
Abstract
BACKGROUND:
Mindfulness-based, in-person programs are effective at reducing stress and enhancing resilience in military and civilian samples, yet few studies have examined or compared training offered via real-time, interactive social media. Such a program would have a wider-reach and could include those unable to attend in-person. There is also interest in resolving ambiguity about the effects of mindfulness training on individual difference variables, such as self-compassion.
OBJECTIVE:
The purpose of this research was to compare pre/post self-compassion for three interventions; Mindfulness-based Stress Reduction delivered in-person (IP), mindfulness meditation training delivered via a Virtual World (VW), and a wait-list Control Group (CG) among active duty and veteran U.S. military.
METHODS:
A 2 (pre/post)×3 (group) factorial design was conducted with 250 active duty and veteran U.S. Military service members, with self-compassion measures as dependent variables.
RESULTS:
Self Compassion improved 10% for the IP group and 14% for the VW group, while the CG group did not improve. Combined treatment groups yielded a 10.3% improvement in self-compassion compared with no change in the CG and with a group×time interaction effect (p < 0.01). Participants with lower initial self-compassion experienced greater benefits than those with higher baseline self-compassion (p < 0.01).
CONCLUSION:
IP and VW Mindfulness Meditation training were equally effective in increasing self-compassion. Adding effective on-line mindfulness delivery will promote self-compassion among a more extensive audience, likely yielding improved coping, confidence, connectedness, cheerfulness, steadiness, and self-satisfaction, while lessening anxiety, fear-of-failure, and stress among participants.
Keywords
Introduction
Work offers numerous health benefits. Relative to unemployed individuals, employees report higher self-esteem and better solution-oriented coping [1] and are less likely to be depressed [2] or contemplate suicide [3]. However, work-related stress can negatively impact employee performance and health. A report by the American Heart Association found high job demands contribute to the $46 billion dollars in annual ‘excess’ health care costs [4]. In addition, it is reported that stress management is effective at boosting individual-level health and, to a lesser degree, organizational health [4].
This paper addresses one portion of a larger study. In the full study, we examined the impact of mindfulness meditation training on resiliency in active duty and retired military service members, measuring outcomes such as stress, coping strategies, physical symptoms, post-traumatic stress, and self-compassion. This paper presents information on the intervention of mindfulness meditation on self-compassion.
U.S. military personnel are exposed to inordinate stress, including frequent deployments, prolonged separation from loved ones, injuries, and combat. Over time, these stressors may individually or collectively contribute to the onset of psychopathologies that can impair performance, such as posttraumatic stress disorder (PTSD) [5–8]. Maintaining emotional and social resilience is challenging in such settings. Accordingly, there is a need to identify reliable and effective techniques and delivery methods for enhancing service members’ abilities to attain and maintain healthy coping behaviors.
Mindfulness training
Mindfulness-based stress reduction (MBSR) training focuses on enhancing present-moment awareness [9]. Participants learn to recognize their state-of-being and their reactions to their internal and external environments in a non-judgmental manner. MBSR techniques include body scanning (focusing attention on particular body parts one at a time), sitting meditation, walking meditation, and Hatha Yoga (stretching movements that focus on the physical sensations of movement). Personal attention is focused on sensations including interoception, sound, sight, touch, proprioception; emotions; and thoughts [9–11]. Mindfulness meditation training has been shown to enhance cognitive and executive functions [12, 13], and decrease symptoms of stress, pain, and sleepiness [14], PTSD [15–18], depression [19, 20], and inattention among military and veteran personnel [18]. Mindfulness meditation training has also been shown to increase emotion regulation [21] and emotional awareness [22]. A review of randomized controlled trials of mindfulness-based interventions delivered in the workplace reported small to large effect sizes (Hedge’s g = 0.32–0.77) supporting its’ effectiveness as an intervention for enhancing occupational wellbeing (e.g. reduced burnout and mental distress) [23].
Mindfulness meditation is offered to U.S. active duty military and U.S. Department of Defense civilians at various locations [24], however it is not offered as part of normal military training for all service members. One reason it is not offered to everyone is a lack of available qualified trainers, particularly in remote locations where military troops are stationed, and many veterans reside. Should teaching remotely prove to be beneficial, then such a delivery method might increase the number of service members and veterans who can learn and use mindfulness to their advantage.
Mindfulness meditation training follows a curriculum that can be adapted for remote delivery. Although different media may facilitate remote training (i.e., videoconferencing), there are distinct advantages to interactive social media as a delivery medium: (1) it allows real-time communications between participants, (2) it provides users with a more interactive experience than other online delivery modalities, and (3) avatar-based services can provide users anonymity, while preserving their ability to interact with others [25]. Research by Rice and Schroeder [25] found that participants who completed in-person delivery of a mindfulness training program reported greater satisfaction with the training and trust, as compared to participants who completed training remotely. However, both training groups demonstrated equivalent learning of mindfulness concepts. This finding suggests that, while offering training online is effective, additional research could provide valuable insight into the mechanisms of change that underly the benefits of participation.
Self-compassion
Although training in mindfulness concepts and practices provides an effective foundation for coping with stress, individual differences in perceptions of, and emotional responses to, negative experiences may color how that training is utilized when needed. A key aspect of military service (or any career that subjects one to hazards, risks, and trauma) is knowing that, when danger is present, you can count on your teammates. However, if a member is emotionally unable to deal with mistakes, their attention may drift from the present moment and put others at risk. Thus, implementing strategies aimed at resolving internal emotional conflicts that interfere with performance (as in mindfulness training) is an essential component of stress management.
Self-compassion involves regarding and behaving toward oneself with benevolence and kind understanding during and following hardship [26, 27]. Offering kind regard to oneself in difficult or life-threatening conditions allows one to see themselves and their situation realistically and without self-blame. That is, they can more easily identify possible methods to rectify situations, take action to solve problems, and prevent a future reoccurrence, without shame or self-recrimination [28]. In this way, self-compassion contributes to coping by enabling one to work through the impact of trauma on emotions and self-esteem.
Neff [26] posited that self-compassion comprises overlapping compassionate and uncompassionate elements (Table 1). Individuals who are self-compassionate respond to adversity with greater compassion and less uncompassion. For example, studies have shown scores on measures of depression, stress, and anxiety are negatively correlated with self-compassion scores and positively correlated with self-uncompassionate scores [29–32]. Although these outcomes support the compassionate/uncompassionate dichotomy, contradictory findings have been reported. In a study of problem drinkers, Brooks et al. [33] found measures of both compassion and uncompassion were positively correlated with depression, anxiety, and stress. This outcome may be due to how self-compassion is defined and measured [34, 35]. Despite conflicting research outcomes, the self-compassion construct is a useful framework for navigating the complex emotional processes associated with coping.
Three subcomponents of self-compassion, definitions, and corresponding uncompassionate subcomponents
Three subcomponents of self-compassion, definitions, and corresponding uncompassionate subcomponents
Mindfulness and self-compassion share conceptual roots in Eastern approaches to wellness [36, 37]. During mindfulness meditation, a person faces their own suffering. In so doing, they do not avoid or resist, instead they learn to acknowledge, and work with, their discomfort. Self-compassion exists in most every society. Therefore, it is reasonable to expect that changes in mindfulness may elicit changes in self-compassion and vice-versa.
Evidence for the effect of mindfulness training on self-compassion has been mixed. Whereas some studies have reported higher scores on measures of self-compassion following mindfulness training [38–40], others found no change in self-compassion following mindfulness training [41]. One explanation for these discrepancies is that mindfulness and self-compassion encompass different responses to life experiences. Whereas a mindful individual may respond non-judgmentally to painful experiences, and both a mindful and a self-compassionate individual may respond to painful experiences by accepting negative emotions, a self-compassionate individual may concurrently temper their response with self-kindness [36]. Thus, despite some conceptual and behavioral overlap, mindfulness and self-compassion appear to be independent constructs [37, 42] and, therefore, changes in self-compassion (or aspects of self-compassion) following mindfulness training (or changes in mindfulness or aspects of mindfulness following self-compassion training) are not necessarily inevitable.
The purposes of this study were to: 1) assess whether mindfulness meditation training has an impact on U.S. active duty and veteran service members’ dispositional self-compassion, and 2) examine whether the delivery mechanism for mindfulness (in-person versus virtual world) has an effect on self-reported dispositional self-compassion. Self-compassion was measured before and after receiving training in-person (IP) or in a Virtual World (VW), or when serving as a member of a wait-list control group (CG) at the same beginning and end points. The hypotheses were: Relative to participants assigned to the CG, participants assigned to the IP and VW groups will report greater improvements in post-training self-compassion. Also, both delivery methods (IP and VW) will be equally effective in enhancing self-compassion, with participants in the IP and VW groups showing higher pre/post change scores on the Self-Compassion Scale Total Averaged Score and subscales measuring compassionate traits, and lower scores on subscales measuring uncompassionate traits, compared with participants in the CG. Individuals at high risk (low initial positive self-compassion scores and subscores, as well as high initial negative self-compassion scores and subscores) will improve more than those at low risk (high initial positive self-compassion scores and subscores, as well as low initial negative self-compassion scores and subscores).
