
Abstract
BACKGROUND:
Telehealth is becoming more prevalent in physical therapy, involving a whole host of clinical services. These services are often provided without structured training in telehealth, and no formal curricula currently exist for this purpose.
OBJECTIVE:
To develop a set of educational competencies (ECs) to guide instruction of telehealth-related skills in entry-level programs (i.e., Doctor of Physical Therapy), existing programs (i.e., residencies and fellowships), and potential future post-graduate programs specific to telehealth physical therapy.
METHODS:
Physical therapists and physical therapist assistants from diverse geographic locations and practice areas were invited to participate on an expert panel. A modified Delphi process was then used to evaluate the acceptability of draft ECs gathered from the extant literature by a steering group. Draft ECs were presented to the expert panel on a questionnaire, which asked expert participants to rate each draft EC according to applicability and clarity. Draft ECs were accepted if they met a priori established criteria for acceptability and clarity. Unendorsed ECs were revised by the steering group according to open-ended comments from respondents and presented during a subsequent round. Three rounds of surveys were undertaken.
RESULTS:
Thirty-eight participants formed the expert panel; 38 participants completed the Round 1 survey, 28 participants completed the Round 2 survey, and 24 participants completed the Round 3 survey. Delphi group members approved 48 ECs in the first round, 23 ECs in the second round, and 2 ECs in the third round. There were 4 ECs that remained unendorsed after the modified Delphi process. Endorsed ECs spanned 7 conceptual areas. Distinct sets of ECs characterized expected end points of first professional degree, existing residency and fellowship, and potential future telehealth physical therapy post-graduate program.
CONCLUSIONS:
Consensus-based ECs identified in this study may guide instruction in knowledge and skills relevant to physical therapy telehealth.
Keywords
Background
The novel coronavirus 2019 (COVID-19) pandemic introduced public health requirements for physical distancing, which challenged traditional notions of current physical therapy delivery models. Building on existing in-person and in-clinic models, many clinicians rapidly incorporated more evaluation and intervention delivered by telephone, video, and electronic mail [1–3], supported by temporary changes in federal and state payment [4–6] and licensure provisions [7–9]. These changes were feasible and acceptable to clinicians and patients for outpatient musculoskeletal care [3], especially when there was payment parity between in-person and telehealth visits [10]. Physical therapy telehealth services may reduce the time needed to access an appointment and improve geographical reach compared to in-person care, with similar patient satisfaction [1]. Survey studies indicate telehealth may be acceptable to patients [11], especially if out-of-pocket expenses for video visits are less than in-person visits [10]. Data suggest telehealth modalities may remain popular as a health service delivery model for physical therapy and rehabilitation in the post pandemic era.
Telehealth has been variously defined by health care and physical therapy professional societies [12]. For example, the World Health Organization defines telehealth as the delivery of health care services, where distance is a critical factor, by all health care professionals using information and communication technologies for the exchange of valid information for diagnosis, treatment, and prevention of disease and injuries; for research and evaluation; and for the continuing education of health care providers, all in the interest of advancing the health of individuals and their communities [13]. The World Physiotherapy/International Network of Physical Therapy Regulatory Authorities propose that digital physical therapy practice describes health care services, support, and information provided remotely via digital communication and devices [14]. The common factors among telehealth definitions are that the clinician interacts with the patient or client at some distance in space and time, and through some type of technology to share information [15].
Telehealth physical therapy involves a distance between the physical therapist and patient/client that introduces unique challenges to organizing and completing the clinical encounter. During the COVID-19 pandemic, physical therapists have reported using a wide range of subjective and objective procedures they have adapted to the telehealth environment [16]. These procedures frequently included subjective questioning and functional testing [16]. Approximately half the time, physical therapists provided self-directed palpation and special tests [16]. Less frequently, physical therapists also performed observational movement analysis, patient reported outcome measures, accessing or ordering clinical imaging, caregiver and family training, and providing on-screen annotation with electronic drawing tools [16]. Common interventions included education, advice, exercise, and self-directed manual therapy procedures [16].
