
Abstract
BACKGROUND:
Dentistry is a physically and mentally demanding profession that involves long periods of muscle imbalance and asymmetrical postures when performing delicate procedures. This can lead to a high incidence of work-related diseases. However, physical activity may prevent or minimize the incidence of musculoskeletal discomfort and pain.
OBJECTIVE:
The present study aimed to determine the association between musculoskeletal disorders and physical activity levels in dentists practicing in Turkey.
METHODS:
This cross-sectional study was conducted between March and June 2023 with dentists from Turkey actively practicing dentistry. The short form of the International Physical Activity Questionnaire was used to determine dentists’ physical activity levels, and the Extended Nordic Musculoskeletal Questionnaire was used to assess musculoskeletal disorders. IBM SPSS 20 software was used for statistical analysis. Data were presented as mean, standard deviation, median, minimum, maximum, percentage, and number. Chi-square, Mann-Whitney U, One-Sample Chi-Square tests, and an ordinal logistic regression test were used. The statistical significance level was taken as p < 0.05.
RESULTS:
A total of 116 dentists (63 females 53 males) between the ages of 24 and 60 (36.37±7.32) were included in the study. Forty-eight participants had a low level of physical activity, 56 had a moderate level of physical activity (MLPA), and 12 had a high level of physical activity (HLPA). There was no significant difference between the gender (p = 0.224) and age (p = 0.469) of the participants and levels of physical activity. Musculoskeletal discomfort was reported by 93.1% (n = 108) of the participants in one or more body parts (p < 0.001) and 55.6% (n = 60) of them were female. The number of dentists with neck (p < 0.001) and shoulder (p = 0.05) problems was significantly higher. There was no significant effect of gender (p > 0.05) on musculoskeletal conditions. However, the relationship between musculoskeletal conditions and physical activity levels was inconsistent. The HLPA group reported the lowest discomfort for all body parts, except the elbows and knees (p < 0.05). The MLPA group reported higher discomfort in the neck, shoulder, upper back, wrists/hands, lower back, and knees. The group with the lowest physical activity exhibited the highest discomfort in the elbow and ankle/feet regions.
CONCLUSION:
This study found that the prevalence of musculoskeletal disorders was high among dentists, many of whom reported either low or moderate physical activity levels. The results of this study may enhance dentists’ understanding of work-related musculoskeletal diseases and promote their participation in physical activities.
Introduction
Musculoskeletal health refers to the strength of muscles, bones, joints, and adjacent connective tissues, and the ability of the musculoskeletal system to function properly. Musculoskeletal discomfort is the most prevalent form of non-cancerous pain [1]. Musculoskeletal disorders (MSDs) include a variety of conditions characterized by chronic pain that affects nerves, muscles, blood vessels, ligaments, tendons, bones, joints, and spinal discs that lead to limitations in mobility and motor skills [2]. MSDs are caused by strenuous and repetitive physical movements such as bending, stretching, reaching, grasping, holding, twisting, turning, pinching, and reaching, all of which can damage tendons, muscles, nerves, and other soft tissues, causing pain, numbness, tingling, burning, stiffness, fatigue, a reduced range of motion and grip strength, loss of normal sensation, or a loss of movement and coordination. Moreover, as the factors that cause MSDs typically consist of strenuous and repetitive movements, the recovery period may be prolonged [2, 3].
Work-related musculoskeletal disorders (WRMSDs) are defined by the International Commission on Occupational Health and Safety as work-related disorders or diseases of the musculoskeletal system. The World Health Organization has defined the term ‘work-related’ as a condition caused by the influence of work performance and work-environment factors [1, 4]. Manual workers are reported to have greater rates of accidents and lower life expectancies. Conversely, administrative workers have better outcomes in these areas. However, administrative workers do report negative health outcomes, as sedentary jobs are an important factor in the development of MSDs and other health problems, including cardiovascular illnesses and weight gain [5].