Materials and methods
Participants
There were 250 active duty and veteran U.S. Military service members who agreed to participate in the study. Participants were recruited from a military post and the surrounding catchment area. All volunteers agreed to participate and read and signed an informed consent form. All procedures were approved by a U.S. Army Institutional Review Board and were conducted in accord with the Declaration of Helsinki of 1964 and its later amendments.
Procedure
Figure 1 displays the recruitment and group assignment process. Participants were assigned to one of three groups: IP (n = 87), VW (n = 90), or CG (n = 73). While participants were encouraged to attend all training sessions, the data reported here focuses on participants who attended at least four of the nine scheduled sessions (8 weekly sessions plus one additional, 7 hour ‘silent retreat’ session during week five or six). 1 Mean (±SD) numbers of sessions attended (out of all nine sessions) were 4.6±3.0 (range 0 – 9) for the IP group and 4.2±3.3 (range 0 – 9) for the VW group. Accomplishing required military missions took priority over research group attendance, limiting the research volunteers availability at given times. Therefore, group assignment was non-random (e.g., That is, one group was filled and initiated, before filling a second group). Research volunteers did not know which group they were assigned to until just prior to the initiation of group training (the week before).
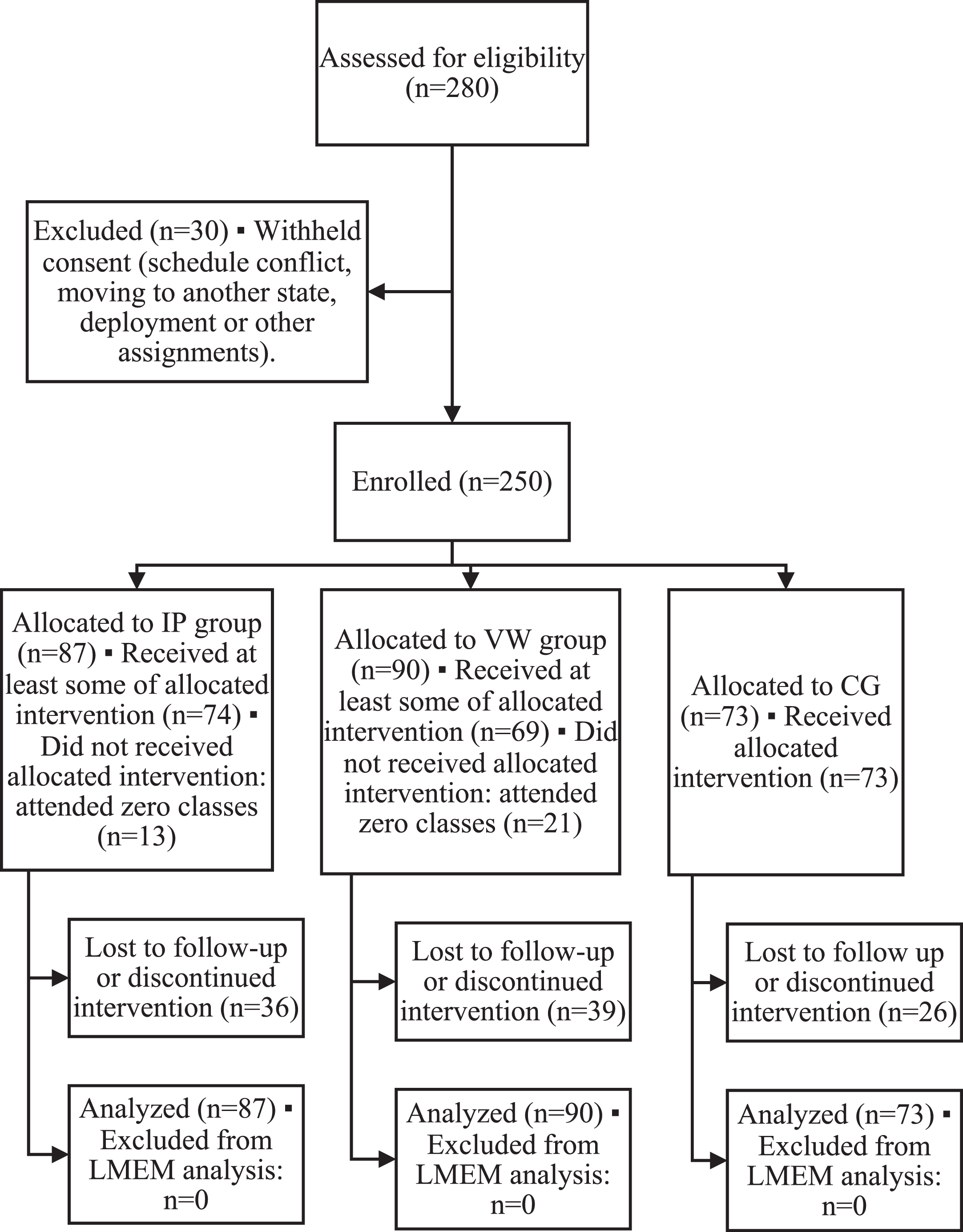
Consort flow diagram.
The IP group completed one 2 to 2½ hour session of MBSR training once a week for eight weeks. On approximately the sixth week of training, they completed a seven-hour silent retreat with their instructor and classmates (total in-person training hours = approximately 27 hours). In addition to class attendance, participants completed MBSR at-home practice assignments and kept a log of their weekly MBSR-related activities. Participants met on-post in rooms designated for this purpose, sitting in a circle facing one another.
The VW group completed one 1½ hour session of mindfulness training once a week for eight weeks through the virtual world of Second Life (secondlife.com). On the sixth week of training the VW group completed a 3½ hour silent retreat in Second Life with their instructor and classmates (total in-class time = 15 hours). Virtual world times were based on a pre-study survey of active duty and veteran service members, asking how long they would be willing to participate in an on-line class, in a series of instructional classes, and how long during a single day (silent retreat), they were willing to participate on-line. Participants were able to select and visually alter their avatars and were taught how to control and move their avatars. During class meetings, participants in the VW group saw the avatars of their instructor, classmates, and themselves in a gazebo, sitting in a circle. They could choose to use either a birds’ eye view or a direct view from the eyes of their avatar. As with the IP group, participants in the VW group completed at-home practice assignments and kept a log of their weekly MBSR-related activities. All handouts and assignments were identical for the intervention groups, as were the daily themes and topics.
Participants in the CG did not receive instruction in mindfulness but were permitted to attend a later mindfulness training class at their discretion. All participants completed the self-compassion measure twice: once prior to the intervention and once after completing mindfulness training (IP and VW groups) or nine weeks after the first assessment (CG).
Demographic questionnaire
This self-report measure included questions about volunteers’ demographics. The questionnaire included age, race/ethnicity, gender, education, marital status, military status, military branch, deployment (i.e., whether they had deployed or not), and time-in-service.
Self-compassion scale (SCS) [26]
The SCS is a 26-item self-report measure. Respondents rate their level of agreement with statements on a five-point Likert scale where 1 = almost never and 5 = almost always. Thirteen items measure compassion, as indexed by scores on three subscales: Self-Kindness, Common Humanity, and Mindfulness. Thirteen additional items measure uncompassion, as indexed by scores on three subscales: Self Judgement, Isolation, and Over-Identification. Scores on the six subscales were calculated as the mean of the subscale item responses. Total scores were calculated by reverse scoring the responses on the uncompassion subscale and then computing a grand mean of all six subscale means [26]. Higher scores indicate greater self-compassion for the total score and for scores on the subscales measuring compassionate traits. Lower scores indicate greater scores for the subscales measuring uncompassionate traits. The SCS has been shown to have both good reliability (alpha values between 0.80 and 0.93) [26] and convergent validity (r values between 0.70 and 0.77) [43].
Data analysis
Descriptive analyses were performed to summarize baseline attributes and self-compassion-related outcomes for participants in the three study groups before and after interventions.
