
Abstract
BACKGROUND:
The impact of work-related tasks with potential biomechanical overload on the musculoskeletal system represents an essential socio-economical challenge.
OBJECTIVE:
This scoping review aimed to map the current literature to identify musculoskeletal disorders and diseases among healthcare professionals and define the approaches used to assess these problems.
METHODS:
The analysis was developed according to the JBI methodologies for scoping reviews and reported following the PRISMA-ScR framework.
RESULTS:
We conducted specific searches on online databases; of the 357 articles initially identified, only 118 met the inclusion criteria.
CONCLUSIONS:
Despite some discrepancies in their unambiguous identification, the presence of work-related musculoskeletal disorders in healthcare professionals is unequivocal. On the other hand, using technology as a supporting evaluation tool still needs to be explored. Furthermore, several improvements are required to enhance the quality of work and simplify the analysis across studies.
Introduction
Musculoskeletal disorders (MSD) are defined as dysfunctions or injuries that damage muscles, joints, bones, ligaments, nerves, tendons, spinal discs and cartilage [1]. These conditions determine pain at different joints and anatomical regions, including shoulder, neck, wrist, arm, knees, feet, hands, upper and lower back and hips [2]. Furthermore, several factors are associated with MSD, such as age, sex, BMI, smoking habits, lack of physical activity in free time, non-work-related exposures, and occupational risk factors [3]. Conversely, musculoskeletal impairments are represented by over 150 different diseases that affect bones, joints, muscles and connective tissues; consequently, affected subjects have temporary or lifelong limitations in functioning and participation [4]. Approximately 1.71 billion people worldwide suffer from issues at the musculoskeletal level [5].
Work-related musculoskeletal disorders (WR-MSD) have a multifactorial aetiology, in which work environment and working activities significantly contribute [6]; moreover, even some work-related psychosocial factors are also associated with WR-MSD, such as job satisfaction, work stress and low social support [7]. WR-MSD represents a social problem because of their profound impact on the quality of life of an individual [8]. They are also a burden from the socio-economic point of view due to their prevalence and because they are frequently associated with absence from working in both Europe and the United States [9]. Furthermore, as reported by the European Agency for Safety and Health at Work (EU-OSHA) [10, 11], MSD are the leading cause of disability concerning workers in all sectors and occupations.
Prevalence of WR-MSD manifests significant differences between occupations [11]. In particular, healthcare workers (HCW) represent one of the sectors most affected by MSD concerns; prolonged standing, highly repetitive work tasks, working in constrained or inappropriate postures, lack of time for recovery and psychosocial factors are the leading causes of dysfunctions in this occupational sector [12, 13]. A recent review of the literature [14] reported a prevalence of MSD of over 80% in physiotherapists, masseurs, nurses, midwives, dentists and surgeons.
According to the literature, the most affected sites for WR-MSD in HCW are, among others, thoracic outlet syndrome [9], shoulder, elbows and hands [15], neck and trunk [16] and lumbar spine [17]. A recent systematic review identified the lower back and neck as the most affected among HCW [18]. Literature also reported diseases linked with work in the healthcare environment. Carpal tunnel syndrome [19], epicondylitis [20], meniscal tears [21], and knee osteoarthritis [22] represented the most studied conditions in the literature [9].
This scoping review paper aimed to map the current literature to identify MSD and diseases in HCW and define all the possible approaches – including technologies - used to assess these problems.
Methods
This paper was developed according to the Joanna Briggs Institute (JBI) methodologies for scoping reviews [23, 24] and reported following the Preferred Reporting Items for Systematic Reviewers and Meta-Analysis extension for Scoping Reviews (PRISMA-ScR) framework [25].
Firstly, the protocol was developed following the literature [26] and registered on Open Science Framework (available at https://doi.org/10.17605/OSF.IO/UMCSN). The protocol has developed thanks to the collaboration of experts in the field, including one physiotherapist, one bioengineer, two occupational medicine specialists, and five resident doctors; the first four subjects are experienced professionals with over 15 years of active work [27].
