
Abstract
BACKGROUND:
Backpack syndrome (BS) is a term used to describe symptoms such as shoulder and back pain that are believed to be caused by carrying a backpack. Few studies have investigated the changes in walking and running parameters with and without backpacks.
OBJECTIVE:
The present study aimed to investigate the differences in walking and running parameters with and without backpacks in primary school children with and without BS.
METHODS:
This cross-sectional study included 51 children (average age 9.3 years, 6– 12 years). Two questions were asked beforehand: whether the respondents had shoulder or back pain when going to school and present; those who answered that they had pain in both cases were defined as the BS group, while the others were the control group. Walking and running at comfortable speeds and walking and running with a 6 kg backpack on their backs were measured.
RESULTS:
During walking, there were main effects for speed, cadence, and strike angle with and without the backpack, but no interactions were identified for any of the parameters. In running, however, there were main effects for speed, stride length, strike angle, and lift-off angle, and an interaction effect was observed for speed and stride length.
CONCLUSIONS:
During walking, carrying a 6 kg backpack increased cadence and walking speed. During running, carrying a backpack caused a decrease in stride length and running speed in the BS group, whereas there was no change in the control group, suggesting that the control and BS groups may respond differently.
Introduction
Backpack syndrome (BS) is a term used to describe symptoms such as shoulder and back pain, headache, and poor posture that are caused by carrying a backpack for extended periods of time. In particular, it can be caused by carrying an inappropriate amount of weight [1]. Therefore, the syndrome is associated with children carrying school textbooks and luggage on their backs. In Japan, BS is recognized as “randoseru syndrome” or “schoolbag syndrome” because elementary school children throughout the country use school bags [2]. However, the term BS is not strictly defined medically, and individual symptoms, causes, and diagnostic criteria have not been established. Therefore, there is no clear definition in the medical literature or diagnostic manuals. However, there have been many studies on back pain in children due to carrying backpacks [3, 4], and it is believed that they should to pay attention to how they carry their school bags while maintaining proper posture as well as the weight and use of their school bags to reduce the burden on the body [3].
It is known that 83% of pupils likely carry school backpacks on both shoulders when carrying luggage [5], and there are many reports on postural changes and the effect of luggage volume due to carrying school backpacks. The increased weight on the student’s back changes the body’s center of gravity and adjusts the load backward [6]. As the external load increases, torso flexion increases markedly in response to motor control mechanisms that attempt to move the body and the bag’s center of gravity forward together to maintain balance [7–9]. The combination of external loading and degree of torso flexion increases the pressure on the intervertebral discs [10–12]. Backpack loading increases the axial pressure on the spine and has been shown to alter disc height and symmetry at the T12-S1 level and the angular values of intervertebral relationships [13], raising concerns regarding the impact of load volume on children with stereotypical development. In a previous study, the posture of walking with a weight of 13.8% of the body weight on the back was analyzed, and the load on the lumbar spine was shown to be more dangerous than that during normal walking [14]. Various studies have shown that backpacks weigh between 10% and 22% of a student’s body weight [15].
However, few studies have investigated changes in walking and running parameters with and without backpacks, with some reporting that carrying a backpack decreases walking stride length [16] whereas others report that it increases stride length [17], and results have not been consistent.
Human gait parameters have been reported to vary slightly among countries, races, and ages [18–20]. There have been several reports of varying gait conditions in typically developing children, and a comparison of gait parameters in barefoot and shoe-wearing conditions has revealed that there is no change in cadence, but that an increase in stride length increases gait speed [21]. Thus, the walking speed varies with stride length and cadence. The presence or absence of a backpack may change the speed adjustment strategy during walking and running in children with or without shoulder or back pain, as in BS. The changes and characteristics of the walking and running parameters with and without a backpack allow for more appropriate involvement in the preventive rehabilitation of children with BS. Accordingly, the present study aimed to investigate the differences in walking and running parameters with and without backpacks in primary school children with and without BS.
The research hypothesis was that, when performed at any comfortable speed, walking would not differ with and without BS, and the presence of a backpack would decrease stride length and slow speed with no change in cadence. During running, the presence of a backpack would cause a different process depending on the presence or absence of BS. Specifically, the presence of a backpack would reduce the stride length, cadence, and speed in the group with BS, whereas the absence of a backpack reduced the stride length and slowed the speed in the group without BS.