Because some participants had missing data at the study endpoint for all outcomes, and because missing data were too numerous to use imputation methods, comparative inferential analyses were performed using linear mixed-effects models (LMEM). In those analyses, we constructed 2×3 factorial models for each outcome, with Time (pre- and post-training) as the within-subjects factor and Study Group (IP vs. VW vs. CG) as the between-subjects factor. The LMEM approach has the advantage of using observed data from every subject, regardless of missing data for variables measured repeatedly over time. Multiple LMEMs were created for each outcome, with each model exploring different possibilities for specifying fixed effects, random effects, interaction terms, and covariance matrix structures. We used the penalized likelihood method for optimal LMEM selection [44], choosing the model with the lowest Bayesian Information Criterion (BIC) magnitude. If more than one model had similarly low BIC values that were not significantly different using chi-square tests, the most parsimonious model with the fewest degrees of freedom was selected. LMEM analyses were adjusted for baseline age, gender, race, and education [45]. Post-hoc tests for multiple comparisons were performed using the least significant difference method [45].
As a second measure of effectiveness, we used the minimum clinically important difference (MCID). This amount is considered as the smallest amount of improvement considered meaningful by a patient. It is considered as a standard for determining the effectiveness of an intervention that includes patient satisfaction with that intervention. For this analysis, change scores were examined to understand the beneficial effects of mindfulness training on participants’ self-compassion. Change scores from baseline were computed with the formula: post-training mean minus (–) pre-training mean. Percent change scores from baseline were computed with the formula: (post-training mean - pre-training mean)/pre-training mean×100. Frequency counts and chi-square analyses were used to assess differences among groups in number of participants who achieved meaningful improvements. Because no minimally important differences have been established for these outcomes, we used >20% vs. <20% improvement from baseline, and also used >10% vs. <10% improvement from baseline to represent two possible thresholds for representing minimally important improvements [46].
Secondary analyses were conducted to see if improvements differed for participants with low vs. high baseline values for the outcome scales, adding baseline low/high status as an additional between-subjects factor in 2×2×3 LMEM analyses. The motivation for using this approach was to investigate the role of individual differences in interpreting the effect of mindfulness on self-compassion. Specifically, we were interested in whether those with more potential to benefit from training, would indeed do so. We formed low/high subgroups using median baseline scores for respective outcome variables.
After the initial analysis finding no difference between the two mindfulness training groups, the two mindfulness training groups were combined into an additional secondary analyses. This assessed outcomes for all participants receiving training compared to the CG with a 2×2 (group×time) factorial design.
SPSS Statistics software version 23 (IBM Corp., Armonk, NY, USA) was used for all analyses. The alpha level used for statistical significance was 0.05; corresponding 95% confidence intervals were computed.
Results
Analyses of demographic data
Study participants ranged in age from 24 to 74 years with a mean of 48.00±12.10 years; 46.0% were female. Self-reported ethnicity was: Caucasian (53.7%), African American (25.4%), Hispanic (17.2%), Asian (2.0%), and Native American (1.6%). Most (71.3%) had earned a college degree; 23.1% had some college experience but no degree; 5.7% attained a high school diploma or GED certificate. Most participants (61.8%) were married or living with a partner.
Most participants were veterans (65.3%), but there were also active duty service members (31.4%), Reserves (2.0%), and National Guard (1.2%). Services represented were Army (58.5%), Air Force (24.1%), Navy (11.3%), and Coast Guard (0.5%). The average time-in-service was 15.20 years (±8.73). Just over half of the participants served on prior military deployments (55.6%).
Analysis of the total averaged score on the SCS
As shown in Fig. 1 and Table 2, there was a significant Group×Time interaction, F (2, 145) = 5.90, p < 0.01. The mean SCS Total Averaged Score increased (improved) from pre- to post-training by approximately 10% from baseline scores in the training groups, while the CG experienced little to no change in mean scores over the course of the study.
Means, standard deviations, 95% confidence intervals, and p-vales for pre- and post- training total and subscale scores on the SCS among the three groups
Means, standard deviations, 95% confidence intervals, and p-vales for pre- and post- training total and subscale scores on the SCS among the three groups
Note. **p < 0.01, *p < 0.05. IP = in-person, VW = virtual world. †Adjusted for age, gender, race, and education.
Post-hoc testing revealed significant improvements for the training groups, p < 0.01, but not for the CG, p = 0.76, and change scores in both training groups that were significantly higher than that in the CG, p < 0.01. However, there was no statistical significance for the difference in mean change scores comparing the IP group to the VW group, p = 0.83.
Proportions of participants with >20% improvements (higher SCS Total Averaged Score) post-training compared to pre-training were significantly better in the training groups when compared to the CG: 27.5% in the IP group; 32.6% in the VW group; 7.0% in the CG, χ2(2) = 9.12, p = 0.01. Likewise, proportions of participants with >10% improvements were significantly different among study groups: 47.1% in the IP group; 51.2% in the VW group; 25.6% in the CG, χ2 (2) = 6.79, p = 0.03.
The median pre-training value for SCS Total Averaged Score was 2.99; participants with scores <2.99 at baseline were classified in the low initial score subgroup. There were differential directions and magnitudes of change in the two subgroups, as reflected in the significant low-high subgroup×time interaction effect, F (1, 137) = 13.17, p < 0.01. In the low initial score subgroup, mean scores in all study groups increased (improved) by relatively larger amounts compared to the high initial score subgroup, where mean scores changed relatively little – increasing by small amounts in the training groups and decreasing by a small amount in the CG. The non-significant 3-way interaction effect, F (2, 137) = 0.07, p = 0.93, revealed the interaction of low-high subgroup and time did not depend on other factors in the design.
Post-hoc testing revealed significant changes in mean score over time for both training groups, p < 0.01 among participants with low initial scores, but only in the IP group among participants with high initial scores, p = 0.04. There were no statistical between-group differences in mean change scores in the subgroup with low initial scores, p > 0.12, but the difference in mean change score for the IP group compared to the CG was statistically significant in the subgroup with high initial scores, p = 0.04.
Analysis of subscale scores on the SCS
Self-kindness subscale
Mean scores for the Self-Kindness Subscale of the SCS increased (improved) from pre- to post-training by approximately 10% of baseline scores in the training groups compared to the CG, which experienced little to no change in scores over the course of the study (Table 2). As shown in Fig. 2, the improvements in the training groups relative to little change in the CG yielded a statistically significant group×time interaction effect, F (2, 161) = 3.17, p = 0.04.

Self-Compassion Scale Total Averaged Score: mean scores by group before and after training using estimated marginal means from the 2×3 linear mixed-effects model.
Post-hoc testing revealed significant improvements for the training groups, p < 0.01, but not for the CG, p = 0.70, and change scores in both training groups that were significantly better than that in the CG, p = 0.03. There was no statistical significance for the difference in mean change scores comparing the IP group to the VW group, p = 0.95.
Proportions of participants with >20% improvements (higher Self-Kindness Subscale scores) post-training compared to pre-training were not significantly different among study groups: 35.3% in the IP group; 34.9% in the VW group; 16.3% in the CG, χ2 (2) = 5.06, p = 0.08. Likewise, proportions of participants with >10% improvements were not significantly different among study groups: 49.0% in the IP group; 46.5% in the VW group; 34.9% in the CG, χ2 (2) = 2.08, p = 0.35.
3.2.1.1. Self-kindness subscale with low vs. high baseline scores. The median pre-training value for Self-Kindness Subscale was 2.80; participants with scores <2.80 at baseline were classified in the low initial score subgroup. There were differential directions and magnitudes of change in the two subgroups, as reflected in the significant low-high subgroup×time interaction effect, F (1, 139) = 14.82, p < 0.01. In the low initial score subgroup, mean scores in all study groups increased (improved) by relatively larger amounts compared to the high initial score subgroup, where mean scores changed relatively little – increasing by a small amount in the IP group, remaining essentially unchanged in the VW group, and decreasing in the CG. The non-significant 3-way interaction effect, F (2, 139) = 0.39, p = 0.68, revealed that the interaction of low-high subgroup and time did not depend on other factors in the design.
Post-hoc testing revealed a significant change in mean score over time only for the two training groups, p < 0.01, among participants with low initial scores, but decreasing significantly only in the CG among participants with high initial scores, p = 0.04. There were no statistically significant between-group differences in mean change scores in the subgroup with low initial scores, p > 0.44, or in the subgroup with high initial scores, p > 0.07.
As seen in Fig. 3, the mean Common Humanity Subscale of the SCS increased (improved) from pre- to post-training in the training groups and remained essentially unchanged in the CG. However, these differences among groups over time were not quite large enough to yield a significant group×time interaction effect, F (2, 164) = 2.52, p = 0.08. There was a significant main effect for time, F (1, 165) = 13.27, p < 0.01, reflecting a general improvement in mean scores over time. The main effect of group was not significant, F (2, 261) = 1.92, p = 0.15.