Telehealth interventions in more common practice since the beginning of the COVID-19 pandemic are consistent with prior calls for a ‘new normal’ in musculoskeletal physical therapy that is primarily active, focused on self-efficacy and self-management, and less reliant on passive hands-on therapies [15, 17]. Yet, despite the range of services provided during telehealth that align with preferred practices, two-thirds of respondents reported not providing any telehealth services prior to the COVID-19 pandemic [16]. This observation suggests that widespread modifications to practice were made without substantial prior training and experience. There is a continued paucity of evidence-based practical guidance for effective physical therapy telehealth practices.
Challenges inherent to working with patients and clients at a distance suggest physical therapists must learn a specific set of knowledge and skills for best practice [15]. Yet, educational competencies (ECs) related to the practice of telehealth physical therapy remain unclear. A recent study identified 60 ECs for telehealth physical therapy across seven domains [18]. However, the reliability and prioritization of ECs in telehealth physical therapy remain unclear. Data to fill these remaining gaps in the literature will assist physical therapy education programs in building curricula to support implementation and high-quality practice. In addition, it is unknown whether current data related to ECs for physical therapy video conferencing will generalize well to other forms of telehealth [18].
To build on nascent findings in the literature, the primary purpose of this study was to independently establish consensus-based ECs in an expert group composed of physical therapists and physical therapist assistants with well-characterized expertise in delivering telehealth through a variety of modalities. The secondary purpose of this study was to prioritize ECs based on level of education, including entry-level Doctor of Physical Therapy programs, existing post-graduate programs (i.e., residencies and fellowships), and future post-graduate programs specific to physical therapy telehealth. For the purpose of this study, we define ECs as knowledge, professional behaviors and clinical skills required by physical therapists to provide quality care to their patients.
Method
Research design
This descriptive study employed a modified Delphi method to reach consensus regarding the development of telehealth ECs for United States-based entry-level physical therapist education programs. The Delphi method is an iterative process for reaching consensus among experts on a given topic [19]. It has been applied successfully across health professions education, including medicine, nursing, and physical therapy [18–21]. The method is iterative and anonymous. The iterative nature of this process may provide participants with the opportunity to assess comments made by other Delphi participants, reflect on their initial judgments, and modify their responses accordingly. The anonymous nature of this process helps offset the limitations of in-person discussions, including dominance of conversations by a single individual or subgroup of individuals and pressure to conform to the group [19, 22]. Data from Delphi approaches are often organized by multiple rounds of surveys completed by group participants [19, 22]. Each subsequent survey is shaped by participant responses to each previous survey [19, 22]. In a modified Delphi approach, the first survey is constructed by pre-selected materials, instead of group consensus that guides first survey design in the traditional Delphi method [22].
Participants
A steering group (TED, ACL, DMM, and BR) was created that consisted of physical therapy clinicians and educators with clinical and scholarly expertise in telehealth physical therapy and Delphi methods. The roles of the steering group were to gather draft ECs for the Round 1 survey, review the quantitative and qualitative data from the Delphi group related to each proposed EC, assess the acceptability of each proposed EC against a priori determined study criteria, recommend modifications to proposed ECs in response to input from the Delphi group, and pilot test study-related surveys. Discrepancies were resolved by discussion and consensus.
Delphi group participants were eligible to participate if they were licensed physical therapists or physical therapist assistants with self-identified experience in telehealth practice, research or clinical leadership. Participants were selected using purposive sampling techniques. The study team was intentional in recruiting and purposefully selecting experts with varied clinical and educational experiences from diverse clinical settings. Recruitment emails initially were sent to Agile Physical Therapy and the Kaiser Permanente Northern California Telehealth Physical Therapy Peer Group. These organizations and individuals were selected because of their longstanding experience with providing and leading telehealth physical therapy for outpatient musculoskeletal care before the COVID-19 pandemic. Recruitment emails were sent to individuals with known expertise outside of outpatient musculoskeletal physical therapy to diversify the Delphi group by practice area and geography. In addition, recruitment emails were sent to the leadership of the Acute Care and Home Health Academies of the American Physical Therapy Association.
