
Abstract
BACKGROUND:
Professional drivers are most likely to experience work-related neck pain due to awkward sitting positions for extended periods of time. Globally, millions of people depend on drivers who dedicate their lives to the craft. However, there is a paucity of data available on professional drivers suffering from neck pain or other musculoskeletal pain in Pakistan.
OBJECTIVE:
To investigate the prevalence of neck pain and its association with postural and ergonomic factors among Pakistani professional drivers.
METHODS:
This was a cross-sectional study conducted from January to June 2022 among 369 professional drivers located in Faisalabad, Pakistan. The data were collected by using a questionnaire comprising different sections, including personal, postural and ergonomic factors among drivers. The Statistical Package for the Social Sciences (SPSS) 25 was used for data entry and analysis.
RESULTS:
The mean age of the participants was 40.83±9.27 years. Among the 369 participants, 129 reported neck pain. The period and point prevalence of neck pain were 35% (n = 129) and 31% (n = 115), respectively. Professional drivers reported a significant association between habitual forward posture and head–neck posture (p = 0.000) and between habitual forward posture and trunk posture (p = 0.000) with neck pain. In addition, ergonomics training (p = 0.002), ergonomics awareness (p = 0.002), and mobile use while driving (p = 0.000) were significantly associated with neck pain.
CONCLUSION:
This study revealed that drivers have greater period prevalence of neck pain than point prevalence. Moreover, this study revealed that age, BMI, lifestyle, health status, medication use, and smoking habits were associated with neck pain in drivers. Drivers who had ergonomic training and awareness were significantly less likely to suffer from lower neck pain. Drivers with a habitual forward posture are more likely to suffer from neck pain than are drivers with a prone posture.
Introduction
Work-related neck pain (WRNP) is the second most frequent complaint of the musculoskeletal system in the working population and is considered the fourth leading cause of disability worldwide [1–3]. According to a recently published study of the global burden of disease, the incidence of neck pain was 65.3 million, and the prevalence of neck pain was 288.7 million in 2017 worldwide [4]. The economic burden of neck pain is remarkable and includes treatment costs, reduced productivity and job-related problems. In 2016, among the 154 health conditions, low back and neck pain had the highest health care spending in the United States, with an estimated 134.5 billion dollars. In 2012, neck pain was responsible for job absences among 25.5 million Americans, who missed an average of 11.4 days of work. In 2017, the global age-standardized prevalence and incidence of neck pain were 3551.1 and 806.6 per 100,000 people, respectively [5].
The biomechanical risk factors identified for work-related neck pain are a complex combination of personal, ergonomic, psychological, postural, social, and environmental conditions [6]. Many professionals are affected by neck pain, such as drivers, dentists, teachers, medical doctors and paramedical staff, computer users, and factory workers, in different ways depending on the nature of their work [7, 8].
Among these professions, professional drivers are the occupational group most affected by WRNP [3, 11]. Professional drivers are individuals whose main function is to drive and handle motor vehicles for public transport over longer periods of time [8, 12]. Driving demands that the driver use repeated physical effort or intense muscular force to carry out different work-related tasks [10, 12]. The incorrect and abnormal postures that are usually assumed by professional drivers are multitasks, habitual forward posture and pimps and racer posture [10]. The multitask posture describes the posture that a driver assumes while performing multiple tasks simultaneously, such as texting, eating, or adjusting the radio. The habitual forward posture occurs when a driver leans forward while driving, perhaps due to long hours behind the wheel. A “pimps and racer” driving posture refers to a lower seating position and a firm grip on the steering wheel [10]. According to previous studies, habitual forward head posture has been viewed as an important postural component of WRNP in professional drivers [10, 14].