Methods
Participants
Recruitment leaflets were distributed to children in all primary and junior high schools in Fukushima City, Fukushima Prefecture, to recruit eligible applicants. The survey was conducted on a holiday day in March, from 9 : 00 a.m. to 4 : 00 p.m., taking into consideration the ease of participation and fatigue of the children. The inclusion criterion was healthy primary and secondary school children with no underlying endogenous diseases. To determine the required sample size, a power calculation was conducted using G power, and the effect size was calculated using a moderate effect size based on Cohen’s criterion [22]. In the generalized linear mixed model (GLMM), referring to the criterion in the two-way ANOVA with the effect size set to 0.25, alpha level set to 0.05, and power set to 0.80, a total sample size of 36 was required.
The participants were 66 healthy primary and secondary school children. To investigate the situation of primary school children, participants who were secondary school children, underwent major trauma or surgery within 6 months, had special educational support, or were unable to complete the measurement were excluded. Accordingly, 51 participants (aged 6– 12 years) who met the inclusion criteria were analyzed. In this study, two questions were asked beforehand: whether the respondents had shoulder or back pain when going to school, and whether they had shoulder or back pain at present; those who answered that they had pain in both cases were defined as the BS group, while the others were the control group (Fig. 1). All participants and their parent provided written and verbal informed consent before participation. The Ethics Committee of Fukushima Medical University granted approval to conduct the study within its facilities (authorization number: 2022-097).
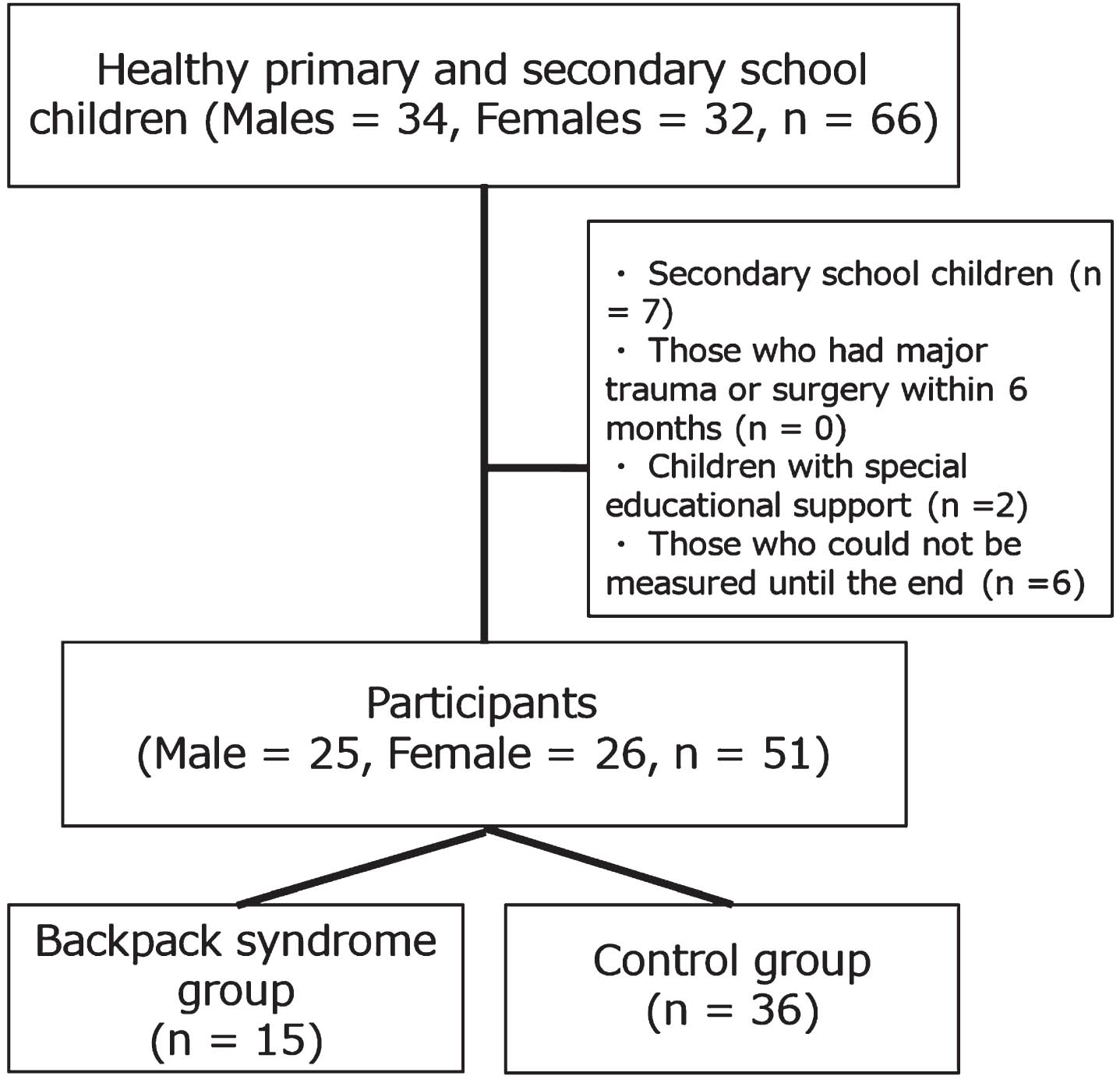
Subject Flowchart.
This cross-sectional study included primary school children in Fukushima City, Fukushima Prefecture, Japan.
Measures
Foot function and morphology
Toe grip strength was measured using a toe grip dynamometer (Takei Scientific Instruments Co., Ltd.), according to a method with established intra- and inter-rater reliability in adults [23]. The participants sat on a chair with the hip in a neutral position of adduction, abduction, internal rotation, and external rotation, and the knee and ankle joints at 90°. The examination procedure was practiced before the actual measurements were obtained. The first proximal phalanx was placed on the grip bar, and the heel stopper was adjusted to fit each participant’s heel. Grasping of the bar was performed with maximum force using all toes twice on each side, and the maximum value was adopted.