A target panel size of at least 25–30 members was established based on prior guidance [22, 23]. This panel size was selected because reliability of results are thought to be maximized and redundancy of inputs is considered optimized. Members of the study team and recruited participants were encouraged to recommend individuals perceived as having the requisite expertise in physical therapy telehealth to increase geographic and practice area representation in the Delphi panel to maximize representation. Individuals who expressed interest in participating were screened based on inclusion criteria and the study team’s desire to have broad representation across practice settings. Participants were informed in advance regarding the study’s purpose, competency inclusion criteria, and duration. The study was approved by the Institutional Review Board at University of the Pacific (Stockton, California, United States; approval #2021-84). All participants consented to participate in each survey.
Instrumentation
This modified Delphi study used a list of ECs for the first round, which was compiled by the study team from resources describing various professional competencies regarding the role of clinicians in telehealth [14, 25]. Incorporating competencies from these pre-existing resources ensured initial content validity of the initial survey. The Round 1 survey consisted of a demographic questionnaire and a set of proposed ECs to which the participants may respond.
Participants provided four inputs for each proposed EC, consisting of a combination of quantitative and qualitative data. First, participants were asked to rate their level of agreement that the proposed EC is appropriate for (1) first professional degree education, (2) education in the context of existing post-graduate programs accredited by the American Board of Physical Therapy Residency and Fellowship Education, and (3) a dedicated telehealth physical therapy fellowship program. Agreement ratings were assessed using a 5-point Likert scale, ranging from “Not At All Relevant” to “Extremely Relevant.” Second, participants were asked to rate clarity of expression for the proposed educational competency. Clarity ratings were assessed using a 5-point Likert scale, ranging from “Extremely Unclear” to “Extremely Clear.” Third, participants were asked to provide a brief written rationale for supporting or rejecting a proposed EC. Fourth, participants were asked to provide a brief open-ended response for how to improve the proposed EC in the event they rejected it.
Procedures
Each survey was pilot tested by a member of the steering group before deployment. All surveys were created and circulated using Google Forms (Mountain View, California, United States). Personalized survey links were distributed to all participants who met the study’s inclusion criteria. Participants initially were provided two weeks to complete each survey round. The steering group sent reminder emails to participants during this window, and two additional email attempts after each two-week window to encourage survey completion. Upon completion of the Round 1 survey, results for each competency were analyzed to determine whether consensus was achieved. If consensus was not achieved for a particular EC, that item was carried forward to the second round after discussions and revisions by the steering group based on participants’ open-ended comments. ECs that achieved consensus but were not perceived as being clear were carried forward with modifications by the steering group to improve clarity. One person from the group combined feedback from steering committee discussions to format the EC. Finally, the Round 3 survey was developed using the same process described for the Round 2 survey. Approximately three weeks elapsed between each survey round. Data were collected over a period of three months, from July to October 2021. Individual responses remained anonymous throughout the study.
Analysis
Consensus for each proposed EC was achieved if two criteria were met: (1) a median score of 4 or greater for relevance for a proposed educational competency; and (2) 80% or greater of participants rating the proposed educational competency as “Somewhat Clear” or “Extremely Clear” (i.e., at least 4 on the 5-point Likert scale). These criteria are consistent with recommended data handling for Delphi studies [19, 22]. The use of median scores for Likert-type scales is strongly favored as a measure of central tendency secondary to potential dispersion of the data [19, 21]. Levels of agreement to establish consensus range from 51% and 80% [19, 21], so the criterion level for clarity used in this study would be considered stringent. Participants remained blinded to relevance and clarity ratings from previous rounds of ECs that were revised. Microsoft Excel (Redmond, Washington, United States) was used to manage the data and to calculate the descriptive statistics used in this study.