Following the general indications, this overall analysis was organized into five different steps: 1. identify the review question; 2. define inclusion criteria and search strategy; 3. perform evidence screening and selection; 4. realise data extraction and data analysis; 5. synthesis section; 6. presentation ofresults [24].
Review question
This work aimed to answer these review questions: “What are the musculoskeletal diseases and disorders present among HCW? And how are these conditions evaluated?”.
Inclusion/exclusion criteria and search strategy
The search was performed in three online databases: Web of Science, Scopus and PubMed. The search strategy included all the discussed and identified keywords and Index terms (see Appendix 1 of Supplementary material). The following inclusion and exclusion criteria were then considered:
Inclusion criteria:
papers focused on HCW; papers published from January 01, 2000, to December 31, 2022; papers written in the English language; papers that include a questionnaire, clinical/physical evaluation, diagnostic imaging or quantitative assessment through dedicated technologies/devices/systems (e.g., cameras, wearable sensors, etc.); experimental or observational studies. Exclusion criteria: veterinary and para-veterinary professions; reviews; book chapters; conference papers.
Evidence screening and selection
Potentially relevant sources were then retrieved in total, and their citation details were managed using the Rayyan web application for systematic review, which was also used to detect and remove duplicates [28]. Titles and abstracts were screened by six reviewers (R.G, A.I.F, D.C., M.M., M.V. P.E.) to assess the inclusion criteria. Disagreements or conflicts among reviewers were solved by discussion. The full text of all the included papers were acquired and then analysed.
Data extraction and analysis
Data were extracted from the included papers by six reviewers (R.G, A.I.F, D.C., M.M., M.V. P.E.), who used the tool described in the protocol, composed by: 1. authors, year of publication, title and name of the journal; 2. Origin/country of origin (where the study was published or conducted); 3. aim/purpose; 4. study population and sample size; 5. demographic characteristics (e.g., gender, age, work position, working experience); 6. methodology: a. study type and design; b. data collection procedure (e.g., questionnaire, physical/clinical examination, imaging, quantitative assessment through dedicate technologies); c. data analysis; 6. conclusions.
According to JBI methodologies for scoping reviews [23, 24], the Risk of Bias in all the included studies was not performed.
Synthesis section
Data synthesis was organised by reviewers in three main cathegories of information. The first included: gender, BMI, comorbilities and smoking habits of subjects included in studies. The second was focused on type of healthcare professionals and their workload. The third was addressed on assessment methodologies used in included studies.
Presentation of results
The results of the search and the study inclusion process were reported in full in the final inclusion of this scoping review and then presented in the PRISMA-ScR flow diagram [25]. Data were then analysed, and percentage values (number of specific cases concerning the overall number of cases) were obtained.
A narrative summary was then realised to describe the results of this review objective and research questions.
Results
General results
The search was achieved in January 2023 in three online databases: PubMed, Scopus, and Web of Science and, 357 results were identified. Following the previously reported process, 65 papers were then identified as duplicates, so 295 papers were initially scrutinised by title and abstract analysis. This process excluded 112 papers. Subsequently, a total of 187 papers were then scrutinised by full-text analysis. In 52 papers, the full text was not available via the University subscriptions, four papers had a different focus, and six papers did not match the eligibility criteria. Finally, 118 papers were included in this scoping review.
In Fig. 1, we report the PRISMA-ScR flowchart. In Appendix 3 and Appendix 4 of the Supplementary Material, all details about the included and excluded papers are available.