The arch-height ratio and footprints were measured in a stationary standing position, with the feet shoulder-width apart and equal weight on both feet. The height from the floor to the navicular tuberosity was measured as the arch height once on each side in the standing position [24]. The arch height ratio was calculated as the ratio of the floor to navicular tuberosity height to foot length. The footprints were measured on each side. However, if the foot moved during the measurement, and the measurement could not be performed, a second measurement was performed. The metatarsophalangeal angle was measured as the angle between the line connecting the first metatarsal head and the first basal phalanx and the line connecting the first metatarsal head and the posterior medial phalanx [25].
Walking and running measurements
Walking and running were measured using two synchronized inertial measurement unit (IMU)-based devices (Physilog5®, GaitUp, Switzerland). Each IMU comprised a triaxial accelerometer (range± 16 g), and triaxial gyroscope (range± 1000°/s) with a sampling frequency of 100 Hz. In the present study, the device was attached to the participant’s everyday shoes in accordance with the manual, and the following were measured twice, each over a 20 m linear path indoors. First, the participants were asked to walk at a comfortable speed for a standard gait assessment. Second, a 6 kg school bag was placed on the participant’s back, and the same instructions as for the gait assessment were given. In 2018, an online survey of 2000 pairs of Japanese children and their parents reported that the average weight of luggage on the heaviest day of the week for a school bag was approximately 6 kg [2]. Therefore, in this study, the total weight of the schoolbag was set and prepared in advance to 6 kg using weights. Third, the participants were instructed to run at a comfortable speed to perform a standard running assessment. Finally, they were asked to carry a 6 kg backpack on their backs and were given the same instructions as for the running assessment. During the measurements, care was taken to ensure that the participants were not fatigued and breaks were taken as necessary.