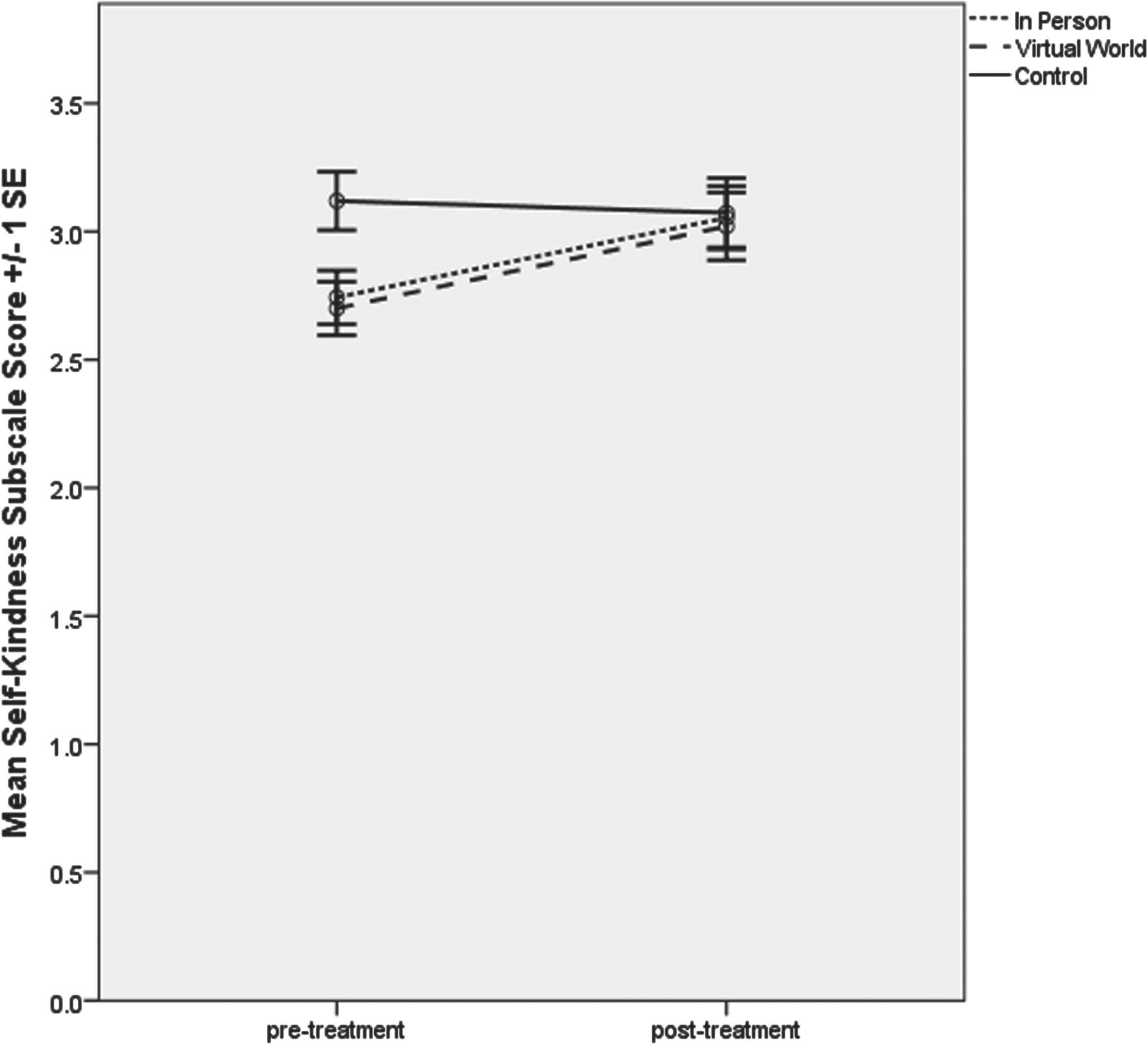
Self-Kindness Subscale of the Self-Compassion Scale: mean scores by group before and after training using estimated marginal means from the 2×3 linear mixed-effects model.
Proportions of participants with >20% improvements (higher Common Humanity Subscale scores) post-training compared to pre-training were not significantly different among study groups: 37.3% in the IP group; 41.9% in the VW group; 30.2% in the CG, χ2(2) = 1.27, p = 0.53. Likewise, proportions of participants with >10% improvements were not significantly different among study groups: 49.0% in the IP group; 53.5% in the VW group; 46.5% in the CG, χ2(2) = 0.43, p = 0.81.
3.2.2.1. Common humanity subscale with low vs. high baseline scores. The median pre-training value for Common Humanity Subscale was 3.00; participants with scores <3.00 at baseline were classified in the low initial score subgroup. There were differential directions and magnitudes of change in the two subgroups, as reflected in the significant low-high subgroup×time interaction effect, F (1, 136) = 18.31, p < 0.01. In the low initial score subgroup, mean scores in all study groups increased (improved) by relatively larger amounts compared to the high initial score subgroup, where mean scores increased by a small amount in the IP group, remained relatively unchanged in the VW group, and decreased by a somewhat larger amount in the CG. The non-significant 3-way interaction effect, F (2, 136) = 0.32, p = 0.73, revealed that the interaction of low-high subgroup and time did not depend on other factors in the design.
Post-hoc testing with the LMEM analysis revealed significant improvements in mean scores over time for all study groups among participants with low initial scores, p < 0.02, but a significant change (a decrease) only for the CG among participants with high initial scores, p = 0.05. There were no statistically significant between-group differences in mean change scores in either subgroup, p > 0.08.
Mean scores for the Mindfulness Subscale of the SCS increased (improved) from pre- to post-training in the two training groups by varying amounts and decreased by a smaller amount in the CG. As shown in Fig. 4, there was a significant Group×Time interaction, F (2, 157) = 3.85, p = 0.02.
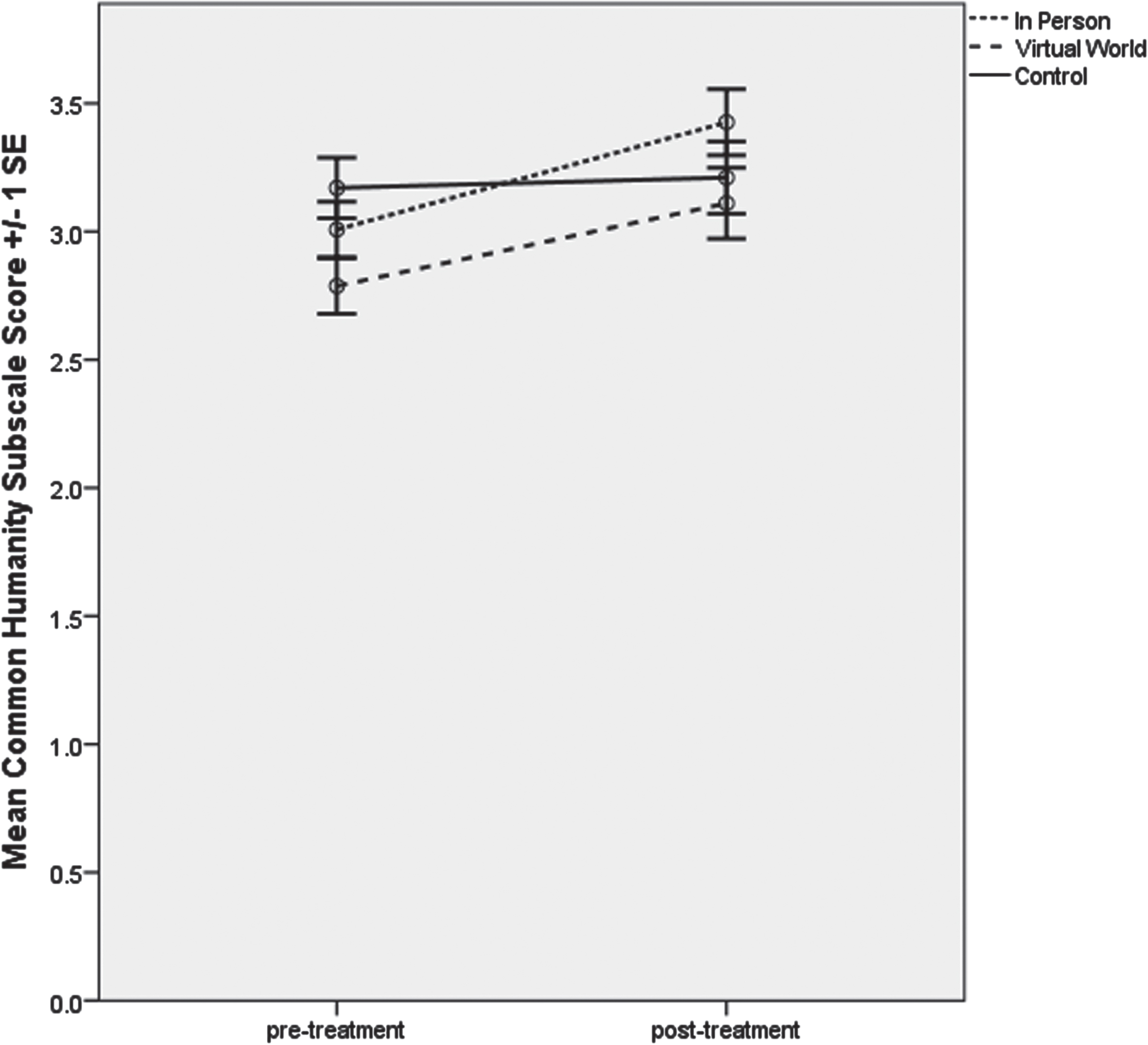
Common Humanity Subscale of the Self-Compassion Scale: mean scores by group before and after training using estimated marginal means from the 2×3 linear mixed-effects model.
