
Abstract
BACKGROUND:
Professional identity encompasses the understanding of professional practices and the development of values and skills within a specific profession.
OBJECTIVE:
This study aimed to assess the suitability of the 9-item Macleod Clark Professional Identity Scale, originally developed by Adams et al. (2006), for Turkish culture and examine its psychometric properties in a sample of postgraduate nurses.
METHODS:
The study was conducted using a methodological approach. The sample consisted of 100 postgraduate nurses. Various analyses were conducted, including descriptive statistics of the scale, Cronbach’s alpha coefficient, item-total score correlation, and scale response bias for reliability assessments. Validity analyses included assessments of language, content, construct validity, concurrent validity, and known group validity.
RESULTS:
The Cronbach’s alpha coefficient for the 9-item Macleod Clark Professional Identity Scale was found to be 0.85, indicating good internal consistency. Item-total score correlations ranged from 0.34 to 0.88. The confirmatory factor analysis goodness of fit indices, except for the AGFI index, had acceptable values after two modifications. The single-factor structure of the scale was confirmed by confirmatory factor analysis. For concurrent validity, the scale demonstrated a positive and robust correlation with scores from the Nursing Professional Commitment Scale, supporting its validity. In terms of predictive validity, a regression model was established to assess the relationship between independent variables and core professional identity, and the model was found to be at acceptable levels.
CONCLUSIONS:
This study showed that the Turkish adaptation of the 9-item unidimensional “Macleod Clark Professional Identity Scale” demonstrates acceptable levels of validity and reliability when administered to postgraduate nurses in Turkey.
Introduction
Professional identity can be described as a combination of attitudes, values, knowledge, beliefs, and skills that individuals within a professional group share, and it is closely tied to the specific professional roles undertaken by these individuals [1]. The development of professional identity is a complex process influenced by various factors, including knowledge, professional authority, community recognition, ethical principles, social culture, gender, work experience, professional knowledge, teamwork skills, workplace learning, interpersonal interactions, and prior awareness of the profession [2].
Theoretical framework: Social identity theory
Professional identity is an integral part of an individual’s social identity [3]. Thus, Social Identity Theory (SIT) provides valuable insights into understanding how professional identity evolves [1]. Initially proposed by Tajfel in 1972, SIT revolves around intergroup social comparisons driven by the innate need for self-esteem, and it seeks to establish or confirm a distinction between the “ingroup” and the “outgroup” in favor of the ingroup [4]. Tajfel and Turner (1986) further emphasized the difference between “interpersonal situations,” where individual behavior is primarily influenced by personal factors, and “group situations,” where behavior is largely shaped by category-based processes, and introduced the concepts of personal and social identity. SIT posits that social identity primarily arises from group memberships and suggests that distinct social groups are defined by social categories that establish power dynamics, status, and prestige among these groups. Individuals position themselves within and across these groups to construct and maintain their social identities [5]. Moreover, SIT asserts that individuals strive to attain or preserve a positive social identity (which boosts self-esteem), and this positive identity largely results from favorable comparisons made between the ingroup and relevant outgroups [6].
Salient groups, which include institutions, organizations, or work groups with which individuals are associated, are diverse. Among these, professional groups (occupational groups) play a significant role in shaping social identity [4]. Professional identity fulfills the need for status, which drives social identification. The process of becoming part of the professional community offers stability, a sense of belonging, and shared values, and reduces uncertainty [3]. Professional socialization is a multifaceted and interactive process. It encompasses learning the roles and responsibilities associated with a profession, including acquiring knowledge, skills, and behavioral norms; internalizing a sense of professional identity, which is related to the values, attitudes, and objectives of the profession, and the unique characteristics of group members [6]. In essence, it entails integrating the group’s values and norms into one’s own behavior and self-concept while adopting a sense of professional identity [1]. Numerous studies in the literature have highlighted that developing a sense of professional identity is a central objective and a beneficial outcome of professional socialization [7, 8]. Role models play a significant role in shaping the cognitive phase of professional socialization, thereby contributing to the development of professional identity [1, 9]. These role models can be professionals working in the same workplace or educators providing instruction to students. The information about the profession that students acquire through their interactions with role models as well as their own experiences forms the core of professional socialization and identity development [1]. Within the literature, the outcomes related to professional identity have been categorized as either strong development of professional identity or inadequate development of professional identity [10].
