the muscle activity (MVC%) at SCM muscle in the dominant and non-dominant side reached 24.80% and 23.90%, and at TRP muscles reached 29.45% and 27.07%, respectively. In comparison with the initial phase (0–15 min), the muscle activity increased (approximately) by 1.47 times at SCM and 1.58 times at TRP muscles respectively by the end (45–60 minutes) of the experiment cycle, as presented in Table 2. A statistically significant difference (p < 0.05) in the average muscle activity of dominant and non-dominant SCM and TRP muscles was observed among different time ranges with pairwise comparison. Prolonged use of smartphones can cause significant discomfort and strain on the SCM [5] and TRP [8] muscles, resulting in anatomical structure deformation and nerve compression [7]. A study reported 2.4% and 3.8% muscle activity (MVC%) at SCM and TRP muscles after a 5-min smartphone usage [28]. In another study of 10-min typing on a laptop, the muscle activity at SCM and TRP reached 1.6% and 2.1% of MVC in flexed head posture, respectively [38]. Similarly, MVC% of TRP varied with different postures of sitting, standing, lying, and walking during 20-min smartphone texting by 15%, 13%, 9%, and 22%, respectively [9], which resulted in a significant increase in pressure point and reduction of muscle hardness [7].
Similarly, after 1-hr smartphone texting, the muscle activity (MVC%) at EDM muscle in the dominant and non-dominant side increased to 14.26% and 14.44%, and at APB muscle increased to 19.87% and 18.75%, respectively. In comparison with the initial phase (0–15 min), the muscle activity increased (approximately) by 1.89 times at EDM and 1.76 times at APB muscles respectively by the end (45–60 minutes) of the experiment cycle. A statistically significant difference (p < 0.05) was noticed in the dominant and non-dominant EDM and APB muscles among different durations with pairwise comparison. Previous studies reported an MVC% of EDM with computer and smartphone typing for 2-min was 7.5% and 3.8% while maintaining 90° LAA and 45° across mid-line [10]. Another study reported on APB muscle with 5-min keyboard typing under different keyboard angles of 40°, 20°, 0°, –20° and –40° exhibited 30%, 21%, 14%, 17%, and 28% MVC, respectively [12]. In another study of 300-character typing, muscle activity (MVC%) reached 7.7% and 19.4% at EDM and APB, respectively [14]. The increased muscle activity at EDM further affects the gripping force [10]; similarly, the abduction/adduction thumb movements during texting increase the APB muscle activity [13], causing discomfort and reducing typing speed.
Comparing both sides’ muscle activity, SCM, TRP, and APB resulted in significantly (p < 0.05) higher muscle activity on the dominant than on the non-dominant side. However, there is no significant difference in EDM muscle on both sides. Past literature demonstrates that dominant muscles exhibited significantly higher muscle strength and activity than non-dominant muscles during smartphone usage [36]. It revealed that muscle tendons are significantly larger with higher cross-sectional areas in the median nerve on the dominant side due to the habit of single-hand smartphone usage. In a study on smartphone usage, both SCM and TRP muscles exhibited higher muscle activity during taping compared to non-taping conditions [30]. The maximum muscle activity reached 14% and 24% for EDM and APB, respectively, for the farthest touch point during the 3-min touch task [11]. During a 1–2 s lift of 10 kg, the MVC reached 44% [6]. However, in the present study, MVC% increased to 22% at SCM, 26% at TRP, 14% at EDM, and 19% at APB muscles without the involvement of any heavy loads, which is solely due to the flexed head and lower-arm posture during excessive smartphone usage. In line with the findings from previous studies, this increased muscle activity (MVC%) for a longer duration could result in severe damage to muscle with reduced muscle stiffness and increased fatigue level [14].
Load acting on cervical C7
The study calculated the load exerted on the C7 region of the neck for different HFA, and the results showed that the load increased with the HFA (ranging from 47.51±9.14 N at 0° to 219.47±42.22 N at 60°). Compared to the neutral head position (approximately 50 N at 0°), the load on the cervical region increased to 98.38 N (15°), 146.20 N (30°), 179.20 N (45°), and 219.47 N (60°). Pairwise comparisons revealed a significant difference (p < 0.05) in the load acting on the cervical C7 vertebra at various HFA. Most participants maintained 27.4±3.18° (approximately 30°) as an average HFA for 47-min (more than 78% of the hour) during 1-hour smartphone texting. Hence, at a 30° HFA, the head’s weight increased to 146.20 N, three times its weight. These findings revealed that an extra 100 N on C7 was acting for the 47-min duration, as there is an increase in gravitation pull due to shifting in the centre of gravity with the change in HFA [20, 27]. It resembles a significant increase in the load on the C7, which further affects the shear forces and intervertebral disc pressure [39], leading to the laxity of the capsular ligament of the facet joint [40].