Post-hoc testing revealed significant improvement in the IP group only, p < 0.01, and a significant difference in mean change scores only when comparing the IP group to the CG, p < 0.01.
Proportions of participants with >20% improvements (higher Mindfulness Subscale scores) post-training compared to pre-training were not significantly different among study groups: 31.9% in the IP group; 27.5% in the VW group; 16.3% in the CG, χ2 (2) = 3.04, p = 0.22. Likewise, proportions of participants with >10% improvements were not significantly different among study groups: 46.8% in the IP group; 30.0% in the VW group; 27.9% in the CG, χ2(2) = 4.24, p = 0.12.
3.2.3.1. Mindfulness subscale with low vs. high baseline scores. The median pre-training value for Mindfulness Subscale was 3.25; participants with scores <3.25 at baseline were classified in the low initial score subgroup. There were differential directions and magnitudes of change in the two subgroups, as reflected in the significant low-high subgroup×time interaction effect, F (1, 138) = 19.55, p < 0.01. In the low initial score subgroup, mean scores in all study groups increased (improved) by varying amounts, but by the smallest amount in the CG. In the high initial score subgroup, mean scores changed relatively little in the training groups but decreased in the CG. There were also differential changes over time among study groups, with the CG scoring worse over time than the training groups regardless of subgroup. The non-significant 3-way interaction effect, F (2, 138) = 0.37, p = 0.69, revealed that the interaction of low-high subgroup and time did not depend on other factors in the design.
Post-hoc testing revealed a significant change in mean score over time for both training groups, p < 0.03, among participants with low initial scores, but only in the CG among participants with high initial scores, p = 0.01. There were no statistically significant between-group differences in mean change scores in the subgroup with low initial scores, p > 0.09, or in the subgroup with high initial scores, p > 0.07.
For all groups, post-training Self-Judgement subscale scores were significantly lower (improved) than pre-training scores, resulting in a significant main effect of time, F (1, 152) = 21.48, p < 0.01. The Group×Time interaction was not statistically significant, F (2, 152) = 2.35, p = 0.10 (Fig. 5).

Mindfulness Subscale of the Self-Compassion Scale: mean scores by group before and after training using estimated marginal means from the 2×3 linear mixed-effects model.
Proportions of participants with >20% improvements (lower Self-Judgement Subscale scores) post-training compared to pre-training were not significantly different among study groups: 31.4% in the IP group; 34.9% in the VW group; 30.2% in the CG, χ2 (2) = 0.23, p = 0.89. Likewise, proportions of participants with >10% improvements were not significantly different among study groups: 54.9% in the IP group; 51.2% in the VW group; 37.2% in the CG, χ2 (2) = 3.15, p = 0.21.
3.2.4.1. Self-judgement subscale with low vs. high baseline scores. The median pre-training value for Self-Judgement Subscale was 3.20; participants with scores <3.20 at baseline were classified in the low initial score subgroup. There were differential directions and magnitudes of change in the two subgroups, as reflected in the significant low-high subgroup×time interaction effect, F (1, 135) = 35.39, p < 0.01. In the high initial score subgroup, mean scores in all study groups decreased (improved) by relatively larger amounts compared to the low initial score subgroup, where mean scores changed relatively little. The LMEM analysis yielded a significant low-high subgroup×time interaction effect. The non-significant 3-way interaction effect, F (2, 135) = 0.48, p = 0.62, revealed that the interaction of low-high subgroup and time did not depend on other factors in the design.
Post-hoc testing revealed a significant improvements (reductions) in mean score over time for all study groups, p < 0.01, among participants with high initial scores, but in none of the study groups among participants with low initial scores, p > 0.41. There were no statistically significant between-group differences in mean change scores in the subgroup with low initial scores, p > 0.41, or in the subgroup with high initial scores, p > 0.11.
The mean Isolation Subscale of the SCS decreased (improved) from pre- to post-training in the training groups compared to the CG, which experienced a relatively small change in scores over the course of the study (Fig. 6). In the LMEM analysis, these improvements in the training groups relative to little change in the CG were not large enough to yield a statistically significant group×time interaction effect, F (2, 149) = 1.77, p = 0.17. However, the model did yield significant main effects for study group, F (2, 253) = 5.18, p = 0.01 and time, F (1, 149) = 12.22, p < 0.01.
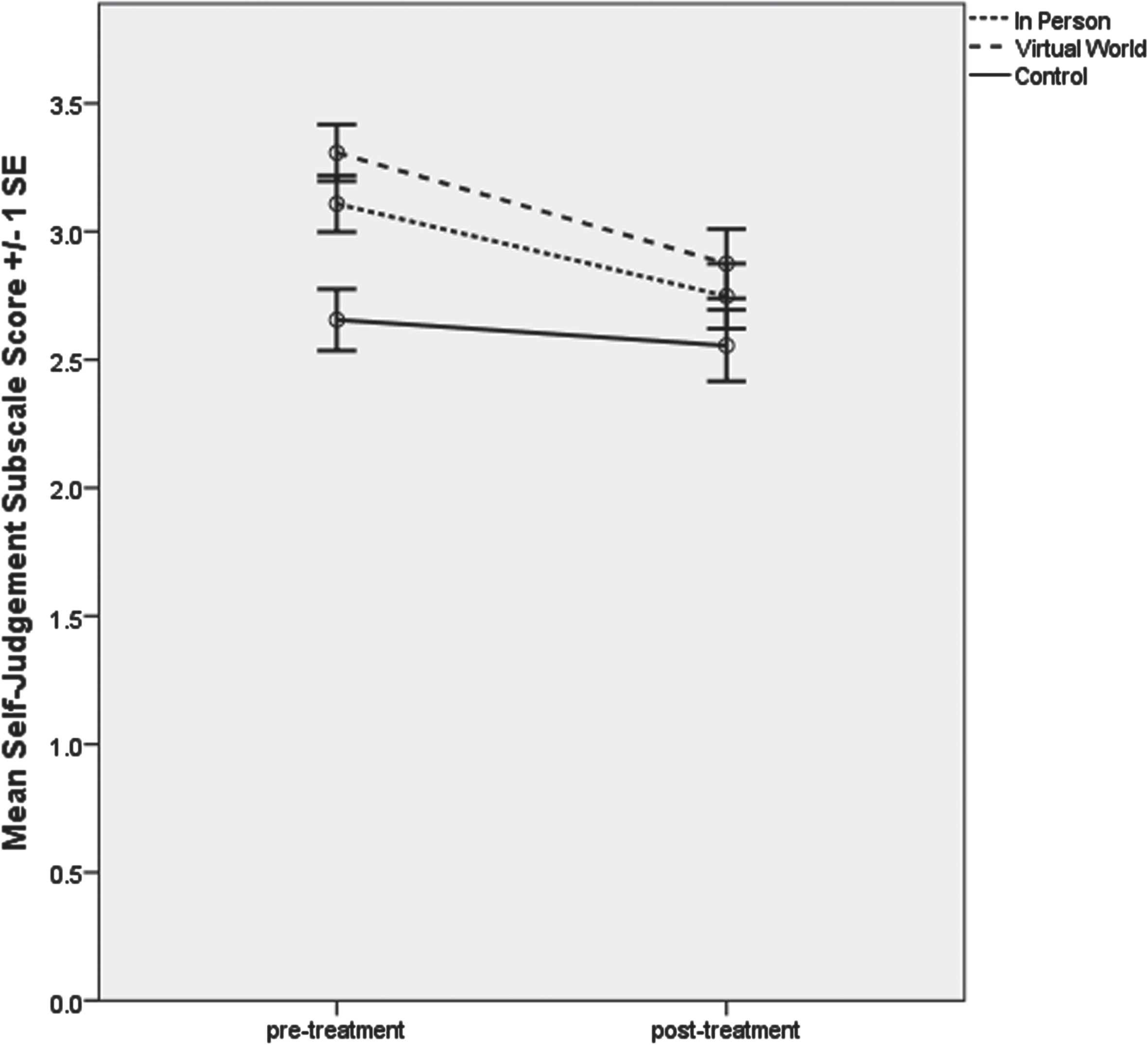
Self-Judgement Subscale of the Self-Compassion Scale: mean scores by group before and after training using estimated marginal means from the 2×3 linear mixed-effects model.