Given the adverse consequences associated with insufficient development of professional identity in the healthcare field, such as students leaving their educational programs or the profession itself and a decrease in commitment to the profession, it becomes crucial to assess the level of professional identity and the factors influencing it to promote its development. In this context, this study holds original value by offering a tool for assessing professional identity within the healthcare domain. Therefore, this study aimed to assess the suitability of the 9-item Macleod Clark Professional Identity Scale for the Turkish cultural context and evaluate its psychometric properties using a sample of postgraduate nurses.
Method
Research type and sample
This methodological study included a total of 100 participants who were pursuing postgraduate education in the Department of Nursing at the Institute of Health Sciences within a public university located in the western region of Turkey. In terms of sample size, it is generally recommended to have a minimum of five times the number of observations for each variable, with a preferable ratio of 10 : 1 [11]. Furthermore, in the literature, MacCallum et al. (1999) suggested that a sample size ranging from 100 to 200 is considered “acceptable” for factor analysis [12]. Considering the scale’s item count (9 items) and existing literature, a minimum sample size of 100 was determined for this study.
The sample consisted of 100 randomly selected nurses (aged 22–47) who were enrolled in the specified institute between January and October 2022. These participants volunteered to take part in the study, and their informed consent was obtained.
Data collection instruments
Procedure
Following the linguistic adaptation, the Davis technique was employed to assess the content validity of the scale during the conceptual evaluation of its items [17]. The content validity index (CVI) was calculated using the Davis technique for content validity [18]. This technique involves ranking expert opinions on a scale from one to four: “not relevant,” “somewhat relevant,” “relevant,” and “very relevant.” For each the item, content validity index (I-CVI) is determined by dividing the number of experts who rated it as three or four by the total number of experts. The overall scale’s content validity (S-CVI) is calculated by averaging the item-level I-CVIs for all items in the scale [18, 19]. To assess content validity, the Turkish version of the scale was presented to nine faculty members with diverse expertise (Public Health, Psychiatry, Nursing). These faculty members conceptually evaluated each item, assigning scores from one to four. A S-CVI above 0.80 is indicative of good content validity [20]. In this study, the CVI for the nine items was calculated to be 0.98, exceeding the recommended threshold of 0.80, indicating adequate content validity. A preliminary version of the scale was pre-tested (with 10 nurses who were pursuing postgraduate education) to assess the comprehensibility of the items. There was no negative feedback or suggestions for corrections during the pre-test. Subsequently, the data collection phase commenced, and the pre-test data were not included in the study.
Data analysis
Statistical analysis was conducted using IBM SPSS (Version 23.0) and the LISREL package programs [21, 22]. Descriptive statistics were computed to describe the participants’ demographic characteristics. To assess the normal distribution of the data, Kurtosis and Skewness values were examined (MCPIS: Kurtosis: 0.459, Skewness: –0.753; NPCS: Kurtosis: 0.917, Skewness: –0.739). Kurtosis and Skewness values within the range of –1.5 to +1.5 are generally considered indicative of normal distribution characteristics [23]. In the score distributions of the scale, the mean, standard error, and standard deviation values of the nurses’ responses to the 9 items in the scale were calculated. In the scale’s reliability assessment, Cronbach’s alpha coefficient, item-total score correlation, and scale response bias were evaluated. Cronbach’s alpha values above 0.70 were considered “adequate” [24, 25]. Cronbach’s alpha values were also computed and analyzed when individual items were removed. The desired item-total correlation values typically range above 0.3–0.4 [24].
