
Abstract
BACKGROUND:
Intensive care physiotherapists are exposed to situations that may cause physical and mental overload, which can lead to the onset of work-related musculoskeletal complaints.
OBJECTIVE:
The objective was to analyze these complaints and to identify activities causing greater overload, factors associated with complaints, and management and prevention strategies.
METHODS:
Cross-sectional study. Data were collected from 125 physiotherapists in the Intensive Care units (ICU) of a tertiary hospital. The questionnaire used was formulated from questionnaires validated in the literature such as Nordic Questionnaire and Bork Questionnaire. Chi-square test was performed to compare the groups with and without complaints. Logistic regression was used to assess the association effects of the variables on the presence of complaints.
RESULTS:
Of those interviewed, 76% had a work-related complaint in the last year, with the “lower back” being the most affected region. Eighty percent had complaints for more than one site. “Transfer” was considered the activity causing the greatest overload. Female sex (p = 0.023), lack of physical activity (p = 0.028), inadequate ventilation (p = 0.001) and inadequate furniture (p = 0.006) showed a statistically significant association effect with the presence of complaints. Inadequate ventilation (p = 0.003) and female sex (p = 0.004) influenced the number of affected areas. Physical activity was considered the main strategy for prevention.
CONCLUSION:
Musculoskeletal complaints accounted for a high percentage of the analyzed sample, mainly in the lower back. The extent of complaints suggests that strategies should be developed and changes in work dynamics should be carried out.
Keywords
Introduction
Repetitive strain injuries (RSIs) and work-related musculoskeletal disorders (WMSDs) are functional and mechanical disorders related to occupational activities that can affect various body structures [1]. They can cause problem symptoms such as pain, discomfort, fatigue, tingling and a drop in performance [1], resulting in absenteeism, task restriction, reduced clinical longevity and even transfer to another professional activity [2, 3]. RSI/WMSDs are the most common causes of complaints affecting workers today [2, 4], and are the result of repetitive movements, the use of high levels of force and the maintenance of incorrect positions for prolonged periods [1, 6].
Studies with health professionals have shown that physiotherapists have a high prevalence of RSIs/WKSDs [4–9], from the beginning of your professional career. The main areas affected are the lumbar and cervical spine, shoulders, hands and wrists [10]. Previous studies indicate a notable prevalence of WMSD among physiotherapists worldwide. Between 53% and 91% of physiotherapists experienced WMSD symptoms at some stage in their working lives [4, 10]. Specifically, data shows that 57.5% of physical therapists in the USA reported WMSD [11], while in Jordan, all physiotherapists interviewed had complaints in the neck [5], and in Vietnam, 76.4% of physiotherapists experienced WMSD [12].
The place of operation and its components can influence complaints. Specifically, in intensive care units (ICUs), physiotherapists have an important role in the treatment of critically ill patients [13, 14]. In this context, they are exposed to situations that may cause physical and mental overload, which can lead to the onset of RSIs/WMSDs as their bodies are their main working tool [5]. The main risk factors are repetitive maneuvers and movements [9, 15–17], static contractions [20], lifting and transferring weight [4, 18], and maintaining inappropriate postures [4, 19–21]. Additionally, limited space, physical barriers, a high number of consultations [22], and a lack of rest breaks can also contribute to the occurrence of complaints [18].
Research indicates that healthcare professionals working in the ICU commonly face musculoskeletal overloads [23], which can result in reduced service time, absenteeism, and professional leave. Among these professionals, nurses are the most studied group in the ICU environment, often experiencing complaints, particularly in the lumbar region due to the demands of caring for bedridden patients [22]. ICU nurses are exposed to various environmental and emotional stressors and perform tasks similar to those of physiotherapists, such as repositioning patients, transfers and assisting with standing, and walking. However, there is a lack of sufficient data addressing the role of physiotherapists in the ICU setting. As the several risk factors involved, it is imperative to conduct studies analyzing the occurrence of symptoms among ICU professionals, particularly physiotherapists. Such research would enhance understanding of the underlying causes and facilitate the development of awareness, management, and prevention strategies, thereby contributing relevant insights to the literature for this high-risk setting and profession.