Characteristics of the Delphi group (n = 38)
Characteristics of the Delphi group (n = 38)
Expert panel characteristics
Expert panel characteristics are summarized in Table 1. The initial expert panel consisted of 38 participants, including 25 women (65.8%). The expert panel consisted of 34 physical therapists (89.5%) with mean age of 42.5 years (95% confidence interval [95% CI]: 41.2–43.8 years). Twenty-seven participants (71.1%) had a Doctor of Physical Therapy degree and their mean experience as a clinician was 15.8 years (95% CI: 14.4–17.3 years). Expert panel participants worked 30.7 hours per week as a clinician (95% CI: 28.5–32.9 hours). Two-thirds of the expert panel also worked as an owner, administrator, or manager for a mean of 9.6 hours per week (95% CI: 7.3–11.9 hours). Most commonly, expert panel participants reported working in an outpatient clinic (n = 31; 81.6%) in an urban setting (n = 33; 86.8%) with orthopedics as the primary practice area (n = 23; 60.5%). Thirty-seven expert panel participants already provided telehealth services for a mean of 2.9 years (95% CI: 2.4–3.3 years). Expert panel participants most frequently reported that one-third or less of overall encounters were telehealth-based (n = 23; 60.5%). Most often reported telehealth services were evaluation (n = 36; 97.3%), treatment (n = 35; 94.6%), and consultation and education for patients, clients, and the community (n = 27; 73.0%). Video (n = 34; 91.9%) and telephone (n = 26; 73.0%) were most frequently used by the expert panel participants.
First-round survey
Thirty-eight participants completed the first-round survey (Table 2), evaluating 76 draft ECs. Of the 48 ECs that were accepted by the Delphi group, 8 involved ethics (16.7%), 2 were regulation (4.2%), 2 were administrative (4.2%), 8 included technical skills (16.7%), 17 involved clinical skills (35.4%), and 11 covered affect and communication (22.9%). Thirty-six ECs applied to all levels of training (75.0%), 5 applied to existing physical therapy post-graduate training programs (10.4%), and 7 ECs involved post-graduate training specific to physical therapy telehealth (14.6%).
Telehealth physical therapy educational competencies accepted after the first round (n = 48). For each competency, values are mean (95% confidence interval) in the first nested row and median (interquartile range) in the second nested row. Values in bold exceeded the threshold for acceptance
Telehealth physical therapy educational competencies accepted after the first round (n = 48). For each competency, values are mean (95% confidence interval) in the first nested row and median (interquartile range) in the second nested row. Values in bold exceeded the threshold for acceptance
The remaining 28 ECs that were not accepted during the first round were edited for clarity by the steering group based on open ended comments by the participants. Draft ECs that were not accepted during the first round predominately related to research and development, regulation, and administration. During the revision process, several draft ECs were divided to be more specific and measurable. The revision process yielded 30 revised draft ECs for presentation on the second-round survey.
Twenty-eight participants completed the second-round survey (73.6%; Table 3). Among the 23 ECs that were accepted in this round, 1 involved ethics (4.4%), 1 related to research and development (4.4%), 8 were regulatory (34.5%), 4 were administrative (17.4%), 3 included technical skills (13.0%), 4 covered clinical skills (17.4%), and 2 were affect and communication (8.7%). Ten ECs applied to all levels of training (43.4%), 2 involved existing physical therapy post-graduate programs (8.7%), and 11 were for post-graduate training specific to physical therapy telehealth (47.8%).
Telehealth physical therapy educational competencies accepted after the second round (n = 23). For each competency, values are mean (95% confidence interval) in the first nested row and median (interquartile range) in the second nested row. Values in bold exceeded the threshold for acceptance
Telehealth physical therapy educational competencies accepted after the second round (n = 23). For each competency, values are mean (95% confidence interval) in the first nested row and median (interquartile range) in the second nested row. Values in bold exceeded the threshold for acceptance
The remaining 7 draft ECs that were not accepted by the Delphi group during the second round were again reviewed and revised by the steering group according to open ended comments by the participants. Draft ECs that were not accepted during the second round primarily related to regulatory and administrative functions. The steering group voted to strike one EC due to redundancy and revised the remaining 6 draft ECs for presentation to the Delphi group on the third-round survey.
Twenty-four Delphi group participants completed the third-round survey (63.2%; Table 4). Two additional ECs were accepted, which involved administrative functions (100.0%). These ECs were considered appropriate for post-graduate programs specific to physical therapy telehealth. Five draft ECs were not accepted during the Delphi group process (Table 5). Of these draft ECs, 4 were not accepted because Delphi group participants could not assign the EC to a level of training and 1 was not accepted because it was insufficiently clear.