Dentistry is a physically and mentally demanding profession that involves the application of technical treatments and high concentration levels [6]. Specifically, dentists work in a tight [7] and often positionally uncomfortable [8] area of the mouth, performing delicate and prolonged procedures. This leads to muscle imbalances and asymmetrical postures for long periods [9]. The fixed position of the neck and shoulders may be a factor in the development of MSDs. In general, workers must maintain balance in the shoulder-neck area during controlled movements of the upper limbs, and the muscles in the region must continuously contract to maintain a stable position for as long as the task requires. These contracted muscles compress the blood vessels, causing discomfort [10]. To perform repetitive and demanding tasks, dentists must spend considerable time in non-ergonomic positions, which can lead to chronic pain exacerbated by unhealthy postures over time [11, 12]. The irregular layout of workstations and the selection of inappropriate tools and equipment may also contribute to these unhealthy postures. Furthermore, the use of additional personal protective equipment that accompanied the onset of the COVID-19 pandemic increased mental stress and the risk of engaging in unstable postures, further reducing freedom of movement [6, 10]. In particular, neck-tilt rotation, forward bending with loss of cervical and lumbar lordosis, and raised arms working in prolonged static isometric/eccentric contractions are the primary risk factors for musculoskeletal pain [13].
Tasks involving repetitive wrist, elbow, and shoulder joint movements (beyond acceptable limits) can cause pain [10]. In particular, dentists are at risk for MSDs given their poor posture, repeated tasks, prolonged static positioning, overexertion with excessive use of minor muscles, tight grasping of instruments, prolonged arm elevation, and using vibrating instruments [2, 14]. Vibration is known to affect tendons, muscles, joints, and nerves, and dentists can experience numbness in their fingers, a decreased sense of touch and grip, and pain when using vibrating instruments [15]. According to a 2009 systematic review, the global prevalence of MSDs in dentists is 64% to 93% [2, 16]. The muscles most affected are the neck [2, 18], back [18, 19], lumbar spine [12, 20], and upper limbs [4, 12]; although, in rare cases, the lower limbs may also be affected.
Physical activity (PA) is a widely recognized therapeutic intervention for a range of medical problems, including vasculopathic conditions such as coronary artery disease, stroke, type-2 diabetes, and obesity. Furthermore, performing more PA is a therapeutic approach to improving musculoskeletal well-being [21]. To prevent WRMSDs, physical exercise, specifically personalized exercises, for a minimum of 10– 15 minutes, 3– 5 days per week, has been found to help relieve musculoskeletal pain among office workers [22, 23]. Several studies have examined the health-promoting benefits of PA (both within and outside of the workplace) on the physical and mental health of workers. Their results have demonstrated that PA can effectively minimize the incidence of MSDs, improve physical fitness [24], improve mental health [25], and indirectly enhance work performance [5]. Moreover, exercise during leisure time can prevent injuries, improve health, and increase the longevity of dentists’ careers [3, 27]. Thus, PA can substantially affect the quality and quantity of MSDs experienced by dentists [28].
This study aimed to analyze the distribution of MSDs in a sample of dentists in Turkey and evaluate whether PA led to differences in musculoskeletal problems.
Materials and methods
Study design
The research is based on a survey design whereby the survey model is conducted on the entire population or a group of samples to be taken from the population to make a conclusion about the population [29]. This was a cross-sectional study conducted between March and June 2023 and was approved by the Ethics Committee of the Faculty of Dentistry, Atatürk University (decision date and number: 25.01.2023/03). Prior to the study, each participant signed an informed consent form in accordance with the Helsinki Declaration of 1975 as revised in 2013.
Study population and data collection tools
Study participants included dentists currently practicing dentistry with at least eight hours of clinical practice per week [30] in Turkey’s private and public sectors. The study excluded retired dentists and dentists who had experienced significant accidents, traumas, or medical conditions resulting in permanent musculoskeletal disability.
The International Physical Activity Assessment Questionnaire Short Form (IPAQ-SF) was used to determine PA levels in dentists. In 1996, Australian researcher Dr. Michael Booth developed a reliable and valid questionnaire to assess a population’s health and PA levels and their relationship. The International Physical Activity Assessment Group developed the IPAQ based on this questionnaire, and Öztürk conducted the Turkish validity and reliability study of the scale in 2005 [31, 32].