The scale’s validity was assessed through linguistic validity, content validity index, followed by construct validity (confirmatory factor analysis), concurrent validity, and known-groups validity. In the literature, CFA is recommended as the initial step in cross-cultural scale adaptation studies. If CFA fails to confirm the dimension structure of the original scale model or if the model-data fit is inadequate, the scale should be further assessed via exploratory factor analysis [26]. In this study, the unidimensional model from the original scale was evaluated using CFA. Summary fit index values, including Chi-square/degree of freedom (χ2/sd), Root Mean Square Error of Approximation (RMSEA), Standardized Root Mean Residual (SRMR), and Incremental Fit Index (IFI), were provided. Various fit indices and cutoff points for these values have been reported in the literature. To indicate an “acceptable” model fit, the following criteria are often used: a χ2/df value below 3, RMSEA and SRMR values under 0.08, and Comparative Fit Index (CFI) and Normed Fit Index (NFI) above 0.90, along with a Goodness-of-Fit Index (GFI) exceeding 0.95. In CFA, a χ2/df value less than 5, an RMSEA value below 0.08, and goodness-of-fit indices (GFI, CFI, NFI) greater than 0.90 are considered “acceptable” for model fit [27]. For concurrent validity, correlation coefficients between the 9-item MCPIS, and NPCS, and its sub-dimensions were examined. Measurement tools that address similar topics are expected to exhibit moderate to strong correlations. Correlation values were interpreted as very weak (0.00–0.10), weak (0.10–0.39), moderate (0.40–0.69), strong (0.70–0.89), or very strong (0.90–1.00) [28]. Known-groups validity was assessed by comparing differences in working conditions, enjoying the profession, and the 9-item MCPIS score using nonparametric tests (Kruskal-Wallis test) because the data did not meet the assumptions of normality based on normality tests. Additionally, variables such as “satisfaction with the institution,” “satisfaction with the profession,” and “intention to quit the profession” were assessed using three separate questions, and data were collected using a 10-cm self-report scale. Participants were asked to rate their level of satisfaction or likelihood on a scale from 0 to 10. For example, one of the questions was “Rate your level of satisfaction with the institution out of 10.” Relationships and differences between the assessment data from these questions and the 9-item MCPIS score were determined.
Ethical considerations
