
Abstract
BACKGROUND:
Strengthening safety compliance behaviour can reduce the organizations’ unexpected financial losses and prevent employees from continuous COVID-19. It drives this study to create a research framework involved by organizational, individual and social factors to predict employees’ safety compliance behaviour.
OBJECTIVE:
This study examines how risk perceptions of COVID-19, employee well-being, workplace health and safety training, safety motivation and safety related stigma impact safety compliance behavior in times COVID-19 pandemic.
METHODS:
A self-administered questionnaire was disseminated to healthcare workers. In all, 344 acceptable questionnaires were derived for further analysis.
RESULTS:
The results revealed that the risk perception of COVID-19 and employee well-being has no significant relationship with safety compliance behavior. Similarly, safety related stigma also has no moderating effect on safety motivation and safety compliance behavior. However, workplace health and safety training and safety motivation have significant relationships with safety compliance behavior.
CONCLUSION:
This study contributes to the literature by illuminating on the importance of organizational, individual, social factors and how they can interact with safety compliance behaviour. Additionally, knowing the unique function of safety related stigma in building safety compliance behaviour may help guide future efforts and training initiatives to enhance workplace safety.
Keywords
Introduction
Researchers have given a lot of attention to safety compliance behaviour because it is a top priority for business performance [1]. Specifically, COVID-19 virus causes employees to live in danger of exposure because it spreads between employees very quickly, increasing the probability that employees with whom they encounter may get infected. Strengthening safety compliance behaviour can reduce the organizations’ unexpected financial losses and prevent employees from continuous COVID-19 infection [2]. Hence, this study create a research framework involved by organizational, individual and social factors to predict employees’ safety compliance behaviour while address literature gaps as below:
Human perceptions of the COVID-19 risk have always been crucial factors in studying the safety compliance behaviour [3]. It should be necessary to find the risk perception level, protective behaviors and correct information to have a plan for COVID-19 controlling [4]. For this reason, it is unclear to what extent employees assess COVID-19 risk and how such assessment affects their safety compliance behavior [5]. At the same time, little is known about the concept of risk perceptions of COVID-19 and its usefulness to promote safety compliance behavior [5]. Employees perceive to have a high risk of COVID-19 during the first pandemic wave because vaccines were unavailable [6]. Such high risk perceptions of COVID-19 trigger employees’ anxiety and worry which could subsequently change employees to engage in safety compliance behavior [7].
Additionally, organizations prioritize employee well-being because it is critical to offer a happy and healthy workplace for the employees [8]. Most importantly, employee well-being determines organization achievement as the employees with higher levels of well-being are more likely to display safety compliance behaviour [9]. However, insufficient concentration has been focused on the understanding of employee well-being, considering scarce empirical evidence on the function of employee well-being in the safety literature [10, 11]. If so, which level of employee well-being will have a strong impact on safety compliance behaviour?
Further, workplace health and safety training is the main element in safety compliance behaviour as it helps workers to gain information, abilities, perform their task effectively and give them control over health and safety issues [12]. Nevertheless, past studies [13, 14] on the effectiveness of safety training to promote safety behaviour do not take COVID-19 pandemic into account, which constrains interpretation of how health and safety training support safety compliance behaviour. Simpeh [15] agreed that the government has introduced new policies, guidelines and rules, requiring safety training for re-opening business when COVID-19 pandemic is evolving every day. By doing this, returning workers feel secure and confident to practice hygiene work protocols i.e., safety compliance behavior.
Moreover, safety motivation is the strong predictor of safety compliance behaviour because employees with a high level of safety motivation tend to engage in the safety behaviors (e.g., safety compliance behavior) [16]. Available empirical evidence [17, 18] also suggests that a worker’s sense of desire for safety determines whether safety compliance behaviour will be improved. However, COVID-19 has unexpected and profound impacts on safety motivation of healthcare workers at all phases [17], requiring a re-assessment of safety motivation.