The IPAQ-SF includes questions about the amount of PA ‘in the last 7 days’ or ‘in any week’. The short form (seven questions) collects information on time spent in moderate and vigorous activities and walking. Time spent sitting was assessed as a separate question. The calculation of the total score for the short form includes the sum of the duration (minutes) and frequency (days) of walking, and moderate and vigorous activity [32]. Walking, moderate, and vigorous activity scores were converted into metabolic equivalents (METs) in minutes per week using the Ainsworth Compendium [33]. An average MET score was based on time spent on each activity intensity and then added together to create a total. This was then converted into three categories: low-, moderate-, and high-activity levels [34].
The Extended Nordic Musculoskeletal Questionnaire (NMQ-E) was used to identify MSDs in dentists. The NMQ was developed by Kuorinka and colleagues in 1987 [35]. Kahraman et al. conducted validity and reliability analyses and adapted it into Turkish [36]. The NMQ-E assesses acute, subacute, and chronic pain conditions by asking about pain, soreness, and discomfort on the day of assessment, in the past 4 weeks and the past 12 months. It further asks whether the pain interferes with the person’s daily life. The questionnaire divides the body into nine regions: neck, shoulder, upper back, elbow, hand/wrist, waist/lower back, hip/thigh, knee, and foot/ankle, and consists of a dichotomous yes/no response option [37, 38].
Statistical analysis
Analyses were conducted using the IBM SPSS 20 statistical analysis program (IBM Corp., Armonk, NY, USA). The statistical significance level was set at p < 0.05. Data are presented as means, standard deviations, medians, minimums, maximums, percentages, and caunt. The normal distribution of continuous variables was assessed using the Shapiro-Wilk and Kolmogorov-Smirnov tests. The Mann-Whitney U test was used to compare two independent groups. Comparisons of continuous variables with more than two independent groups were analyzed using the Kruskal-Wallis test. The one-sample Chi-square test was used to compare two ratios. In comparisons between categorical variables, the Pearson Chi-square test was used. An ordinal logistic regression test was performed to identify an association between PA and musculoskeletal pain.
Results
A total of 327 questionnaires were distributed and the response rate was 35.47% (116/327). A total of 116 dentists (63 females (54.3% ), and 53 males (45.7% )) between the ages of 24 to 60 years (mean±standard deviation: 36.37±7.32) participated in the study.
Table 1 shows the proportion of yes/no responses regarding pain areas, with 93.1% of the participants answering ‘yes’ to the question, “Do you have pain?” The ratio between dentists with and without pain was statistically significant (p < 0.001), with the rate of pain in the neck and shoulder regions was higher and statistically significant (p < 0.05). In the elbows, hips, thighs, knees, and ankles, the proportion of participants reporting no pain was significantly higher (p < 0.001) than those reporting pain. There was no statistically significant difference between the rates of pain experienced in the upper back, wrists, hands, and lower back (p > 0.05).
Pain prevalence and body regions experiencing pain by dentists in Turkey

Pain prevalence and body regions experiencing pain by dentists in Turkey
Statistical significance: **: p < 0.001; *: p < 0.05; One-sample-X2: One-Sample Chi-Square test value.
Table 1 shows the participants’ responses regarding pain and where it was experienced. Pain was primarily reported in the neck, shoulder, upper back, and waist regions, with less pain in the elbows, wrists, hands, hips, thighs, knees, ankles, and feet. No significant difference was found between males and females regarding the occurrence of pain and the body region where it was felt (p > 0.05) (Table 2).
Comparison between gender and pain regions

&Pearson’s chi-squared test; p < 0.05 is considered statistically significant.
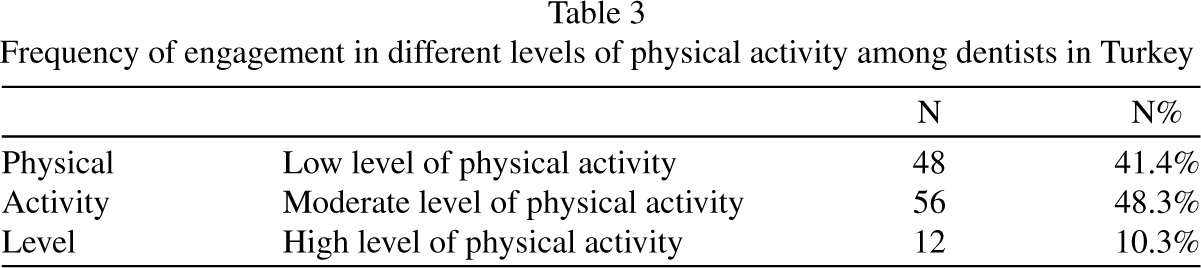
Forty-eight participants (41.4% ) engaged in low levels of PA (LLPAs), 56 (48.3% ) engaged in moderate levels of PA (MLPA), and 12 participants (10.3% ) reported high levels of PA (HLPA) (Table 3). No significant differences were found between PA levels and gender (p = 0.224) (Table 4). Similarly, no significant differences were found (p > 0.05) between age and gender and different PA levels (Table 5).