Abnormal posture alters the muscular length-tension relationship, increases muscular activity and causes hypo-lordosis at the cervical spine, thus leading to hyperflexion of the lower cervical spine and hyperextension of the upper cervical spine. All these changes alter the biomechanics of the cervical spine and subsequently cause pain [15, 16]. An imperfect and unsuitable vehicle seat design has also been recognized as a significant risk factor that directly affects the posture of drivers [17, 18]. Neck pain associated with work is also expected to become more prevalent in developing countries as young generations age [8]. Pakistan is an underdeveloped country, and according to reports, there has been a progressive increase in the number of drivers that serve the economy of Pakistan. Most of the studies in Pakistan have reported on WRNPs in housekeepers, teachers, mobile users, and dentists [19, 20]. To the best of authors’ knowledge, there is a lack of literature on work-related neck pain and associated postural and ergonomic factors among Pakistani professional drivers. The aim of this study was to determine the prevalence of neck pain among professional drivers in the city of Faisalabad, Pakistan, and its association with ergonomic and postural risk factors.
Methods
This was a cross-sectional survey among the professional drivers of Faisalabad, Pakistan. The data were collected from 11 randomly selected sites, including car stands, buses, urban transports, trucks, and semitrailers of Faisalabad, using a convenience sampling technique and after permission from the bus station administrators. The study included male professionals working for companies or self-employed individuals who had been driving for at least 12 months and for at least six hours per day or more and who were willing to participate. Drivers with a history of surgery in the cervical region, such as removal of the vertebral disc, whiplash injury, removal of the spinous process of the cervical vertebrae or recent trauma, including serious accidents, injuries or fractures, and neurological impairments, such as traumatic brain injury and tumors, were excluded. This study was approved by the Research Ethical Committee of Riphah International University Islamabad, Pakistan Written informed consent was obtained from the participants before the one-on-one interview.
An online sample size calculation tool called EPITOOL [21] was used to calculate the sample size using a confidence level of 0.95 and a margin of error of 5% with a population size of 20,000. A sample of 369 professional drivers was used for the current study.
Data collection procedure
The data were collected by using an extensive questionnaire comprising questions such as personal factors, work-related factors, postural and ergonomic factors, and characteristics of pain, including intensity (using the visual analog scale) [22] and assessment of musculoskeletal complaints (using the modified Nordic Musculoskeletal Questionnaire) [23, 24]. (Annexure-I)
Personal factors, work-related factors, and characteristics of WRNP
The first section consisted of questions addressing personal factors such as sex, age, weight, height for BMI calculation, marital status, dominance of hand, status of physical activity, education status, history of smoking and alcohol status, any history of injury or trauma, and medical history asked from the participants [12]. For work-related factors, various questions, such as job nature, driving hours in a day, overtime work, total experience in the profession and in current place, frequency of taking breaks in a day, average mileage per day, and safety training, were asked [12]. Questions about the postural factors of drivers while driving were asked after assessing their sitting posture, standing posture (cervical, thoracic, or lumber curves were increased, decreased, or normal, respectively) [25].
Ergonomics, vehicle characteristics, WRNP characteristics and neck range of motion
Questions about ergonomic factors such as mobile use while driving with or without hand frees, the position of the arm and neck during driving, and whether ergonomic training was received were asked [26]. Question regarding the characteristics of the vehicle were completed by measuring different angles, such as the seat back angle and distance from the steering wheel, and questions such as the mirror used and adjustability of the vehicle, such as seat height, steering wheel, and seat back space, were asked from professional drivers [12]. Questions about WRNP characteristics, such as neck pain frequency; duration, type, and onset of neck pain; and exaggerating and alleviating factors, were collected [27]. The neck range of motion was measured by using a bubble inclinometer in all directions, including flexion, extension, right side bending, and left side bending [28].
Musculoskeletal disorder screening using the Modified Nordic Musculoskeletal Questionnaire (MNMQ)
“The Nordic Musculoskeletal Questionnaire (NMQ) originated from a program which was financed by the Nordic Council of Ministers “to screen Musculoskeletal disorders [23]. It can be used as a questionnaire or as a structured interview to assess low back pain, neck pain, upper extremity pain, and lower extremity pain [23]. This questionnaire has been used to identify musculoskeletal disorders in different regions of the human body in epidemiological and surveillance studies [23, 24].