Telehealth physical therapy educational competencies accepted after the third round (n = 2). For each competency, values are mean (95% confidence interval) in the first nested row and median (interquartile range) in the second nested row. Values in bold exceeded the threshold for acceptance
Telehealth physical therapy educational competencies accepted after the third round (n = 2). For each competency, values are mean (95% confidence interval) in the first nested row and median (interquartile range) in the second nested row. Values in bold exceeded the threshold for acceptance
Draft educational competencies not accepted during the Delphi group process
This study used a modified Delphi process to derive consensus-based ECs for telehealth physical therapy, which can be used in first professional degree programs, existing residencies and fellowships, and potential future postgraduate training programs specific to telehealth physical therapy. The size of the expert group in this study was within acceptable ranges for size [22, 26] and demonstrated adequate representativeness to generalize to many areas of outpatient physical therapy practice. The principal findings of the study were 73 ECs identified within 7 conceptual areas.
Ethics (9 ECs)
Telehealth physical therapy ethics guides the professional conduct of physical therapists in the virtual treatment space. Ethical activities involved acting with honesty and integrity, protecting one’s own and the patient’s/client’s privacy, assessing and accommodating individual needs and preferences, determining when a caregiver or advocate must be present, adhering to cultural and religious norms, determining when ancillary services may be necessary to optimize communication, and informing the patient of their rights, responsibilities, and right to refuse its use. These ECs provide a framework for a telehealth code of ethics for physical therapists by meaningfully building on normative ethical foundations and adapting them to guide conduct within the digital clinic space [27]. Perhaps supporting the foundational nature of ethical thinking to practice, all ECs in this domain were considered skills consistent with expectations for the first professional degree.
Clinical skills (21 ECs)
Clinical skills in telehealth physical therapy involve important adaptations of in-person skills. The ECs identified in this study suggest that patient triage is important in the virtual and physical clinic spaces. In addition to triaging the patient for conditions that may not respond to physical therapy intervention, the physical therapist must triage the patient for appropriateness of telehealth services. The ECs in this study support that risk management practices, such as for personal and environmental emergencies, must be handled remotely in telehealth physical therapy. This finding is consistent with prior telehealth competencies in physical therapy literature [18]. Examination-related ECs from this study support the need for physical therapists to develop procedural and digital means to gather relevant information to complete a differential diagnosis and to develop a plan of care. The ECs also support the need to use health information and clinical guidelines from reputable sources to inform the development of a diagnosis, as well as to formulate and carry out the plan of care.
Affect and communication (13 ECs)
Communication of content and affect were considered important in telehealth physical therapy practice. Practice in the remote environment may limit the set of important context cues that are important to build a therapeutic relationship between the patient and clinician. As such, affect and communication ECs were prominent findings in this study. This emphasis by the Delphi group suggests the important of ensuring the patient’s affective needs are met and to respond in a situationally congruent manner while providing telehealth physical therapy. Telehealth physical therapy appears to place a specific premium on openness and flexibility, recognition and understanding, and welcoming and confidence-building. While many of these communication characteristics may not be unique to the virtual clinic space, educational activities may emphasize how they are adapted with the use of video and audio communications technologies and further academic and clinical training is necessary [18].
Administrative (8 ECs)
Program administration in telehealth involves operational considerations of service delivery, including workflows, policies and procedures, and workforce development. Unique administrative functions appear to characterize telehealth physical therapy, which was reflected in ECs endorsed by the Delphi group in this study. Adherence to standards that enable consistent and accurate collection and exchange of health information across health systems and services was identified as a first professional degree skill. The other administrative ECs were selected for a potential future post-graduate training program directed to telehealth physical therapy. These competencies involve developing policy, assessing the quality of clinical education, advocating for mutually advantageous payment models, promoting digital equity, and teaching telehealth physical therapy in professional and post-professional courses.