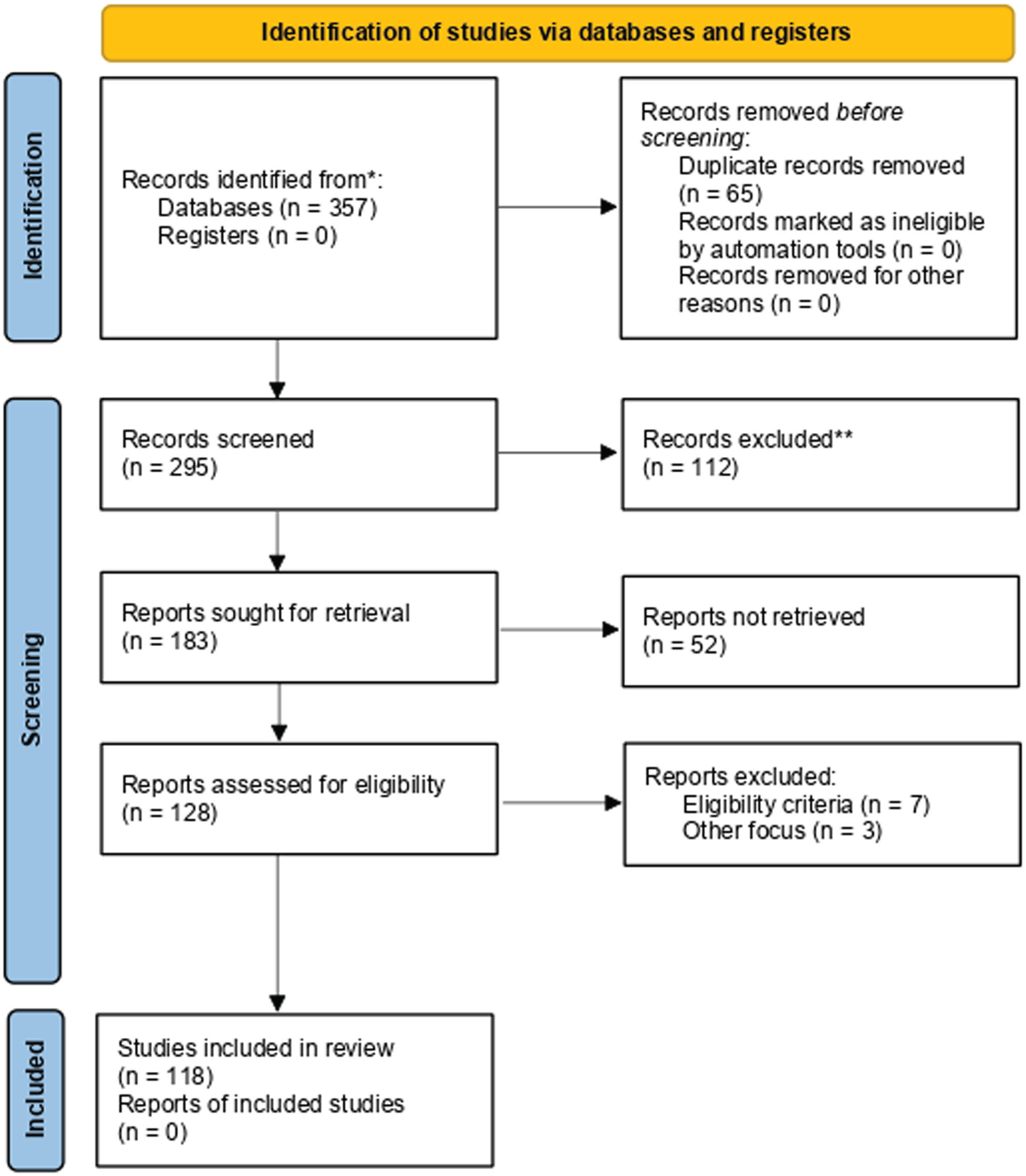
PRISMA flowchart. In this image, the paper selection is described following the PRISMA guidelines. Rayyan’s online application has been used to support this process.
Considering the temporal evolution of the published studies, most of the articles (75%, n = 89) were published after 2017, 26% (n = 31) between 2010 and 2016, and 4% (n = 5) were published before 2010.
Studies were mainly conducted in Europe 33% (n = 39) and Asia 38% (n = 45), followed by North America 19% (n = 23), with a lower proportion elsewhere: 3% (n = 4) in South or Central America, 2% (n = 3) in Africa, 1% (n = 1) in Australia. A small percentage (5%, n = 6) were multicentric (Fig. 2).