Musculoskeletal manifestations in working populations are well recognized by using the approach of the Health and Safety Executive (HSE) [23]. The highest frequency rates of musculoskeletal pain and associated issues were reported when this questionnaire was provided as part of a specific study on musculoskeletal problems and working factors rather than when it was administered periodically as part of a general health examination [23]. It can also be used as an assessment tool to rule out MSDs in an ergonomic setting and for the health care of the working population to detect whether anybody has issues with their locomotor system [24].
The Modified Nordic Musculoskeletal Questionnaire has been applied to different groups of occupations and worker chains, such as call focus laborers, vehicle drivers, health care workers and ranger service laborers, including construction workers, to assess musculoskeletal issues [23, 29]. Reliability and validity are the two most essential elements for the assessment of different outcome measuring tools [24]. The validity and reliability of the modified Nordic Musculoskeletal Questionnaire, which is a test–retest procedure, have been assessed in different countries, and the questionnaire has been reported to be the most valid and reliable tool for assessing musculoskeletal pain [23].
Moreover, the Modified Nordic Musculoskeletal Questionnaire is a significant questionnaire for the assessment of musculoskeletal symptoms; it consists of 36 structured questions with two choices, yes or no, divided into four columns to assess different regions of the human body with musculoskeletal issues [23, 24]. It consists of a body map that represents nine parts of the human body [23]. Participants were asked if, in the last 12 months, they had any pain or trouble that interferes with performing normal activities of daily living. The presence of any functional impact or musculoskeletal pain in the last 7 days was determined if the patients had visited any health care professional for assessment [23]. This process is completed by selecting the Yes or No options given in each column. (56)
Assessment of pain intensity using the visual analogue scale (VAS)
The VAS is a pain rating scale that was originally designed in 1921 by Patterson and Hayes [30]. It is the most valid and reliable instrument for assessing or subjectively measuring the intensity of pain for both acute and chronic pain patients [30]. The VAS comprises a 100 mm horizontal line with the terms “no pain” on the left side of the scale (0 cm) and “worst pain” on the right side of the scale (10 cm) [31]. The VAS depends on self-reported symptoms of pain that are measured by a hand mark at any point between no pain and the worst pain relevant to the intensity of the patient’s pain [30].
Patients were asked to mark the level of their neck pain by underlining the point or by making a circle on the point of interest of the horizontal line that best describes the level of intensity of pain from the last 24 hours [31]. This tool is most widely used in clinics, home settings and for research purposes [30]. The score obtained from this scale can also be used to assess the progress of patients toward recovery by comparing the scores with the previous score, and we can also compare the level of pain perceived by patients with similar pathologies [30].
The questionnaire was tested by an expert panel to determine whether it met the study objectives, and changes suggested by the expert panel were incorporated into the questionnaire. To determine whether each question was valid, a pilot study was conducted before the survey began.
The principal investigator and two other investigators specializing in physical therapy took 12–15 minutes to collect data from each participant. Then, the participants were asked to sit on their driving seat as they siting while driving for 5 minutes to assess their posture while driving and to evaluate the characteristics of the vehicle, such as seat back angle, distance from the steering wheel, seat angle, adjustability of the driving seat height, frequent use of mirrors during driving and the presence of a seat cushion with back support [28].
Statistical analysis
Using SPSS version 25 for Windows, the data were entered and analyzed. A binary logistic regression test was used to assess associations between work-related neck pain and risk factors. A P value less than 0.05 was considered significant. The odds ratio was calculated to determine or quantify the strength of the association between WRNP and its associated risk factors.
Results
The purpose of this study was to determine the prevalence of work-related pain in the neck and its association with risk factors among professional drivers. For this purpose, 369 professional drivers were selected from different vehicle stations based on predefined criteria. The current study reported that three hundred and sixty-nine males were from different age groups, and most of them were from the 25–34 age group (225 [61%]). The mean BMI score was 26.47 (M = 26.47, SD = 3.38). A total of 236 (64.0%) participants were living a sedentary lifestyle, 130 (35.2%) were living an active lifestyle, 133 (36.0%) were engaged in exercise, and the majority (236; 64.0%) were not performing exercise. All the participants (369, 100.0%) were right-handed (Table 1). A driver considered active is one who runs more than 3 miles at the same pace or engages in physical activity of equal intensity and quantity.