Permission was obtained from Adams et al. (2006) via email for the adaptation of the measurement tool into Turkish. Additionally, ethical approval for the study was obtained from the local ethics committee of the institution where the researchers are affiliated (Decision date: December 01, 2021; Decision No: 20.478.486/1070).
Results
Characteristics of the sample
According to the results, the mean age of the nurses was 32.07±5.21 years (22.00–47.00). 83% were female, 73% were married, 36% were following postgraduate education, 51% worked in a hospital, 56% worked more than 40 hours per week, 51% worked day shifts, 70% evaluated the working conditions as moderate, and 62% liked the profession. It was found that the mean duration of professional experience and employment in the institution were 9.22±5.14 and 5.86±4.29 years, respectively. The mean score of satisfaction with the institution was 5.40±2.33 (out of 10), the mean score of satisfaction with the profession was 6.53±2.14 (out of 10), and the mean score of the intention to quit the profession was 4.43±2.87 (out of 10). The mean score of the NPCS was 77.65±13.80, the mean score of the Willingness to Make Effort subscale was 37.87±7.18, the mean score of the Maintaining Professional Membership subscale was 23.88±5.82, and the mean score of the Belief in Goals and Values subscale was 15.90±2.77.
Descriptive statistics and reliability analyses of the scale
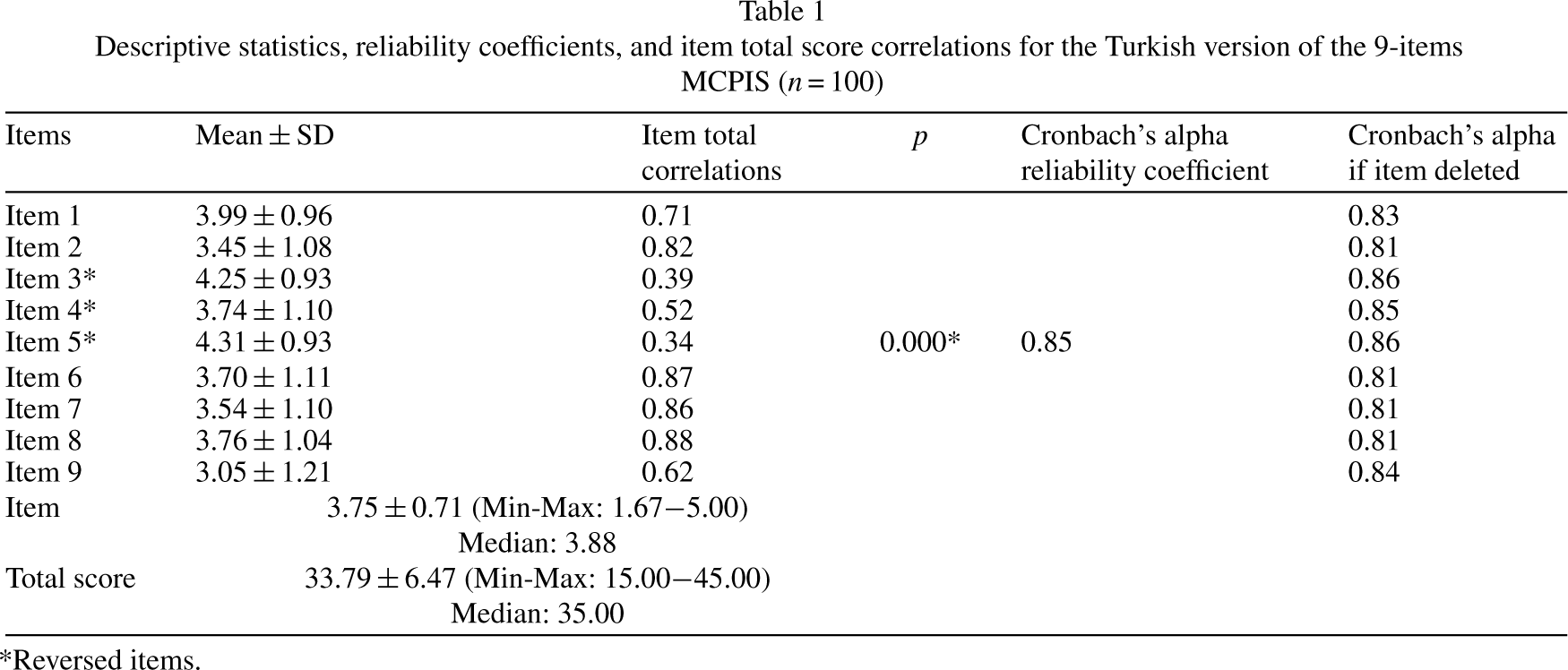
The mean 9-item-MCPIS total score was 33.79±6.47 (Min-Max: 15.00–45.00; Median: 35.00) and the mean item-total score was 3.75±0.71 (Min-Max: 1.67–5.00; Median: 3.88). The mean scores of the 9-item MCPIS items ranged between “3.05 and 4.31”. As a result of the item analysis performed to test the internal consistency of the scale, the item-total score correlations of the items were found to be between 0.34–0.88 (p < .01). The Cronbach’s alpha coefficient of the unidimensional 9-item MCPIS was calculated at 0.85. In the internal consistency analysis performed by removing items 3 and 5, a minimal increase (0.86) was observed in the Cronbach’s alpha value of 0.85. The data for all items of the scale without disturbing the original scale structure is presented in Table 1.
Descriptive statistics, reliability coefficients, and item total score correlations for the Turkish version of the 9-items MCPIS (n = 100)
Descriptive statistics, reliability coefficients, and item total score correlations for the Turkish version of the 9-items MCPIS (n = 100)
*Reversed items.
In the study, Hotelling’s T2 test was performed to check whether the responses of the individuals to the scale items were equal, and the Hotelling value was found to be T2: 111.946, p = .000.