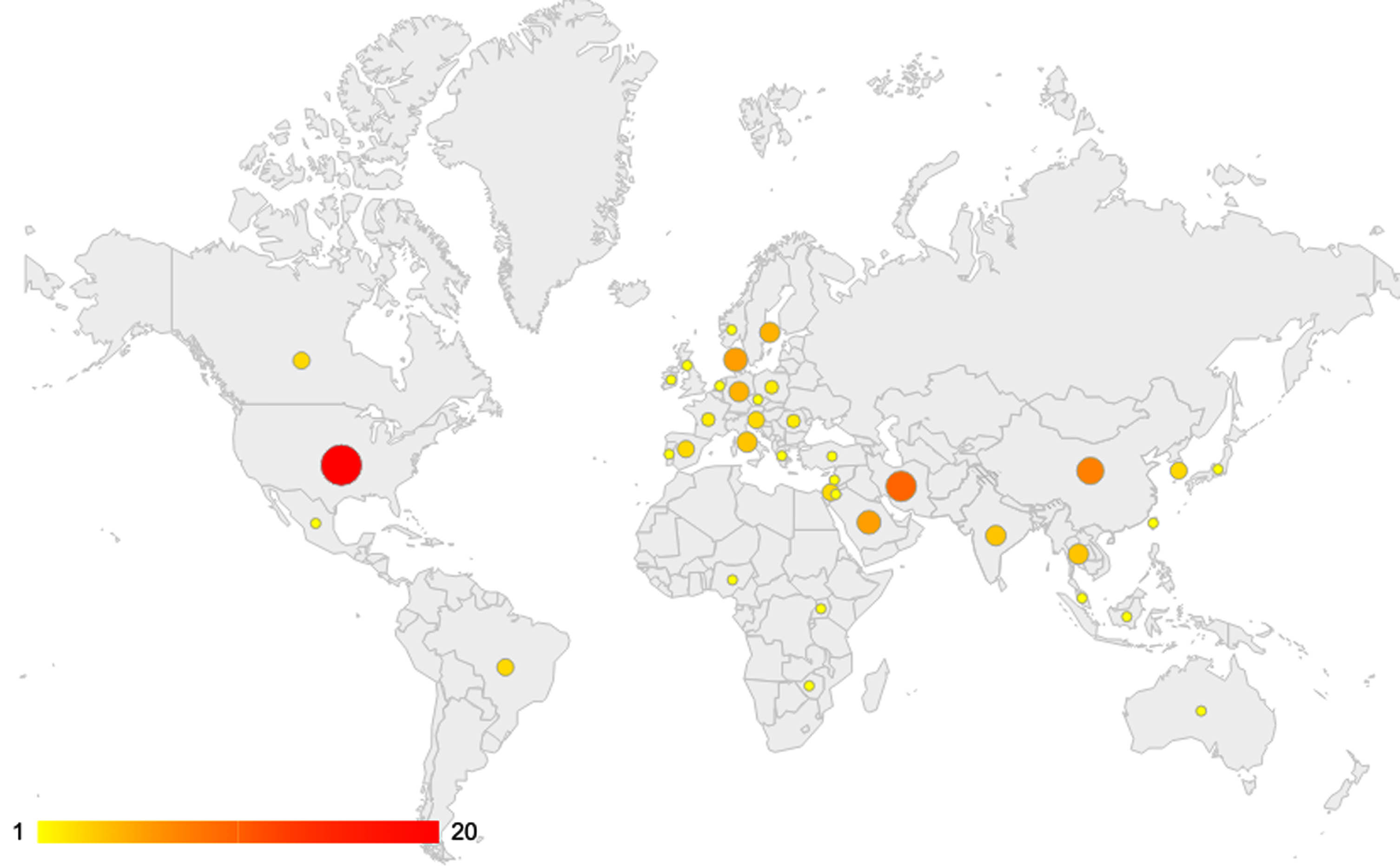
Geographical distribution of Studies.