Frequency of engagement in different levels of physical activity among dentists in Turkey
Comparison of physical activity levels with gender
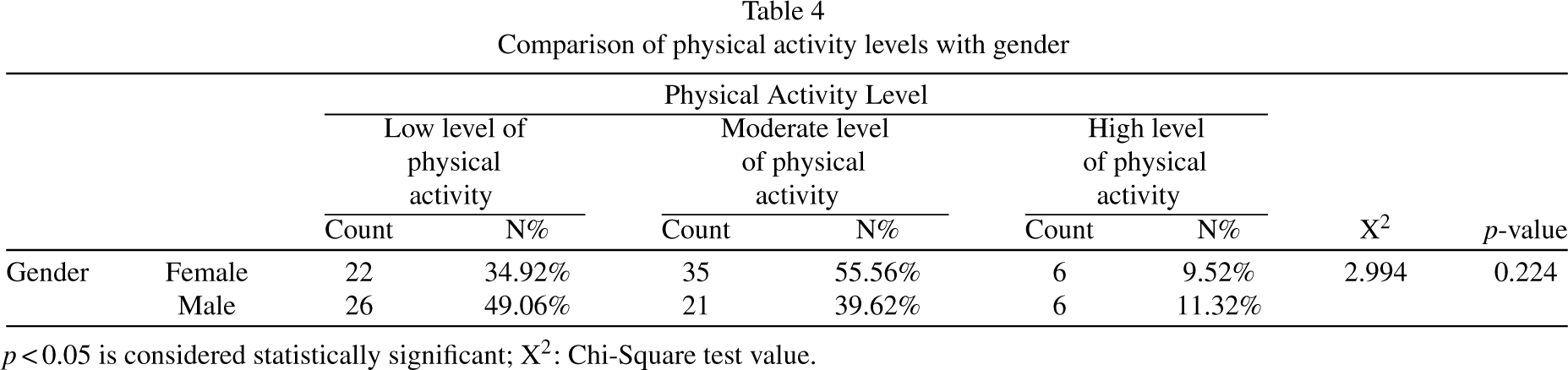
p < 0.05 is considered statistically significant; X2: Chi-Square test value.
Comparison of gender and physical activity level with age

p < 0.05 is considered statistically significant; ¥: Mann-Whitney U Test; £: Kruskal-Wallis test
When comparing pain areas with different PA levels (Table 6), significant differences were found between the groups regarding pain in the neck, shoulders, upper back, wrists, hands, waist, hips, thighs, and ankles (p < 0.05). However, there were no significant differences between the PA groups regarding pain in the elbows and knees (p > 0.05). Discomfort was significantly less in the HLPA group, while there was no significant difference between the LLPA and MLPA groups. The ordinal logistic regression model found no significant relationship (p > 0.05) between PA levels and MSDs between PA level and musculoskeletal pain region (Table 7).