Proportions of participants with >20% improvements (lower Isolation Subscale scores) post-training compared to pre-training were not significantly different among study groups: 31.4% in the IP group; 37.2% in the VW group; 16.3% in the CG, χ2 (2) = 4.96, p = 0.08. Likewise, proportions of participants with >10% improvements were not significantly different among study groups: 51.0% in the IP group; 48.8% in the VW group; 39.5% in the CG, χ2 (2) = 1.34, p = 0.51.
3.2.5.1. Isolation subscale with low vs. high baseline scores. The median pre-training value for Isolation Subscale was 3.00; participants with scores <3.00 at baseline were classified in the low initial score subgroup. There were differential directions and magnitudes of change in the two subgroups, as reflected in the significant low-high subgroup×time interaction effect, F (1, 135) = 34.60, p < 0.01. In the high initial score subgroup, mean scores in all study groups decreased (improved), whereas mean scores changed relatively little in the subgroup with low initial scores (p > 0.08). The non-significant 3-way interaction effect, F (2, 135) = 2.47, p = 0.09, revealed that the interaction of low-high subgroup and time did not depend on other factors in the design.
As shown in Fig. 7, mean scores for the Over-Identification Subscale of the SCS decreased (improved) from pre- to post-training in the training groups by larger amounts compared to the CG, which experienced only a small reduction in mean score over the course of the study. These improvements in the training groups (relative to little change in the CG) yielded a significant group×time interaction effect, F (2, 147) = 3.53, p = 0.03
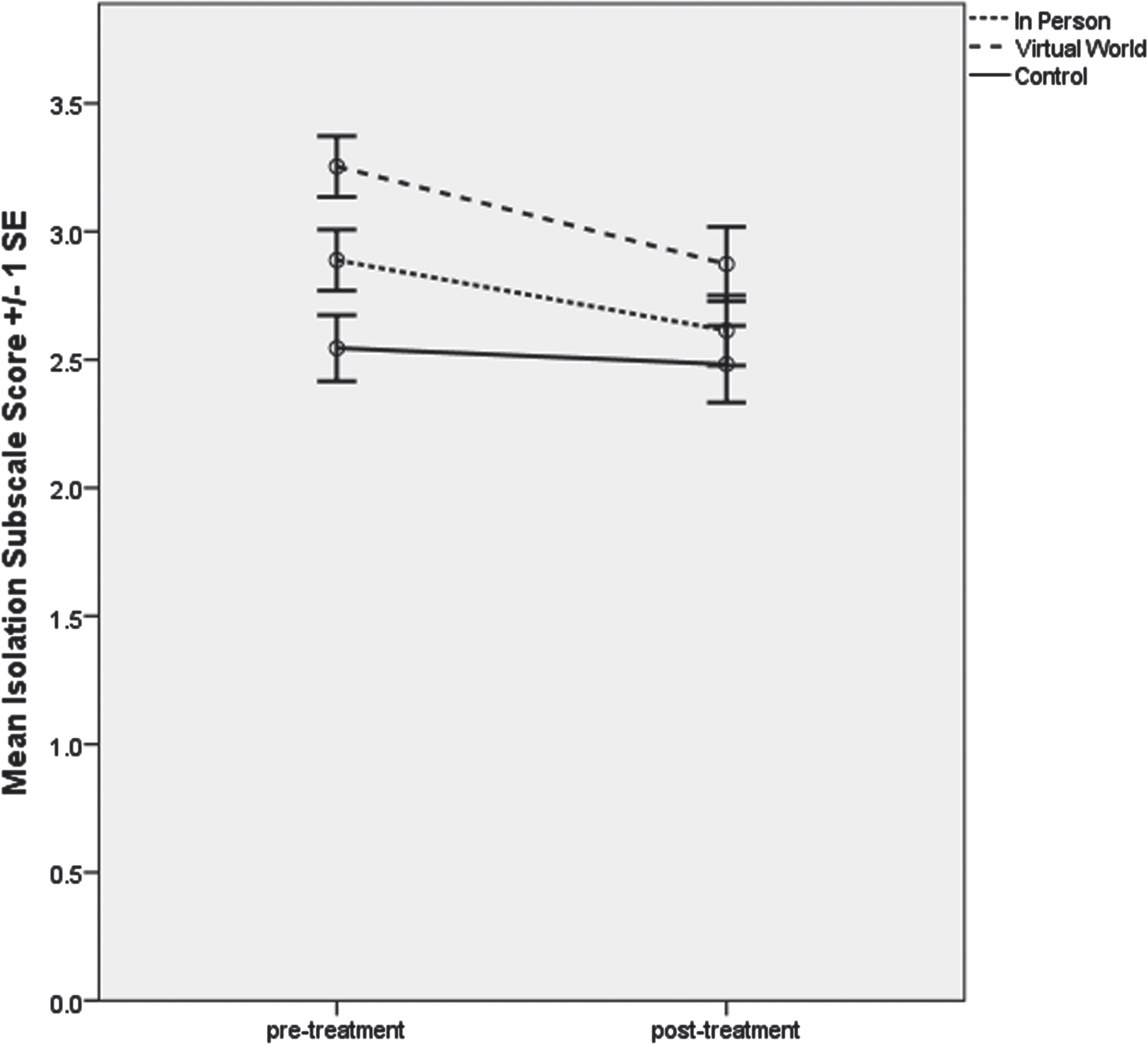
Isolation Subscale of the Self-Compassion Scale: mean scores by group before and after training using estimated marginal means from the 2×3 linear mixed-effects model.
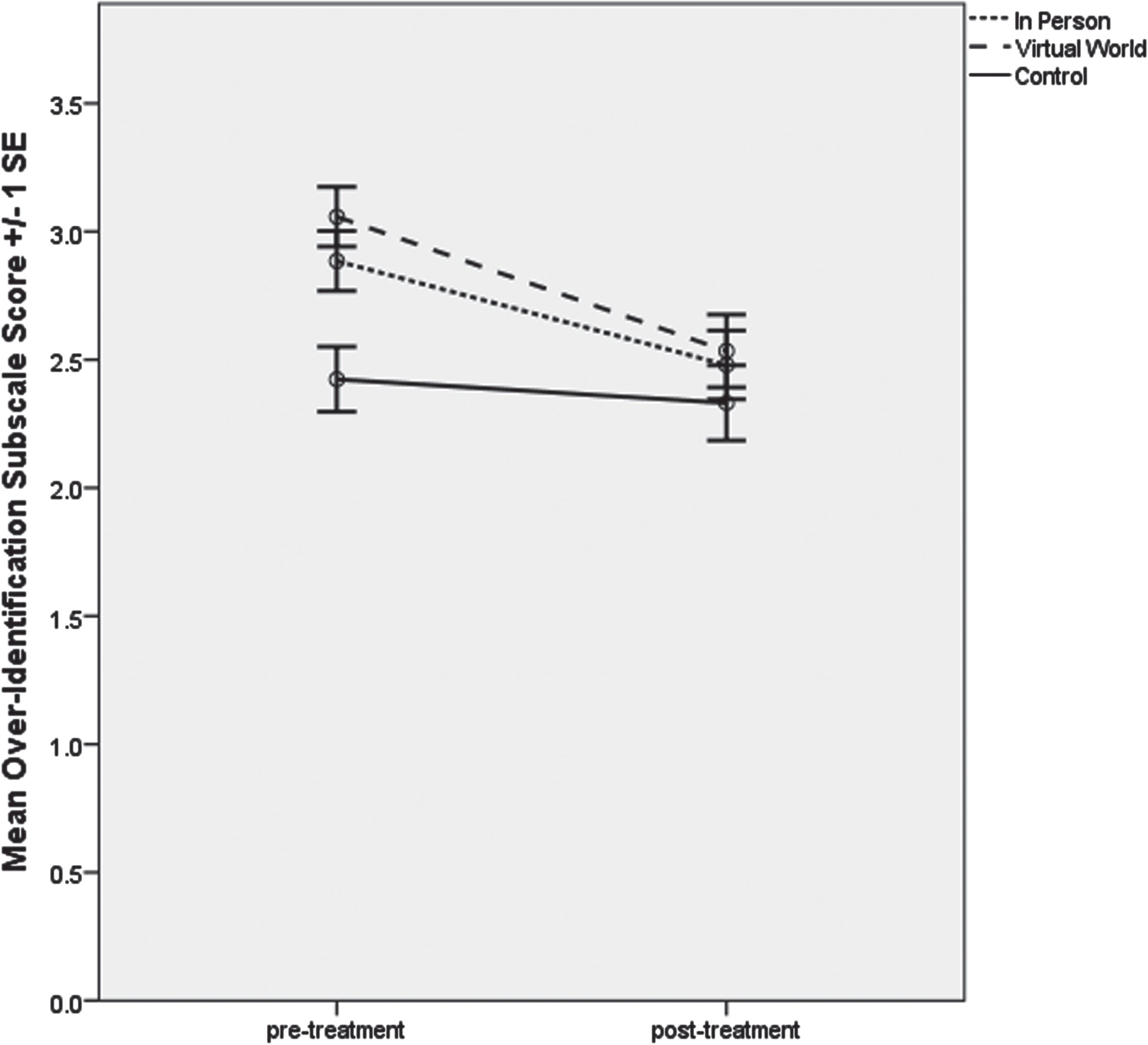
Over-Identification Subscale of the Self-Compassion Scale: mean scores by group before and after training using estimated marginal means from the 2×3 linear mixed-effects model.