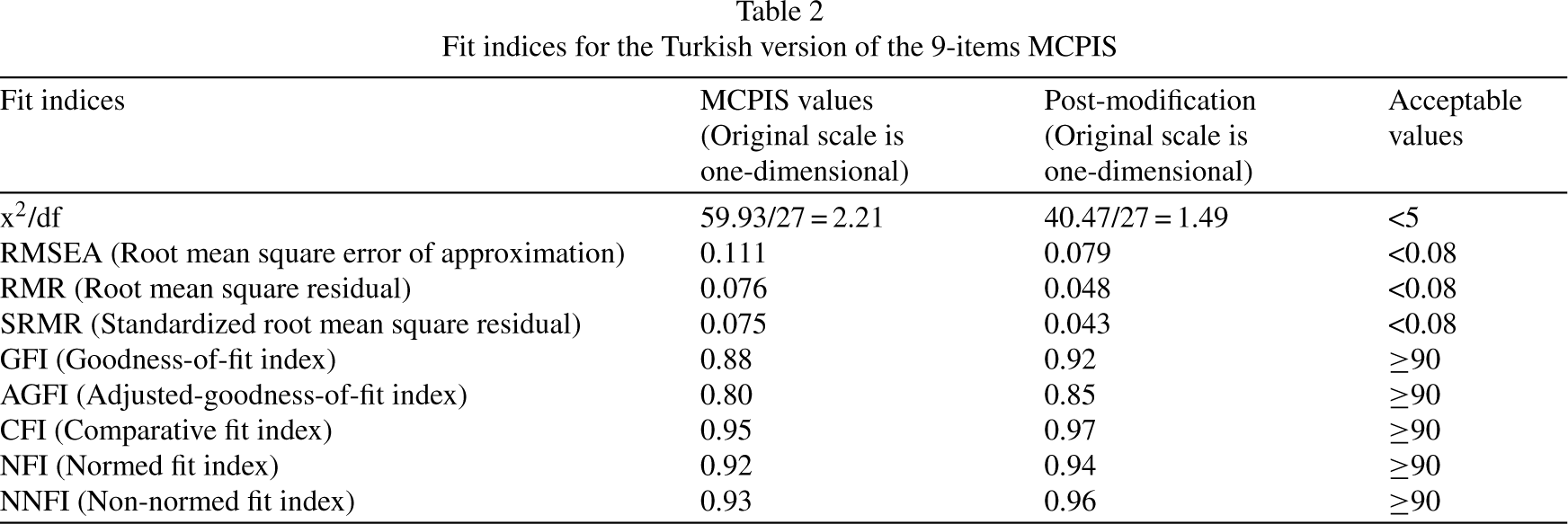
In the study, initially, CFA was conducted to assess the 9-item MCPIS developed by Adams et al. (2006) and determine its alignment with the theoretical structure. In this analysis, the covariance matrix was employed to examine the relationships among items and the Maximum Likelihood estimation method was applied to assess the generated matrix. Various goodness-of-fit indices were utilized to evaluate the data’s compatibility with the model, including χ2/df, RMSEA, RMR, SRMR, GFI, AGFI, CFI, NFI, and NNFI. Summary fit indices of the unidimensional model are given in Table 2.
Fit indices for the Turkish version of the 9-items MCPIS
Fit indices for the Turkish version of the 9-items MCPIS
It was observed that χ2/df, RMR, SRMR, CFI, NFI, and NNFI indices exhibited values within the acceptable range. However, the RMSEA, GFI, and AGFI indices fell below the acceptable thresholds (Fig. 1). Following two modifications aimed at improving the goodness-of-fit indices, the study found that χ2/df, RMSEA, RMR, SRMR, GFI, CFI, NFI, and NNFI indices reached acceptable levels, while the AGFI index remained below the acceptable threshold (Table 2). Consequently, the results of the CFA confirmed the one-factor structure of the 9-item MCPIS. Standardized estimates (Maximum Likelihood) for items 1, 2, 6, 7, 8, and 9 were above the acceptable threshold of 0.45, with values ranging between 0.67 and 1.00. However, for items 3, 4, and 5, the standardized estimates (Maximum Likelihood) fell between 0.27 and 0.43 (between 0.25 and 0.43 in the modified model). The t values for the 9-item MCPIS were found to be statistically significant at the p < .05 level. Factor loadings for the MCPIS model were observed to range from 0.28 to 0.93 (with factor loadings between 0.27 and 0.93 in the modified model).

Path diagram for the MCPIS.
Correlation values were calculated between the 9-item MCPIS score and the NPCS, a scale evaluating professional commitment and its sub-dimensions. A positive and strong correlation was found between the 9-item MCPIS and the NPCS (r = 0.701, p = .000). There was a positive and strong correlation between the sub-dimensions of Maintaining Professional Membership and Belief in Goals and Values and MCPIS (r = 0.848, p = .000; r = 0.793, p = .000, respectively), and a positive and very strong correlation between the Willingness to Make an Effort sub-dimension and MCPIS (r = 0.927, p = .000, Table 3).