Besides that, employees are open to stigmatization and favoritism resulting from anxiety about the COVID-19 virus infection [19, 20]. Therefore, the research framework suggests safety related stigma (employee judgment of participating in workplace safety incidents may evoke unfavorable treatment and evaluation) as a boundary role that links between safety motivation and safety compliance behaviour. It is appropriate to examine the role of safety related stigma as it has seldom been investigated in safety literature. The reason is that stigma is widely tested in healthcare and medical literature [21, 22].
Inspired by all these gaps, this study examines how risk perceptions of COVID-19, employee well-being, workplace health and safety training, safety motivation and safety related stigma impact safety compliance behavior during COVID-19 pandemic. This study contributes to the literature review by illuminating on the importance of organizational, individual, social factors and how they can interact with safety compliance behaviour. Additionally, knowing the unique function of safety related stigma in building safety compliance behaviour may help guide future efforts and training initiatives to enhance workplace safety, enable organizations to support Sustainable Development Goals (SDGs) i.e., responsible consumption and production (goal 12).
Literature review
Risk perceptions of COVID-19 and safety compliance behavior
The risk perceptions of COVID-19 are highly associated with safety compliance behavior is understandable from Protection Motivation Theory (PMT) [23]. PMT suggests fear is an unhappiness that is derived from undesirable effects of threat on the individual and community [23]. Such fear encourages individuals and communities to engage in alleviating behaviors towards threats [24]. In the context of COVID-19 pandemic, the government has encouraged special precautionary measures, concentrating on good hygiene management, mask use, and social isolation [25]. By limiting the virus’s transmission, these suggestions were intended to lessen the effects of COVID-19 on individuals and communities [26]. Consequently, individuals and communities’ risk perception of COVID-19 have been well-observed as many of them took the advised steps such as hand washing and maintaining distance with infected people [3, 27]. Vitale [28] empirically proved that perceived seriousness and risk can lead to employees’ precautionary behaviors i.e., body temperature monitoring and extraordinary sanitisation, following the workplace safety measures to enhance the general health and wellness of people and organizations.
H1: Risk perceptions of Covid-19 positively influences employee safety compliance behaviour.
Employee well-being and safety compliance behavior
This study integrates Social Exchange Theory (SET) to explore employee well-being and safety compliance behavior. SET theory suggests a successful relationship can assist employees to recognize their organizations, comply with their obligations and responsibilities, and encourage them to respond in the positive behavior such as safety compliance behaviour [3, 29]. Specifically, employees that work in high-risk environments present a problem for management to ensure their well-being while providing safety and protection [30]. Thus, when management places a premium on establishing and executing safety management strategies (e.g., communication, training and rules), it has a positive effect on employees’ safety responsibility as well as willingness to enhance safety compliance behaviour [30]. Mihalache [31] showed that lower levels of employees’ mental well-being have a detrimental effect on the organization outcome (e.g., safety compliance behavior). The greater chance of unemployment, accidents, work stress and unhealthy lifestyle practices result in lower levels of employees’ mental well-being which avoid concentration [32]. Under this situation, using a heavy machine can lead to severe injuries or accidents to the employees [32].
H2: Employee well-being positively influences employee safety compliance behaviour.
Workplace health and safety training and safety compliance behavior
Workplace health and safety training can determine safety compliance behavior [12]. In this regard, SET predicts workplace health and safety training will encourage employees to reciprocate via demonstrating higher enthusiasm and devoting more effort in their work. Workplace health and safety training improves employees’ extrinsic motivation to exchange the support they receive from their organizations [33]. In exchange, employees may take part in positive behavior, showing safety commitment and higher levels of safety compliance behavior [34]. Chang [35] reported that one of the important organizational parts to protect employees’ safety in COVID-19 pandemic is training such as requesting COVID-19 safety instructors to conduct in-person or online training. This is to alert employees about their COVID-19 rights and responsibilities regarding workplace safety and inform employees of the government’s directions and instructions on COVID-19 [35]. As such, employees can take precautionary measures to avoid COVID-19 infection such as mask wearing and hand washing i.e., safety compliance behavior. Additionally, to respond to the shortage of workers in the COVID-19 crisis, training programmes should involve the larger workforce to reduce the risk of infection such as discouraging handshakes and frequent handwashing to improve safety compliance behavior [36].