The frequency of pain in different body regions according to levels of physical activity
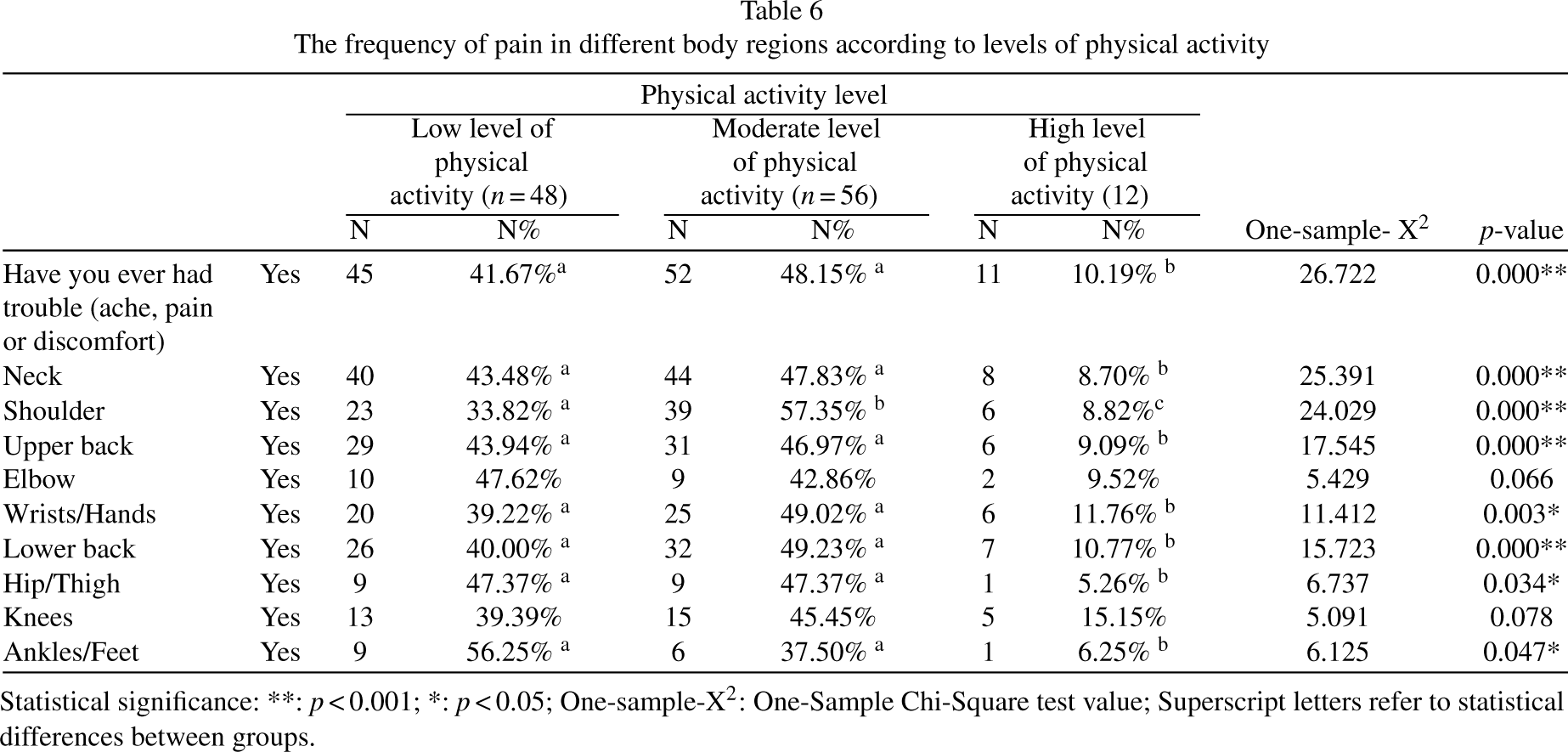
Statistical significance: **: p < 0.001; *: p < 0.05; One-sample-X2: One-Sample Chi-Square test value; Superscript letters refer to statistical differences between groups.
Results of a multinomial logistic regression test of association between physical activity level and pain regions

Statistical significance: p < 0.05; CI: Confidence interval; R2CS: Cox & Snell’s R2; R2N: Nagelkerke’s R2.
A number of research studies have investigated the musculoskeletal health of dental professionals [12]. Some have also assessed the prevalence of PA in the general population and different categories of healthcare professionals, including physicians, physiotherapists, and medical students. However, there is a lack of studies investigating PA among dental professionals [39]. Therefore, this cross-sectional study is one of the few to assess the prevalence of MSDs and PA levels among Turkish dentists.