Demographic profile of the participants

Demographic profile of the participants
Overall, 62 (16.8%) participants developed habitual forward driving postures, 35 (9.5%) participants developed multitasker driving postures, and 6 (1.6%) and 266 (71.9%) participants developed Pmp postures while driving. There were 150 (40.7%) participants with normal postures in the sitting, standing, sitting trunk, and standing postures and 219 (59.3%) participants with increased postures in the sitting, standing, sitting trunk, and standing postures. Twenty-six (7%) participants had flat backs in both the sitting and standing positions, while 306 (81.9%) had normal lumbar spine postures in both the sitting and standing positions. Thirty-seven (10%) participants had hyperlordotic lumbar spine postures in both the sitting and standing positions (Table 2).
Participants’ information on postural and ergonomic factors

The findings of the current study revealed that 89 (24.1%) participants had taken ergonomics training for driving, 89 (24.1%) participants had attended ergonomics awareness training sessions, 43 (11.7%) participants had attended 1–2 ergonomics awareness sessions, 252 (68.3%) participants were using mobile phones during work, 84 (33.3%) were using mobile phones without hands, 168 (66.7%) were using mobile phones without hands, 4 (1.1%) participants positioned their arms above shoulder level during work, and 365 (98.9%) participants positioned their arms below shoulder level during work. A total of 339 (91.9%) participants had arms that were comfortable during work, 30 (8.1%) participants had arms that were not comfortable during work, 148 (40.1%) participants had neck, back, and shoulders that were comfortable during work, 221 (59.9%) had neck, back and shoulders that were not comfortable during work, 62 (16.8%) participants had back problems, and 129 (34.4%) participants had neck problems. Thirty (8.1) participants had a shoulder problem (Table 2).
There was a significant association between normal weight, overweight BMI, and neck pain. Seventy (80.5%) participants had no neck pain, while 17 (17.5%) had neck pain in the normal weight group. (CI = .10–.438, p = .000). One hundred thirty-nine (63.5%) participants had no neck pain, while 77 (36.5%) had neck pain in the overweight group. (CI = .330–1.056, p = .036) (Table 3).
Association of work-related neck pain with personal factors of participants (N = 369)

95% CI – 95% confidence intervals (CI), binary logistic regression (adj) OR-odds ratio, *Significant at p < 0.05.