H3: Workplace health and safety training positively influences employee safety compliance behaviour.
Safety motivation and safety compliance behavior
Safety motivation and safety compliance behavior is underpinned by expectancy valence theory which suggests that if individuals think that doing safely would result in better consequences, they will be more inclined to act safely [16]. In fact, employees can be motivated to improve their safety behaviors if they perceive compliance will lead to positive outcomes (e.g., reduce accidents and injuries). Previous research [20, 37] has demonstrated that safety behaviour in a variety of work environments is significantly influenced by safety motivation. For example, Calik [37] found that serious games (a teaching strategy) can be used to encourage students’ safety motivation to avoid the spread of COVID-19 infection and develop safety compliance behavior. Serious games foster power, novelty, and challenge in students that increase their safety motivation and apply COVID-19 infection control in clinical situations [37]. Similarly, Kim [20] also proved that safety motivation is positively correlated with safety compliance behavior by having a safety climate which can impact safety knowledge, involvement and contributing to safety compliance behaviors.
H4: Safety motivation positively influences safety compliance behaviour.
Moderator role of safety related stigma
Safety related stigma can be referred to as the employee’s concerns about safety events that would evoke adverse treatment or evaluation from others in the organization [19]. For instance, when an employee has COVID-19 infection in the organization, the employee has concerns that he or she would be judged unfavorably by their peers, head of department, employer, or maybe being withdrawn from others in the organization. Prior studies [38, 39] have shown that safety-related stigma influences workers’ health and safety because it is related to mental illness such as stress, burnout, depression and loneliness. Worries about the virus contamination and its spread cause stigmatization, which increases stress and anxiety and safety compliance behavior [40]. Therefore, drawing upon expectancy valence theory, stigma will act as a moderator between safety motivation and safety compliance behaviour [19]. Based on expectancy valence theory, individuals would not work hard on activities that may cause negative rewards, thus reducing their motivation [41]. If safety related stigma is high, safety motivation may reduce which negatively influences safety compliance behaviour [20]. Having said that, when employees have stigmatization, they are not interested in following safety practices and contributing to safety issues in the organization owing to lower safety motivation triggered by safety related stigma. On the other hand, if safety related stigma is low, safety motivation may increase as the undesirable effect of stigma reduces [20]. Hence, employees with no stigmatization are preferred to following safety practices and engaging in safety behavior.
H5: Safety related stigma moderates safety motivation and safety compliance behaviour.
Methods
Study design
This is quantitative research because this method can generalize and attain detail about a specific group of samples to represent the population [42, 43]. Besides, this is a cross-sectional design as data was acquired at a single moment in time, whether it be days, weeks, or months [42, 44]. Also, this is a correlational study because it lists several factors that impact safety compliance behavior which provide better understanding on the connection nature between the factors.
Population, sample and data collection
The total population consists of 214626 healthcare workers in government or private healthcare settings [45]. The healthcare workers in this study referred to physicians, dentists, pharmaceutical officers, nurses, science officers, X-ray technicians, physiotherapists and medical laboratory technicians. A total of 355 government and private licensed hospitals were identified from the website of Malaysian Medical Association [46]. Human resource departments of these hospitals were contacted to get their permission for participation. Of these, only ten hospitals were allowed to participate. Subsequently, 880 questionnaires were disseminated in proportion to the number of healthcare workers in each hospital. Only healthcare workers who have been employed by the hospital for more than six months were the subject of this investigation. This is consistent with the studies of Nasurdin [47] who claimed that six months are relevant for a worker to get used to the work environment. One week was given to the respondents to complete the questionnaire. Human resources department or authorised managers collected the completed questionnaire. After a week, the researcher returned to the hospitals and clinics to obtain 365 completed questionnaires, yielding 41.48% response rate over data collection from early August 2021 until mid-December 2021. According to Fincham [48], such response rate was deemed adequate and satisfactory for questionnaires. 344 questionnaires were acceptable for data analysis after outliers were eliminated.