Walking and running data, excluding two cycles at the start and end of the obtained data, were used for the analysis. For each measurement, the average values of the two measurements of stride length, cadence, speed, strike angle, and liftoff angle obtained from the data of the right foot were adopted. Stride length describes the distance between two successive footprints on the ground, from the heel of the foot to the heel of the same foot, one cycle later. The cadence is the number of cycles per minute. Speed, the walking and running stride velocity, is the mean speed of forward motion, calculated in m/s. The strike angle is the angle between the plantar surface and ground at heel strike on the vertical plane. The lift-off angle is the angle of the between the plantar surface and ground at the end of the push phase, just at takeoff.
Statistical analysis
First, the normality of all the variables was checked using histograms. Second, the attributes of the participants were compared using the unpaired t-test and chi-square test. Finally, the walking and running parameters were compared using the GLMM and Bonferroni’s multiple comparison test, with groups as the without-subject factor, and normal and with a backpack as the within-subject factors. All analyses were performed using SPSS statistical package for Windows, version 27.0. software (IBM Corp., Armonk, NY, USA). Statistical significance was set at p < .05.
Results
Participants’ attributes are listed in Table 1. There were 15 (29.4%) participants in the BS group and 36 (70.6%) in the control group, with no differences in age, foot function, or morphology between the two groups.
Subject attributes
Subject attributes
Average (standard deviation); SMI: skeletal muscle mass index, *vs. control group, *p < 0.05.
The GLMM results for walking for the groups and the availability of backpacks are presented in Table 2, and the GLMM results for running are presented in Table 3. The parameters are listed in Table 4. In terms of the walking parameters, for the GLMM results on cadence, speed, and strike angle, the main effects were not observed by group but were observed by backpack presence (cadence: F = 5.738, p = 0.020; speed: F = 6.937, p = 0.011; strike angle: F = 5.418, p = 0.024). The interactions (group×availability of backpack) were not significant. For the results of the GLMM on stride length and lift-off angle, main effects were not observed by group or backpack availability. The interactions (group×availability of backpack) were not significant.
Generalized linear mixed model table for each parameter during walking
*p < 0.05.
Generalized linear mixed model table for each parameter during running
*p < 0.05.
Comparison of each group’s parameters for dominant and non-dominant feet
Average (standard deviation), *normal vs. backpack, †backpack syndrome group vs. control group, *, † p < 0.05.
In terms of the running parameters, for the results of the GLMM on stride length, a main effect was not observed by group but was observed by backpack presence (F = 12.160, p = 0.001). An interaction was observed for stride length (F = 4.443, p = 0.040). In the results of the multiple comparison test, in the BS group, stride length was significantly shorter when running with a backpack than during normal running, whereas in the control group, there was no difference between normal running and running with a backpack. In addition, the stride length in the BS group was shorter than that in the control group during normal running. For the results of the GLMM on cadence, a main effect was not observed by group or backpack availability. The interaction (group×availability of backpack) was not significant. For the results of the GLMM on speed, a main effect was not observed by group but was observed by backpack presence (F = 7.337, p = 0.009). An interaction was observed for speed (F = 4.324, p = 0.043), and in the results of the multiple comparison test, in the BS group, speeds were significantly slower when running with a backpack than during normal running, whereas in the control group, there was no difference between normal running and running with a backpack. For the results of the GLMM on the strike angle and lift-off angle, main effects were not observed by group but were observed by backpack presence (strike angle: F = 4.841, p = 0.033; lift off angle: F = 4.093, p = 0.049). The interactions (group×availability) were not significant.
In a review of back pain in primary to high school students, the prevalence of back pain ranged from 14.6% to 36% depending on the age of the participent [4]. In a survey of 164 primary school children, 32.5% of all respondents reported back pain [1], and 35% in a survey of 287 respondents [26]. As back pain includes the upper back, lower back, neck, and shoulders, which are the most prevalent body regions [27], the incidence of back pain depends on its definition of back pain. In this study, the prevalence of BS was 29.4%. In the present study, BS was defined in children who met both the criteria of having shoulder stiffness/back pain when going to school and having shoulder stiffness/back pain at the present time, which may have slightly reduced the incidence of back pain in primary school children compared to previous studies of back pain in primary school children.
In a reference database of Japanese children’s gait, stride length, cadence (127.2 steps/min), and speed (1.21 m/s) were reported for children of a similar age as the present study children [28]. This is similar to the results for normal walking in the subject children, and together with the incidence of BS in the subject children, supports its validity.