The NMQ-E has been used in both international and national studies of dentists [40, 41]. In our study, the NMQ-E was used to measure MSDs. The ‘yes’ response to the question “Have you ever had problems (aches, pains, or discomfort)” was significantly higher among the study participants (p < 0.001; Table 1). Our findings are consistent with other studies in the literature. According to a study by Kerosuo et al [42], the prevalence of MSDs in dentists was 70% . In another study by Kandemir et al. [43], the authors found the prevalence of MSDs in dentists to be 82% . In studies by Nokhostin and Zafarmand [44] and Gopinath et al. [45] found that 67.5% and 73.9% of dentists, respectively, had musculoskeletal problems. One study investigating the prevalence of work-related musculoskeletal pain among dentists in Slovenia found that most of the participants suffered from pain [46]. Factors such as frequent bending, pushing and pulling, static work posture, weightlifting, repetitive movements, vibration, and prolonged, heavy, and intense work, were considered physical risk factors and the causes of musculoskeletal pain [47]. Dental working positions have also been implicated in causing cumulative microtrauma and muscle imbalances, neuromuscular limitations, pain, and dysfunction [6]. It has been reported that dentists must contract more than 50% of their body muscles to maintain their bodies in a fixed position against gravity. These postures often result in prolonged, repetitive muscle contractions characterized by classic muscular imbalances [48].
In our study, we found that the neck (79.3%, p < 0.001) and shoulder (59.1%, p < 0.001) regions most commonly experienced musculoskeletal problems, followed by the upper back (57.9%, p = 0.092) and lower back (56.0%, p = 0.194) (Table 1). Similarly, in their meta-analysis of 41 studies conducted in Western countries, Lietz et al. [49] found that the neck was most affected (58.5% ), followed by the lower back (56.4% ), shoulder (43.1% ), and upper back (41.1% ). Akesson et al. [50] also reported that MSDs were more common in the neck and shoulder regions. Likewise, other studies in the literature have shown that the most common sites of pain in dentists are the neck and shoulder regions, and the back, lower back, and wrist [43–45, 47]. A study investigating general dentists, orthodontists, and office workers showed that the neck (53% ) and shoulders (56% ) were the sites most involved in MSDs, followed by back pain (28% ) and pain in the arms and hands (17% ). In our study, less pain was reported in the elbow (18.1%, p < 0.00) and lower body (hip/thigh, knee, and ankle/feet; p < 0.001) than in other body regions. (Table 1). In the literature, the elbows, wrists, and finger joints are less commonly reported as the location of musculoskeletal symptoms [42]. Prolonged static postures (sitting or standing) are characteristic of a dentist’s work and are associated with neck, shoulder, and lower back symptoms [51]. Furthermore, micro-injuries and pain are frequently caused by insufficient time for tissues to regenerate due to overuse [52]. The working position of the dentist can also influence the location where the pain appears. Pain in the spine, neck, shoulders, and upper limbs is more common when working in a sitting position. While, standing has led to lower back pain, varicose veins, poor posture, and flat feet in dentists [48]. Moreover, there is a clear correlation between the total number of hours dentists work and the severity of the MSDs [51].
In our study, no significant differences were found between MSDs and gender (Table 2; p > 0.05). However, conflicting results have been reported with both similar [53, 54] and different [43, 45] results from ours. Ohlendorf et al. [55] also found no significant differences between females and males regarding the overall occurrence of pain. However, other studies have found significant differences in the occurrence of MSDs between males and females in the overall population and within the dental profession [56]. A higher prevalence of MSDs in females has been found and could be attributable to a heightened sensitivity to pain, as well as the effects of sociocultural, psychological, and biological factors, or hormonal and reproductive factors (e.g., estrogen levels) [57]. Moreover, the musculoskeletal system of females can exert only two-thirds of the force compared to the male system. Thus, women may face greater difficulty in stabilizing their bodies and compensating for the physical strain associated with delivering dental care [55].
According to the World Health Organization, physical fitness is a state of health and well-being, which can be achieved through regular exercise or PA [56]. Physical fitness may also influence professional success by improving work performance with fewer health problems. Dentists must work under stress for long periods, which leads to numerous work-related disorders, especially neck, back, and shoulder pain. Therefore, a dentist needs excellent stamina and strength throughout the working day to minimize fatigue and increase productivity. Thus, engaging in physical fitness is important to avoid work-related hazards, especially MSDs [57].
