
Abstract
BACKGROUND:
Work ability meetings (WAM) are an essential and common tool of disability management in occupational health services in Finland. Meetings are held between an employee, a supervisor, and an occupational physician (OP). The aim is mainly to support work ability.
OBJECTIVES:
To describe challenges and resolutions in the meetings as described by OPs.
METHODS:
An internet survey was emailed to the members (n = 1304) of the Finnish Society of Occupational Health Physicians in August 2014. We asked physicians to describe those WAMs they had attended, especially challenges and resolutions concerning WAM.
RESULTS:
A total of 302 (23%) OPs responded to the survey. Most severe of the challenges were personal conflicts and a lack of confidence between the parties at the workplace. Also, the participants’ views may differ about the purpose and goal of the meeting. The respondents noted that the employer might be unable to organize modified work for disabled employees. As a resolution, OPs need to prepare well and maintain their professional and neutral role in WAMs in all cases. OPs also mentioned the need for training in insurance medicine and rehabilitation as well as skills as a mediator.
CONCLUSIONS:
WAM is a potential tool for return to work and disability management in collaboration between employees, employers, and occupational health when all the participants reach a common goal and become aware of their role in the process. OPs need to recognize possible conflicting interests and contact each party before WAM. Keeping confidentiality in WAMs is a crucial matter.
Keywords
Introduction
The work ability meetings (WAMs) are negotiations where an employee, a supervisor, and an occupational health service (OHS) physician meet to manage the employee’s work disability or to find solutions to the employee’s return to work (RTW) problems [1]. With an ageing workforce, the WAMs have become a popular intervention in Finnish OHS, as it has shifted its focus from primary prevention of occupational diseases towards the protection of work ability [2]. Furthermore, since employers in Finland are obliged to organize occupational health care for all employees by law [3], OHS has a unique opportunity to provide services to support the maintenance of work ability of all employees.
In Finland OHS’s main interest is to support the work ability in the context of workplace and the employer, who pays the OHS’s services [3]. The employee is served by OHS, and the insurance system compensates lost working time to the employer or the employee by the certificate of OHS.
WAMs solve work ability and return to work issues and – problems in a discussion between an employee, a supervisor, and an occupational physician. For practical reasons most WAMs are hold without assistance of other OHS practitioners such as OHS nurses. Physicians should have good negotiation skills which include effective communication of goals, needs, and wants [4]. Essential skills include leadership, effective communication, and negotiation within an ever-changing milieu, not only differences between generations but also ethnicity, race, and sex [5]. Good negotiation skills could enhance the effectiveness of one’s strategies to execute change and increase organizational performance [5].
More research on the conduct, outcomes, quality, and effectiveness of WAMs is needed. In a survey of all Finnish OHS units in 2005, WAMs or joint discussions were mentioned only by 10% of units as one of the RTW practices [6]. Nowadays, occupational physicians (OPs) use WAMs in their everyday work. About half of the supervisors have participated in WAMs [7]. The contents of WAMs from the perspective of OPs, the criteria to call up these meetings, and the contents and action plans made are published earlier [8].
Today, most OHS physicians have this WAM intervention in their toolbox. However, more is still needed to know about the conduct of WAMs. This survey aimed to study challenges, resolutions, facilitating factors and beneficial procedures in WAM.
Methods
An Internet survey was sent to OPs who were members of the Finnish Society of Occupational Health Physicians and had an email address. There were approximately 1650 members in the society in 2014. We targeted the survey on members at clinical work since OPs participate in WAMs.
This survey focused on WAMs the physician had attended, the challenges, e.g., conflicts at the workplace, attitudes and motivation of supervisors and employees, as experienced by physicians, and factors that made easier and benefitted the WAMs.
We formulated the questionnaire using the authors’ experience on WAMs and the comments of the five occupational health physicians in the piloting phase. We sent the survey in August 2014, with two reminders to enhance the percentage of respondents. All the authors are also experienced OPs in practice and WAM is in their everyday use. Questionnaire was formulated by NH, JL and AL. Qualitative analyses were made by all the authors and quantitative analyses were made by JL.
In an open-ended question, we asked about the challenges the physicians had faced in conducting WAMs. In the same way, we asked about factors which make WAMs easy and successful. In addition, we asked an open-ended question about processes and practices that benefit WAM. Then we formulated the main categories of challenges and facilitators. Questions were” By your experience what makes WAM challenging? By your experience what makes WAM easy? What kind of procedures or preparation help WAM? “
Then all three authors classified responses to two first questions into emerging categories, and NH analysed and classified the question three. In cases where all three authors agreed, the response was included in a particular category. Some physicians reported several challenges and facilitators resulting in more than one response for each participant. The responses in each category were counted and summarized in verbal form.