The aim of this study was to analyze musculoskeletal complaints in ICU physiotherapists and to identify activities causing greater overload, factors associated with complaints, and management and prevention strategies.
Materials and methods
A cross-sectional study was carried out in the intensive care unit (ICU) of a public tertiary reference hospital in São Paulo (Brazil), which cares for highly complex patients. Data collections were conducted in both medical and surgical intensive care units. ICU physiotherapists are exposed to physically demanding tasks while caring for hospitalized patients. Among the primary occupational activities performed by physiotherapists in the ICU are aspiration (via orotracheal, tracheostomy, or nasotracheal cannula), secretion removal maneuvers, manual hyperinflation maneuvers (bag squeezing), limb mobilizations, changes from the decubitus position, scapular and pelvic dissociation in bed, as well as passive or active-assisted exercises, patient transfers, and aiding dependent or semi dependent patients in sitting and orthostatism. These tasks necessitate significant physical effort on the part of the physiotherapist.
Participants
This study was approved by the ethics committee of the local institution. For data confidentiality, we used the REDCap system for data entry and management. The inclusion criteria were physical therapists working in the ICU. The inclusion criteria included physical therapists working in the ICU, selected to represent a population dealing with specific procedures for highly complex patients. Exclusion criteria were chosen to minimize confounding factors, excluding pregnant women, who might report musculoskeletal complaints related to pregnancy, and physiotherapists with preexisting musculoskeletal complaints unrelated to work, as this study aimed to evaluate work-related complaints. Additionally, participants who did not complete the questionnaire were excluded to facilitate subsequent data analysis.
Assessments
Data collection was performed through a self-administered electronic questionnaire (Appendix 1). The questionnaire was distributed by email, and a study collaborator carried out an active search for professionals. The sample was a convenience sample. Each participant could answer the questionnaire only once. The study period was from July 2018 to January 2022.
Instrumentation
To formulate the questionnaire used in this study, questions were sourced from validated questionnaires in the literature, such as the Nordic Questionnaire and Bork Questionnaire, forming a specific assessment for this paper. [4, 26]. The questionnaire was divided into six sections, each tailored to specific assessments: (1) participant characterization; (2) work-related complaints and their locations; (3) risk factors; (4) work and environmental factors; (5) work and emotional factors; and (6) management and prevention strategies. The first section included questions for identification, demographic information, professional background, place of work, and performance. In the second section, questions from the Nordic Questionnaire of Musculoskeletal Symptoms [24, 25] were used to identify reports of work-related complaints, including their location on the body, frequency, severity, and influence on professional activities. The third section used a questionnaire developed by Bork et al. (1996) [4] to classify risk factors, rating the contribution of each factor/task to the occurrence of problematic symptoms (17 conditions using a scale of 0 to 10). The fourth section identified the environmental factors and the individual/work furniture relationship in the ICU. The fifth section related work in the ICU to emotional factors. Finally, the sixth section identified management and self-protection strategies to minimize the risk of RSIs/WMSDs disorders and suggestions for reducing burdens. All collected data were entered in an Excel spreadsheet.
Statistical analysis
A descriptive analysis of the collected data was performed, with a simple frequency distribution and the calculation of percentages for categorical data. The participants were separated into groups with and without complaints. The physiotherapists who responded “YES” to the question “In the last 12 months, have you filed any type of complaint that you believe is related to work?” were categorized into groups with complaints, while those who responded “NO” were categorized into groups without complaints.
For statistical analysis, isolated variables were selected by our study as possible risk factors associated with the occurrence of complaints among ICU physiotherapists. The selected variables related to individuals were sex, BMI, practice of physical activity and hours of sleep. Years of professional experience, weekly workload at the evaluated hospital, total weekly workload, shift, ergonomic training and knowledge of self-care protocols were the variables related to work in the ICU. The selected variables related to emotional factors were emotional involvement and stress in the ICU and those related to environmental factors, adequacy of ventilation, adequacy of illumination and adequacy of furniture.