The IPAQ was developed by a group of specialists in 1998 to facilitate the monitoring of PA using a global standard. The IPAQ-SF has since become a widely used questionnaire and is recommended as a cost-effective way to assess PA [58]. According to the IPAQ-SF results in this study, 58.6% of the dentists were either highly or moderately physically active ((Table 3). The prevalence of PA among healthcare providers (HCPs) varies in the literature. Some studies have reported HCPs having higher levels of PA than the general population but but others suggested that HCPs are less active than the general population [39]. Sri Latha et al. [59] reported that 61% of dental HCPs were physically active. Sapna et al. [57] showed a maximum (72% ) of dental postgraduates were physically active. However, Singh A. et al. [60] reported that 68% of dental HCPs had LLPA. Öztürk and Çelik [61] reported that only 15% of dentists included in their study were physically active, and 66% were reported to be minimally active in Turkey. In our investigation, 41.4% of our study population were deficient in PA (Table 3). The primary factors contributing to this may be attributed to the operating hours of the clinics, which predominantly appeal to the working population by offering evening appointments. Some dentists also teach at dental institutions or work in dental hospitals during the day and subsequently pursue their private practice in the evenings [62]. Another potential factor may be long working hours [39, 61].
The PA of our subjects according to gender was similar, with no significant differences between males and females (Table 4; p = 0.224). These findings are in contrast to the studies by Thakar et al. [62] who found female dental students to be more active than males and Roshini et al. [63], who reported that male students were more physically active. However, the present findings are similar to the results by Sapna et al. [57], which showed similar PA levels in both genders. No relationship was found between the PA levels and participants’ mean age (Table 5; p = 0.469).
MSDs are multifactorial health problems influenced by factors such as prolonged static muscle tension, repetitive tasks, gender, and PA levels. Reports in the literature have found a strong correlation between PA level and health status in adults [64]. However, the literature is inconsistent in its findings regarding the relationship between PA and MSDs, suggesting a lack of consensus on this issue [64].
Our results found that dentists in the HLPA group had reduced musculoskeletal pain, aches, or discomfort (Table 6; p < 0.05). Other studies have confirmed strong and significant correlations between regular and frequent PA and a reduction in musculoskeletal pain and the number of sites where pain is felt [65]. Furthermore, participation in PA helps the body adjust to muscle weariness that may arise while working [66]. Dentists with low PA have a significantly higher number of sites with musculoskeletal pain compared to those who regularly perform PA [67]. Moreover, dentists who perform LLPA are more likely to experience less flexibility in their joints and less extensibility in their connective tissue. As a result, they have a higher likelihood of experiencing musculoskeletal pain compared to those who routinely participate in physical exercise [68]. A study by Sharma and Golchha reported that 75% of dentists were at risk of developing occupational MSDs and that the prevalence and severity of musculoskeletal complaints were reduced by 20% and 80%, respectively, by regular, specific exercise [69]. Individuals who are not physically active have been reported to have a higher risk of developing MSDs due to decreased nutrient and oxygen flow to the muscles. Thus, 20 minutes of aerobic physical exercises three to four times weekly is advised for dental professionals [48, 70]. In addition, the incidence and risk of MSDs can be reduced by dentists working in appropriate postures, with intermittent working hours, and targeted and personalized PA [70].
Study limitations
There are several limitations to this study. First, the sample size may not have been large enough to detect small but important differences, which would decrease the generalizability of the results. Furthermore, for the HLPA group, the sample size was much smaller than other groups. Second, self-reported survey studies have fundamental challenges related to the subjectivity of respondents in observing and assessing themselves [42]. Finally, there is the possibility of a health worker effect in cross-sectional occupational health studies, as serious cases may have been missed as individuals would have left the profession due to the severity of their symptoms [42].
Conclusion
Our results revealed a high prevalence of musculoskeletal pain among dentists. The most common areas of musculoskeletal pain were the neck and shoulder. Most dentists participating in this study indicated either low or moderate levels of PA. These findings emphasize the need to address musculoskeletal conditions and improve PA levels in dentists to reduce their pain and discomfort.
Footnotes
Conflict of interest
The authors declare that they have no conflicts of interest.
Financial disclosure
The authors report no funding.
Data availability
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Ethics approval statement
Ataturk University Faculty of Dentistry Ethics Committee (Decision date and number: 25.01.2023/03).
Patient consent statement
The study participants were informed about the study and signed voluntary consent forms.