The results were analyzed using descriptive analysis by IBM SPSS for Windows (version 27, IBM Corp., Armonk, NY, USA).
Results
We sent the emails to 1304 members, and 17 emails were returned informing that the recipient was retired or working outside OHS. As a whole, 302 (23%) OPs responded.
The responding OPs were more often women (69%), and their mean age was 51.6 years (SD 8.6 years). The majority of them were specialists in OHS (59%). Their most common workplace (57%) was in the private sector and less often in municipal (20%), employer’s own or jointly organized OHS (20%). Most OPs (84%) had worked in the OHS for at least seven years. They were experienced in participating in WAMs and most often attended them weekly (mean 4.4 per month, SD 3.4). The OPs assessed their level of professional competence as good, and 9% considered themselves experts.
Challenges in meetings
A total of 259 (85%) physicians reported challenges in the WAM process. The challenges included problems in the process, participants or the OHS role (Fig. 1).

Challenges in work ability meetings (%).
The most striking challenge in meetings was a conflict between parties. Of all the respondents, 25% reported conflict as a challenge. Mistrust and personal conflicts in the workplace may hinder fruitful negotiations for a RTW. In addition, a conflict of interest from both the supervisor’s and employee’s sides may complicate the process. Employers who are unfamiliar with work accommodations or dealing with employees with mental or physical disabilities are not willing to offer work with reduced demands or modified work tasks. Employees with current medical limitations in their working capacity may lose their motivation and interest in their previous work tasks. Of the respondents, 17% mentioned contradicting goals as a challenge in meetings.
The participants’ views on the meeting’s purpose and goals may differ. The motivation and willingness to negotiate a solution, redesigning the work tasks or reformulation the work duties, may differ or lack totally. Moreover, the interpretation of the cause of the problem, health, or motivation, may vary.
In some cases (11% of responses), no solution was settled for example, suppose the supervisor highlights economic benefits and productivity in a short-sighted way, and the employee is unwilling to discuss the causes and consequences of the health problem. In that case, the WAM may end up with no result. To reach a solution, cooperation and goodwill are needed from both sides.
If the supervisor and the employee cannot discuss the problems together, the WAM negotiation may start with quite distant views and the role of the OHS becomes crucial. Then, the OHS contributes by getting the parties to negotiate and cooperate towards a common goal.
An employer may not have realistic possibilities to organize modified work for the employee with health-based limitations. Uncertainties in the forthcoming health status and work ability can make supervisors wary of modifying work. The employees may need to improve their professional skills to allow realistic options for a new work plan. Also, the passive and negative attitude of the employee may hinder all attempts to modify work tasks.
Participants
The participants’ attitude (14%) and motivation (12%) emerged as one of the major challenges of WAMs. Several responders adduced that one of the challenges of the WAMs is the participant’s lack of motivation or commitment to the process. Some employees seem not to have any motivation to work, or their motivation is relatively low. Also, the participants are not motivated to find and commit to the solutions in the WAM. Some employees or supervisors would not like to participate in the WAM at all.
If the supervisor will or cannot take the employer’s responsibility, they will or cannot suggest any work arrangements or other solutions. Several respondents notified that some supervisors don’t have any understanding, knowledge, or previous experience in handling those cases. The situation is challenging if the participants are not oriented or prepared for the upcoming work ability meeting. On the other hand, some participants have strong opinions of the situation or the desired results in advance.
Participants may be inflexible and refuse collaboration in the WAMs, or they refuse to reveal the essential facts affecting work ability. According to the responders, it is also challenging when some participants behave inappropriately or depreciatingly in the negotiation. For example, sometimes, the participants emphasize economic issues over the compromise. Sometimes the participants also want to use the WAM inappropriately.
OHS
Strict confidentiality of medical information (11%) or denying any handicap from the employee’s side may block realistic planning of work accommodations. Unrealistic optimism and the desire for a solution may mislead occupational health service to recommendations which do not work in practice.
In the WAMs the OHS physician must be able to reveal a sufficient description of the employee’s work ability without giving confidential information to any outsiders, including the supervisor. The secrecy of medical facts may cause problems when aiming to solve health-related issues in the negotiations. It is also the case when the employee does not want all the health issues affecting her/his work ability to be discussed in the negotiation. This kind of decision should be made in agreement with the employee.