The findings of the study revealed that 129 (35%) drivers had a period prevalence and 115 (31%) had a point prevalence. Professional drivers driving urban transport (transport in urban areas) had the highest prevalence of WRNP (35%), while those driving cars had the lowest prevalence (9.3%) (Figs. 1 and 2).
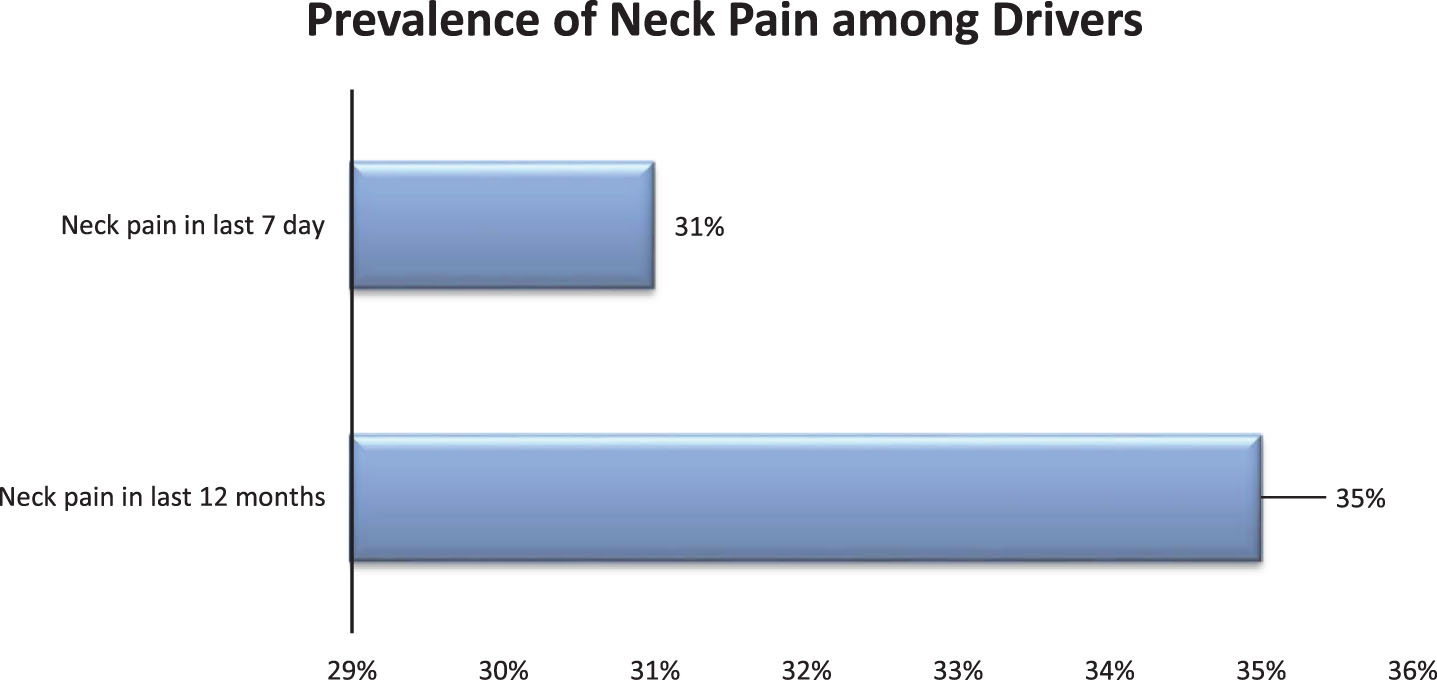
Prevalence of neck pain among professional drivers.

Prevalence of work-related neck pain among professional drivers of cars, buses, trucks, urban transport and semitrailers.
In this study, the majority of participants (65%) did not experience neck pain, while 0.5% experienced mild neck pain during rest, 34.4% experienced moderate neck pain during work, 30% experienced mild neck pain, and 4.6% experienced moderate neck pain during rest (Fig. 3).

Neck pain intensity of drivers during rest and during work.
Binary logistic regression was used to determine the associations between postural factors and neck pain. There was an association between posture acquired while driving and neck pain. There was a 7.691-fold greater risk of neck pain in the habitual forward posture group than in the jejunal posture group (p < .001, CI: 4.060–14.569). There was a.01-fold lower risk of neck pain due to a normal sitting head–neck posture than due to an increased sitting head–neck posture (p < .001, CI:.002–.041). There was a.01-fold lower risk of neck pain due to a normal standing head–neck posture than due to an increased standing head–neck posture (p < .001, CI:.002–.041). There was a.01-fold lower risk of neck pain due to a normal sitting trunk posture than due to an increased sitting trunk posture (p < .001, CI:.002–.041). There was a.01-fold lower risk of neck pain due to a normal standing trunk posture than due to an increased standing trunk posture (p < .001, CI:.002–.041). There was a.01-fold lower risk of neck pain due to a normal sitting trunk posture than due to an increased sitting trunk posture (p < .001, CI:.002–.041). There was no significant difference in the handgrip strength of the right hand for patients with no neck pain or neck pain. There was a significant difference in the handgrip strength of the left hand for patients with no neck pain (29.39±1.82) or neck pain. (30.10±2.09). There was a 9.168-fold greater risk of neck pain when the trunk was approximately perpendicular to the floor than when the trunk was not perpendicular to the floor (p < .001, CI:.2.78–.30.18). There was a 6.203-fold greater risk of neck pain in hips than in knees (p < .001, CI:.2.75–.14.004) (Table 4).