Proportions of participants with >20% improvements (lower Over-Identification Subscale scores) post-training compared to pre-training were not significantly different among study groups: 38.0% in the IP group; 34.9% in the VW group; 20.9% in the CG, χ2 (2) = 3.43, p = 0.18. Likewise, proportions of participants with >10% improvements were not significantly different among study groups: 52.0% in the IP group; 48.8% in the VW group; 34.9% in the CG, χ2 (2) = 3.00, p = 0.22.
3.2.6.1. Over-identification subscale with low vs. high baseline scores. The median pre-training value for Over-Identification Subscale was 3.00; participants with scores <3.00 at baseline were classified in the low initial score subgroup. There were differential directions and magnitudes of change in the two subgroups, as reflected in the significant low-high subgroup×time interaction effect, F (1, 139) = 28.21, p < 0.01. In the high initial score subgroup, mean scores in the two training groups decreased (improved) by relatively larger amounts compared to the CG, where the mean score decreased by a smaller amount. In the low initial score subgroup, mean scores changed relatively little. The non-significant 3-way interaction effect, F (2, 139) = 2.79, p = 0.06, revealed that the interaction of low-high subgroup and time did not depend on other factors in the design.
Post-hoc testing revealed a significant change in mean score over time only for the two training groups among participants with high initial scores, p < 0.01. There were statistically significant between-group differences in mean change scores comparing both training groups to the CG, but only in the subgroup with high initial scores, p < 0.02.
Relative to the CG, participants in the IP and VW groups demonstrated significant pre/post training improvements in Total Average Scores on the SCS, Self-Kindness, and Over-Identification, resulting in significant Group×Time Interactions. Relative to the CG, participants in the IP group demonstrated significant improvement in Mindfulness, which also resulted in a significant Group×Time interaction. No other significant group×time results were found.
The MCID analyses extended the findings of the primary analyses. For the total average SCS, both training groups showed a 20% and a 10% improvement from baseline, and both were significantly different from the CG.
Analyses of participants with low and high baseline scores showed the following significant changes: Total SCS: Those with low initial scores improved more than those with high initial scores, and the IP group with high scores improved more than the CG with high initial scores. Both training groups with low initial scores improved significantly more than the CG in subgroups Self-Kindness and Mindfulness. Subgroups with high initial scores that decreased (worsened over time) included the CG for Self-Kindness, Common Humanity, and Mindfulness.
Discussion
Impact of mindfulness training on self-compassion
The primary objective of this study was to examine the impact of Mindfulness Training on Self Compassion as measured by the SCS. The research results support the hypothesis that mindfulness-meditation training will increase self-compassion. This was shown in improvements in the total average SCS for both mindfulness training groups, but not the CG. In addition, the hypothesis is supported in the improvements in the Self-Kindness subscale, and the improvement (decreased score) in the uncompassion subscale of Over-Identification, while the CG did not. The IP group improved significantly on the Mindfulness subscale compared with the CG, but the IP group was not different from the VW group. No significant differences were seen between the IP and VW training groups, thus demonstrating that both were equally effective at improving self-compassion.
Overall, the results of the current study paint a complex picture of the relationship between mindfulness and self-compassion. In some cases, post-training shifts in one component of self-compassion (e.g., Mindfulness) occurred in tandem with post-training shifts in another (e.g., Over-Identification). This pattern agrees with Neff’s framework [26]. Yet, in other cases, changes in one element (e.g., Self-Kindness) were independent of changes in its correspondent (Self-Judgement). Taken collectively, these findings suggest that the impact of mindfulness training on self-compassion is not cumulative. Post-training changes may depend on the delivery modality and structure of the training, sample-specific factors, and other variables.
Mindfulness and Over-Identification subscales fall on the same continuum, with mindfulness being equated with a larger, non-judgmental experience of compassion when we make mistakes, while over-identification leaves us in the midst of our errors. Individuals who over-identify, tend to over-identify with their own problems, suffering, thoughts, and emotions. At times this identification with their negative issues is emphasized over all other life circumstances, making them less capable of adapting to life challenges. In this study, over-identification decreased in the training groups, thus helping participants to be more adaptable, positive, and able to move on to consequent life demands.
Self-Kindness falls on the same continuum as Self-Judgement. The improvements seen in both mindfulness training groups equates with a greater understanding that we, as individuals, are not perfect. Instead of harshly criticizing ourselves through put-downs, reproaches, and denigrations, higher self-kindness is associated with recognition that we are fallible, but not a failure; that we suffer, yet we can take steps to overcome; and that self-encouragement yields more than self-flagellation. Self-kindness leads to greater emotional self-control. Self-Kindness significantly improved among the training groups, but not Self-Judgement, Common Humanity or Isolation.
While it is tempting to speculate that demographics might have contributed unobserved variance to the findings of this study, recall that the LMEM analyses controlled for age, gender, race, and education effects. A more likely explanation for the outcomes is the lack of explicit instruction in all subcomponents of self-compassion in mindfulness training [37]. Stated differently, the inclusion of specific instruction in self-compassion in the mindfulness training classes might have yielded a more consistent impact on pre- to post-changes in self-compassion. It appears the daily themes and topic areas led to greater introspection in how participating active duty and veteran service members take care of themselves (Self-Kindness) and how often they are fully present in their daily lives (Mindfulness); but not specifically on how they collectively viewed themselves and others (Common Humanity and Isolation). This is particularly interesting, as military professionals may see self-kindness as weakness and the ability to “Soldier Through” as a strength.
As Self-Kindness and Self-Judgement are on the same scale, improvements in Self-Judgement might have been expected. The non-significant changes in post-training scores on the Self-Judgement subscale may reflect the culture of the military which emphasizes stoicism, emotional control, non-acceptance of failure (invulnerability) [47], and acceptance of personal accountability for both self and all those whom a leader supervises (including failures). In addition, todays’ U.S. military services place mission accomplishment above all else, with an emphasis on discipline, acceptance of legitimate authority, and self-less service. This cultural perspective may induce trepidation in terms of self-compassion, especially for those whose self-motivation included harsh self-judgement or the belief that compassion is tantamount to weakness [48]. This may be true as well, for those whose external incentives from parents, teachers, or supervisors has involved reproach and reprimand. Self-critical thoughts impede present-moment awareness and interfere with decision-making processes.
These findings support prior outcomes in which emotional stability [49, 50] and resilience [51, 52] were associated with mindfulness, mindfulness training, self-compassion and self-compassion training. One possibility is that individuals who are high in mindfulness and self-compassion are more at ease with cognitively restructuring stressful situations as compared with those who are low in self-compassion [52, 51]. Positive reframing is similar to cognitive restructuring in that calamitous consequences are subsequently viewed as growth producing, and positive reframing has been found predictive of successful coping among active duty service members [53]. Interventions that offer strategies for reframing stress could enhance workplace wellness.
Thresholds for minimum clinically important difference on the SCS
To our knowledge this was the first study to examine changes over time dichotomized by cutoff scores to represent potential thresholds for minimally important improvements pertaining to the effect of mindfulness meditation instruction on self-compassion. For the total averaged SCS, proportions of participants with improvements meeting or exceeding both thresholds (20% and 10% change) were greater in both training groups than in the CG, and these differences among groups were statistically significant. The same pattern of higher proportions of participants in the training groups attaining either threshold held true for subscale analyses, although the differences among groups were not statistically significant for the subscales. It should be noted that, although these findings are consistent with prior research that assessed MCIDs in psychological health following in-person mindfulness training [46] and remote mindfulness training [61], further research to establish appropriate thresholds discriminating trivial improvements from meaningful or important thresholds is warranted, given that such thresholds have proven extremely useful in clinical research [62, 63].