Contradictory role of OH physician’s (7%) as a chairperson and secretary at the same time is also a challenge. A physician should be active and lead the conversation towards workability, cool down the discussion when needed, and remain neutral and constructive in the negotiation.
Negotiation skills and knowledge are needed. The OHS physician shall keep a neutral attitude and be objective. Physicians should be able to read the situation and silent signals, listen, and activate the discussion. Also, the physician would find common advantages, coordinate different opinions, be diplomatic, solve the situation and make compromises without dictating attitude. Physicians find it challenging to show determination, courage, and resiliency, and to make a difficult decision when needed. OP's knowledge of rehabilitation and insurance medicine is needed in WAMs. Legal advisers and union members as participants in the WAMs are considered as a challenge rather than a resource.
Resolutions (facilitation factors and beneficial procedures) for meetings
The responders identified several factors which may contribute to an effortless WAM in this study. In addition, the responders also adduced beneficial procedures preceding WAMs. Experience of the participants (21% of responses), trust between them (8%) and their clear roles (7%) facilitated the negotiations. (Fig. 2).
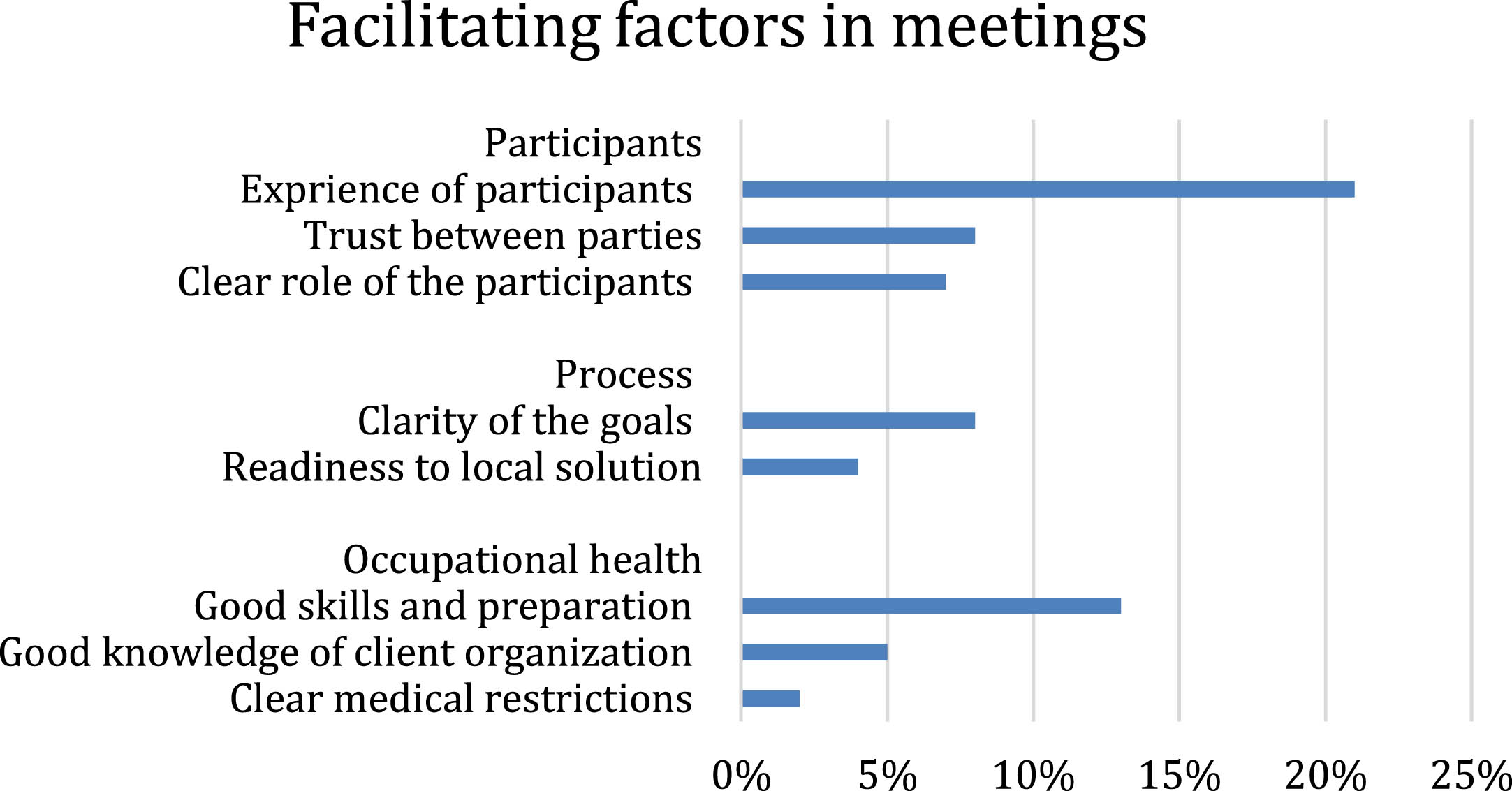
Facilitating factors in WAM.