Association of postural factors with and without neck pain in participants (N = 369)

The binary logistic regression results showed that there was a significant association between “yes” ergonomics training and neck pain. Seventy (78.7%) participants had no neck pain, while 19 (21.3%) had neck pain in the yes group. (CI = .239–.735, p = .002). One hundred and seventy (60.7%) participants had no neck pain, while 110 (39.3%) had neck pain in group no. Binary logistic regression showed that there was a significant association between the ergonomics awareness session group attended and neck pain. Seventy (78.7%) participants had no neck pain, while 19 (21.3%) had neck pain. (CI = .239–.735, p = .002). One hundred and seventy (60.7%) participants had no neck pain, while 110 (39.3%) had neck pain in the group who did not attend. Binary logistic regression showed that there was a significant association between following any recommendation of “yes” and neck pain. One hundred and fourteen (97.4%) participants had no neck pain, while 3 (2.6%) had neck pain in the yes group. (CI = .008–.085, p = .000). One hundred and twenty-six (50.0%) participants had no neck pain, while 126 (50.0%) had neck pain in group no. Binary logistic regression revealed that there was a significant association between mobile use during workgroup “yes” and neck pain. One hundred and twenty-six (50.0%) participants had no neck pain, while 50 (126%) had neck pain in the yes group. (CI = 11.8–122.8, p = 0.00). One hundred and fourteen (97.4%) participants had no neck pain, while 3 (2.6%) had neck pain in group no. Participants who responded yes varied from each other according to their results. Fifty-two (61.9%) participants had no neck pain, while 32 (38.1%) had hands-free neck pain. Seventy-four (44.0%) participants had no neck pain, while 94 (56.0%) had hands-free neck pain (Table 5).
Association of ergonomic factors with and without neck pain (N = 369)

Sitting on an uncomfortable seat for a long period of time with continuous microvibration due to uneven road surfaces and the vibratory motion of the engine is an inescapable part of drivers’ daily routine. With the passage of time, various changes have been made in vehicles and driving factors due to advancements in technology, which require specific rules or guidelines to be followed for proper vehicle functioning. Several studies have reported that work-related neck pain is the most frequent complaint of drivers and significantly affects their work efficiency [32, 33]. In this cross-sectional study, we assessed work-related neck pain incidence and its association with ergonomic and postural risk factors.
According to this study, 35% of drivers experienced neck pain. These results are supported by the study of Rehan et al., who reported that 34% of drivers experienced work-related neck pain [34]. In contrast, Alperovitch (2010) reported that WRNP was present in 21.2% of drivers, followed by shoulder pain in 14.7%, upper back pain in 8.3%, elbow pain in 3% and wrist pain in 3% of bus drivers due to uncomfortable seats and disturbed ergonomics [35]. In contrast, another study conducted in 2016 concluded that 18% of drivers experienced neck pain, 6% felt pain in the upper back, and 6% reported pain in the lower back [10]. The variation in results might be because of variations in driving experience, total driving hours in a day and circumstances faced during driving.
This study revealed that work-related neck pain was significantly associated with personal factors, such as age (35–54 years), BMI, and health status, in participants with a p value less than 0.05. Participants aged 25 to 54 years reported more work-related neck pain. This finding is consistent with the results of Shariat, Ardalan, who reported that there was a significant association between musculoskeletal pain and age groups ranging from 15 to 45 years and that musculoskeletal pain was significantly associated with health status and BMI [36]. Another study by D.G. Hoy reported that neck pain is more prevalent in 35- to 49-year-old participants. This may be because of the increase in neck pain in participants with age due to age-related changes in bones and muscles [37].
Our study reported that smoking is significantly associated with WRNP (p value less than 0.05), as participants who did not smoke were at least at risk of developing neck pain compared to those who were currently smoking. A study in Japan concluded that smokers were at greater risk of pain development [38]. Another study conducted in Saudi Arabia supported this finding; in this study, Meo et al reported that workers who smoke had greater manifestations of musculoskeletal system pain [39].
This study reported that out of 129 participants with WRNP, only 25 (6.8%) had pain on the right side of the neck, while the majority (104; 28.2%) had neck pain on both sides of the neck. The findings of this study are consistent with those of the G.P.Y. Szeto report, which concluded that neck pain in urban transport drivers in Hong Kong is chiefly reported on both sides of the neck [25]. On the other hand, in contrast to this study, another study concluded that only 9% of the drivers experienced bilateral neck pain, and 9% of the drivers experienced neck pain on one side of the neck [10]. The conflicting results may be due to the habit of using mobile phones while driving and commonly watching a side mirror while driving, depending on the type of vehicle used.