Impact of delivery modality on outcomes
A second objective was to examine the effect of mindfulness training offered in person and in a virtual world on self-compassion outcomes. The findings demonstrated both the IP and VW groups showed improvement, with no significant difference between them, but with differences shown between their combined scores and the CG, consistent with the outcomes from prior studies [38, 54]. This finding supports the effectiveness of both IP and VW remote delivery of mindfulness training.
Prior research has shown improvements in psychological health following mindfulness training delivered remotely [55–60]. The findings reported here contribute to the literature as the first study to examine and compare virtual world mindfulness training with in-person mindfulness training, finding both effective for increasing self-compassion. Moreover, these findings indicate that an abbreviated version of mindfulness training can be offered in a VW real time remote delivery, achieving the same level of improvements in total self-compassion as in-person training. This finding is true also for improvements in the subscales of Self-Kindness, Mindfulness, and Over-Identification.
In our current world situation, contingency plans for replacing one-on-one workplace interactions has begun. Enabled by digital tools and collaboration applications, and invigorated by the stay-in-place requirements recently dictated by the international presence of Corona Virus – 19, remote methods of influencing resilience and mental health are imperative. The VW training was twelve hours shorter than the in-person training in this study. Offering training programs with shorter time commitments than traditional mindfulness training programs could boost participant retention [68]. Also, VW training can be offered in locations in which a trained professional is not physically available, thus reducing time and increasing availability. This option may be attractive for budget-constrained organizations [69]. The one case in which VW may not be indicated is for use with individuals who have comorbidities that include social isolation such as PTSD, or loneliness such as with depression and anxiety [70]. However, additional research is needed to corroborate these findings.
Comparison of scores between participants scoring low vs. high on the initial SCS
Also contributing to the body of knowledge on mindfulness training and self-compassion, this is the first study to systematically examine the effect of mindfulness meditation training on self-compassion by comparing participants that scored low and high on the SCS at baseline. The main finding from the comparative analyses stratified by groups with low and high baseline scores is that at post-training assessment, individuals with low initial total self-compassion scores reported increased compassion and individuals with high initial uncompassion scores reported decreased uncompassion following IP and VW mindfulness training. This suggests that participants at risk, that is those with lowest compassion and highest uncompassion, have the most to gain from mindfulness training, supporting findings in which patient populations show advances in compassion [38, 64]. One exception occurred in which the high initial score group also improved for the IP group in Mindfulness.
This same pattern was found in the outcomes of the SCS compassion subscales when stratified by low vs. high initial scores. For the Self-Kindness, Mindfulness, and Over-Identification subscales, the two mindfulness groups improved significantly in the at-risk groups (positive self-compassion with low initial scores and negative self-compassion with high initial scores), compared to the CG. Although not significant, improvements of larger magnitude were seen in the at-risk groups, where even the CG showed improvements, albeit smaller improvements than in the training groups in Common Humanity and Self-Judgement. Two exceptions were seen, in which the CG group with high initial scores in Common Humanity and Mindfulness scored worse over time compared with the CG. These findings are logical and pass the “common sense” test, yet they are important as at-risk scores can serve as a screening tool for those who might benefit the most from training, possibly indicating that training to improve successful coping is not a “one size fits all”. That at-risk individuals showed improvement in scores on the compassion subscales following mindfulness training suggests that, even in the absence of explicit instruction in self-compassion, mindfulness training improves self-compassion.
The IP findings on the SCS total score and Mindfulness subscale may reflect our earlier findings in which individuals with symptoms of PTSD being more likely to select VW training, but less likely to complete on-line, virtual world mindfulness training [65]. This may reflect VW training as reinforcing the social isolation already prevalent among those with PTSD [66].
As previously discussed, prior research [67] has shown uncompassion as negatively associated with facets of trait mindfulness (acting with awareness and non-judgement of inner experience). One possibility is that for participants with high uncompassion baseline scores, the mindfulness training elevated facets of mindfulness associated with compassion (non-reactivity, observing inner experience, and describing inner experience), which prompted elevations in compassion at post-testing. Future research could examine this possibility in greater detail.
Another possibility is that increasing mindfulness reduces barriers to self-compassion [71]. For example, coping techniques learned during mindfulness training may enhance one’s preparedness to confront difficult emotions associated with traumatic experiences. Other mind-body interventions, such as Mindful Self-Compassion [71], offer instruction in techniques (e.g., “soften-soothe-allow”) that are designed to help participants navigate complex emotions (e.g., shame) while working towards self-compassion. Participation in a self compassion-focused intervention is associated with improvements in military veterans’ psychological well-being [68, 69]. Whatever the reason may be for shifts in compassion scores, this research sheds further light on the relationship between self-compassion and mindfulness.
Conclusions
Mindfulness meditation is an effective intervention for reducing stress and enhancing psychological wellness. In the current study, participation in either in-person or virtual mindfulness training yielded similar results and both modalities were more effective than a CG in increasing self-compassion. One implication of the results is that mindfulness meditation training could be offered to employees who work on site or remotely. Another finding was that individuals who were considered at-risk benefited to a greater extent than those considered not at risk. This suggests that employees in high-stress occupations could benefit from the strategies and techniques that are taught in mindfulness-meditation training, in terms of self- care, forgiveness, and understanding. Such improvements may increase personal flexibility and resilience.
Self-compassion, an important component of emotional resilience, was elevated after participation in our mindfulness meditation training. This outcome suggests that in addition to reducing stress, participation in mindfulness meditation training enhances other aspects of psychological health. Individuals who are emotionally resilient can self-regulate emotions and reduce the negative impact of self-criticism and rumination. In addition, emotional resilience increases work productivity and personal feelings of self-worth and psychological well-being. Thus, a second implication of the results is that while some people come by self-compassion naturally, others must learn it. Luckily, it is a learnable skill through Mindfulness meditation training or Self-Compassion training.
Several suggestions are offered: The results suggest that mindfulness meditation be offered to active duty service members as a part of their resilience training. This will encourage service members to adopt a larger perspective, a willingness to view personal experiences realistically without being caught in negative reactivity, and a sense of personal emotional composure, level-headedness, and control. Mindfulness meditation training may also be beneficial for civilian employees of the military services, contract personnel, and other individuals in high-stress, high- demand jobs. Clinical practice guidelines might include Mindfulness training as a viable intervention tool. Establishing Thresholds for Minimum Clinically Important Differences for Self-Compassion would be a worthwhile endeavor within psychological services. Leveraging technology to deliver wellness interventions reduces barriers to care that many people experience, including military personnel. The present study supports virtual worlds as a viable platform for delivering mindfulness training. Other platforms (e.g., mobile health (mHealth) applications) offer promising possibilities, but more research is needed to effectively develop, package, and market solutions.
Finally, as we know, research begats research, raising new questions and considerations. While the findings from the current study build on prior work by demonstrating the viability of mindfulness training for increasing self-compassion, more research about the relationship between mindfulness and self-compassion is warranted.
Limitations
Two limitations of this study include the subject pool being restricted to U.S. active duty military and veterans and group versus individual randomization. Also, although both the IP and VW courses were taught by fully trained MBSR instructors, it was not possible to have the same instructor for each condition, which limits the ability to account for potential instructor effects. These shortcomings limit causal inference. Finally, it may be that the study was statistically underpowered to detect significant differences for the Common Humanity, Self-Judgement, and Isolation subscales. The data did show greater improvements in the training groups than in the CG for these subscales, but it did not reach statistical significance.
Ethical approval
The study was approved by the San Antonio Military Medical Center Institutional Review Board and was performed in accordance with the ethical standards of the 1964 Declaration of Helsinki.
Informed consent
All participants provided their written informed consent before participating in the study. The informed consent form was approved by the U.S. Army, Brooke Army Medical Center Human Research Protections Office, Institutional Review Board.
Conflict of interest
The authors have no conflicts to declare.
Footnotes
Acknowledgments
The authors acknowledge the U.S. active duty and veteran service members who chose to volunteer their time to participate in this study. They also thank their colleagues: Gary Boykin, Leah Enders, Angela Jeter, Cory Overby, Jessica Villarreal, and Jim Hewson for their integral assistance with this research.
Funding
This research was funded by the U.S. Army Deputy Chief of Staff, G-8, Army Study Program Management Office, Washington, DC, USA (Study #: ARL 1704059-1).
Disclaimer
The views expressed in this article are those of the authors and do not reflect the official policy or position of the Department of the Army, Department of Defense, the U.S. Government, or Applied Research Associates (ARA).