Clarity of the goals (8%) and readiness to local solution (4%) facilitate the process. For an effortless meeting, transparent and shared objectives between the participants are needed, as well as a genuine desire to solve the present situation the likelihood of a successful WAM increase when the participants work together to achieve common goals. The participants’ motivation and attitude affect the WAM’s outcome. Also, so when the participants are well prepared for the negotiations. The preparations could include, e.g., assessing the viable solutions before the WAM. Since communication skills do affect negotiations, the responders found it essential that trust, mutual respect, and cooperation between the participants exist before the implementation.
Moreover, it is easier to conduct WAM when the participants know each other beforehand and there are no conflicts between them. Honesty and transparency are also crucial. The compassionate supervisor improves the possibility of a successful WAM. The WAM is easier to conduct if all the participants are familiar with their roles in the negotiation. In addition, it helps if the process is adequately described with structured forms and note-collecting protocols.
The most critical factor in aiding the WAMs was the OP’s experience in negotiation and preparation in advance (13%) and knowing of the client organization (5%). Explicit medical restrictions (2%) in the employee’s tasks were mentioned only a few times.
As a beneficial procedure preceding WAMs, it is essential to support and familiarize the employee with the WAM, hear the employee’s wishes and expectations for the WAM’s outcomes, and agree upon which topics are included in the negotiation. Preparing and hearing the supervisor’s view is similarly beneficial. The supervisor’s benefit from familiarization with the aims and goals of the WAM and need supplementary information for this kind of negotiation.
It is also helpful that the supervisor has acquainted himself/herself with the work ability case when preparing for the negotiation. It was beneficial that the supervisor and the employee discussed before the WAM.
About half of the responders found it essential to understand the employee’s state of health clearly. Subsequently, OP's appointment preceding WAM is needed for an up-to-date work ability estimate.
Also, proper knowledge of the workplace and a job description as well as to be aware of the possibilities of work modifications are helpful when the physician is orientating to the negotiation. Several responders found it essential to discuss with the supervisor before the WAM. This helps prepare the supervisor to plan and prepare for the possibilities and alternatives in the work arrangements. In addition, physicians found it favorable to have an individually planned action plan before WAM. Finally, some responders found it advantageous to have strict guidelines for the WAM protocol.
According to our study, the most striking challenge in work ability meetings is a conflict between supervisor and employee and a lack of confidence between the workplace parties. The views and goals of the participants may differ, and sometimes, no common solution is reached. Also, employers may have little possibility for adjusted work. To ensure success, an OP needs to prepare for the meeting and contact both parties beforehand, in particular if there is any doubt about the problems in the meeting. Good information on the work ability and the work tasks of the employee and work accommodation options in the workplace helps OPs to succeed, as does confidentiality of the conduct.
Despite the close connection of OHS to the workplace and employee work ability, negotiations are not always easy or straightforward and may have challenging factors. In these cases, occupational health physicians can feel helpless in front of arguing participants. Supervisors may even blame OHS for failure in the meeting. OHS may also be considered too passive or unrealistic concerning workplace realities [9]. Mediation can help in resolving workplace relationship conflict [10, 11].
Seing et al. [1] reported an unequal distribution of power among cooperating actors as employers often determined whether persons could return to work and if they had sufficient work ability. In RTW negotiations, three perspectives prevail: medical, workplace and regulatory perspectives, and each one should be considered in the process [1].
We found that employers need clarification about the work ability of the returning employee. Clear work modification advice or explicit medical constraints in the employee’s tasks are beneficial and effective in the return-to-work process [12]. Occupational physicians offer important information to the supervisor on the health-related factors in the ‘trial and error’ process of return to work [13]. Developing collaborative working relationships helps to manage the situation in complex environments [14]. In the negotiation process, the occupational health physician is also a broker between the employer and the insurance system. Supervisors often consider the OHS role beneficial and essential, but they want control over the process. The role of OHS is best as a consultant to the employer [8].