A report by Ehliched George concluded that the commonly acquired postures while driving are the racer posture, the multitasker posture, the pmp posture, and the habitual forward posture [40]. This study revealed that 75.81% of drivers who experienced neck pain adopted a habitual forward posture, 8.6% adopted a multitask posture, 33.33% adopted a racer posture, and 28.9% held a pimp posture while driving. In support of these results, the findings of the Porter study parallel those of this study, which he conducted to assess the driving postures acquired by drivers while driving. He concluded that 37% of drivers adopted a habitual forward posture, 19% acquired a racer posture, 26% of drivers had a multitasker posture, and only 8% of drivers had a pmp posture during driving [10]. In contrast to these results, a study reported that only 3% of drivers at the university had acquired habitual forward posture, 3% had acquired racer posture, 15% had acquired multitasker posture, and 79% had acquired the posture of pimps. This is because of the differences in the ergonomic factors of driving, seat height and working environment and the time of day driving [10]. Poor posture is strongly associated with neck pain in professional drivers. Sitting in a static position with poor posture for extended periods of time can lead to neck and upper back discomfort and pain [41].
The current study revealed that 25 (6.8%) drivers had pain on the right side of the neck, while 104 (28.2%) drivers had bilateral neck pain. The findings of this study are consistent with those of Szeto and colleagues, who concluded that neck pain in urban transport drivers in Hong Kong was chiefly bilateral to the neck [25]. In contrast, another study concluded that only 9% of drivers experienced bilateral neck pain, and 9% of drivers experienced unilateral neck pain [10]. These conflicting results might be due to the habit of using mobile phones, which are commonly used to watch side mirrors while driving, and vehicle type.
This study revealed that 37.9% of bus drivers experienced neck pain. In support of this, the findings of the study of Magnusson et al. reported that heavy vehicle drivers have a high prevalence of neck pain [42]. Moreover, the findings of the current study revealed that the majority of drivers (75.81%) who experienced neck pain adopted a habitual forward posture. Findings parallel to this study were reported in a study by Kashif et al. [10].
Only professional male drivers located in Faisalabad were included in this study. In this study, only 5 groups of vehicles— cars, buses, trucks, urban transport and semitrailers— were assessed. Therefore, the results may not be applicable to the general driving population, such as female drivers, Rikshaw drivers and motorbike riders. The study findings may not apply to other populations since the study relies on self-reported data. Professional drivers who participated in the study might not be representative of all professional drivers. Furthermore, the study likely relies on self-reported data, which may be subject to recall and reporting biases. The findings of this study will be helpful for strategic policy makers, work-related medical health care clinicians and transport associations and organizations to design different schemes, programs and strategies for the rehabilitation and automotive industry to reduce biomechanical and ergonomic risks and to decrease the consequences, uneasiness, and perceived discomfort of incorrect driving posture by addressing the design of driving seats. This study will also be helpful for promoting the importance of ergonomic training for drivers to increase their awareness of the ergonomic risks of their workstations. Assessment of perceived vibration during driving should be performed in future studies.
Conclusion
The findings of the study revealed that drivers had a greater incidence of neck pain than did drivers with a greater prevalence of point pain. Moreover, professional drivers driving urban transport had the highest prevalence of WRNP, while those driving cars had the lowest prevalence. A significant association was found between driving and neck pain and age, BMI, lifestyle, health status, medical history, and smoking habits. Drivers with ergonomic training and awareness were significantly less likely to experience lower neck pain. Postural factors were found to be associated with neck pain in this study. A habitual forward posture was more likely to cause neck pain than a habitual posture. There was more neck pain among drivers with sitting and standing head, neck and trunk postures than among those with normal posture.
Ethical approval
The ethical approval for the current study was granted by Research & Ethics Committee of Riphah International University, Islamabad, Pakistan.
Informed consent
Written consent was taken from each participant before their data collection.
Conflict of interest
None to declare.