For the comparison between the groups with and without complaints, the selected isolated variables were used, and the outcomes were analyzed using the chi-square test (X2). A chi-square (X2) test was also performed to analyze the comparison between the groups with and without complaints regarding the lower back and the other isolated variables. The lower back was selected because it was the region with the largest sample group in this study, allowing for more robust statistics. The alpha level was set at 0.05.
A linear logistic regression model was used to assess the association effects between the independent variables and the presence of a complaint variable. Additionally, linear logistic regression was performed for the variable indicating the presence of lower back complaints. The final model was constructed using the stepwise backward method, with a significance value of 0.10 considered for removing the variables at each step. Variables were considered to show a potential association if their p-value was less than 0.2.
To analyze the effect of independent variables on the number of regions with complaints, a backward-style multiple regression analysis was performed. Association variables were selected based on a significant level of p < 0.05 for inclusion and p > 0.10 for exclusion. The quality of the model was assessed by its predictive accuracy measured through R square.
Results
Sociodemographic and occupational information
A total of 129 physiotherapists participated in the study and completed the questionnaires. Four participants were excluded according to the criteria (3 who were pregnant and 1 who was not working in the ICU); therefore, 125 participants were included. All participants worked in the ICU of the tertiary hospital analyzed, performing similar functions. The participants’ sociodemographic and occupational information is presented in Table 1. We divided the demographic and labor characteristics in Table 1 into subgroups for better visualization and characterization of the population. We sought to specify and detail the characteristics based on data from the literature regarding specific populations that may have greater or lesser risk of musculoskeletal complaints. Therefore, we detail the percentages related to weight range, age and gender that can provide greater understanding of how our population presents itself in relation to these factors. As well as work characteristics such as working hours that can favor the emergence of work-related complaints. The largest concentration of physiotherapists are aged up to 35 years, demonstrating that many young people begin their work in intensive care.
Sociodemographic and occupational information of physical therapists who worked in the ICU and participated in the study
Sociodemographic and occupational information of physical therapists who worked in the ICU and participated in the study
A total of 125 participants composed the complete study sample. Data are presented as absolute numbers (%); >bigger; <minor; ≤ less than or equal to.
In the analysis of the frequency of musculoskeletal complaints, 76% (n = 95) of the professionals stated that they had had some work-related musculoskeletal complaint in the last year. Problem symptoms had manifestations in different regions, as illustrated in Fig. 1. Problem symptoms in the lower back were the most common among physiotherapists (67.4%). The sum of the percentages exceeded 100%, as each physiotherapist could mark more than one option. Regarding the number of regions affected, 32.6% of the participants had complaints regarding 2 body segments, followed by 21.1% with complaints regarding 3 segments, 20% with complaints regarding 1 segment, 16.8% with complaints regarding 4 segments and 9.5% with complaints regarding 5 or more segments. The presence of more complaints per individual can be classified as a worse physical condition compared to the presence of fewer places of complaints.

Regions of work-related musculoskeletal complaints according to respondents. A total of 95 participants (76%) had work-related complaints.
In the specific responses to the Nordic Questionnaire, it was possible to analyze the frequency, intensity, manifestation and consequences of musculoskeletal complaints. These data are shown in Figs. 2–4. We presented the details of the Nordic Questionnaire data based on the study by Vachinska et al. [27].