Instrument development
This study incorporates tested scales from other studies, which improves the validity and reliability of the results [49–51]. Safety compliance behavior is measured by a five-item scale adopted from Chi [12]. The items reflected employees’ behaviour in promoting their individual health and safety. The composite reliability was 0.93.
The adoption of four-items scale risk perception of COVID-19 from Chi [12] that reflect the concern of the general public about contracting the COVID-19 virus or passing it on to family members. The composite reliability was 0.72.
Employee well-being is reflected by a four-item scale concerned with employees physical, psychological well-being and health outcomes from stress and accidents [52]. The composite reliability was 0.78.
Workplace health and safety training is measured by a five-item scale that are concerned with the management practices such as training for newly hired employees, revealing safety issues during training sessions, encouraging employees to participate in training programmes and hazard evaluation training [12]. The composite reliability was 0.91.
Safety motivation is represented by three item-scale that assess the willingness of an individual to exert effort to enact safety behaviours, as well as the valence associated with those behaviours [53]. The composite reliability was 0.92.
Safety related stigma is measured by three item-scale that examine employee attitudes involved in a safety-related incident resulting in adverse treatment from supervisors and co-workers [19]. The composite reliability was 0.96.
These constructs were operationalized using a five likert scale with a value of 1 (strongly disagree) to 5 (strongly agree).
To guarantee questionnaire statements were straightforward and concise, we did a pilot test with 50 healthcare staff or authorities prior to conducting the actual study. These staff from the pilot survey were later not included in the main survey.
The relevant actions were taken in this investigation to lessen the possible danger of common method variances (CMV). First, respondents were urged to complete the questionnaire depending on their own perspectives and experiences after being informed in the cover letter that there is no one correct response to each question. Based on Mackenzie [54], a cover letter that stated there are no acceptable or incorrect responses and common to have diverse options for questionnaire statements, the tendency of CMV may be decreased. Second, CMV was unlikely noteworthy. This is because respondents were unable to cognitively identify the complicated relations created by the moderation effect of safety related stigma in the safety compliance behavior [55]. Such moderation is one of this study’s research focuses.
Participants
This study had 344 participants from healthcare staff or authorities of hospitals and clinics. Around 146 (42.4%) are nurses and 21 (6.4%) are laboratory workers. There are 184 (53.5%) respondents are female and 160 (46.5%) are male. Majority of the respondents are between 25 to 34 years old (47.7%) while the rest were over 55-year-old (1.2%). In terms of years of experience, 108 respondents (31.4%) were mostly lower than 5 years. Lastly, 263 (76.5%) are non-executive job positions whereas 81 (23.5%) are executive job positions.
Results
The study used the PLS-SEM, or partial least squares based structural equation modelling method to examine the data. Table 1 shows the data had a satisfactory measurement model.
Reliability and validity results
Reliability and validity results
Note: *=items dropped as the items below loading values 0.40; CR = composite reliability; AVE = average variance extracted.
The value of composite reliability in Table 1 was significantly higher than the cut-off value of 0.70 [56–58], indicating that the measurement model’s internal reliability was very excellent. The average variance extracted (AVE) lowest score, which was 0.55, was higher than the cut-off value of 0.50 [56]. Besides, Heterotrait-Monotrait (HTMT) ratio for every construct as displayed in Table 2 is lower than the threshold value of 0.90 [59]. As a result, the measurement model’s convergent and discriminant validity were approved.
Discriminant validity results
Discriminant validity results
Note: HTMT0.90 criteria.