Regulatory (10 ECs)
Regulatory affairs in telehealth involves determining and following the appropriate laws and regulations that govern physical therapy telehealth practice, as well as to both create and act on opportunities to influence telehealth laws and policies. The Delphi group endorsed various competencies in regulatory affairs related to telehealth physical therapy in this study. Determination of payment sources, following rules established by payment policy, and adhering to policy to promote digital equity were considered ECs consistent with first professional degree training. Most ECs for regulation were identified as relevant to a potential future telehealth physical therapy post-graduate training program, including familiarity with the various types of information and communication technologies, strategy development, and consulting with government policymakers. These ECs can help position physical therapists in key decision-making capacities with respect to how physical therapy telehealth is regulated, in addition to the implementation of those regulations at the level of practices and health systems.
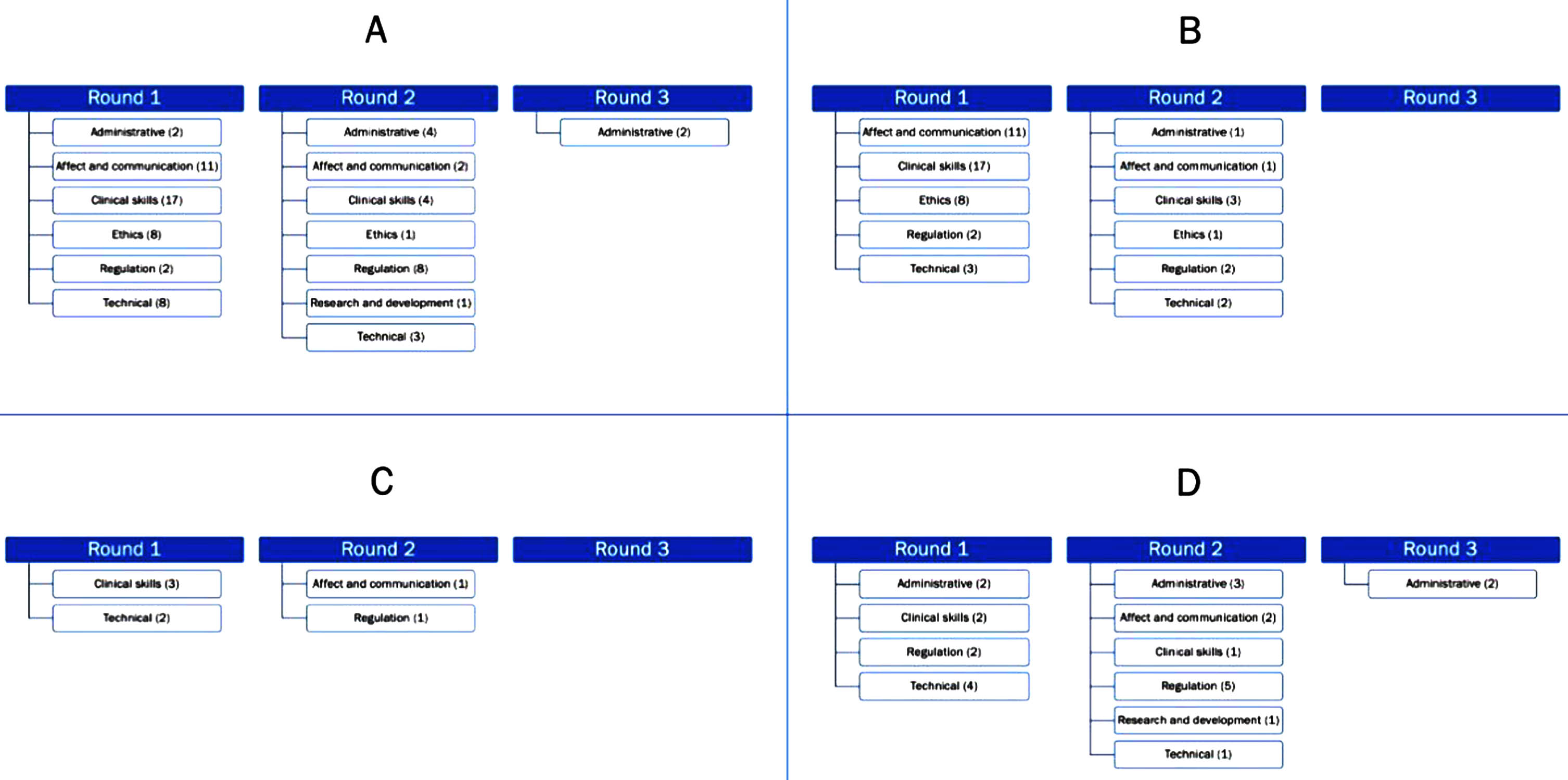
Approved educational competencies, including the total number approved in each category (A), as well as competencies approved as unique to Doctor of Physical Therapy first degree education and training (B), existing residency and fellowship programs (C), and a future telehealth focused post-graduate education and training program (D).