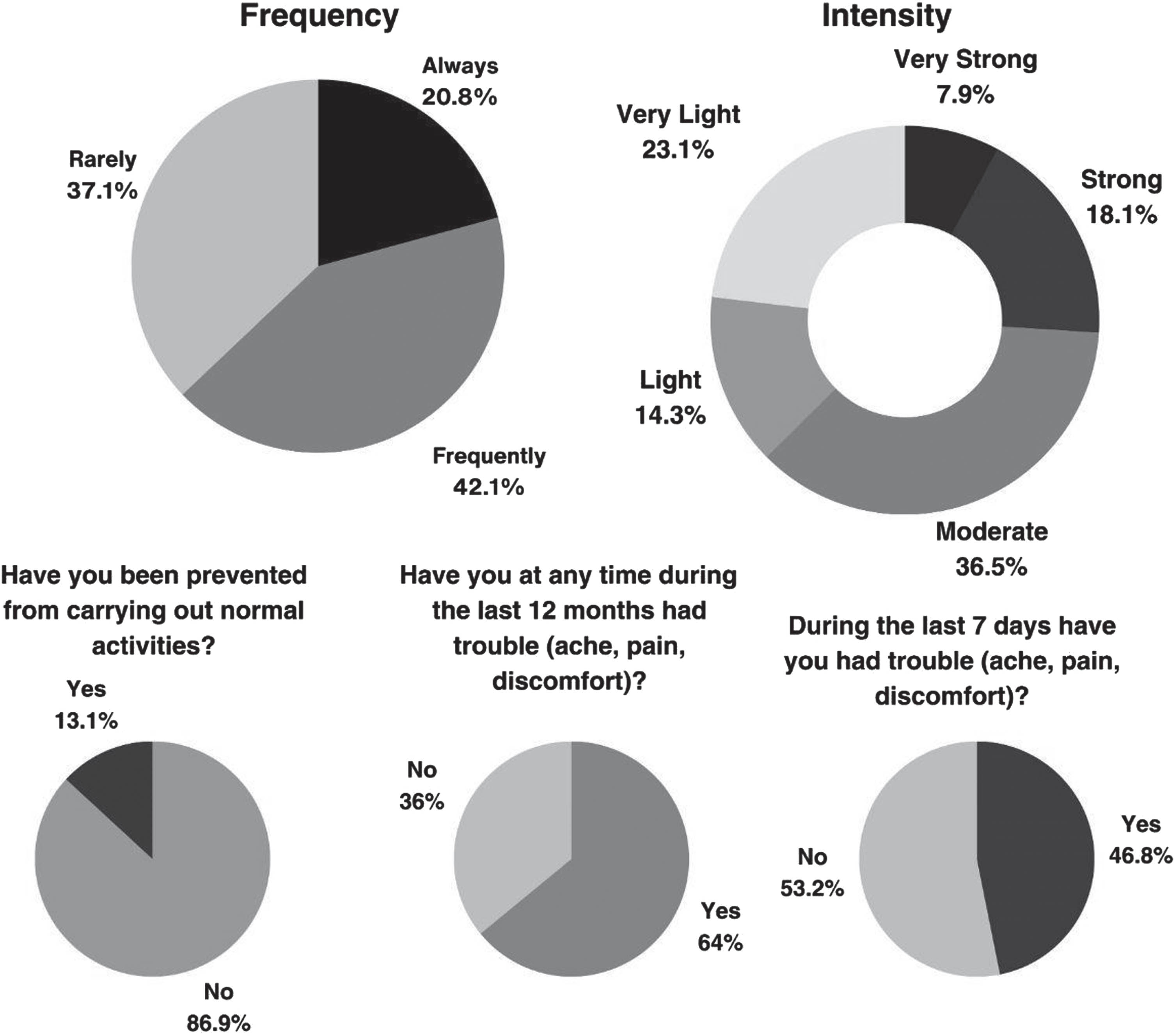
Classification of musculoskeletal complaints according to the Nordic Questionnaire regarding the region, frequency, classification, manifestation and barriers to carrying out activities due to discomfort. A total of 95 participants had work-related complaints.

Classification of musculoskeletal complaints according to the Nordic Questionnaire regarding the region, frequency, manifestation and barriers to carrying out activities due to discomfort. A total of 95 participants had work-related complaints.

Classification of musculoskeletal complaints according to the Nordic Questionnaire regarding the intensity. A total of 95 participants had work-related complaints.