PLS-SEM indicator for model fit implied standardized root mean square residuals (SRMR) = 0.074, showing sufficient and significant fit. According to Henseler [60], to be declared a good fit in the research model, SRMR must be lower than 0.08. Then, the coefficient of determination (R2), effect size (f2), and the predictive significance (Q2) were then presented to evaluate the structural model’s performance. Generally, the research model’s explaining power is strong as 49.2% of the variance in safety compliance behavior is explained by employee well-being, risk perception of Covid-19, safety motivation, safety related stigma and workplace health and safety training. In terms of Cohen’s [61] effect size (f2), the results revealed that employee well-being (0.006), risk perception of COVID-19 (0.007), safety motivation (0.054) have a small effect on safety compliance behavior while workplace health and safety training showed a substantial effect of 0.549. Finally, Q2 shows the value above zero (safety compliance behavior = 0.38), demonstrating the research model is predictively valid. Table 3 is the hypothesis testing result. The results can reinforce the significant influence of workplace health and safety training (H3) and safety motivation (H4) on safety compliance behavior. Whereas, the influence of risk perception of COVID-19 (H1) and employee well-being (H2) on safety compliance behavior are insignificant and cannot be supported. Table 4 results suggest that there is insignificant moderation influence of safety related stigma on safety motivation and safety compliance behavior (H5).
Results of hypothesis testing
Results of hypothesis testing
Note: *t value > 1.96 = significance < 0.05, EWB = employee well-being, RCP = Risk perception of Covid-19, WHST = workplace health and safety training, SM = safety motivation, SCB = safety compliance behavior.
Moderation result
Note: SM = safety motivation, SRS = safety related stigma, SCB = safety compliance behavior.
There was an insignificant relationship between risk perception of COVID-19 and safety compliance behavior, implying that the healthcare workers do not believe their work is highly dangerous, thus they are less inclined to act safely to prevent harm to their own personal safety. This is contrary to prior studies [3, 27] that proved a significant relationship between risk perception of COVID-19 and safety compliance behavior.
Besides, employee well-being has an insignificant relationship with safety compliance behavior despite prior studies [30, 31] demonstrating a significant relationship. This could be explained by the fact that the healthcare workers have stress and emotional exhaustion, undoubtedly not following expected work processes and wearing protective devices. Liu [62] points out employees who experience stress and emotional exhaustion have no energy to work thoughtfully and have a negative impact on safety compliance behavior.
Workplace health and safety training is associated with safety compliance behavior, representing healthcare workers are offered opportunities to gain safety behaviour, skills, and knowledge, leading them aware of the possible job hazards and risks, as well as the repercussions of disregarding the COVID-19 threats. This is quite beneficial in providing healthcare workers with vital information to carry out their duties without contracting an infection. It is in line with earlier studies [12, 33] that have emphasised the beneficial part that workplace health and safety training plays in forming safety compliance behavior.
Besides, safety motivation plays a role in influencing safety compliance behaviour. Specifically, healthcare staff or authorities are more likely to take the necessary steps to ensure workplace safety if they are motivated to follow the laws requiring them to do so and actively participate in safety-related activities. This result is consistent with prior studies [20, 53] that demonstrates the significant influence of safety motivation on safety compliance behavior.