During walking, there were main effects for speed, cadence, and strike angle with and without the backpack, but no interactions were identified for any of the parameters. Specifically, cadence and speed increased in walking with a backpack compared to those in normal walking for all participants, and the strike angle was slightly larger, with a mean value of 2.3°. This result differed from the research hypothesis, which considered that carrying a backpack would lower the stride length and thus slow down the speed. The subject schoolchildren slightly increased their cadence and speed by performing an effortful gait to maintain a comfortable speed with a 6 kg weight on their backs. Muscle activity in the peri-ankle muscles become more active with increasing cadence. In the present study, the muscular activity of the ankle dorsiflexor muscle group increased with increasing cadence, and the heel ground contact angle with the floor increased, albeit only slightly.
In contrast, in running, there were main effects for speed, stride length, strike angle, and lift-off angle, and an interaction effect was observed for speed and stride length, indicating that the BS and control groups followed different paths in running. In the BS group, stride length was on average 0.22 m shorter and speed 0.3 m/sec slower with the backpack. However, in the control group, the stride length and speed did not change with or without the backpack. This partially supported the research hypothesis that carrying a backpack in the BS group would reduce stride length and velocity and differed from the research hypothesis that lower stride length would slow velocity in the control group. Previous research has shown that children carrying loads exhibit decreased ankle dorsiflexion, maximum hip extension, and pelvic rotation range [29]. The increase or decrease in the hip extension range of motion is directly related to the stride length. Similarly, during running, a decrease in hip extension movement was thought to have led to a decrease in stride length, which in turn led to a decrease in running speed. Running with a backpack on requires greater muscle activity in the trunk and lower limbs than walking. This running was a “comfortable speed.” The running parameters of the control group did not change with or without the backpack, which suggests that the control group had sufficient physical function to maintain a comfortable speed compared to the BS group; that there were no differences in foot function or structure between the two groups also suggests the need for future research on trunk and peri-hip function.
During running, the strike angle was, on average, 3.5° greater and the lift-off angle was slightly 1.5° greater with the backpack compared to normal in all participants. Similar to the changes during walking, effortful running to maintain a comfortable speed with a 6 kg weight on the back is thought to have resulted in more muscular activity in the peri-ankle muscles and an increase in the heel ground contact angle with the floor and the floor kick-off angle during heel contact. The angular change in the strike and liftoff angles was negligible for both walking and running, and it is unlikely that the slight angular change had a significant effect on walking and running. However, it was found that the presence of a backpack may change shock absorption at initial contact and kick-out at the terminal stance in both walking and running.
Limitations
This study has some limitations. This was a cross-sectional study with a small number of participants in the BS group; therefore, the generalizability of the results may be limited. In addition, postures during walking and running were not investigated in this study. In the future, the number of participants should be increased and their posture and trunk and hip functions while carrying a backpack should be investigated.
Conclusions
The prevalence of BS was 29.4% in all participants. During walking, carrying a 6 kg backpack increased cadence and walking speed. During running, carrying a backpack caused a decrease in stride length and running speed in the BS group, whereas there was no change in the control group, suggesting that the control and BS groups may respond differently. Our findings provide a useful avenue for improving health conditions and more appropriate interventions for schoolchildren with shoulder and back pain.
Reporting guidelines
Reporting is in accordance with the STROBE Statement for cross-sectional studies listed in the EQUATOR Network for Reporting Guidelines.
Ethical considerations
The Ethics Committee of Fukushima Medical University granted approval to conduct the study within its facilities (authorization number: 2022-097). All participants were children, no intrusive measures were used, and no deception of participants was used. A detailed explanation of the procedure is given in the methods section.
Informed consent
The participants and their parent have consented to the use of the anonymized data for scientific purposes. A detailed explanation of the procedure is given in the methods section.
Footnotes
Acknowledgments
Conflict of interest
The authors declare there are no competing interests.
Funding
This study was financially supported by The Nakatomi Foundation.
The following information was supplied regarding data availability: Data are available at Figshare: Differences in walking and running parameters in elementary school students with and without backpacks (dataset).
DOI: 10.6084/m9.figshare.24944925.