Regarding the study design, the majority of studies (93%, n = 110) were Not-Randomized Controlled Trials (NRCT); 6% (n = 7) were Randomized Controlled Trials (RCT). Only one study was an RCT protocol.
Number and gender of participants
Concerning the included population, 32% included less than 50 subjects, 12% included 50 to 99 subjects, 38% included 100 to 499 subjects, and 17% included over 500 subjects. In 3% of cases, they were not declared this variable.
Considering the gender of people included, 52% (n = 61) of studies were primarily directed to females (10 included only women; 51 had a substantial prevalence in female subjects), and 28% (n = 33) mainly included males (4 only males; 29 had a considerable prevalence in male subjects). Two studies involved the same number of males and females. Finally, 25 studies did not declare the gender of the investigated population.
Concerning the age of people involved, 28% of studies had a mean age between 40–49 years, 23% between 30–39 years, 10% of studies less than 30 years, and 3% of studies more than 50 years. 20% did not declare the mean age, and 18% expressed this value in classes instead of the mean age.
Body Mass Index, comorbilities and smoking habits of included subjects
Body Mass Index (BMI) value was evaluated in 52% (n = 62) of studies; in 18% (n = 21) of them the population had a mean BMI of 18.5–24.9 (healthy weight), 12% (n = 14) had a mean BMI of 24.9–29.9 (overweight), 1% (n = 1) had a mean BMI of 30–34.9 (obese class I), 1% (n = 1) had a mean BMI of 35–39.9 (obese class II). 21% (n = 25) of studies expressed the BMI by dividing the sample size into different classes.
Comorbidities were evaluated only in 3 studies. Other studies reported generic information about this critical part. From these three papers, Iqbal and colleagues reported that 5% of the population included was affected by hypertension, diabetes or cardiac problems [29]; Alnefaie and colleagues reported that 16.5% of the included population was affected by chronic disease [30]; Jradi and colleagues reported that 10.2% of the included population was affected and 89.8% was unaffected by comorbidities [31].
Smoking habit was evaluated in 25% of studies (n = 30). In 11% of studies (n = 13), there were less than 25% of smokers. In 12% of studies (n = 14), more than 25% of smokers were reported. About 3% of the studies (n = 3) divided the population into classes. Moreover, 15% of studies (n = 18) considered physical activity and training.
Type of healthcare professionals included and their workload
Focusing on the type of professionals, among all the studies, 40% (n = 47) investigated nurses; 25% (n = 30) involved surgeons; 11% (n = 13) included dental workers and, in 12% (n = 14) physiotherapists were taken into attention. Finally, 22% of studies [n = 26] investigated other or multiple professions.
Referring to work experience, 13% of included studies (n = 15) involved professionals with 10–15 years of experience, in 11% of cases (n = 13), professionals had more than 15 years, and in 10% of cases (n = 12), professionals had less than ten years of working experience. 46% of included studies (n = 54) did not declare this value, and 23% (n = 27) expressed this value in classes.
Concerning workload, in 9% of studies (n = 11), workers declared to be working less than 40 hours per week, while in the other 7% of studies (n = 8), they claimed to be working at least 40 hours per week. In 10% of studies (n = 12), the working time was expressed in classes. We underline that most studies (76%, n = 90) did not value this parameter.
Assessment methodologies employed in included studies
Addressing the need for assessment methodologies, 85% of studies (n = 100) used questionnaires to evaluate MSD. Among them, 42 used validated questionnaires, 31 not-validated questionnaires, and 11 modified questionnaires. Moreover, 16 studies were conducted integrating validated questionnaires and an additional questionnaire that was not validated or altered. Analysing the most used validated questionnaires; we can affirm that Nordic was used in 30 cases in the original version and in 12 in the modified one; Borg was used in 11 cases in the original version; Nasa Task Load Index (TLX) was used in 5 studies in the original version and 4 the modified version.
In the analysis of technologies, in 22% of studies (n = 26), specific technology was included: cameras in 7 studies; surface electromyography in 4 studies, and inertial measurement units in 4 studies.