In a more specific analysis of the presence of the complaint during a given occupational task, 45.3% of the 95 participants experienced the problem symptom for the first time when transferring a patient from lying down to sitting and vice versa. A total of 41.1% of the subjects reported experiencing the symptom when transferring a patient from sitting to standing or vice versa. According to 71.6% (n = 68) of the physiotherapists, the problem symptom was exacerbated with clinical practice. Of the physiotherapists with complaints, 62.1% (n = 59) did not seek medical attention and 72.3% had no diagnosis. When analyzing the behavior of these pain complaints, 76.8% had a gradual onset, and 48.4% did not undergo any treatment. Regarding the moment of onset of the problem symptom, 51.6% experienced the problem symptom for the first time carrying out work activities in the first 5 years after graduation, while 22.1% had already experienced the symptom before graduation (in practical learning activities).
Due to the complaint, 38.9% of the participants changed their work habits, 35.8% changed the treatment applied, and 26.3% limited the time providing care (increased administrative time). None of the physiotherapists changed areas/specialties, but 26.3% considered changing areas and 10.5% considered changing professions.
In the analysis of activities causing greater overload, 51.2% of the total population considered transfers as the task with the greatest musculoskeletal overload, followed by changes from the decubitus position, mobilizations and orthostatism. Transfers are tasks that require excessive use of strength and weight bearing associated with tilting and rotation movements of the trunk, performed repeatedly during the work shift in the ICU.
For descriptive analysis, conditions and tasks that could contribute to the development of these complaints were classified through the questionnaire developed by Bork [4]. The questionnaire had 17 conditions and tasks, and the tasks were classified using a scale ranging from 0 to 10 (from 0 to 1: “no problem”, 2 to 7: “minimum to moderate problem” and 8 to 10: “big problem ”). Table 2 shows the activities and their degree of risk, classified by the physiotherapists. The greater demands for strength and weight bearing in inadequate postures, the excessive repetition of these tasks and exhausting shifts present the highest risk classifications according to the sample analyzed.
Percentage of responses indicating the classification of activities as risk factors for the development of work-related musculoskeletal complaints
Percentage of responses indicating the classification of activities as risk factors for the development of work-related musculoskeletal complaints
A total of 125 participants composed the complete study sample.
Another objective of the study was to analyze factors associated with pain complaints. As factors associated with pain can be multifactorial, we analyzed environmental and emotional factors. Regarding environmental factors, 12.8% of the physiotherapists considered the lighting in the ICU to be inadequate, 51.2% considered the ventilation in the ICU to be inadequate, and 20.8% did not think the furniture in the ICU was adequate (beds, workspace, tables, computer positioning, etc). Regarding emotional factors, 36.8% (n = 46) of the participants reported that working in the ICU affected their life outside the hospital. Emotional involvement with work and ICU patients was classified as moderate by 38.4% (n = 48) of the participants. Stress in the ICU was classified as moderate by 31.2% (n = 39) of the participants and as severe by 27.2% (n = 34). Overall, 45.6% of the participants reported being sleep deprived, and 33.6% reported sleeping less than 6 hours per night.
For a more specific analysis of the association of factors with complaints, a comparative analysis was performed using a chi-square test, and an analysis of the effect of independent variables on the presence of complaints was performed using logistic regression. We chose to perform three separate analyses for better characterization: pain complaints, lower back complaints and the number of affected sites.
A chi-square test was performed to compare groups with and without complaints. The results indicated statistically significant differences between groups for female sex (p = 0.019), inadequate ventilation (p = 0.004), and emotional involvement (p = 0.027). Additionally, a simple regression analysis was performed to identify variables with the potential to be included in the final logistic regression. Variables were removed at each step if their significance value exceeded 0.10, while those with a significant level of p < 0.05 were included and p > 0.10 were excluded. The final logistic regression model, which included variables such as female sex (OR = 3.988), lack of physical activity (OR = 3.221), inadequate ventilation (OR = 6.670) and inadequate furniture (OR = 8.010) showed a statistically significant association effect for the presence of complaints (Table 3). These findings indicated that the selected variables can predict a cause-and-effect relationship for the occurrence of work-related musculoskeletal complaints, thereby increasing the risk of WMSD occurrence.