Bivariate correlations between 9-items MCPIS and NPCS (n = 100)

Bivariate correlations between 9-items MCPIS and NPCS (n = 100)
The 9-item MCPIS was tested for predictive validity with the variables; satisfaction with the institution, satisfaction with the profession, and intention to quit the profession. A positive and moderate correlation was found between the MCPIS and the measures of satisfaction with the institution and satisfaction with the profession (r = 0.410, p = .000; rs = 0.454, p = .000, respectively). There was a negative and weak correlation between the MCPIS and the criterion of intention to quit the profession (rs=–0.388, p = .000). It was found that the mean scores of the nurses in the MCPIS who evaluated the working conditions poorly were lower than those who evaluated them well and moderately, and the mean scores of the nurses who partially liked and disliked the profession were lower than the mean scores of those who liked the profession (p < .05). Table 4 presents the results of the regression models. The models in Table 4 show the extent to which each independent variable is related to basic professional identity by controlling for other independent variables in the model. The direction and strength of the relationship between professional identity and the independent variables can be determined by examining the sign, significance, and magnitude of the regression β coefficients. Model diagnostics were checked and found to be at acceptable levels. [Regression assumptions were checked against the assumptions of the regression model (normality, linearity), such as case-by-case diagnostics, multicollinearity diagnostics (including VIF and tolerance), outliers, and model fit; all were found to be acceptable]. All three models had a significant F-ratio at the 95% confidence level.
Multiple regression model predicting the professional identity of graduate nurses

Multiple regression model predicting the professional identity of graduate nurses
b<0.05, a < 0.001, Note: Standard errors are shown in parentheses.
In this study, the psychometric properties of the Turkish version of the 9-item MCPIS were evaluated. The study included two parts: the first part focused on presenting the basic distributional properties of the scale items, while the second part examined reliability and validity findings. The study had a sample size of over 100 participants, which is recommended in accordance with literature guidelines. Having a sample size that is at least 5–10 times the number of items on the scale is considered appropriate for psychometric evaluations [11, 12]. The mean total score of the 9-item MCPIS Turkish form was 33.79±6.47 (Min-Max: 15.00–45.00; Median: 35.00). The mean total item score was 3.75±0.71, (Min-Max: 1.67–5.00; Median: 3.88). In a study conducted by Cowin et al. (2013) with nursing students (n = 162), the mean MCPIS item-total score in the original English language was reported as 4.18±0.55 [13]. In a descriptive cross-sectional study of 102 paramedic students on a university campus, the range of MCPIS scores was between 15 and 45, with a mean score of 38.77 and a standard deviation of 4.89 [29].
Regarding the reliability findings, the Cronbach Alpha reliability coefficient for the whole scale was 0.85, and it can be said that the internal consistency of the 9-item MCPIS in the Turkish version is as high as recommended. In the original scale study, in which the majority of the sample consisted of nursing students (48%), the Cronbach alpha reliability coefficient of the nine-item single-component scale in English was found to be 0.79 [1]. Worthington and colleagues (2013) investigated the validity and reliability of the MCPIS when administered to first-year undergraduate nursing students in its original (English) language. Their findings revealed a Cronbach Alpha reliability coefficient of 0.83 [14]. Similarly, Cowin et al. (2013) reported a Cronbach Alpha reliability coefficient of 0.78 in the original (English) version of the scale when utilized in their study involving nursing students [13]. In a separate study that aimed to translate the 9-item MCPIS into Persian and assess its psychometric properties among Iranian nursing students, the Cronbach’s alpha value was established at a robust 0.87 [30]. It is noteworthy that our study demonstrated high reliability-coefficients across three language versions of the scale, encompassing English, Persian, and Turkish.
In our study, we conducted an internal consistency analysis, which revealed a minimal increase (from 0.85 to 0.86) in the Cronbach’s alpha values for items 3 and 5 when they were removed from the scale. However, it is important to note that even with the removal of these two items, the Cronbach’s alpha values did not exceed 0.85 for any of the items. Given that the removal of items from a scale is generally discouraged in scale adaptation studies, as supported by the existing literature [26], we made the decision to retain all original items in the scale. This choice was made because the model we were validating was not specific to a particular sample. Worthington et al. (2013) previously reported a unidimensional structure for the 9-item MCPIS, consistent with our findings [14].
In our study, we evaluated item-total score correlations, which assess how well each item aligns with the overall scale [11]. These correlations ranged from 0.34 to 0.88, indicating that the items shared similar characteristics and displayed strong internal consistency. Consequently, in the Turkish version of the 9-item MCPIS, we found an acceptable level of reliability, with all items effectively measuring similar qualities.
Furthermore, Hotelling’s T2 test was conducted, and it revealed a significance level of p < .05, which indicated that the scale did not exhibit response bias, adding further credibility to our findings.