Post-subjective assessment
Based on the post-subjective analysis, the study findings revealed that 80% of the participants indicated > 4 (discomfort) on a Likert scale of 5-point at the neck region. The post-subjective analysis showed a statistically significant difference (p < 0.05) with pairwise comparison among different time ranges. A significant increase in discomfort at the neck was observed at the end (45–60 min) of the study period from the initial period. In line with the study, 95% of smartphone users experienced upper extremities and neck pain [24], leading to muscle discomfort, and 18.8% persistently developed MSD [25, 26].
The findings of this present study indicate that prolonged (1-hr) smartphone use leads to increased muscle activity, resulting in muscle fatigue and discomfort. These results also apply to industrial workers working in prolonged flexed upper body and head postures, such as chip designing, soldering, MEMS handling and assembly. Based on the flexion-angle data, it was observed that participants maintained an average HFA of 27.4±3.18° for 47-min and LAA of 82.94±7.03° for 35-min in a sitting posture. The data presented in Table 3 shows that the use of a smartphone does not have a significant impact on HFA and LAA over time. However, the usage of a 1-hr smartphone has a significant effect on muscle activity and subjective evaluation. Generally, muscle possesses elastic nature, and the human musculoskeletal system consists of slow-twitch and fast-twitch fibres. The present study focused solely on slow-twitch fibres. Therefore, the increased flexion angle pattern with smartphone texting increases muscle activity with duration. A higher degree of flexion in the cervical spine places a greater demand on the SCM and TRP muscles to generate counterbalancing forces developed by the head’s weight. Hence, the resistive support movement of the SCM and TRP muscles is lost due to postural maintenance. The EDM and APB muscle loads increase with the increase in wrist flexion/extension and thumb abduction/adduction movements and velocities, which further affects the relaxation and stabilization of hands by reducing the gripping force and typing speed. Maintaining the same posture for long durations causes postural stress and discomfort, leading to muscle fatigue [16]. This phenomenon led to increased standard deviation in HFA and LAA, where participants often adjust/alter their head to reduce discomfort/pain, which alters the hand angle to have clear visibility of the smartphone screen. The theoretical evaluation specified that the load acting on C1-C7 increased by 4.6 times at 60° HFA.
This study revealed a clear association between postural angles and muscle activity, which is accompanied by a gradual increase in neck discomfort due to muscle fatigue. In line with the past literature, the study findings demonstrated that (i) prolonged smartphone usage increases muscle activity with flexed postures, (ii) mechanical load on cervical spine vertebrae increased by 3–5 times [20, 21], and (iii) higher flexion angles cause MSD with postural stress and muscular imbalances [16]. Based on the experimental results, the hypotheses were validated, as contrary to the first hypothesis, the muscle activity (MVC%) significantly differed for eight muscles. Similarly, the second hypothesis is rejected, as muscle activity significantly varied for both sides in SCM, TRP and APB. The third hypothesis is accepted, the HFA and LLA have a minimal range of motions.
Limitations and future scope
The pre-subjective analysis revealed that the participants reported varying postures, tasks, and increased smartphone usage duration of 3–4 hours. However, this study focused on the effects of 1-hour smartphone texting while sitting on a non-adjustable office chair with 54 participants aged 20–28. On the other hand, several other studies have conducted muscle fatigue-related analyses with time intervals ranging from 3–20 minutes [8–11, 29]. Furthermore, only theoretical calculations of the load acting on cervical vertebra C7 were performed using equation (b). Though the current age group (young adults) reported texting and gaming as their major activity, only texting is reported in this study with a single smartphone. In the future, more smartphone content with varied screen sizes and age groups should be considered with gender differences for a better understanding of content, age-based and gender-based disorders.
Conclusion
This study elucidates the effects associated with prolonged (1-hr) smartphone texting by analyzing muscle activity, body posture, and subjective analysis. An experimental trial was conducted on 54 young adolescents with 1-hr smartphone texting using both thumbs while resting their hands and back on supports in the sitting position. After 1-hr smartphone texting, the muscle activity (MVC%) significantly (p < 0.001) increased at eight upper-extremities SCM (24.80%), TRP (29.45%), EDM (14.44%) and APB (19.87%) with 27.4±3.18° and 82.94±7.03° HFA and LFA, respectively. It was observed that continuous 1-hr smartphone usage significantly (p < 0.001) increased muscle activity by 1.5–1.9 times, mechanical loads on the cervical by 4.6 times, and subjective discomfort by 3 times. It further leads to MSD with reduced gripping strength and muscle stiffness. It was noted that various aspects (content, posture, duration) could lead to smartphone-related MSD. In summary, the study indicates a potential risk to the cervical spine in prolonged smartphone usage with a sitting posture. Further, the methodology and results could be implemented for other digital medium users and industrial workers working in prolonged flexed postures.
Ethics statement
The study was approved by the SRM Medical College Hospital and Research Centre (ethical clearance number: 1980/IEC/2020) and performed in accordance with the Declaration of Helsinki.
Informed consent
Informed consent was obtained from all subjects involved in the study.
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
The authors thank the Robotics Lab of the Department of Mechanical Engineering at SRM Institute of Science and Technology, Kattankulathur, India, for providing the required facilities for this research study.
Funding
This research received no external funding.