The degree of exposure to biomechanical overload during work activity was evaluated in 13 studies. 3 studies used the QEC scale, the REBA scale was used in 4 studies, and the RULA method was used in 5 studies. Additionally, in 1 paper, the REBA scale and the RULA method have been used together.
Finally, we highlight that about 8% of the studies (n = 9) were focused on seminars, training or tailored physical activity among HCW aimed at MSD prevention.
Discussion
General comments
To our knowledge, despite the presence of a recent systematic review [18] focused on the prevalence rate of WR-MSD in HCW, this is the first scoping review which is focused on WR-MSD and disease among HCW and on the identification of the approaches used to assess them. In this frame, it is worth noting that, in the literature, when focusing on MSD, the term “disorder” is often interchanged with “disease” and vice versa, although they do not denote the same conditions. In fact, “disease” identifies conditions characterised by structural damage with a loss of function and specific symptoms and signs [30]; on the other hand, “disorder” is a condition characterised by loss of function without structural damage, whereas the presence of signs and symptoms is not essential to define a disorder. For example, musculoskeletal pain does not necessarily suggest an underlying structural change, so it can be considered a disorder. This underlying noise in the search led to discrepancies in the identified pathologies [31].
Specifically focusing on the clinical aspects, we notice that none of the studies comprehensively reported clinical objective details about the medical diagnosis. We strongly believe this is a fundamental aspect that must be covered in this kind of analysis, together with the adoption of the International Classification of Disease (ICD-10) [32–34], which allows us to unambiguously identify diseases and then analyse the different conditions in-depth, giving researchers the possibility to compare the situation worldwide. However, the research of correlation between musculoskeletal symptoms and anthropometric factors emerged from included studies. According to current evidence from the literature, BMI is one of the most critical factors associated with musculoskeletal pain uprising [35]. Among the included studies, 51% analysed this aspect, but few quantitatively evaluated the correlation between BMI and MSD. By stratifying it in classes, we report that about 21% of the included studies reported the BMI value. In this frame, the choice to report anthropometric and demographical data, as well as the work experience, only in value ranges instead of descriptive statistics (i.e., average value and standard deviation) may be helpful for the paper’s readability. Still, it makes sense to compare different studies whenever they do not report the information about data distribution.
Concerning the healthcare professionals included, the results point out that the categories most analysed were nurses and surgeons working in public and private companies. This finding is consistent with the current literature since data report that professionals close to patients and their aid are more vulnerable to MSD [36]. However, it is worth explaining that the exact professional figure has a different scope of practice and tasks among other countries due to the organisation of each specific National Healthcare Service [37]. In Europe, for instance, 13 countries present significant heterogeneity in laws and regulations on nurse prescribing [38]. These general differences in medical assistance planning imply different biomechanical overloads associated with their working activities [39]. Furthermore, the differences in the definition of working activities are based on other working backgrounds among medical doctors, nurses, etc. The Italian Healthcare System, for instance, includes social health workers (e.g. certified nurse assistants) [40] who assist patients in their daily activities and personal hygiene and cooperate with healthcare professionals. The presence or absence of this professional figure drastically changes the biomechanical workload for other healthcare professionals.
From the analysis of included studies, musculoskeletal symptoms were studied using specific surveys where healthcare professionals filled in questionnaires and reported their opinions and feelings. Among others, the most used questionnaire was the Nordic Musculoskeletal Questionnaire [41], developed in 1987 in English and Scandinavian languages and translated into several idioms. Further included studies used a modified version of the Nordic Musculoskeletal Questionnaire, where authors added custom-made sections; in these specific cases, it needs to be clarified whether these questionnaires were previously validated.