Technical skills in physical therapy telehealth involve proficiency with service delivery models and health information systems broadly, as well as understanding of the specific hardware and software necessary to conduct visits and documentation. The need for technical competency seems obvious for effective telehealth physical therapy. ECs for technical competency at the first professional degree level were primarily basic troubleshooting and utilizing established technologies, policies, and procedures within existing models of clinical service delivery. Development of those technologies, policies, procedures, innovative service delivery models, and alternatives was endorsed for a potential future telehealth physical therapy post-graduate training program. In addition, competencies were identified for training patients to use information and communication technology, in addition to training physical therapists and physical therapist assistants.
Research and development (1 EC)
This study identified an EC that involves collaboration with members of other disciplines and the technology industry to develop innovative technologies, processes, policies, and procedures for telehealth service delivery. The physical therapist’s role in telehealth research and development is important to ensure hardware and software that meets the needs of patients, clinicians, and rehabilitation systems. Informed collaboration with and leadership of multi-disciplinary teams will necessitate developing a familiarity with technological development and implementation. The Delphi group identified these inter-sectoral collaborations specifically may be opportunities for students of future telehealth physical therapy post-graduate programs. In fact, other research methodology and statistical analysis with platform and panel trials and other observational and cohort studies may be required to address complex multi-level telehealth implementation when randomized trials are not feasible [18].
This study did not specify telehealth modality; yet overall, this study generally agrees with the only other existing study to develop ECs for physical therapists who engage in videoconferencing, a specific physical therapy telehealth modality [18]. Using a Delphi process involving an international cohort of physical therapists, Davies et al. [18] found 60 ECs organized into 7 conceptual domains. There was substantial overlap in the content of recommendations and conceptual domains between Davies et al. [18] and the present study, indicating a high level of agreement. Agreement between findings of these studies is evidence in favor of content validity for these ECs. Differences in findings between studies may be related to differing compositions and experiences of the expert panel participants between studies, differences in candidate ECs entered into the modified Delphi process, and more general focus of this study on physical therapy telehealth more broadly rather than videoconferencing. The present study also developed competencies that may be appropriate for post-graduate training programs. These findings may stimulate the ongoing development of expertise in telehealth by providing the basis for curricular additions to existing residencies and fellowships, as well as the formation of future post-graduate programs specific to telehealth and digital physical therapy practice.
A unique contribution of this study was the identification of educational level for which an EC may be most appropriate. For example, in this study, three clinical skills were considered most appropriate for existing residency and fellowship programs, including presenting patient data clearly to colleagues using information and communication technology, design and implement a risk prevention plan to support patient safety, and to provide advice about reliable and safe health information on the internet. These functions appear appropriate for clinical experts who provide high level care, participate in the development of processes and procedures, and educate other physical therapists. Two clinical skills were considered appropriate for future post-graduate training programs specific to telehealth physical therapy, including to analyze the quality of digital resources and to determine the risk or benefit associated with distance and cost. These administrative functions by physical therapists specifically prepared to perform appraisals of quality for digital health information and cost-benefit analyses may inform clinical processes and procedures to be implemented by staff physical therapists. Additionally, this study addresses educational competencies based on entry-level clinical Doctor of Physical Therapy degree and beyond. There is substantial diversity in education standards and expectations for physical therapists in different parts of the world, therefore the standards provided by Davies et al. may not specifically address the needs and gaps in educational qualifications of PTs in the United States of America [18].