Final logistic regression model for the presence of general complaints and for the presence of complaints regarding the lower back and final multiple regression model for the number of affected areas
Final logistic regression model for the presence of general complaints and for the presence of complaints regarding the lower back and final multiple regression model for the number of affected areas
OR = odds ratio CI = confidence interval.
Through a chi-square test, the specific analysis of the most affected site (the lower back) showed that the number of years of professional activity (p = 0.018), the weekly workload (p = 0.001) and inadequate ventilation (p < 0.001) were different between the groups. A simple regression analysis was also performed to indicate variables with the potential to be included in the final logistic regression. For each step, a significance value of 0.10 was used as the threshold for removing variables, while variables meeting the criteria of p < 0.05 were included and those with p > 0.10 were excluded. The final logistic regression model, which included variables such as weekly workload (OR = 3.265 for 30–40 h and OR = 4.138 for >40 h) and inadequate ventilation (OR = 3.052), showed a statistically significant association effect (Table 3). These results indicate that the selected variables can predict a cause-and-effect relationship for the occurrence of lower back complaints, thereby increasing the risk of lower back WMSD occurrence.
In the final multiple regression model, the standardized coefficients showed that inadequate ventilation, followed by female sex, were the variables that most influenced the number of affected areas.
We also sought to analyze management and prevention strategies for work-related musculoskeletal complaints inside and outside occupational activities. Regarding nonoccupational strategies to emotionally disconnect from their work in the ICU, 48.8% of the physiotherapists used leisure activities, followed by “family and friends” (26.4%). Of the total sample, 45.6% believed that physical activity was the main strategy for preventing work-related complaints. However, only 38.4% of all respondents reported performing some type of physical activity frequently.
We also analyzed strategies for managing complaints at the time of occupational activities. In Table 4, we describe the strategies adopted by the physiotherapists interviewed and their frequency.
Frequency of different types of strategies adopted by physiotherapists for managing and preventing musculoskeletal complaints in relation to their occupational activities
Frequency of different types of strategies adopted by physiotherapists for managing and preventing musculoskeletal complaints in relation to their occupational activities
A total of 125 participants composed the complete study sample.
Our study aimed to analyze musculoskeletal complaints in ICU physiotherapists, identify factors associated with these complaints and identify strategies for management and prevention. The sample analyzed was primarily composed of young individuals. Our main findings showed a high prevalence of complaints among these physiotherapists, with the lower back region being the most commonly affected. Additionally, a significant percentage of individuals reported complaints in more than one site (80%). These complaints often occurred frequently and were characterized by moderate to strong intensity in most individuals. In our study, several factors were associated with general complaints, including female sex, lack of physical activity, inadequate ventilation, and inadequate furniture. Specifically, complaints related to the lower back were associated with a weekly workload exceeding 30 hours and inadequate ventilation. Additionally, factors influencing the number of complaints included female sex and inadequate ventilation.
The most common site and the site with the highest frequency of complaints identified by ICU physiotherapists was the “lower back” [4, 19]. Specifically, regarding performance within the ICU, the current scenario is of great importance for the early rehabilitation of these patients, in addition to improving the survival of patients with greater deficits. This results in increasing and intensifying care for more dependent patients, in addition to a greater number of consultations and, consequently, greater exposure to risks. Thus, work activities, such as “transferences” (classified as a task with greater overload in our study), are performed more by physiotherapists and require greater use of strength and bearing weight in unfavorable positions. In addition, physical barriers connected to patients (probes, accesses and devices) can make it even more difficult to manipulate patients in and out of bed (Fig. 5). This whole performance scenario can justify our expressive findings of complaints in these professionals.

1. Orthostatism of patients, 2. Physical barriers connected to ICU patients, 3. Preparation of physiotherapists to perform patient transfers. Researchers’ collection.