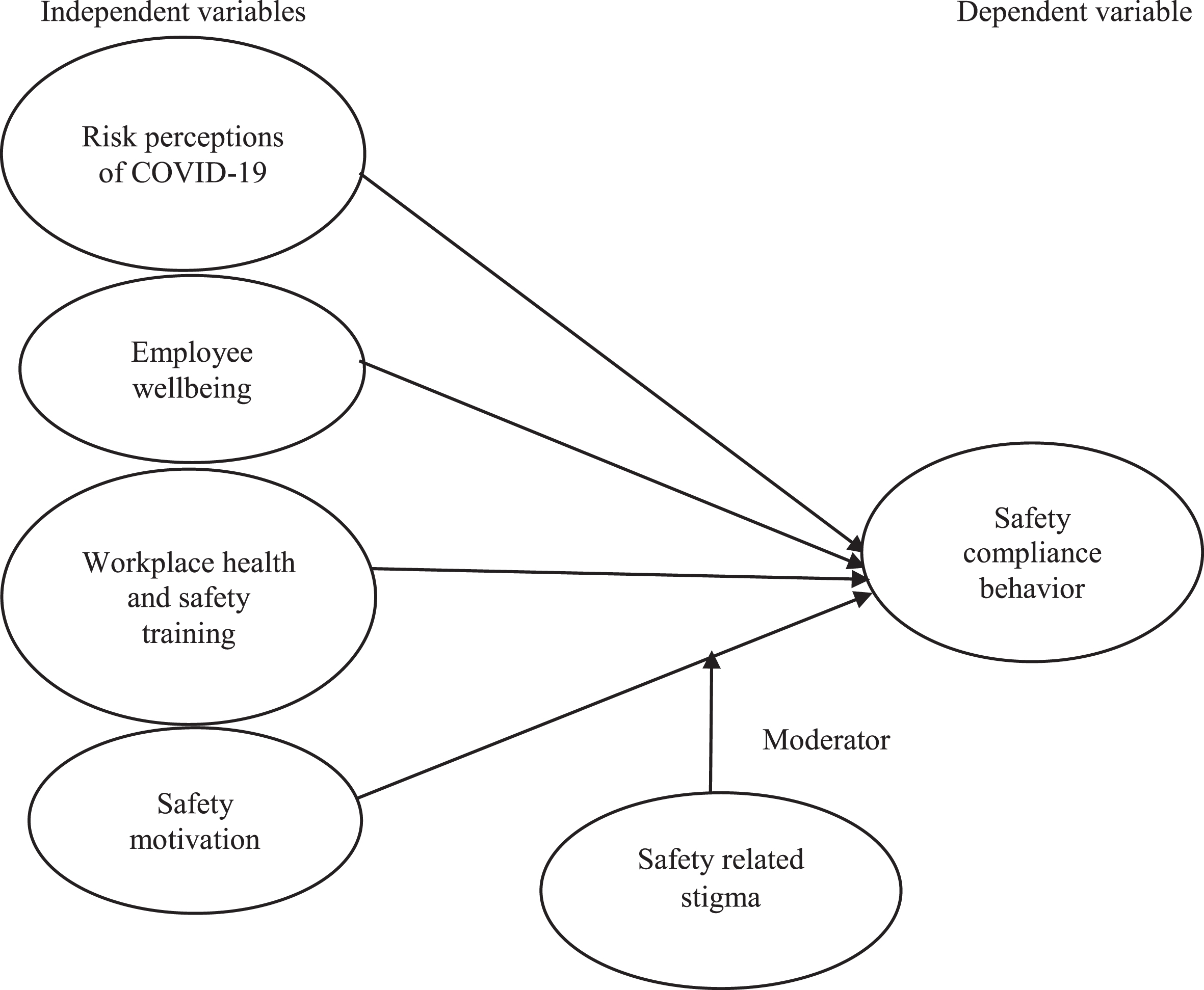
Research framework.
However, aligned with prior studies [19, 25] this study revealed that for Malaysian healthcare staff, the moderation effect of safety related stigma on safety motivation and safety compliance behavior was not statistically significant. The possible reason for this is cultural differences have different ways in viewing safety related stigma [20]. Malaysia has collectivist cultures [63] which consider safety related stigma a weakness and something to hide. This is harder for workers to share openly and ask for help, thus feeling stress and helplessness, resulting in no safety motivation and safety compliance behaviour.
Theoretical implications
This study makes significant contributions to the literature on healthcare. Once again, current study is an early effort to understand and assess the safety compliance behavior of healthcare professionals. To the greatest of our knowledge, there is limited literature on healthcare related to the COVID-19 pandemic that discusses a conceptual framework of safety compliance behavior. Additionally, there is no empirical data in the literature on healthcare that links the important elements that motivate healthcare workers to perform safely including attitude (safety motivation, risk perception of COVID-19), contextual (safety related stigma), individual (employee well-being), organizational (workplace health and safety training) factors.