Only 21% of included studies assessed MSD by using objective methods. The most used technologies were cameras: thanks to that, several photographic sequences are usually made during daily activities to provide objective feedback for the risk assessment. In second place, video cameras are reported to be used to acquire the working tasks during the daily shift. In general, all these instruments were used without the definition of a specific protocol for the acquisition and analysis, but only by empirical approach; indeed, this issue makes it difficult to analyse and compare different reported situations and conditions. Finally, a small percentage of the identified studies report the use of wearable sensors to quantify specific information concerning the activities performed by the worker; in particular, we found the reported use of surface electromyography for detecting muscular activation and fatigue and inertial measurement units to estimate worker movements.
To conclude, some studies also evaluated the efficacy of training events in managing WR-MSD. In particular, the most common solution was participation in seminars. The training efficacy was evaluated using specific questionnaires, where musculoskeletal symptoms were estimated before and after the training. On the other hand, no particular evaluation of the training events was used.
Implications, recommendations and future directions
Firstly, we remark on the confusion in the definition of the clinical aspects (i.e., sometimes the term “disease” has been used instead of “disorder” and vice versa), and we also detected bad variability in the terms used to indicate pathologies. To solve these problems, we encourage the use of ICD-10, which allows us to “code” in an unmistakable way the pathologies and health-related issues; indeed, this system has been adopted in more than 100 World Health Organisation (WHO) countries and translated into more than 30 languages and permits a better and unequivocal communication among researchers to improve the use of literature results in the clinical context. Secondly, we highlight the scarce use of technological instruments and validated tools as an evaluation medium. In our opinion, this can compromise the study’s replicability and increase variability in the assessment. Furthermore, introducing and using specific technology can support the correct ICD-10 classification. Thirdly, it is worth underlining the need to evaluate and measure essential factors regarding the subjects included in the studies, such as BMI, comorbidities and degree of exposure to biomechanical overload during work activities using validated scales or methods. Fourthly, we firmly think it is essential to introduce, share and use reliable and standardised tools and methods to obtain objective criteria in the assessment process; the use of a standardize approach is indeed essential to ensure the possibility of comparing also the outcomes provided by different studies.
Finally, we recommend the adoption of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) [42] in the case of observational studies or the CONsolidated Standards of Reporting Trials (CONSORT) Statement [43] in the case of randomised trials for accurate and complete reporting. Considering all these aspects can help improve the external validity of studies and the quality of their results.
Limits
This project presents several methodological limitations. Firstly, our time range was limited to 2000 to 2022: technologies used before 2000 are considered outdated. In addition, the literature trend reported a substantial increase in this kind of analysis in the last decade. Secondly, we decided to include only English-written papers. Thirdly, we have not retrieved the full text of 52 papers: we had no additional budget to buy papers, and due to the limited time scheduled for this project, we did not write to authors. Fourthly, the choice of presenting a scoping review as a specific study design can be considered weaker concerning the more generalised systematic review; however, this methodology has been improving thanks to the contribution of more and more researchers, as highlighted in the literature [24]. We followed the most recent guidelines and publications in this field to reduce bias and methodological errors.
Conclusions
This scoping review mapped the current literature analysing WR-MSD and diseases among HCW and defined the methods used to assess them. The presence of musculoskeletal disorders in healthcare professionals is unmistakable, and the researchers’ attention to this field has been improving more and more during the last decades. An improved quality of studies and a wider adoption of validated questionnaires and technologies help enhance our knowledge and evidence in this field.
Author contribution
Study concept & design: RG, SE, LNF.
Acquisition of data: RG, SE, DPG, LNF.
Analysis and interpretation of data: RG, SE, DPG, AIF, DC, MM, MV, PE.
Drafting of manuscript: RG, AIF, DC, MM, MV, PE.
Critical revision of manuscript for intellectual content: RG, SE, GDP, LNF.
Open science framework registry number
Rossetto, G., Sala, E., De Palma, G., Albertelli, I.F., Donatoni, C., Mazzali, M., Merlino V., Paraggio E., Lopomo, N.F. (2022, July 11). Musculoskeletal disorders and diseases in healthcare workers: a scoping review protocol. https://doi.org/10.17605/OSF.IO/UMCSN.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Conflicts of interest
The authors declare that they have no conflict of interest.