Regarding construct validity, we employed a Confirmatory Factor Analysis (CFA) to assess the scale’s conformity with the original theoretical structure established by Adams et al. (2006), and it was determined that the goodness of fit indices other than RMSEA, GFI, and AGFI met acceptable values. After two modifications to evaluate the change in the goodness of fit indices, it was determined that all the goodness of fit indices except the AGFI goodness of fit index met acceptable values. These findings indicate that the single-factor theoretical structure of the 9-item MCPIS by Adams et al. (2006) was confirmed, and the scale items adequately represented the single factor [1]. In the study of Cowin et al. (2013), who compared five scales on professional identity in a sample of nursing students, the goodness of fit results obtained from CFA were χ2/df = 277.917/27 = 10.29, RMSEA = 0.240, and GFI = 0.71 [13]. In this study, better goodness of fit indices was obtained compared to the results of Cowin et al. (2013). The results indicate that the study data showed a good fit for the original model. In Cowin et al.’s study from 2013, where they compared five professional identity scales among a sample of nursing students, the goodness-of-fit results from the CFA were as follows: χ2/df = 277.917/27 = 10.29, RMSEA = 0.240, GFI = 0.71 [13]. Our current study yielded even more favorable goodness-of-fit indices when compared to Cowin et al.’s results (2013), which suggest that our data aligns well with the original model.
The strong correlations (r-value from 0.701 to 0.927) observed between the 9-item- MCPIS and the NPCS and its sub-dimensions, which assess professional commitment in nursing, provide robust evidence of the scale’s validity. These strong correlations also indicate the presence of a strong professional identity among individuals with high professional commitment. Consistent with existing literature, it has been reported that an inadequately developed professional identity can contribute to nursing students dropping out of their programs and established nurses leaving the profession [14].
In terms of predictive validity, our study examined various criteria, including satisfaction with the institution, satisfaction with the profession, intention to quit the profession, working conditions, and liking the profession. Positive correlations were found between the 9-item MCPIS and the criteria of institutional and professional satisfaction, while a negative correlation was observed with the intention to quit the profession, which demonstrated that the scale possesses predictive validity. Regarding working conditions and liking the profession, the higher mean scores among nurses who rated working conditions favorably and expressed a liking for the profession indicate that the scale can discern anticipated differences in these areas. The literature has consistently highlighted how a strong professional identity contributes to increased job satisfaction and reduced intentions to leave the nursing profession [13, 31–33]. Additionally, the original scale study reported statistically significant relationships between students’ professional identity, work experience, understanding of teamwork, self-reported knowledge about their own profession, and cognitive flexibility [1].
A study comparing the psychometric properties of professional identity scales in health program students using the Consensus-based Standards for the Selection of Health Measurement Instruments (COSMIN) checklist rated the quality of the 9-item MCPIS as “good” [34]. This study also noted the scale’s developmental aspect over time, as it captured changes in knowledge, beliefs, and values through social interactions, which was considered a strength; however, it identified deficiencies related to the conceptual framework as a weakness [35].
It is important to acknowledge certain limitations of the 9-item-MCPIS. As a self-report scale, responses may be influenced by social desirability bias. To address this limitation, we implemented anonymous data collection and confidential data management. Another limitation is that the scale lacks subscales; all items are grouped within a single domain. Lastly, it is worth noting that our sample primarily consisted of nursing professionals pursuing postgraduate education, and our results are presented within this context.
Conclusion
In conclusion, the Turkish adaptation study of the 9-item unidimensional “Macleod Clark Professional Identity Scale” with a sample of postgraduate Turkish nursing professionals demonstrated an acceptable level of validity and reliability. This makes it a valuable and practical measurement tool for conducting studies on professional identity among healthcare professionals.
Author contributions
Ethical approval
Permission was obtained from Adams et al. (2006) via email for the adaptation of the measurement tool into Turkish. Additionally, ethical approval for the study was obtained from the local ethics committee of the institution where the researchers are affiliated (Decision date: December 01, 2021; Decision No: 20.478.486/1070).
Informed consent
All nurses signed an informed consent form prior to enrollment in the study.
Conflict of interest
None to report.
Footnotes
Acknowledgments
Not applicable.
Funding
Not applicable.