This study also offers fresh perspectives on the influence of safety-related stigma on the connection between safety motivation and safety compliance behavior. This is due to the fact that the present amount of literature on safety-related stigma is very poorly understood. Unfortunately, contrary to expectancy valence theory, the findings show that safety related stigma does not necessarily function as a moderator to measure safety compliance behavior. Additional research is required to draw definitive findings on the relationship between safety-related stigma on safety motivation and safety compliance behavior.
This study enlarges the usefulness of expectancy valence theory. Despite that it has not yet fully embraced it, especially in the healthcare industry. This study forms the expectation on the basis of expectancy valence theory and found that this theory well describes employees who can be motivated to improve their safety compliance behaviors if they perceive compliance will lead to valued outcomes. Thus, the findings thus provide fresh evidence found in the job related literature [64, 65], workplace safety behaviour studies have opportunities for the theory’s use in the study of safety-related behaviour by healthcare researchers.
This study contributes to both workplace health and safety training and safety compliance behavior literature by using SET as a theoretical basis to add empirical evidence regarding the role of health and safety training in enhancing safety compliance behavior.
Practical implications
The research findings offer healthcare professionals substantial managerial implication in a timely manner. First, healthcare authorities who are eager to improve their safety compliance behavior should be aware of the functions of workplace health and safety training and safety motivation. Thus, healthcare authorities should make sure healthcare workers receive frequent safety training to ensure they are aware of safety concerns and how to handle protective equipment. As such, training programmes for healthcare workers would change their attitudes and perceptions about safety policies and practices, which would reduce risky behavior [66]. Moreover, healthcare authorities should set up mechanisms for motivating employees to improve safety behavior by rewarding them for following safety procedures, taking part in safety classes, and bringing up unique safety ideas.
Additionally, the findings urge healthcare authorities to not eliminate risk perception of COVID-19 and employee well-being to achieve safety compliance behavior. Instead, healthcare authorities should not prioritise risk perception of COVID-19 and employee well-being to achieve safety compliance behavior despite understanding their benefits. For example, it is unnecessary for healthcare authorities to impose mandatory physical activities intervention (e.g., walking, jogging, dancing, yoga) to reduce employees’ anxiety and thereby improving their well-being to achieve safety compliance behavior [67]. Further, healthcare authorities can optimize the work schedule of healthcare workers by avoiding strenuous shifts and fluctuating work hours. This is to ensure they have better sleep quality, mood and subsequently maintain their well-being to enhance safety compliance behavior [68].
The insignificant influence of safety-related stigma shows that safety-related stigma can be considered by the healthcare authorities as the replacement instead of addition for improving safety motivation and safety compliance behavior. To ensure that organisational practices and policies reflect the desire to promote safety motivation and safety compliance behavior while avoiding safety-related stigma, healthcare authorities must carefully assess the impact of those practices and regulations. For example, while healthcare authorities would wish to encourage healthcare workers about the value of safety behavior, they should refrain from taking too harsh actions against healthcare workers that might raise concerns about safety-related stigma.
Research limitations and future research suggestions
There are issues with the current study that require more analysis. The study is restricted to Malaysian context and safety compliance behavior may alter depending on the area. Future research should concentrate on different geographic regions to learn more about safety compliance behavior, broadening the generalizability of this study’s findings. Besides, this study concentrated on safety compliance behavior from the standpoint of employees rather than taking into account customers’ perspectives associated with the healthcare industry. Future studies are necessary to look at safety compliance behavior in a comprehensive view of the healthcare industry from the viewpoints of both customers and employees.
Ethical approval
Not applicable.
Informed consent
Informed consent was obtained from all participants.
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Funding
Not applicable.