The present study identified more general competencies for physical therapists than previous research, which could be applied to a wider range of information and communication technologies. Access and literacy with digital technology is becoming better recognized as an important determinant of health [28–30]. The frequency of household broadband access and internet access still lags in the United States compared to other wealthy countries [31], although the frequency of mobile broadband access is high [32]. Disparities in digital access led Menendez and colleagues to describe the ‘telehealth paradox,’ in which patients with chronic health conditions and poor access to in-person care who may benefit most from telehealth participate the least [33]. The ECs identified in this study will prepare physical therapists to address the digital divide by understanding and deploying diverse information and communication technologies, as well as to identify patients and clients who may require referral for subsidized access to broadband services and digital devices as well as provide a hybrid approach to in-person and digital care.
There is a mismatch between empirically derived measurements [34] and patient perceptions [35, 36] of the utility and quality of telehealth physical therapy, which introduce challenges to long-term implementation. Bennell and colleagues established that many patients were unlikely to pursue individual sessions through telehealth after in-person sessions became available again during the COVID-19 pandemic, even though their general perceptions of the telehealth experience were positive and physical therapists intended to continue to provide virtual services [35]. These findings agree with data from Barton and colleagues, who identified concerns among patients that telehealth physical therapy is inferior to in person care, despite a high proportion of clinical improvement and patient perception of increased access to services [36]. By contrast, Tenforde et al. measured a high rate of patient satisfaction and intended future utilization of telehealth rehabilitative services [37]. Patients identified additional benefits of eliminating travel time and convenience [37]. Yet, they reported technology and absence of hands-on care by a clinician as limitations [37]. In addition, large percentage of Medicare beneficiaries utilizing telehealth services in physical therapy during the pandemic had a pre-existing patient- to-provider relationship [38]. These data suggest that practices associated with the ECs identified in this study— such as patient screening for appropriateness of telehealth physical therapy, patient education regarding the potential benefits and limitations of telehealth modalities and making visible clinical markers of improvement to patients— may be important to providing high-value care. Implementing observations from this study may narrow the efficacy-satisfaction paradox of telehealth, especially for patients who are new to the attending clinician and new to telehealth as a modality to receive care.
This study had limitations that may be addressed by future research. The Delphi process was modified in that the expert group was provided with draft ECs to approve instead of developing them. This methodology may have biased the group toward only considering the draft ECs that were presented to them and may have limited consideration of others that could have been noteworthy to include. Although steps were taken to recruit a diverse cohort across practice areas, the composition of the Delphi process was heavily weighted toward practicing physical therapists working in urban outpatient orthopedic settings. This characteristic may limit generalizability of findings to practice areas that were under-represented in the expert group. The expert panel’s assessment of appropriateness for ECs for a potential future telehealth physical therapy fellowship may have been limited by the fact that the fellowship does not yet exist, so criteria, objectives, and endpoints for this program might have been difficult for the expert panel to anticipate. Nevertheless, the group had substantial practical experience in telehealth physical therapy, and the ECs identified through the Delphi process generally agree with extant literature. Further work should be undertaken to operationalize the results of this study in building curricula for Doctor of Physical Therapy and residency and fellowship programs, as well as to characterize the potential role and need for specific telehealth physical therapy post-graduate training programs. Most of the expert panel engaged in significant telehealth physical therapy practice prior to the COVID-19 pandemic, which positioned them to understand the educational needs in telehealth physical therapy outside the context of a public health emergency. Yet, it is difficult to determine whether and how the experience of the COVID-19 pandemic may have affected the responses generated from the Delphi sample.
In conclusion, the purpose of this study was to identify ECs in delivering telehealth through a variety of modalities and to target ECs appropriate to specific levels of physical therapy education, including first professional degree (i.e., Doctor of Physical Therapy), physical therapy residency, or telehealth physical therapy post-graduate programs. This study provides a set of consensus-based ECs in telehealth physical therapy, which both validate and build on previous work. Findings from this study may be used to construct and evaluate curricula to better train physical therapists and physical therapy assistants to provide high quality telehealth, and therefore, to improve satisfaction and quality of care.
Ethical approval
This study was approved by the Institutional Review Board at University of the Pacific (Stockton, CA, USA; approval #2021-84).
Informed consent
All participants indicated informed consent to participate in each survey for this study.
Conflict of interest
The authors affirm no financial/commercial and non-financial/commercial conflicts of interest in the material presented in this manuscript.