The association of some intrinsic and extrinsic factors with the work activities of ICU physiotherapists had effects on the predisposition of work-related complaints. Female sex was associated with the presence of complaints in our study, and reinforcing these data, previous studies have shown that women interpret stimuli differently from men and have lower pain thresholds [28–31]. Hormonal changes related to the menstrual cycle and women’s age are described as factors that can significantly influence pain perception [29–31]. Not practicing physical activity was also associated with an increased number of complaints in our study. Aerobic and strengthening physical activities have numerous systemic benefits in the short and long term, reducing the risks of developing or progressing musculoskeletal changes [32]. Despite the knowledge about the importance of physical activity and its benefits in the prevention and progression of musculoskeletal complaints [32], notably, most physiotherapists participating in the study did not practice physical exercise, most likely due to their demanding physical and emotional routines and their long working hours.
The workload was also directly associated with complaints. A longer work history involves a greater number of consultations and frequency of activities that involve more efforts. Work activities such as “Transfers”, which were classified as a task with greater overload, end up being carried out more, requiring greater use of strength and weight bearing in unfavorable positions. In addition, as we analyzed professionals within an environment with greater intellectual and attentional demands, external stressors could also become factors associated with the development or exacerbation of complaints. An environment with inadequate ventilation can act as a stressor in the workplace, contributing negatively during work.
The management and prevention strategies mentioned by the population of this study were also reported in previous studies [10]. Within the context of the ICU, three strategies draw attention in a negative way: the selection of techniques that will not aggravate the injury, stopping treatment if it causes or worsens discomfort, and reducing service time. This is because these strategies involve the selection of interventions within a patient’s therapeutic plan, causing the complaints to impact the therapy offered to the patient. On the other hand, some positive strategies used by a considerable number of individuals, such as teamwork, asking for help with a heavy patient, using proper body mechanics and adjusting the height of the bed, should be optimized and recommended to all professionals.
As the literature has shown, the high incidence of WMSDs in various medical areas, including among physiotherapists, reinforces the importance of gaining a better understanding of the risk factors contributing to these complaints, as well as developing strategies for their prevention and management. Our data aids in understanding the prevalence of WMSDs among a population of ICU physiotherapists and the associated risk factors related to their work activities, thereby facilitating the construction of therapy and self-care strategies. The results of this study add knowledge to the literature and promote updates in the work environment of ICUs. The acquisition of devices and technologies aimed at reducing physiotherapists’ workload and physical strain on their bodies is one example. Additionally, encouraging ergonomic training and the development of protocols for the physical and emotional care of physiotherapists can be beneficial.
This was a single-center study, despite being a hospital with a high demand for these professionals. A part of our data collection was carried out during the COVID-19 pandemic, and although it was a time of greater demand, a specific analysis of the data did not show any difference during the period. The work of physiotherapists in ICUs is in great demand at all times. A limitation of our study was its cross-sectional design, which precluded the evaluation of temporal variability in complaints. Another limitation was the assessment of complaint intensity by subgroups rather than through a numerical scale, which would have provided a more precise quantification of the complaints evaluated.
Physiotherapy professionals in ICUs present with a high percentage of musculoskeletal complaints, mainly in the lower back region, with a significant percentage having complaints regarding more than two parts of the body. The main related factors that can be modified are the adequacy of ventilation, the practice of physical activity, the adequacy of furniture and the weekly workload. Some interesting management strategies were reported by some professionals and can be extended to all. Other strategies may be harmful and should be reviewed in clinical practice. Therefore, the extent of complaints related to the work of ICU physiotherapists suggests that strategies and changes in work dynamics should be carried out to raise awareness and protect these professionals.
Ethical approval
The study was approved by the Faculdade de Medicina da Universidade de São Paulo (CAAE: 81215617.1.0000.0068; Number: 2.545.535).
Informed consent
All participants provided written informed consent prior to participation.
Conflict of interest
The authors have not potential conflicts of interest to disclose.
Footnotes
Acknowledgments
The authors thank the Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) and Faculdade de Medicina da Universidade de São Paulo (FMUSP).
Funding
Financing for the publication fee was provided by the Faculty of Medicine of the University of São Paulo.