MacEachen et al. [15] have pointed out that communication barriers must be overcome to support work ability and the return-to-work process. Further physicians should be well advised to hone their skills of negotiation so that they resolve divergence of interests. Physicians, as a negotiator, should identify the needs in the negotiation and establish their best alternative [3]. A fundamental goal in any negotiation should be establishing a relationship and seeking an agreement that provides win-win opportunities for all parties. Negotiations skills can be attributed to integrity, credibility, effective listening, having a vision of the destination, fairness, humility, and caring [16].
In our study the WAMs seemed to be more accessible and more successful when the occupational health physician had experience in negotiations and was familiar with the case in advance. Also, the meetings were more manageable when all the participants were prepared for the negotiations, were familiar with their roles, and cooperated to achieve common goals. Preparing employees and supervisors for the negotiation and having a definite action plan for the meeting supported the success of the OHS. Juvonen-Posti et al. [17] have reported that the experiences of the participants highlight the importance of being heard, gaining information, and finding concrete mutual solutions.
In this study, motivational issues emerged as one of the major challenges in meetings. The participants may need to commit to the process and solve the situation. Also, the views on the purpose and goals of the meeting may differ. Some disabled employees are not motivated to work, or their motivation is relatively low. Different aspects of work motivation of disabled employee can be acquired in a targeted interview [18]. Motivation and interest in the work may be even more critical than health issues.
Similar interventions to WAM exist in other countries called RTW coordination interventions [19] or RTW case conferences [20]. In Sweden RTW coordination is managed by RTW coordinators in public health settings [21]. In Denmark case managers are either specialist in social medicine, social workers, or occupational therapist [22]. Experts for resolving workplace relationship conflicts are also needed for mediation [9].
The health care professional must safeguard the secrecy of health information [23]. In addition, the General Data Protection Regulation [24] applies to all access and use of patient records. Thus, physicians are also obligated to the secrecy of health information in the work ability meetings.
Healthcare professionals face privacy problems when having dual loyalties towards employees and employers [25]. Based on a survey study, the dual loyalty of issues in occupational health service is most validly solved in the tripartite cooperation when dealing with delicate subjects from a privacy point of view, such as drug and work community problems, sexual harassment, and work ability [26]. WAM with all parties concerned is an efficient means to achieve rehabilitation goals and tackle injurious work assignments and reduced motivation to achieve sooner return towork [27].
In our study, confidentiality emerged as one of the challenges in the meeting, but it was not prominently emphasized. The obligation of confidentiality is a crucial and self-evident part of professional ethics, which might explain the small number of answers concerning the confidentiality issue in this survey. In this study, the occupational physicians were quite experienced in their jobs and, therefore, also experienced in cooperating with employees andemployers.
The study had some limitations. First, we developed the questionnaire for the needs of this survey, and the validity or reliability of the questionnaire was not tested. Secondly, since our survey concerned the occupational physicians who were members of the Finnish Association of Occupational Health Physicians and whose email addresses were available, some of the members were not contacted. The study is from year 2014, but the process of WAM and the role of the physician are the same also later. The response rate was 23% which was moderately low and may cause selection bias. Finally, this was a survey for charting the physicians’ experiences of WAM in OHS. The meeting challenges and resolutions might differ if employees or managerswere asked.
In the future the strengthening of the facilitating factors of WAM should be studied as well as the effectiveness of the WAM in whole in the return-to-work process. Studying other participants view of WAM could be worthwhile.
Conclusion
Work ability meetings between occupational health, supervisor and employee can facilitate return to work and disability management and help stakeholders resolve differences in rehabilitation options. Good preparation and clear roles help in conducting the meetings. However, sometimes a contested terrain of interests and motivations prevails, and the physician needs negotiation skills and experience in the meeting.
Author contributions
All authors contributed to the study's conception, design, and material preparation. Data collection was done by NH and quantitative analysis was performed by JL and qualitative analysis was done by all authors. All authors contributed to writing the manuscript, full text reading, and extraction. All authors read and approved the manuscripts.
Compliance with ethical standards
Ethical approval is not needed for a survey which do not collect any confidential data. This survey concerns occupational health physicians’ experiences of WAM and they answered anonymously. Physicians or patients cannot be identified.
Informed consent
Not applicable.
Conflict of interest
The Authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
None to report.
Funding
The authors report no funding.